This brochure was published by the City of Göteborg
Source: Working together for a drug-free society SRF_Broschyr(SWEDEN) January 2009

Promoting Good Practice In Prevention
This brochure was published by the City of Göteborg
Source: Working together for a drug-free society SRF_Broschyr(SWEDEN) January 2009
Received from AALM Americans Against Legalising Marijuana – 09 October 2025
| On The Ingraham Angle, Fox News medical contributor Dr. Marc Siegel responded to a recent video from President Donald Trump, who appeared to endorse CBD use among seniors.
Dr. Siegel’s reaction was both clear and alarming: “Marijuana is the most dangerous drug in America.” He cautioned that while CBD is often marketed as a harmless wellness product, the truth is far more complicated. Many CBD items sold today are unregulated and frequently contain undisclosed levels of THC, the psychoactive compound found in marijuana. Dr. Siegel explained that modern marijuana is 20 to 30 times stronger than it was in decades past, creating unpredictable effects—especially for older adults who may already be taking multiple medications. For seniors, the combination of high-potency THC and prescription drugs can lead to confusion, anxiety, and dangerous interactions. Siegel emphasized that Americans are being lulled into a false sense of safety by clever marketing and political endorsements that blur the line between medicine and addiction. Despite being sold as “natural” and “therapeutic,” these products remain largely untested, inconsistent, and risky, particularly for vulnerable populations. 🚨 Why It MattersPresident Trump’s public support for CBD among seniors raises serious concerns about normalizing drug culture under the guise of health and wellness. When national figures promote substances without FDA oversight or long-term safety data, the result is confusion, not compassion. Seniors deserve real medical protection, not another gateway to unregulated drug exposure. At Americans Against Legalizing Marijuana (AALM), we stand with medical professionals like Dr. Siegel in calling out this dangerous trend. We are urging policymakers to investigate how CBD and marijuana marketing is targeting older Americans and to hold those responsible accountable. |
To access the full article, please click on the ‘Source’ link below.
Source: https://static1.squarespace.com/static/599a426ee45a7ccab72c77d2/t/63b361cb6350f410413b2878/1672700379514/Risks+of+Marijuana+Use+%28AALM%29.9.1.2022.pdf
by DAVID EVANS – 19 August 2025
There are established five schedules of controlled substances, to be known as schedules I, II, III, IV, and V.
(1) Schedule I–(A) The drug or other substance has a high potential for abuse.(B) The drug or other substance has no currently accepted medical use in treatment in the United States.(C) There is a lack of accepted safety for use of the drug or other substance under medical supervision.
(2) Schedule II–(A) The drug or other substance has a high potential for abuse.(B) The drug or other substance has a currently accepted medical use in treatment in the United States or a currently accepted medical use with severe restrictions.(C) Abuse of the drug or other substances may lead to severe psychological or physical dependence.
(3) Schedule III–(A) The drug or other substance has a potential for abuse less than the drugs or other substances in schedules I and II.(B) The drug or other substance has a currently accepted medical use in treatment in the United States.(C) Abuse of the drug or other substance may lead to moderate or low physical dependence or high psychological dependence.
(4) Schedule IV–(A) The drug or other substance has a low potential for abuse relative to the drugs or other substances in schedule III.(B) The drug or other substance has a currently accepted medical use in treatment in the United States.(C) Abuse of the drug or other substance may lead to limited physical dependence or psychological dependence relative to the drugs or other substances in schedule III.
(5) Schedule V–(A) The drug or other substance has a low potential for abuse relative to the drugs or other substances in schedule IV.(B) The drug or other substance has a currently accepted medical use in treatment in the United States.(C) Abuse of the drug or other substance may lead to limited physical dependence or psychological dependence relative to the drugs or other substances in schedule IV.
Moving marijuana to Schedule III would not legalize the drug, however, the change would greatly serve to benefit state legalized commercial marijuana companies who would no longer be subject to IRS Section 280E and thus could deduct business expenses and drastically increase their profit margins. This means more advertising and normalization. Not only would this mean that marijuana corporations would be able to deduct expenses for advertisements appealing to youth and the sale of kid-friendly marijuana gummies, but it would also dramatically increase the industry’s commercialization ability.
—
Source: www.drugwatch.org (drug-watch-international@googlegroups.com)

Can New York clean up its public drug-use problem?
Mayor Eric Adams aims to try: On Thursday, he called on the state Legislature to allow clinicians and judges to compel people into treatment when their drug use is hurting them and the city.
“We must help those struggling finally get treatment, whether they recognize the need for it or not,” Adams said at an event hosted by the Manhattan Institute (where I work).
“Addiction doesn’t just harm individual users; it tears apart lives, families and entire communities, and we must change the system to keep all New Yorkers safer.”
Adams’ proposed state law, the Compassionate Interventions Act, may face an uphill battle in Albany, as “harm reduction” advocates assail it as coercive and dangerous.
But involuntary treatment should be a tool in New York’s arsenal for dealing with the public drug use that has plagued it for years.
Last year it reported nearly 4,000 homeless residents with a history of chronic substance use — probably an undercount, as such people are less likely to be identified by the city’s annual late-night census.
Regardless, it’s not hard to find people shooting up on New York’s streets — just visit the Hub in The Bronx or Washington Square Park in Manhattan.
Such behavior makes whole swaths of the city unlivable.
Public drug use hurts both users — there were more than 2,100 overdose deaths in the five boroughs last year — and the places where they use.
It deters commerce, and creates environments conducive to more serious crime.
Too often the city has responded to these situations with benign neglect, exemplified by its two “supervised consumption sites,” which give people a place to use with Narcan-wielding staff standing by.
These sites continue to operate, in spite of the fact that they don’t work and violate federal law.
Leaving people free to abuse drugs, it turns out, doesn’t save lives.
Involuntary treatment, by contrast, tries to correct the behavior that drives drug users to hurt both themselves and others.
That’s why 37 other states already permit it — and why New York under Adams’ plan would join them.
Critics will insist that involuntary drug treatment doesn’t work, and that people have to want to change.
But the balance of the evidence suggests that involuntary treatment performs as well as voluntary treatment.
That’s backed up both by older research on California’s involuntary-treatment scheme, and by strong indications that drug courts, which route drug offenders into treatment instead of prison, can reduce recidivism.
Opponents will also say that it’s immoral to compel people to get treatment they don’t want, and that it violates their “bodily autonomy.”
But there’s no right to shoot up in public spaces, or to ruin your body with fentanyl. And New Yorkers should have the right to expect their public spaces to be free from disorder, including public drug use.
The biggest challenge for Adams, though, may be the state’s limited treatment capacity.
New York state as a whole has only 134 long-term residential treatment facilities.
As of 2023, the most recent available data, they were serving 2,935 clients — fewer than the city’s tallied homeless drug-addict population.
Implementing the Compassionate Interventions Act will almost certainly require more funding for treatment beds, much as Adams’ previous efforts to institutionalize the seriously mentally ill did. That will have to be part of any ask in Albany.
But the mayor’s proposal will also allow diversion to outpatient treatment programs, including a new $27 million investment in contingency management therapy — an evidence-based intervention that has been shown to help treat drug addiction.
What happens if Albany says no to Adams’ proposal? Or if Adams is out of the mayoralty come the next legislative session?
The NYPD can still work to clear encampments. And the city can still try to divert drug users into its drug-courts system, which, while useful, faces administrative problems and lacks transparency.
But actually getting drug users the help they need, rather than just cycling them through the city’s jails, will be hard — much as the administration struggled to handle the seriously mentally ill before it had the power to compel them into treatment.
SOURCE: https://nypost.com/2025/08/14/opinion/involuntary-treatment-can-solve-the-public-drug-scourge/
Dear Surgeon General Adams,
I am an Australian Professor of Addiction Medicine and researcher at the University of Western Australia and Edith Cowan University both in Perth, Western Australia.
I have been becoming increasingly concerned at the implications of cannabis legalization across USA for patterns of congenital anomalies both in USA and across the world.
The incidence of many congenital anomalies are rising in many places. This rise is even more marked if therapeutic early termination for anomaly (ETOPFA) are taken into account.
In 2007 the American Academy of Pediatrics issued a position statement which noted that cannabis was a known teratogen for cardiovascular anomalies based on three studies. They cited ASD, VSD and Ebstein’s anomaly in particular as major concerns. This is also important as cardiovascular anomalies form the largest single group of congenital anomalies. As you would be well aware foetal anomalies is the single major cause of death in the first year of life. The aetiological pathway is further strengthened by the fact that the endocardial cushions have high density expression of CB1R’s cannabinoid type 1 receptors from very early in embryonic life. This fits with the significant association of cannabis with defects of structures derived from the endocardial cushions and the associated conoventricular ridges including the cardiac valves and the interatrial and interventricular septa.
Prof. Peter Fried in Ottawa has headed up a comprehensive, careful and detailed longitudinal study of brain damage in children exposed to cannabis in utero. They have been publishing positive findings from this study for forty years showing documented deficits of executive and higher brain function, the need to recruit more brain to perform tested tasks documented on fMRI, in primary school, middle school, high school and even into young adulthood. It has now been convincingly demonstrated that endocannabinoids send the “off” signal halting synaptic neurotransmission at both stimulatory and inhibitory synapses and hence shutting down the brain’s normal oscillatory processes. Brain oscillations are known to form a key an pivotal function early in brain development guiding the migration and axonal projection of developing neuronal progenitor cells, and also guiding synapse formation.
As you would be aware many neural progenitor cells fail to integrate into the neural network and die due to lack of circuit stimulated connectivity. This applies to both stimulatory and inhibitory synapses. Hence synaptic firing is therefore critical for synapse formation and integration and survival of the new nerve cells. Since cannabis and its constituent cannabinoids shut down this firing and resultant neural oscillations they necessarily impede brain development both in the cortex and in key subcortical major centres including the thalamus and hypothalamus. Hence the demonstration by the Fried group that cannabis users have smaller cortical thickness and hippocampal volumes – the hippocampus first encodes memory – fits well with the known developmental biological mechanisms.
Given that cannabis in Colorado now is commonly at or above 30%, and was historically only 1-2% when most of its epidemiological studies were done; and given also that cannabis oils at up to 99% THC content are also increasingly widely available the conclusion becomes inescapable that the vast majority of children significantly exposed to these concentrations of cannabis in utero will be adversely and permanently affected. Importantly no population measure of this very important damage I easily accessible.
10 studies have linked cannabis exposure to incidence or severity of gastroschisis. This case is strengthened by the high density of CB1R’s on the omphalovitelline artery, and the many studies now which implicate vasoactive drugs in the pathogenesis of this condition. Indeed although the activity of cannabinoids on arterial structure is not widely understood is has been documented in minute detail by no lesser a resource that Nature Reviews of Cardiology. And obviously cannabis arteriopathy underlies the elevated rate of both myocardial infarction and stroke seen in adults with cannabis exposure about which Dr Nora Volkow, Director of NIDA has commented in New England Journal of Medicine.
A spectacular study from Hawaii in 2007 demonstrated that cannabis use was associated with Down’s syndrome incidence at a rate 526% elevated above background.
This is significant for several reasons. Firstly a substantial body of evidence shows that cannabis has been known to test positive in the micronucleus assay since the 1960’s. This is a major test for genotoxicity. The implications of this devastating genetic damage were worked out for the whole world to see by David Pellman’s lab in New York and links cannabis exposure directly with abnormalities of cellular division including the three major clinical trisomies – trisomies 21, 18 and 13 – and Turner’s syndrome, XO.
Furthermore this implies that since cannabis is linked with cardiovascular, neuropsychiatric and chromosomal defects, these being the three major groups of congenital disorders.
If one goes to Colorado as a rather obvious test case indeed one finds a rise there of 70% in both total major congenital anomalies, and also cardiovascular anomalies, especially atrial septal defect and ventricular septal defects, which are the most common, exactly as predicted by the embryology.
Indeed, the particular thoroughness of the way in which all kinds of social and health data is collected and made available in the USA, together with the very considerable spread in attitudes to drug legalization in different states, make USA the perfect teratological laboratory to study the mutagenic and genotoxic effects of cannabinoid exposure. My colleagues in addiction medicine and I at my university, aided by some of the top statisticians in this country have now commenced the enormous task of analyzing the US cannabis exposure data by state from the National Survey on Drug Use and Health, together with cannabis concentration data quoted by Dr Nora Volkow the Director of NIDA in New England Journal of Medicine, together with projections of the applicable therapeutic termination rates taken from the Western Australian Register of Developmental Anomalies are analyzing this data at this time.
Whilst our findings have not been finalized the following remarks can already be made:
The population exposure to cannabinoids remains highly significant including consideration of state and year
Please note that none of these metrics quantitate what I regard as the most serious area of all – the neurobehavioural toxicology so carefully documented and chronicled with every imaginable psychological and imaging test at every developmental stage into young adult by the methodical Ottawa investigators referenced above.
I am aware of course of the signal service performed in this area by your predecessor Dr Murthy in relation to his report on “Facing Addiction in America.”
Naturally I am very concerned indeed that the USA, having avoided the horrors of thalidomide directly due to the due diligence of your FDA staff at the time, is sailing directly into an even worse teratological morass related to the legalization of cannabis in your country, which apparently even your President appears to be powerless to avert. It is of the greatest concern to me that the carefully orchestrated US cannabis legalization campaign seems to be operating is such a manner as to at once bypass and simultaneously intimidate the FDA quality control and checks and safety balances processes.
The medical conclusion appears inescapable to me that cannabis use should be avoided by males and females in the reproductive age group especially if involved in pregnancy or even considering pregnancy – because of the long half lives involved and its sluggish release from the body’s fat stores. It is well known that these same young adults is the group most keen to use cannabis products! Indeed it is well documented that cannabis both increases sexual libido and reduces inhibitions; albeit after time and habituation it reduces both sexual desire and performance. This sets up an inescapable and unavoidable reproductive and genotoxic paradox – which also greatly escalates the present discussion beyond the arena of personal civil liberties to the future of our coming generations.
Naturally I am particularly keen to discuss these issues with yourself at your earliest available opportunity.
The teratological aspects of this epidemic seem to have been completely and systematically overlooked in the current discussions.
Please help me assist your wonderful, beautiful, noble and courageous nation at this critical juncture in your history.
And I am sure it will be self-evident to you that anything that happens in USA has enormous ramifications around the world, as you are obviously that world’s leading democratic nation.
Hence USA is not only legislating for America – but for all citizens of the planet – present and future. Because of the epigenetic implications – not discussed above but very well substantiated nonetheless – for the next four generations – this is the next 100 years.
In such a circumstance – truth can be your only meaningful defence. And it must be your final bastion – and the last great hope of civilization.
I am very keen to set up a time which would be suitable to yourself to discuss these issues on the phone.
Oddly it seems to me that few professionals understand these issues thoroughly.
And even more strangely – it seems to me strange that USA, having alone amongst the family of nations done so extremely well with thalidomide, at the present time gives every appearance of acting before she has thought carefully, methodically and deeply about the ramifications of her present actions in this field.
With very best wishes,
Yours sincerely,
Dr. Stuart Reece,
Australia.
Email sent in copy to Drug Watch International June 2018 drug-watch-international@googlegroups.com
![]()
by Robyn Oster – Associate Director, Health Law and Policy – July 2025
Reminder: The U.S. Preventive Services Task Force (USPSTF), an expert panel, evaluates preventive services and recommends which should be provided at no cost.
The details:
The bigger context:
Source: https://drugfree.org/drug-and-alcohol-news/supreme-court-upholds-aca-preventive-care/
itvx news – Tuesday 24 June 2025

Cannabis activists and entrepreneurs, hold cannabis plant as they march to Government House in Bangkok, Thailand in 2024.Credit: AP
Thailand is moving to pass new legislation banning cannabis for recreational use in a major reversal, three years after the country became the first in Asia to decriminalise the drug, local media reports.
On Tuesday, Public Health Minister Somsak Thepsuthin said he had signed an announcement limiting cannabis to medical use only, Bangkok news site Khaosod confirmed.
Under the changes, people wishing to purchase cannabis must have a doctor’s prescription and a medical certificate indicating their illness.
Operators selling the drug will need to have a doctor present at the shop to renew or apply for a license to sell.
Somsak also said that in the future, cannabis will return to being considered a narcotic.
It is not clear when the regulation will take effect or when it will be re-listed.
Banged up abroad: How many Brits are being arrested over alleged drug smuggling?
Thailand to crack down on cannabis after smuggling cases involving UK tourists
Is cannabis legal in Thailand?
Medical marijuana has been legal in Thailand since 2018, but decriminalisation in 2022 took things a step further, making it no longer a crime to grow and trade marijuana and hemp products, or to use any parts of the plant to treat illnesses.
It was a rarity in the region where many countries give long jail terms and even death sentences for people convicted of marijuana possession, consumption or trafficking.
Smoking marijuana in public remained illegal even under the relaxed laws.
Subscribe free to our weekly newsletter for exclusive and original coverage from ITV News. Direct to your inbox every Friday morning.
What happened when cannabis was decriminalised?
The relaxed laws saw a lucrative cannabis industry catering to locals and foreigners alike boom across the Southeast Asian nation, with thousands of cannabis dispensaries sprouting up across Thailand, as well as other cannabis-themed businesses like weed cafes and hemp spas, and beauty treatment.
Cities like Chiang Mai and the capital Bangkok have even held weed festivals, and decriminalisation has been a major draw for tourists.
Pro-legislation advocates have argued that the cannabis boom across Thailand has helped many Thais, from farmers to small business owners and workers behind the counter.
Critics say the decriminalisation was rushed through, causing confusion about the regulations.
Last year, a new conservative government vowed to tighten the rules around the drug after a string of alleged smuggling cases involving tourists.
Hundreds of British citizens are currently detained across the world, accused of narcotics smuggling offences.
Prisoners Abroad – a charity assisting Britons who are arrested and detained overseas – told ITV News it is currently supporting 431 people around the globe who are facing drugs charges.
This includes 22 people in Thailand.
Source: https://www.itv.com/news/2025-06-24/thailand-to-ban-recreational-cannabis-three-years-after-decriminalisation
DAVE EVANS, LISKOWITZ V. describes a significant victory re Vapes. The court upheld the Complaint for:
COUNT I:
DEFECTIVE DESIGN – NEW JERSEY PRODUCTS LIABILITY ACT – N.J.S.A. 2A:58C-1 ET SEQ.
COUNT II:
PRODUCT LIABILITY – FAILURE TO WARN (NEW JERSEY PRODUCTS LIABILITY ACT – N.J.S.A. 2A:58C-1 ET SEQ.
III and VI were dismissed without prejudice
The order – -which runs to 30 pages – can be accessed hereby:
To access the full document: Click on the ‘Source’ link below, at the foot of this web page.
* * * * * *
In a first of its kind lawsuit in New Jersey, a victim of Big Cannabis is seeking to hold it accountable for the terrifying mental health disorder Plaintiff suffered after using intoxicating hemp cannabis products.
The plaintiff is an athletic professional. While training, Plaintiff began consuming intoxicating cannabis hemp products.
After a few months of use, Plaintiff became psychotic and suicidal, suffering from extreme delusions and paranoia, and was hospitalized. After the hospitalization, the Plaintiff was discharged to Plaintiff’s parents, and they flew back to their home state for further treatment.
While traveling, the Plaintiff believed that they were being followed by the FBI and would be subject to arrest. To protect the parents from arrest, Plaintiff sought the opportunity to flee. While traveling home from the airport, the plaintiff jumped out of the back seat car window and ran across six lanes of traffic and, to the horror of the parents watching from the car, and jumped off a 135-foot bridge, landing head-first into a river.
Miraculously, Plaintiff survived, but Plaintiff’s injuries included a torn ACL, right shoulder dislocation, and extensive road rash. Plaintiff subsequently received substance abuse and psychological treatment and stopped using hemp products. Plaintiff and family are still recovering from this harrowing ordeal.
As established by decades of medical research and as recognized by the National Institute of Health (NIH), the National Academy of Sciences, and the Center for Disease Control (CDC), cannabis use is indelibly linked to the development of psychosis and other mental health disorders such as schizophrenia, suicidal ideation, and depression.
Despite the robust evidence, Big Cannabis refuses to warn consumers of the devastating potential side effects. Worse, Big Cannabis actively and maliciously markets these products as safe, even medicinal.
We are in the midst of a gathering mental health epidemic caused by increasing use of cannabis, especially high-potency cannabis after years of Big Cannabis’s sophisticated and coordinated legalization efforts. There are tens, if not hundreds, of thousands who have been injured in a similar way to the Plaintiff. Many, however, have failed to draw the connection between their cannabis use and their mental health disorders because the public relations arm of Big Cannabis has so effectively hidden and confused the association in an effort to realize extravagant profits.
This suit, drawing upon various consumer protection laws, seeks to hold the cannabis industry accountable for its lies and its failure to adequately warn an unsuspecting public of its products’ considerable and often devastating dangers.
The suit also seeks to raise awareness about the association between cannabis and mental health disorders so that those affected current or former users who have suffered at the hands of Big Cannabis can take action.
The case has survived a Motion to Dismiss
The Plaintiff is being represented in this matter by attorney David Evans whose office is in Flemington NJ . If you, or someone you know, has been affected by cannabis, Mr. Evans will be happy to discuss your potential claims.
Mr. Evans can be reached at 908-963-0254. (www.addictionslaw.com)
To access the full document:
Possession of hard drugs such as cocaine and heroin treated as a health issue rather than a criminal matter by UK forces
It represents a six-fold increase in drug users escaping prosecution since 2016, when the proportion was only 7.5 per cent.
In some forces, more than 80 per cent caught with cocaine, heroin or other class A drugs escaped any criminal punishment.
They were instead handed community resolutions, which do not result in a criminal record and only require an offender to accept “responsibility” for their crime, or were let off “in the public interest”.
Only a third of class A drug possession offences resulted in a charge.

But critics have warned police against “decriminalising drugs via the back door by ignoring tens of thousands of offences”.
At least a quarter of the 43 police forces in England and Wales have adopted “diversion” schemes where users caught with small amounts of drugs like cannabis are “diverted” to treatment or education programmes rather than prosecuted, particularly for first-time offences.
Nearly three-quarters (72.1 per cent) of those caught in possession of cannabis were let off without any criminal sanctions.

The Treasury and Cabinet Office have put £1.9 million into evaluating the approach in partnership with five universities, the National Police Chiefs’ Council (NPCC) and the College of Policing, the standards body for forces in England and Wales.
The College said the aim of the diversion scheme was to “reduce re-offending and wider harms by approaching substance use as a health issue rather than a criminal justice issue”.
The research will compare re-offending rates, hospital and treatment admissions with the aim of establishing “whether and how drug diversion works, for whom, when and why”.
But Chris Philp, the Tory shadow home secretary, warned the move amounted to decriminalisation by stealth.
“Parliament has rightly legislated that certain drugs are illegal because they cause serious harm to health, lead to antisocial behaviour and fuel acquisitive crime like theft, burglary and shoplifting as addicts steal to fund buying drugs,” he said.
“Police should not be decriminalising drugs via the back door by ignoring tens of thousands of offences. People who break the law should be prosecuted, and a magistrate or judge can decide what to do.
“Options a magistrate has available include fines, community service and addiction treatment requirements as well as prison.
“We have seen many US and Canadian cities devastated by soft drugs policies. These have allowed ghettos to develop where zombified addicts loiter unpunished and law abiding members of the public fear to go. We can’t allow the UK to go the same way through weak policing.
“We need a zero tolerance approach to crime, including a zero tolerance approach to drug taking.”
But the College of Policing defended its approach and pointed to research, based on 16 different studies, that showed drug diversion had resulted in a “small but significant” reduction in drug use, particularly among young people.
The Telegraph analysis showed that Warwickshire had the lowest proportion of offenders caught with class A drugs who were let off, at just 9.2 per cent, while Dyfed Powys had the highest at 88.6 per cent.
Nerys Thomas, Director of Research at the College of Policing, said:“We are focussed on cutting crime and keeping the public safe. Class A drugs are the most harmful category and being found in possession of them is a criminal offence.
“The government has provided funding to understand what initiatives could be used to reduce offending and protect the public. This includes a piece of work between the College, the University of Sheffield and 11 other agencies across the criminal justice system to interview hundreds of officers and drug offenders and analyse police data to understand if diversion schemes can reduce crime.
“The results of this study will be made publicly available next year.”
Source: https://www.telegraph.co.uk/gift/6e423b9614e616f8
For Immediate Release
June 7, 2018
Contact: Bob Bushman
The National Narcotics Officers Association Coalition today released a letter to the President urging him not to weaken the memo issued by US Attorney General Jeff Sessions on January 4, 2018. The letter warns the President of the connection between legalized marijuana, the black market, and foreign cartel activity, as extensively documented by NBC News and Newsweek.
The text of the letter is as follows:
June 7, 2018
The President
The White House
1600 Pennsylvania Avenue, N.W.
Washington, D.C., 20500
Dear Mr. President,
We write as representatives for major law enforcement organizations representing federal, state, and local law enforcement. We are deeply concerned about reports that you may be considering action to overturn the January 4, 2018 Memorandum from the Department of Justice that merely restates current federal drug laws.
The fact is, gangs and cartels have been making liberal use of legalization to provide cover for their illegal activities. These gangs have ties to Mexican, Cuban, Vietnamese, and Russian cartels.[i] The gangs often purchase homes in residential neighborhoods, wire in extra electricity and water capacity, and convert them into multi-million dollar grow houses in suburban neighborhoods. These gangs are also trafficking in other illegal drugs, organized crime, and prostitution. Crime has been steadily increasing in Colorado in all categories since legalization, including violent crimes.[ii]
Make no mistake, the black market does not honor state lines. Colorado and other legalized states have many embarrassing examples of providing cover for trafficking of marijuana to other states. In one of the most egregious examples, Operation Toker Poker, 62 people and 12 businesses were indicted for growing marijuana under the cover of legalization. Colorado Attorney General Cynthia Coffman said, “The black market for marijuana has not gone away since recreational marijuana was legalized in our state, and in fact continues to flourish.”[iii]
In another example, an organized crime unit with multiple licenses to grow and manufacture marijuana was finally caught after several years of shipping marijuana to other states. The Drug Enforcement Administration agents in Colorado indicated that this was a common arrangement.[iv]
Other states, like Oregon and California, have been growing much more marijuana than the state can consume and are mass exporters of marijuana to other states. The California Growers Association estimates that their members grow at least eight times as much marijuana as the entire state of California can consume and ship the rest out of state.[v] The Oregon State Police estimate that their state grows four to five times as much as it can consume, shipping the rest as far as Florida and even abroad.[vi]
We urge you to see through the smoke screen and reject attempts to encourage more drug use in America.
Sincerely,
National Sheriffs’ Association
Major County Sheriffs’ Association
Major Cities Chiefs Association
National Narcotics Officers’ Associations’ Coalition
National High Intensity Drug Trafficking Area Directors’ Association
Law Enforcement Action Network
CC: Marc Short, Office of Legislative Affairs
Kellyanne Conway, Counselor to the President
James Carroll, Acting Director of the Office of National Drug Control Policy
The Honorable Jefferson Sessions, Attorney General of the United States.
Source: Copy of letter June 2018 https://www.nnoac.com/
by Shane W. Varcoe , Director@dalgarnoinstitute.org.au – 23 May 2025
“I was talking to a tradesman in my home on Wednesday and he asked me what I did…. After explanation about Weed…. He said.. “I wen to a local doctor and just said I had trouble sleeping and can I have cannabis… got a script, no more questions asked.” This is so utterly corrupt and it’s ubiquitous now! ” Shane W. Varcoe
Comment by Jo Baxter, DFA (Australia)
This is a very serious situation for the US and the world generally. Such a softening is akin to what the then Federal Health Minister, Sussan Ley did when she passed the law that allowed Medicinal Cannabis to be legalised in Australia. Now we are seeing a misuse of the ‘legal’ system with doctors overprescribing and not even consulting in person with patients to whom they prescribe the drug.
On Fri, May 23, 2025 at 7:51 AM Herschel Baker <hmbaker1938@hotmail.com> wrote:
The evidence is in Cannabis must remain Schedule 1 Epidemiology of Cannabis Albert Stuart Reece, Gary Kenneth Hulse
https://shop.elsevier.com/books/epidemiology-of-cannabis/reece/978-0-443-13492-0
WASHINGTON, D.C. – During his confirmation hearing before the Senate Judiciary Committee on April 30, DEA administrator nominee Terrance Cole declined to commit to the proposed federal rescheduling of cannabis, leaving a critical policy question unresolved as the process transitions to new leadership under the Trump administration.
The popular and game-changing rescheduling proposal backed by Donald J. Trump to reclassify cannabis from Schedule I to Schedule III under the federal Controlled Substances Act (CSA) remains formally active but administratively paused by a DEA judge.
If enacted, rescheduling cannabis to Schedule III would formally acknowledge the accepted medical use of cannabis under federal law. It would also allow for FDA-supervised research and development of cannabis-based drugs.
Although cannabis would still be classified as a controlled substance and remain under the oversight of the DEA and FDA, reclassifying it to Schedule III would significantly benefit legal cannabis businesses by changing how they are treated under federal tax law.
Specifically, it would exempt them from the limitations of Section 280E of the Internal Revenue Code, which currently bars businesses trafficking in Schedule I or II substances from deducting ordinary business expenses. Due to this restriction, legitimate cannabis companies paid over $1.8 billion more in federal taxes in 2022 than comparable non-cannabis businesses, according to data from Whitney Economics.
Reclassification would not federally legalize recreational cannabis, authorize interstate commerce, or override any state-level prohibitions.
Reclassification was initiated nearly three years ago during the Biden administration. Still, on January 13, 2025, one week before President Trump took office, the DEA’s Chief Administrative Law Judge cancelled a public hearing scheduled for January 21 and ordered parties to check back in with him in 90 days.
There is no statutory deadline for the DEA to complete the rescheduling process, so the current pause could extend indefinitely.
Cole, a longtime DEA official nominated to be administrator in February, told lawmakers on April 30 that reviewing the agency’s stalled administrative process to move cannabis from Schedule I to Schedule III would be “one of [his] first priorities.”
Though cannabis was not mentioned in Cole’s opening remarks, he emphasized a focus on combating the fentanyl crisis and leveraging his 30 years in law enforcement to address cartel-related threats. “It’s time to move forward,” he said of the stalled rescheduling process.
But when pressed by US Senator Alex Padilla (D-CA) on whether he would ensure the proposed rescheduling is carried out, Cole would not commit. Here is a bit of back and forth between the two:
“I need to understand more where they are and look at the science behind it and listen to the experts and really understand where they are in the process,” Cole said.
Padilla, referencing the directive initiated in 2022, reiterated: “We know where we are. We know what the directive is: Get it to Schedule III. Are you committed to seeing it to fruition?”
Cole responded, “So, I don’t know. I haven’t seen that, sir.”
“So, you’re leaving the door open to changing course as to—?” Padilla asked.
“I’m leaving the door open to studying everything that’s been done so far, so I can make a determination, sir,” Cole said.
Padilla concluded the exchange by stating: “So, make myself a note here—no answer to that particular question.”
Source: Shane W. Varcoe , Director@dalgarnoinstitute.org.au – 23 May 2025
This is a copy of an email sent by Stuart Reece to members of the Australian Northern Territory government, particularly addressing Dr Jennifer Buckley.
Dear Dr Buckley,
I am a Professor of Addiction Medicine at Edith Cowan University on Western Australia, and an Associate Professor of Addiction Medicine at the University of Western Australia. I hold an earned Doctorate of Medicine from the University of New South Wales in addiction to my basic medical degree.
I understand that your committee is considering adopting a harm reduction strategy focussed view of the management of drug addiction in the Northern Territory including the potential legalization and or decriminalization of all drugs in your jurisdiction.
I wish to place before you my carefully considered opinion that such a strategy would be an unmitigated disaster for the people in your care.
The strategies employed by the harm minimization lobby globally make it very plain that their rhetoric is merely the soft front edge of the full legalization approach sponsored by George Soros. In this country it has been championed by its unparalleled champion Dr Alex Wodak, President of Australia’s Drug Reform Foundation which unashamedly openly and overtly proposes the legalization of all drugs – goodness only knows why…
Why indeed … when there is overwhelming evidence of the innumerable harms directly attributable to drug addiction itself.
I work with drug addicts all day long. Most of those I work with in my clinic agree that slackening off of the laws in this area would be an unmitigated disaster – and that is drug addicts in treatment!!!!
One of the very obvious features of drug addicted patients – of all sorts – is the accelerated pattern of disease which they virtually all get. Disorders of brain, heart, circulation, liver, muscle wasting, psychology, bones, reproductive system and immunity together with cancers, elevated death rates and major anomalies in the babies born to addicted parents – have all been described in virtually every addiction.
It has recently been shown that the maintenance of cellular energy stores is critical to the upkeep and maintenance od NA. Without good energy stores DNA become fractured and broken, cells age, cancers form and abnormal babies are born and infertility rises. The community pays the cost – obviously; and individual patients bear the brunt of the illnesses.
It is known moreover that from age 20 the energy inside cells halves every 20 years. Declining cellular energy stores therefore form one of the key cellular measures of ageing. Restoring those energy stores is therefore a major project within anti-ageing medicine and a major therapeutic goal for clinical medicine.
IT HAS BEEN KNOWN FOR SEVERAL DECADES THAT ALL THE ADDICTIONS DRAMATICALLY REDUCE CELLULAR ENERGY STORES – AND THEREBY DIRECTLY PHENOCOPY CELLULAR AGING –WHICH OBVIOUSLY EXPLAINS THE POLY-SYNDROMIC MULTISYSTEMIC CLINICAL PRESENTATIONS OF DRUG ADDICTION.
For example data emerging from our still on-going analysis of the rates of deformed babies in Colorado show that most of the cannabis related anomalies are rising, which includes all of the fastest growing anomalies, and that the overall rate of congenital heart defects and total defects has almost doubled 2000-2013; Cannabis was only fully legalized in Colorado in 2014!!! That is the good news – for it has also been shown that cannabis interferes with the basic processes of brain formation also. The babies born to drug dependent parents are very obviously very far from normal in most cases – certainly when the addictions are severe – when indeed children are lucky to survive even until birth! So cannabis is a known teratogen and its widespread use is likely to cost the community very dearly in the years to come.
I have attached for your benefit some submissions I recently made to the FDA and WHO on the subject of cannabis genotoxicity and cannabis teratogenicity. With your permission I would also like to place this material which explores these themes in much greater depth, in evidence before your committee.
Since I have spent a whole professional lifetime studying these issues I trust it is clear that I could place mush more evidence before you.
I am happy to answer any other questions you might have.
Similar remarks can be made in relation to opioid and amphetamine abuse.
I understand clearly that in parts of the Northern Territory drug use is rife. I also understand that in parts drug use if forbidden by local community law and alcohol is banned in many places, so-called “dry communities.” The answer to this is proper education of the community and appropriate constraint of drug use and drug trafficking by law enforcement in line with our international obligations under the Single Convention, the United Nations Convention of the Rights of the Child and many others.
I would point out that it is my view, and also that of many other well informed experts and individuals, that the very obvious gaping hole in the our drug education for the community is an obvious major breech in our community response to the issues of drug enforcement, which almost alone allows the media-driven misinformation and disinformation of the crazy ideologues with virtually unlimited financial resources to push our society in directions which we would never normally go if the truth was well known and widely disseminated and widely taught and widely practised. It is the yawning gaping hole in the public education program alone which allows the lies, dissembling and dissimulation of the crazy anarchists to threaten not only the wellbeing of our communities, but indeed the sustainability of western culture into the future.
And I might add their genetic and epigenetic pool for the next hundred years….
That is to say – it is not the threats of the lies of the media barons and dysfunctional popular rock idol darlings – who keep committing suicide – which is the major threat to our culture – but the absence of truth in the public place – which is obviously officially sponsored – which allows these lies to flourish in the first place. The implication is that a modicum of well-informed public health education would quickly drown out a whole cacophony of media-driven highly-paid lies. It is therefore our joint responsibility to make sure that the popular narratives of our culture are fact-based and evidence-driven rather than purely ideological and agenda-driven as at present.
Thankyou for considering my material.
I am happy to work further with your committee to assist you in your deliberations.
Yours sincerely,
Prof. Dr. Albert Stuart Reece,
MBBS(Hons.), FRCS(Ed.), FRCS(Glas.), FRACGP, MD(UNSW).
Edith Cowan University, Joondalup,
Source: Copy of email sent to Drug Watch International for distribution by Stuart Reece. May 2018
To maximize their effectiveness, prevention programs must reach adolescents before they are exposed to substance use in their peer groups. Yet nearly one-third of 12- to 17-year-olds reported that they did not see or hear any substance use prevention messages in school, according to the 2023 National Survey on Drug Use and Health. This lack of prevention education has serious implications for health equity, as racial and ethnic minority youth are less likely to report seeing these messages in their schools.
Prevention takes a village. All sectors of a community must be aligned in order to set healthy norms. This approach guides the Drug-Free Communities Support Program, which involves sectors from businesses and media to schools and religious organizations.
Unfortunately, numerous actors that pursue private profits at the expense of public health actively undermine these efforts. These include marijuana shops and, more recently, psychedelics shops. Our children are given conflicting messages when we tell them not to use addictive substances now being promoted throughout their neighborhoods.
Given the increasing embrace of mind-altering drugs at the state level, it’s no surprise that drug use has risen. A study published in the Journal of the American Academy of Child and Adolescent Psychiatry found that recreational marijuana legalization was associated with a 13 percent increase in past-month marijuana use among youth ages 12 to 17, and a 22 percent increase among young adults ages 18 to 25. Between 2012 and 2023, the prevalence of marijuana use among 19- to 30-year-olds increased from 28.1 percent to 42.4 percent, while it more than doubled from 13.1 percent to 29.3 percent among 35- to 50-year-olds, according to the Monitoring the Future survey. Over this same period, annual overdose deaths nationwide more than doubled from 41,502 to 105,007.
As highlighted in the Foundation for Drug Policy Solutions’ The Hyannis Consensus: The Blueprint for Effective Drug Policy, the nation’s drug policy “should promote a health standard that normalizes the non-use of substances.” Our drug policies should not make it easier to use licit and illicit substances.

Other things being equal, the harms of drug use will decline as the prevalence of drug use declines. Notably, the White House recently estimated that the societal cost of illicit opioids was $2.7 trillion––with a “t”––in 2023, which is “equivalent to 9.7 percent of GDP.” Viewed through this lens, prevention is essential and must remain central to drug policy efforts. A proactive, upstream approach premised on prevention will also reduce strain on downstream systems like treatment and recovery.
Policymakers must remember that prevention programs are cost-effective. A 2016 report from the surgeon general explained:
Interventions that prevent substance use disorders can yield an even greater economic return than the services that treat them. For example, a recent study of prevention programs estimated that every dollar spent on effective, school-based prevention programs can save an estimated $18 in costs related to problems later in life.
National Prevention Week is also a fitting time to spotlight novel approaches to prevention. The Icelandic Model is particularly promising. A 2019 study explained that “by working to increase social and environmental protective factors associated with preventing or delaying substance use and decreasing corresponding risk factors, the model prevents substance use by intervening on society itself and across a broad spectrum of opportunities for community intervention.” In practice, this approach may encourage youth to join community groups and participate in extracurricular activities, which are protective factors against substance use.
To scale what we know works, White House Office of National Drug Control Policy director nominee Sara Carter should relaunch a national prevention campaign, similar to the National Youth Anti-Drug Media Campaign. Those public awareness efforts were particularly effective in reducing rates of tobacco use, and will help set strong anti-drug cultural norms and promote health.
The current administration deserves praise for centering prevention in a recent statement of its drug policy priorities. We fully support its plan to “encourage educational campaigns and evidence-based prevention programs, particularly in schools and communities.” But it’s time we back it up with dollars and programs. As we recognize National Prevention Week, we must not forget about the importance of prevention and its role in helping more Americans live healthy, drug-free lives.
Dr. Kevin Sabet is President of Smart Approaches to Marijuana (SAM) and the Foundation for Drug Policy Solutions (FDPS) and a former White House drug policy advisor across three administrations.
The views expressed in this article are the writer’s own.
Source: https://www.newsweek.com/save-americas-youth-lawmakers-should-invest-drug-prevention-opinion-2071582
by Drug Free America Foundation <hhorning> 10 April 2025 15:45
|
The Food and Drug Administration warned a California cannabis company on Monday that its injectable hemp CBD could be posing “serious harm” to public health, telling the company that its product is violating federal law.
The FDA, however, warned Pico IV in a Monday letter that it is breaking the law by marketing CBD as a “dietary supplement,” even though it is explicitly designed to not be ingested and instead be injected. The agency also said the product is “especially concerning” because injectable drugs “can pose risks of serious harm to users.” The FDA said injecting anything directly into a person’s bloodstream can “lead to serious and life-threatening conditions.”
Pico IV CEO Joe Young said in an emailed statement to SFGATE that “public safety is our top priority” and that the company’s product undergoes a process “designed to ensure sterility and safety.”
“We are confident in the safety profile of our product and are working diligently to provide the FDA with the necessary information to resolve their concerns,” Young’s statement said.
Pico IV’s website states that it offers the world’s first injectable CBD product. The product is produced from American-grown hemp plants, a legal category for some cannabis plants, and is “completely sterile and safe for intravenous use.” It is not available for regular retail sale; only “physicians, providers, and IV therapy clinics” can purchase vials of the injectable CBD, according to the company’s website.
Toxicologists have long been concerned about cannabis products because they do not face rigorous federal safety standards. Cannabis products are also at a higher risk of being contaminated with heavy metals and pesticides. Pico IV says on its website that all of its products are tested by third-party labs for purity.
|
Vern Pierson is the district attorney of El Dorado County and was a co-sponsor of Proposition 36. He is a past president of the California District Attorneys Association.

California’s drug crisis has only escalated, with so-called “compassionate solutions” like harm reduction and past policies that decriminalized hard drugs making things worse.
Many drug addicts in the state have essentially faced two stark choices: homelessness or incarceration. This false dichotomy has normalized substance abuse, endangered public safety and failed to address the root causes of both homelessness and addiction.
In response, California voters last fall overwhelmingly passed Proposition 36, a third option that prioritizes rehabilitation over incarceration and offers a clear path to recovery, helping break the cycle of addiction and homelessness.
Programs like syringe exchanges, for example, have fallen short in addressing addiction itself. While well-intentioned, these programs have led to unintended consequences, including public spaces littered with used needles, increased health risks and the normalization of drug use. While syringe exchanges help reduce disease transmission, they don’t always guarantee that people enroll in treatment programs, and research shows they can even increase mortality rates.
The scale of this problem is stark. In 2021 alone, nearly 11,000 Californians died from drug overdoses, with over two-thirds involving opioids like fentanyl. Each of these lives lost represents a missed opportunity for intervention and recovery. Prop. 36 has given the state a framework to address this crisis by requiring treatment and rehabilitation for people struggling with addiction. This approach has the potential to reduce recidivism, save lives and help people reclaim their futures.
Source: https://calmatters.org/commentary/2025/01/addiction-homelessness-crisis-proposition-36/
by David Evans, Senior Counsel, CIVEL (USA)
January12, 2025
Article forwarded by Hershel Baker, Drug Free Australia. He opens by saying: “Please find evidence below on a current project to make the marijuana industry legally accountable to their victims in the U.S. if they are SUCCESSFUL, it will become very useful to Victims in many other countries including Australia.”
Legal Primer – Cannabis Industry Victims Educating Litigators (CIVEL) <https://www.civel.org/legalprimer>
The marijuana industry referred to here are those who illegally, negligently or fraudulently produce, market, or distribute marijuana products including those that have not been approved by the FDA or approved under federal law.
Today’s marijuana products can be high in potency and can reach 99% THC.
These products can be very destructive and cause addiction, mental illness, violence, crime, DUIs and many health and social problems. Young people are particularly vulnerable. We must protect them.
A first step is to educate lawyers and the community by providing legal and scientific guidelines for litigators so they can take the marijuana industry to court. We have produced six litigator guidelines:
We will arm the legal profession to recognize cases, prepare them and then litigate as was done in the cases against big tobacco and is now being done against the opiate companies.
We will not conduct litigation. Our goal is to get the legal profession to initiate litigation by educating them as to the legal issues and strategies involved. We also plan to educate the public about how the marijuana industry has destroyed lives and families and to support the victims.
For more information contact Senior Counsel, David G. Evans, Esq.
Email: seniorcounsel@civel.org <mailto:seniorcounsel@civel.org>
Please see our legal primer on marijuana and federal law
LEGAL PRIMER <https://www.civel.org/s/LEGALPRIMERCSA2017.pdf>
Other Important Documents
* CATEGORIES OF THE VICTIMS OF THE MARIJUANA INDUSTRY
<https://www.civel.org/list-of-marijuana-industry-victims>
* MARIJUANA AS A MEDICINE – POLICY, SIDE EFFECTS, SPECIFIC ILLNESSES
<https://www.civel.org/s/2CIVELMARIJUANA-AS-A-MEDICINE-POLICY-SIDE-EFFECTS-S
PECIFIC-ILLNESSES.pdf>
* THE FAILURES OF THE STATES TO REGULATE MARIJUANA
<https://www.civel.org/s/THE-FAILURES-OF-THE-STATES-TO-REGULATE-MARIJUANA-ST
UDIES-SHOW-THAT-MARIJUANA-PRODUCTS-HAVE-HIGH-LEVE.pdf>
* INTERACTIONS BETWEEN MARIJUANA AND OTHER DRUGS
<https://www.civel.org/s/4-CIVELINTERACTIONS-BETWEEN-MARIJUANA-AND-OTHER-DRU
GS.pdf>
* MARIJUANA AND VIOLENCE
<https://www.civel.org/s/5CIVELMARIJUANA-AND-VIOLENCE.pdf>
* MARIJUANA USE AND MENTAL ILLNESS AND BRAIN DAMAGE
<https://www.civel.org/s/6CIVELMARIJUANA-USE-AND-MENTAL-ILLNESS-AND-BRAIN-DA
MAGE.pdf>
* MARIJUANA USE AND DAMAGE TO HUMAN REPRODUCTION
<https://www.civel.org/s/7CIVEL-MARIJUANA-USE-AND-DAMAGE-TO-HUMAN-REPRODUCTI
ON.pdf>
* CONCERNS ABOUT CBD
<https://www.civel.org/s/8CIVEL-CONCERNS-ABOUT-CBD.pdf>
DISCLAIMER OF LEGAL ADVICE
This should not be considered legal advice. This is for informational purposes only. Use of and access to these materials does not in itself create an attorney – client relationship between David G. Evans or CIVEL and the user or reader. Mr. Evans or CIVEL cannot vouch for any study cited herein since they did not do the study. The readers should consult the study and make their own interpretation as to its accuracy. Please also be advised that case law and statutory and regulatory laws cited herein may have been amended or changed by the time you read this.
David G. Evans, Esq. – Senior Counsel – Cannabis Industry Victims Educating Litigators (CIVEL) (USA)
Source: Email by Herschel Baker <hmbaker1938@hotmail.com> Sent: 11 January 2025 23:06
Most Mondays, the Sixth Street entertainment district would be quietly nursing the hangover from another rowdy weekend, the only souls on the street those who sleep in the shelters, alleys, and sidewalks. But emergency dispatchers were getting repeated reports of people in distress.
The first call came in just after 9 a.m. from someone calmly describing an overdose in an alley. But, as the minutes dragged on, panic crept into the caller’s voice. “I’m scared,” she blurted out. “Oh, my gosh, I’m so fucking scared. Somebody’s going to die because of these people.”
“What happened?” asked the operator.
“Somebody tried to say ‘Don’t call the ambulance,’” the caller responded. “Oh, my God. Oh, my God.”
A little before 10 a.m., a security guard flagged down one of the Austin police officers flooding the district. Two men were sitting on the ground next to a trash bin in an alley near Sixth and Red River Street, slumped forward. Only 20 minutes earlier, both men had been walking and chatting. Now, they weren’t breathing.
The officer administered naloxone and began performing CPR. Paramedics took one to a hospital. The other, 51-year-old Benjamin Arzo Gordon, couldn’t be revived.
The alley where Gordon died had become the epicenter of a mass casualty event. During a two-hour span that Monday morning, at least six others overdosed and were revived with naloxone in a four-block radius in downtown Austin. Over 72 hours, Austin police reported more than 70 overdose calls. Records from Travis County, which includes most of Austin, and neighboring Williamson County indicate that as many as 12 may have died. The culprit: a bad batch of crack cocaine.
Through dozens of open records requests and interviews, the Texas Observer and Texas Community Health News have pieced together what happened during those deadly days—and how changes to state law might have saved lives. Across the capital city, people who consume crack, a stimulant, were suffering symptoms consistent with poisoning from opioids like heroin or fentanyl, the incredibly potent prescription painkiller.
The adulterated crack impacted Central Texans from many walks of life. Among the people who died were a construction worker from Honduras and a young man from Wimberley, who passed away in his parked truck with the engine running. Crack rocks found at the scene of some of the deaths tested positive for fentanyl.
A small, inexpensive item might have averted some of these deaths. Fentanyl testing strips can be used to check for the presence of the synthetic opioid. With an appearance similar to an at-home COVID-19 test, the strips are dipped in water in which a small amount of the drug has been dissolved. A line indicates if fentanyl is present.
But such testing strips are illegal in Texas. They’re considered paraphernalia, and possessing one is a Class C misdemeanor. While the Texas House passed a bill that would have legalized them in 2023, the Senate declined to vote on it.
In general, Texas has been reluctant to embrace the strategy of harm reduction, a broadly defined term for helping people who use drugs without stigmatizing or imposing strict parameters, while also involving drug users in planning and implementation. Harm reduction has been promoted in the United States since at least the 1980s. A classic early example is teaching people who inject drugs to clean needles with bleach, preventing the spread of HIV. The overall approach is sometimes pitched as a means to keep people alive long enough to get off drugs, but many practitioners simply seek to keep substance users safe and healthy, regardless of plans to enter treatment.
Under the administration of President Joe Biden, the federal government embraced aspects of harm reduction. Some states have as well. But policies favored by many Texas officials reflect the singular goal of making it as difficult as possible to use drugs. As it turns out, research and interviews with both experts and users of drugs show, making drug use more difficult also makes it more dangerous. Though Texas ranks low among states in fatal overdose rates, federal data shows the Lone Star State’s rate stayed nearly flat from 2023 to 2024, while overdose deaths fell significantly nationwide.
In recent months, top Texas officials have not only rejected harm reduction but have also openly antagonized those who practice it.
The prevailing attitude in the state is, “Why should we try and save their lives? They’re just going to use again,” said Joy Rucker, a nationally known advocate who launched Texas’ largest harm reduction nonprofit. In California, where she used to work, harm reduction organizations get robust public funding and operate openly.
“Texas was just a rude awakening,” she said.
A tall, thin Houston native with a quick sense of humor, Benjamin Arzo Gordon had been living on the streets of Austin for years. A January 2024 photo in the Austin American-Statesman shows him with a close-cropped white beard and a gray beanie, at Central Presbyterian Church downtown, looking pensive as he discusses harsh winter weather.
Andi Brauer, who oversees the church’s homeless outreach programs, said Gordon was a regular at weekly free breakfasts, cracking jokes with her and other volunteers and taking a genuine interest in her wellbeing.
“He’d always say, ‘You need to sit down and eat,’” Brauer recalled. “Or, if somebody was sometimes threatening or rude to me, he would say, ‘Don’t mess with Andi.’” She once printed out a photo of the two of them and used it to make a card for him.
In the alley where he died, Gordon was known to stop by with meals from the nearby food truck where he worked. “He used to help people in the alley,” said Loretta, a 55-year-old Austinite who herself suffered an overdose after Gordon.
Bokhee Chun, a Central Presbyterian volunteer, remembered Gordon would sing her hymns. Some months before he passed, Brauer said, Gordon came in to fill out a volunteer application.
Like many who died last April, Gordon was an experienced drug user. His drug of choice, crack, put him at little risk of sudden death by itself. But the crack he smoked that spring day was laced with a substance that has become synonymous with America’s failed drug policies.
Initially, fentanyl was used alone or to boost the potency of other opioids and depressants like heroin and prescription pain pills. But, in recent years, people killed by fentanyl are increasingly found to have stimulants like cocaine or methamphetamine in their systems. Explanations for this vary. Stimulants may be intentionally adulterated to hook users on fentanyl. A stimulant user might take opioids to come down. An unsophisticated dealer with a small stimulant supply may add fentanyl to stretch it. And failure to clean scales or surfaces can also mix fentanyl with another drug.
In Texas, overdose rates increased dramatically starting in 2020. From June 2023 to June 2024, more than 5,000 people died of an overdose in the state, with Travis County recording the highest fentanyl-related death rate among Texas’ most populous counties in recent years. Though Texas has one of the lower overdose rates in the nation, deaths in the state declined by less than 3 percent from 2023 to 2024, while the rest of the nation saw a drop of nearly 15 percent, per the federal Centers for Disease Control and Prevention. In October, the Texas Department of Health and Human Services (HHS) announced that it recorded a 13-percent drop in the state over the same period—but its figures include only those overdoses deemed accidental, not those labeled intentional, suicide, or of undetermined cause.
Experts also question the general accuracy of Texas’ numbers. In much of the state, underfunded and under-trained justices of the peace are charged with death investigations. Overdoses, which require costly autopsies and toxicology reports, are easy to overlook.
In response to the overdose increase, HHS in 2017 launched the Texas Targeted Opioid Response (TTOR) initiative. HHS is also part of a state awareness campaign using billboards and social media ads focused on cautionary tales of young Texans who overdosed. At the same time, state leaders have doubled down on criminalization.
In 2023, the Legislature passed a law allowing prosecutors to bring murder charges in fentanyl overdose cases. Critics say this discourages people from reporting emergencies, and research shows such laws harm public health. Some who overdosed in Austin last April had shared drugs, putting survivors at risk of being charged. In 2021, the Legislature passed a good samaritan law ostensibly meant to protect people who call 911 to report an overdose. The law created a defense for people arrested for low-level possession, but it has so many caveats—you can only use it once in your life, it doesn’t apply if you’ve been convicted of a drug-related felony, you can’t use it if you’ve reported another overdose in the last 18 months—that you’d need a flow chart to understand it. Critics say the statute’s of little use.
“The fentanyl-induced or the drug-induced homicide laws, that jacks up the consequences and the intensity so much more,” said Alex White, director of services at the Texas Harm Reduction Alliance, an Austin non-profit that does street outreach, operates a drop-in center, and provides supplies including for hygiene and wound care.
Some states, like Maryland and Vermont, make a point of prioritizing input from people who use or have used drugs while crafting policy. Harm reduction advocates say this is lacking in Texas, though HHS does have a low-profile advisory committee that is required to include members who’ve received mental health or addiction treatment.
“If you’re thinking that you know how to serve folks, and you don’t have those folks at the table when you’re trying to serve them, it’s not going to work,” said Stephen Murray, a paramedic and overdose survivor on Massachusetts’ Harm Reduction Advisory Council.
Rapid changes in the drug supply can make it difficult to conclusively track policy impacts. Critics blame Texas’ persistent overdose rate at least partly on punitive laws, but a few western states including liberal Oregon—which famously passed a drug decriminalization ballot measure in 2020—actually saw overdoses increase between 2023 and 2024. To this, some experts and at least one study counter that fentanyl’s delayed arrival on the West Coast has distorted the death rates, and that Oregon specifically did not implement sufficient services alongside decriminalization.
Texas Governor Greg Abbott’s office did not respond to a request for comment for this story.
Loretta woke up on the morning of Monday, April 29, in the alley where she often goes to smoke crack and sometimes spends the night. She grew up in East Austin, only blocks away.
Loretta said she lent her pipe that morning to a friend who’d just purchased drugs. Then she heard someone ask, “What’s wrong?” and saw the friend staring up, trance-like.
“He stayed looking at the sky,” Loretta said, reclining and rolling back her eyes to demonstrate. “The next thing I know he just went like this,” she said, as she pantomimed slumping limply to the side. “I was shaking him, and I said, ‘What’s wrong, what’s wrong?’ And after that he just didn’t answer.”
Despite fear she’d be held responsible, Loretta yelled to a friend to call 911. Police and paramedics swarmed the area. Loretta watched as someone else collapsed. “She hurt herself hard on the concrete and I said, ‘Oh, my God, hell no, this is not happening.’”
Soon, an acquaintance ran up to say Loretta’s boyfriend had also collapsed in a nearby portable toilet. “He was slurring like a baby, like a little boy,” Loretta said. “He started to lose consciousness. I slapped him hard. It hurt my hand. And I shook him and I started praying.”
Around the time that Loretta was calling out for help for her boyfriend, and EMTs were trying unsuccessfully to save Gordon, Adam Balboa showed up to work at an Austin-Travis County EMS (ATCEMS) station in south Austin. A case manager for a unit focused on substance use, Balboa heard the overdose reports and symptoms being described and knew what would save the most lives. “We needed to flood the downtown area with as much Narcan as possible,” he said.
Opioids in the bloodstream bind to receptors in the brain, creating euphoria. But by a quirk of physiology, excessive opioids bound to those receptors interfere with the body’s ability to measure its need for oxygen, slowing breathing—to the point where it can be fatal. Mouth-to-mouth resuscitation can keep someone alive. Narcan temporarily blocks the receptors to opioids, essentially short-circuiting an overdose if delivered in time.
The medics and police officers in downtown Austin were running out of naloxone, but Balboa didn’t just want to get them more. He also wanted to get it in the hands of people who use drugs, along with their friends, family, and neighbors. So he and colleagues began throwing together kits containing Narcan, a CPR mask, and instructions, and he hurried downtown with his SUV loaded up with the blue zippered pouches. “Everybody was super receptive,” he said. “They were clipping it to their belts and … going about their normal business.”
As common-sense as that response seems, it’s one strongly associated with harm reduction. By handing out naloxone downtown, Balboa was helping those most vulnerable to the tainted drugs help one another. It’s also a response that would have been impossible a few years ago.
Balboa’s unit is the brainchild of Mike Sasser, a 51-year-old ATCEMS captain who’s been in recovery for 21 years. A longtime paramedic who often worked with Austin’s unhoused population, Sasser became friends in 2018 with Mark Kinzly, a lion of the Texas harm reduction movement. Kinzly, who passed away in 2022, had helped start the Texas Overdose Naloxone Initiative, which was getting grants to distribute the medication. He had a seemingly simple idea for Sasser: ATCEMS could use grant money to buy Narcan, pass it out, and train people how to use it.
“My mind was blown,” Sasser said. “Why have I never thought about this? That would save so many lives.”
ATCEMS doctors then wrote prescriptions that allowed medics to hand out naloxone (today, it’s available over the counter). Sasser’s unit also began reaching out directly to overdose survivors and administering a maintenance drug that reduces opioid cravings, and it now includes two full-time case managers who run an overdose reversal education program called Breathe Now.
All of this fits under the philosophy of harm reduction, which can also include teaching people to use drugs more safely and providing supplies like clean glass pipes, which help prevent disease and infection. Providing food, water, hygiene products, or wound care to people who feel stigmatized in doctor’s offices is another tenet.
“We want to provide people with what they need, so we can build that trust,” said Em Gray, whose NICE Project provides supplies to Austinites, many of them unhoused, and stocks Narcan vending machines. “That’s how we show that we are there for them; we’re there to improve their quality of life, there to reduce their overdose death rates.”
There’s little funding available in Texas for the nonprofits and mutual aid groups that do this work. Across the state, harm reductionists often operate out of backpacks or car trunks.
To the state’s credit, Texas has taken some steps to increase naloxone distribution. TTOR does this with an annual federal grant of about $5.5 million. In 2019, TTOR, whose Narcan distribution program is administered by the University of Texas Health Science Center at San Antonio, gave about 40 percent of its naloxone to law enforcement agencies—even as research shows it’s more effective to give the medication to laypeople, who are typically first on the scene and present no threat of arrest—an analysis by Texas Community Health News found. By 2022, TTOR’s emphasis had shifted, with law enforcement making up only about 15 percent of its distribution.
But police are still prioritized in Texas’ long-term naloxone plan. Under a different state program started in April 2023, the Texas Department of Emergency Management (TDEM) began distributing $75 million worth of the medication over 10 years. That naloxone, donated by a pharmaceutical company as part of a court settlement over opioid deaths, is largely earmarked for first responders. Of the more than 150,000 doses that TDEM distributed from April 2023 to September 2024, 118,000 went to law enforcement agencies, mostly sheriff’s offices. Many of these offices cover areas that lack other harm reduction infrastructure, but records provided by TDEM show sheriffs aren’t using the naloxone. Of 13 counties in which agencies reported using doses from TDEM by September, the highest rate of use was 3 percent. Much of that naloxone will expire later this year. In an email, a TDEM spokesperson said the agency had “yet to turn down a request for naloxone” and that “Administration or disposition of distributed naloxone is up to the receiving entity how they see fit, in accordance with manufacturer’s guidance.”
When it set the state’s two-year budget in 2023, the Legislature allocated an additional $18 million in opioid settlement funds to UT Health San Antonio, but it’s not clear the appropriation will be renewed.
In the meantime, harm reductionists rely on a patchwork of naloxone sources, including local governments.
“Had we not saturated Austin with Narcan leading up to [the April] event, then that event would have been a lot more detrimental than it was,” said Sarah Cheatham, a peer support specialist with The Other Ones Foundation, an Austin nonprofit serving the unhoused. “Even when it was hard to get in our hands, we were out there doing this communication for months before this happened.”
By late morning on April 29, the Austin Police Department (APD) had some idea what was happening. Crack rocks and pipes had been found at the scene of a number of overdoses in an area known for its use, and officers had interviewed some who’d been revived with naloxone. They began looking for people seen on surveillance cameras and suspected of selling the tainted crack. While responding to an overdose, detectives found one suspect standing in front of a tent, just a block from police headquarters.
While cops made arrests, harm reductionists tried frantically to figure out what was going on. A little after noon that Monday, Claire Zagorski, a graduate research assistant at the University of Texas at Austin who’s worked in harm reduction for years, messaged a group chat: “Austin folks there’s a bad batch downtown as of this AM. Not sure on specifics but it does respond to naloxone.”
Groups started handing out Narcan and warning the communities they serve, but without any official information from local governments. “We were really just kind of going in blind,” Cheatham said. “We were all talking to each other about, ‘Who’s going to these camps? Where is it happening? Is it happening downtown?’ And I was mainly reaching out to the people that I know.”
Research shows that, given the chance, drug users will reduce their risk of overdose—including by carrying naloxone, not using alone, or taking a small tester dose. But, lacking detailed information, harm reduction workers in Austin were constrained. “It’s distressing that the thing that got everyone activated was me being notified by a backchannel,” Zagorski said.
When local officials finally made public statements hours after the flood of 911 calls, they only addressed some questions. Whatever was killing people was responding to Narcan, officials said, in a news release and press conference. But they were vague about which drug was adulterated, and there was no mention of test strips.
“It was a very chaotic scene at first,” APD Lieutenant Patrick Eastlick told the Observer. “Something we can look at in the future is, if this happens again, that we reach out to these different groups where we can spread the word.”
Open conversations about drugs are difficult in a state where top elected officials are cracking down on services for people who use them. In late November, state Attorney General Ken Paxton filed a headline-grabbing lawsuit to shut down a homeless navigation center at a south Austin church. The suit specifically blames the Texas Harm Reduction Alliance’s needle exchange program for “the prevalence of drug paraphernalia, including used needles, littering the surrounding area.” Drug use around the church “fuels criminality, and creates an environment where nearby homes and businesses are at constant risk of theft,” the complaint states.
Critics say efforts like Paxton’s just push drug use out of sight, creating greater risk. “It sends the message to people who use drugs that they should hide it, they should be kept in the dark and in the closet,” said Aaron Ferguson of the Texas Drug User Health Union. “The closet is a very dangerous place for people who use drugs. It’s where overdoses happen. It’s where stadiums full of people die every year.”
At least two who died in the Austin overdose outbreak were found alone. Family members of at least two others who perished at home told police they didn’t know their loved one had used drugs that day.
How state officials talk about drug use, critics note, also suggests that only some lives matter. For example, in a 2023 legislative hearing, GOP state Senator Drew Springer—in a successful attempt to woo conservative support for requiring school districts to stock naloxone in middle and high schools—distinguished between different groups of Texas children. “I think the general public, when they hear ‘overdosing,’ they think ‘That’s just a druggie, and that’s a druggie kid’s problem,’” he said. “No, it’s your kid’s [problem], because he may be taking a Xanax or an Adderall” without knowing fentanyl was present.
Claudia Dambra, who runs Street Value, a drug user health organization in Houston, criticized messaging that condemns certain substance users. “All it’s doing is creating more separation,” she said. “It feels like this weird, forced social Darwinism. … It feels like they’re picking us off.”
In an email, an HHS spokesperson said the agency does not discriminate: “[HHS] substance use programs offer treatment and recovery support for people, regardless of substance use duration.”After the horror of watching her boyfriend taken away in an ambulance, Loretta wandered through downtown Austin. Near APD HQ, in the area where police had arrested their suspect earlier, she was offered crack that her friend insisted came from a reliable source. Stressed and scared, she took a hit.
“I started getting a headache right away, like oh, my God, I’ve got a migraine or something. And I started throwing up,” she said. “I said, ‘Call the police, I’m sick.’”
Loretta didn’t lose consciousness, but she was vomiting as police questioned her. Eventually, she was taken to a hospital. She would be among the survivors.
Today, Loretta says that she gets test strips from harm reduction organizations, which quietly distribute them despite state law, and she gives them to friends. But, at the time, she knew little about them. Organizations that distribute strips generally can’t use grant money for their purchase, and government agencies, like ATCEMS, don’t distribute them.
Back in 2023, it seemed Texas was poised to legalize the strips. Before that year’s legislative session, Abbott said he supported allowing the tests, and legislators in both chambers introduced bills to legalize equipment for checking a range of drugs. One by Houston-area Republican Tom Oliverson, which was limited to fentanyl strips only, sailed through the House.
Oliverson, an anesthesiologist who has prescribed fentanyl to patients, said he’d heard from family members of people who purchased black-market pills without knowing they included the powerful opioid.
“That’s literally like stepping on a landmine,” Oliverson told the Observer. “You heard a click and the next thing you know, you were gone. Nothing you could have done could have saved you. You didn’t know it was there, right? Except for the fact that there are test strips.”
The bill received tepid support from harm reductionists, who were frustrated by its narrowness. The drug supply is constantly changing: Today, the dangerous veterinary tranquilizer xylazine is increasingly used to supplement other drugs. “We’re really trying to craft language that’s inclusive,” said Cate Graziani, former head of the Texas Harm Reduction Alliance and current co-director of a spinoff advocacy group, Vocal TX. “We don’t want to go back to the Legislature every time we have a new overdose prevention tool.”
Oliverson said the bill only applied to fentanyl “because it is that much more dangerous, because it is that much more powerful. … People say to me, ‘I don’t like the idea of giving people test strips because it gives them confidence in the illegal drugs that they’re buying, and I want to discourage people from using illegal drugs,’” he said. “Well, I want to discourage people from using illegal drugs too, but having them insta-killed by a mislabeled pill that they bought, the first time they took it, is not an effective strategy for recovery.”
While other drug-checking legislation failed that session, Oliverson’s bill passed the House 143-2—but it never received a hearing in the Senate Criminal Justice Committee. “They just could not get over the idea that you are making it safer for people to use illegal drugs and that we shouldn’t make it safe for people to use illegal drugs,” Oliverson said, “because they shouldn’t be using illegal drugs at all.”
Oliverson said he’ll introduce a similar bill this session and may rewrite it to include xylazine, but he made it clear he doesn’t support other harm reduction measures like needle exchanges. Such a bill will simply fizzle again, though, barring a change of heart in the Senate, which is run with an iron fist by Republican Lieutenant Governor Dan Patrick, whose office did not respond to arequest for comment for this article.
“It’s so demoralizing to live in a state where your elected leadership is so unwilling to do something so small as legalizing fentanyl test strips, because there’s so much stigma around drug users,” Graziani said.
By the afternoon of April 29, the tainted crack had made its way to south Austin. Loretta Mooney, another ATCEMS case manager in the substance use unit, was off work but rushed in. Dispatchers could see a new cluster of calls developing on Oltorf Street, east of Interstate 35.
By the time Mooney responded to her first call, at an apartment complex, medics had administered naloxone and revived a woman. Mooney handed out a few doses, then responded to another call from a fast food restaurant across the street. Someone had flagged down police, concerned about a man collapsed against the restaurant’s wall. Officers began CPR and administered Narcan. Mooney gave the man an additional dose and continued life-saving measures. Still, the 53-year-old died.
The situation was starting to look similar to downtown earlier in the day. Teenagers at another apartment complex began waving down Mooney and the officer. They ran over. Mooney administered naloxone to an unconscious woman and helped the officer deploy a breathing bag and mask. After a few minutes, the woman began breathing on her own again.
With Balboa now on his way to meet her and most of the calls near her covered, Mooney came to the same conclusion Balboa had that morning. “I was like, ‘Bring me all the Narcan you have and we’re going to start teaching these kids,’” she said.
On the lower level of a terraced parking lot, Mooney and the officer spread out naloxone kits and gathered the teenagers who had flagged them down.
“I’m telling the kid that came to get me specifically … ‘Because of you, this woman is alive,’” Mooney said. “We’re on the side of [the road] with, you know, ages 10 to 16, teaching them how to use Narcan.”
While Mooney and then Balboa, too, instructed people in the neighborhood how to use naloxone, a new crisis emerged. Some of the people who had bought the tainted crack were now behind the wheel. First responders were rushing to car wrecks and stalled vehicles.
Responding to the new calls, Mooney and Balboa saw the results of their impromptu training. As Balboa headed to a pawn shop where someone was overdosing, he got stopped in traffic. With his lights and sirens going, trying to weave through vehicles, he saw the teenagers they’d trained earlier.
“Before I can clear an intersection, they’d already sprinted over, pulled out a kit, and started giving Narcan,” he said. “Not only were they excited and ready to help and empowered to be able to do so, but when that opportunity finally came for them, they ran at it.”
As evening fell, the dying slowed. Behind closed doors, away from passersby armed with naloxone, however, it wasn’t through yet. A woman staying at a motel on Oltorf woke up during the night and called her 61-year-old husband, only to hear his phone ringing in the bathroom, then find him lying on the floor. The partner of a 57-year-old man got out of bed to get him warm milk after she noticed his nose bleeding, but, when she came back, he wasn’t breathing. A 36-year-old parked his truck in a lot in north Austin; when a security guard called 911 hours later, he was already dead. Around midnight, a son found his 63-year-old father deceased in an Oltorf apartment.
Later that same Tuesday, Loretta was released from the hospital. Downtown again, she found out her boyfriend had also survived and been released.
The following day, a man in southeast Austin woke up in the afternoon to find that a friend he’d let stay in his apartment had died while he slept. After agonizing for nearly two hours, he called the cops. That afternoon, a 34-year-old resident of Williamson County, just north of Austin, was found on the floor of his bedroom, where police found crack laced with fentanyl. Between April 28 and May 6, nine people in Travis County died from the toxic effects of fentanyl and cocaine, according to Travis County Medical Examiner records, in addition to the Williamson County death. At the request of APD, the Travis medical examiner withheld the cause of death in two other fatal overdoses that may have been related.
In the aftermath, APD made a handful of arrests. In some cases, police affidavits show, detectives were following information about who may have sold the tainted crack; in others, undercover officers simply went to known drug markets and arrested anyone who would sell to them. Eastlick, the APD lieutenant, said investigators believe the crack was adulterated at the local level, not higher up the drug supply chain, but that police had been unable to prove anyone intentionally sold tainted drugs. “It was a short surge … so our thinking is that it was not intentional,” he said.
As the tainted substance faded from the Austin drug supply, Cheatham said she and others heard stories of people who overdosed and were revived by naloxone without the authorities ever being alerted. In Austin’s camps and alleys, anonymous drug users helped one another.
Many of those who died remained anonymous as well, victims of an event whose details remained unclear and which took its toll mostly on the sort of people society tends to lose in its cracks.
Brauer and Chun, with the Central Presbyterian church, didn’t learn of Benjamin Arzo Gordon’s death until months afterward, when contacted for this story. In early November, the pair traveled to the indigent burial cemetery in northeast Travis County. In the wide, level graveyard, rows of nondescript markers rested flush to the ground. By Gordon’s, they left a bouquet of artificial flowers and a potted plastic plant.
“Just being able to picture him so clearly, knowing him as somebody that I value, that I enjoyed seeing, that was full of life and laughter despite the situation he was in—to hear about the way that he died of a drug overdose, probably fairly anonymously, just was incredibly sad to me,” Brauer said. “So because I didn’t get a chance to say goodbye … it just felt like something we needed to do to honor him.”
Editor’s Note: This article was produced in collaboration with Texas Community Health News and Public Health Watch. Daniel Carter contributed reporting.
Source: https://www.texasstandard.org/stories/texas-war-on-drug-users-fentanyl-overdoses-narcan-austin/
Ketamine could be upgraded to a Class A drug as the government seeks expert advice on its classification, the Home Office has said.
Illegal use of the drug has reached record levels in recent years, with an estimated 269,000 people aged 16-59 reporting ketamine use in the year ending March 2024.
Increasing ketamine’s classification would bring it in line with drugs including cocaine, heroin and ecstasy (MDMA) and mean up to life in prison for supply and production.
The policing minister will ask the Advisory Council on the Misuse of Drugs whether its classification should be changed and “carefully consider” its findings.
Ketamine can cause serious health problems including irreversible damage to the bladder and kidneys.
It is also one of the most detected drugs in incidents of spiking.
While commonly used on animals and in healthcare settings, ketamine is also thought of as a party drug due to its hallucinogenic effects.
An estimated 299,000 people aged 16-59 reported ketamine use in the year ending March 2023 – the highest on record.
Ketamine was upgraded from a Class C substance in 2014 due to mounting evidence over its physical and psychological dangers.
Currently, the maximum penalty for producing and supplying ketamine is up to 14 years in prison. Possession can carry up to five years in prison, an unlimited fine, or both.
Should it be upgraded to a Class A drug, supply and production of it could carry up to life in prison,, external while possession could carry up to seven years in prison, an unlimited fine, or both.
A coroner’s prevention of future deaths report called for action over the drug’s classification, after a man died from sepsis caused by a kidney infection that was “a complication of long-term use of ketamine”.
Greater Manchester South senior coroner Alison Mutch noted that James Boland, 38, started taking the drug as he believed it to be “less harmful” than Class A drugs.
She wrote , externalin November: “Maintaining its classification as a Class B drug was likely to encourage others to start to use it or continue to use it under the false impression it is “safer”.”
Policing minister Dame Diana Johnson has pledged to “work across health, policing and wider public services to drive down drug use and stop those who profit from its supply.
“It is vital we are responding to all the latest evidence and advice to ensure people’s safety and we will carefully consider the ACMD’s recommendations before making any decision.”
The findings are still valid as to why marijuana should not be rescheduled as determined in the Denial of Petition To Initiate Proceedings To Reschedule Marijuana, by the Drug Enforcement Administration (DEA), 81 FR 53767-01(August 12, 2016)
Human Physiological and Psychological Effects of Marijuana
MARIJUANA AND MENTAL ILLNESS
Recent studies show a connection between marijuana use and mental illness. In 2017, the National Academy of Sciences (NAS) concluded after a review of over 10,000 peer-reviewed academic articles, that marijuana use is connected to mental health issues (like psychosis, social anxiety, and thoughts of suicide). [1]
A study discussed in an October 2017 Scientific American shows that people who had consumed marijuana before age 18 developed schizophrenia approximately 10 years earlier than others. The more marijuana you take – and the higher the potency – the greater the risk. [2]
A November 2017 report on a study found that marijuana use in youth is linked to bipolar symptoms in young adults. [3]
References
[1] Health Effects of Cannabis and Cannabinoids: Current State of Evidence and Recommendations for Research.
http://nationalacademies.org/hmd/~/media/Files/Report%20Files/2017/Cannabis-Health-Effects/Cannabis-chapter-highlights.pdf
[3] http://www.newswise.com/articles/view/685947/?sc=dwtn November 2017
THERE IS A LINK BETWEEN MARIJUANA USE AND OPIATE USE
Marijuana use is associated with an increased risk for substance use disorders. [1] Marijuana use appears to increase rather than decrease the risk of developing nonmedical prescription opioid use and opioid use disorder. [2] In 2017, the National Academy of Sciences (NAS) landmark report written by top scientists concluded after a review of over 10,000 peer-reviewed academic articles, that marijuana use is connected to progression to and dependence on other drugs, including studies showing connections to heroin use. [3]
New research suggests that marijuana users may be more likely than nonusers to misuse prescription opioids and develop prescription opioid use disorder. The investigators analyzed data from more than 43,000 American adults. The respondents who reported past-year marijuana use had 2.2 times higher odds than nonusers of meeting diagnostic criteria for prescription opioid use disorder. They also had 2.6 times greater odds of initiating prescription opioid misuse. [4]
References
[1] JAMA Psychiatry. 2016 Apr;73(4):388-95. doi: 10.1001/jamapsychiatry.2015.3229.
Cannabis Use and Risk of Psychiatric Disorders: Prospective Evidence From a US National Longitudinal Study. Blanco C1, Hasin DS2, Wall MM2, Flórez-Salamanca L3, Hoertel N4, Wang S2, Kerridge BT2, Olfson M2. https://www.ncbi.nlm.nih.gov/pubmed/26886046
Cadoni C, Pisanu A, Solinas M, Acquas E, Di Chiara G. Behavioural sensitization after repeated exposure to Delta 9-tetrahydrocannabinol and cross-sensitization with morphine. Psychopharmacology (Berl). 2001;158(3):259-266. Available from: https://www.researchgate.net/publication/11640927_Behavioral_sensitization_after_repeated_exposure_to_D9-tetrahydrocannabinol_and_cross-sensitization_with_morphine
[2] Cannabis Use and Risk of Prescription Opioid Use Disorder in the United States, Mark Olfson, M.D., M.P.H., Melanie M. Wall, Ph.D., Shang-Min Liu, M.S., Carlos Blanco, M.D., Ph.D. Published online: September 26, 2017at: https://doi.org/10.1176/appi.ajp.2017.17040413
[3] Health Effects of Cannabis and Cannabinoids: Current State of Evidence and Recommendations for Research. See: http://nationalacademies.org/hmd/~/media/Files/Report%20Files/2017/Cannabis-Health-Effects/Cannabis-chapter-highlights.pdf
MARIJUANA USE BEFORE, DURING OR AFTER PREGNANCY CAN CAUSE SERIOUS MEDICAL CONDITIONS
Prenatal marijuana use has been linked with:
1. Developmental and neurological disorders and learning deficits in children.
3. Premature birth, miscarriage, stillbirth.
4. An increased likelihood of a person using marijuana as a young adult.
5. The American Medical Association states that marijuana use may be linked with low birth weight, premature birth, behavioral and other problems in young children.
6. Birth defects and childhood cancer.
7. Reproductive toxicity affecting spermatogenesis which is the process of the formation of male gamete including meiosis and formation of sperm cells.
References
Volkow ND, Compton WM, Wargo EM. The risks of marijuana use during pregnancy. JAMA. 2017;317(2):129-130.
https://www.drugabuse.gov/publications/research-reports/marijuana/letter-director
Source: Email from Dave Evans to Drug Watch International April 2018
WASHINGTON – Formal hearing proceedings regarding the proposed rescheduling of marijuana will begin on December 2, 2024 at 9:30 A.M. ET in the North Courtroom at DEA Headquarters located at 700 Army Navy Drive, Arlington, VA. This preliminary hearing will serve as a procedural day to address legal and logistical issues and discuss future dates for the evidentiary hearing on the merits. No witness testimony will be offered or received at this time.
In-person attendance is limited to designated participants and credentialed members of the media who have received confirmation of their in-person attendance.
WHAT: Commencement of formal hearing proceedings regarding the proposed rescheduling of Marijuana
WHO: Open to designated participants and designated credentialed members of the media.
WHEN: December 2, 2024 | 9:30 a.m. to 5 p.m.
WHERE: DEA Headquarters | 700 Army Navy Drive, Arlington, Va. 22202 | North Courtroom
FOR MEMBERS OF THE PUBLIC: Members of the public will have access to the court sessions virtually at www.DEA.gov/live.
FOR NEWS MEDIA: News media wishing to attend in person must RSVP to DEAPress@dea.gov by 10 a.m. on November 29, 2024. Due to limited capacity, RSVPs will be accepted on a first come, first served basis.
Designated members of the media should arrive no later than 9:00 a.m. on December 2 and follow all security screening procedures. Media credentials are required to be visible while inside DEA Headquarters. Video and audio recordings are not permitted at any time inside the courtroom.
Background:
On May 21, 2024, the Department of Justice proposed to transfer marijuana from schedule I of the Controlled Substances Act to schedule III of the CSA, consistent with the view of the Department of Health and Human Services that marijuana has a currently accepted medical use as well as HHS’s views about marijuana’s abuse potential and level of physical or psychological dependence. The CSA requires that such actions be made through formal rulemaking on the record after opportunity for a hearing. If the transfer to schedule III is finalized, the regulatory controls applicable to schedule III controlled substances would apply, as appropriate, along with existing marijuana-specific requirements and any additional controls that might be implemented, including those that might be implemented to meet U.S. treaty obligations. If marijuana is transferred into schedule III, the manufacture, distribution, dispensing, and possession of marijuana would remain subject to the applicable criminal prohibitions of the CSA. Any drugs containing a substance within the CSA’s definition of “marijuana” would also remain subject to the applicable prohibitions in the Federal Food, Drug, and Cosmetic Act. For more information, visit www.DEA.gov.
Source: https://www.dea.gov/stories/2024/2024-11/2024-11-26/dea-hold-hearing-rescheduling-marijuana
The martial language used by the government when presenting its plan to combat drug trafficking cannot mask the wide blind spots in its announcements, particularly in terms of health and social issues.
Gang warfare in a growing number of towns, repeated shootings punctuated by the deaths of ever-younger teenagers, drug traffickers with increased financial power and influence operating even from their prison cells… There can be little doubt that France, like other European countries, is grappling with the scourge of drugs on an unprecedented level. Criminal groups thrive on an illicit market estimated at over €3.5 billion, posing an ever-growing threat to the lives of entire neighborhoods, to public health and even to democracy.
There are, however, some grey areas surrounding this legislative measure, which is scheduled for parliamentary review in 2025, notably as regards the precise scope of the new prosecutor and the expansion of the current anti-drug office. As for the immediate measures announced on Friday, they remain imprecise, both in terms of the reinforcement of the Paris prosecutor’s office, to which a “coordination unit” would be attached, and the resources devoted to scrambling the telephone conversations of prisoners at the “top end” of the criminal spectrum, who would be assigned to specialized prison quarters.
But the martial language used by the two ministers to demonstrate their willingness to “join forces” over and above their political differences, cannot mask the blind spots in their announcements. Significantly, the health minister was not consulted. Information on addiction, risk reduction for drug users and providing care for people addicted to drugs are a few examples of these blind spots.
Cracking down on trafficking and putting pressure on the supply of illicit substances are essential, but they cannot be effective unless they are accompanied by strong action on demand and without a debate, informed by other countries, on the benefits and risks of partial decriminalization. At a time when consumption is becoming commonplace in many circles, from the most disadvantaged to the most privileged, public authorities should also strive to build and disseminate a counter-narrative to that of social ascent through trafficking.
A real “national cause,” the battle against drug trafficking requires France to build the conditions, if not for a consensus, at least for a political majority. This requires not only the addition of a strong preventive component but also that the government distances itself from the interior minister’s constant conflation of drugs and immigration.
Supporters of psilocybin expressed dismay at the bans after thousands of people reported benefits from using the psychedelic drug
Oregon Capital Chronicle, November 7, 2024- by Ben Botkin and Lynne Terry.

Image: PIXABAY
Voters in more than a dozen Oregon cities, including in the Portland area, voted to ban the regulated sales and use of psilocybin mushrooms.
Anti-psilocybin measures were on the ballots in 16 cities and unincorporated Clackamas County, and are passing in coastal communities to urban Portland and central and southern Oregon by 55% to 70% of the vote.
Bans against psilocybin businesses are passing in Brookings, Rogue River, Sutherlin, Redmond, Lebanon, Jefferson, Sheridan, Amity, Hubbard, Mount Angel, Estacada, Oregon City, Lake Oswego, Seaside and Warrenton. Redmond’s measure would enact a two-year moratorium on psilocybin businesses.
There was one notable outlier. The measure to ban psilocybin could fail in Nehalem, a small community in Tillamook County, according to initial returns. But it is failing by only three votes. The unofficial results on Wednesday were close: 80 voters oppose the ban and 77 voters support.
Comment was not immediately available from psilocybin opponents. Supporters of the drug expressed disappointment with the results Wednesday.
“I think it’s really unfortunate that local communities, often rural communities continue to prevent access to psilocybin services, especially given that we’ve seen over 7,000 people go through the Oregon program, and there’s been so many stories of healing and benefit for those who have done it,” said Sam Chapman, a longtime psilocybin advocate who is policy and development director for the Microdosing Collective, a nonprofit supporting use of the drug in small doses.
Chapman played a big role in getting Oregonians to approve licensed psilocybin treatment centers, facilitators and manufacturers with the passage of Measure 109 four years ago by 56% of the vote. The measure required the Oregon Health Authority to start a program to allow providers to administer psilocybin mushrooms and fungi products to people 21 or older.
To date, the health authority has licensed about 1,000 staff, including 350 facilitators who work directly with clinics while they’re on the hallucinogen. The agency has also licensed 30 psilocybin centers – from the Portland area to Eugene to Ashland and beyond – along with a dozen manufacturers and one lab.
Chapman said these centers give the state another “tool in the toolbox” to treat mental illness, especially depression, anxiety and PTSD, especially for veterans.
“We’re actually seeing the proof of concept for the people who are going through Oregon’s service centers now,” Chapman said. “I think the mental health crisis in rural communities is especially unique in that these rural communities are struggling not just for mental health but economically as well.”
The economy of the psilocybin industry has been soft, caused mainly by the cost of a single session, which can range from hundreds to several thousand dollars, with many customers flocking to Oregon from out of state.
Chapman said rejection of psilocybin is linked to a lack of education about the drug and how the industry works in Oregon. Consumers cannot buy the drug in stores, as they can for marijuana, and treatments are regulated.
“They don’t understand psilocybin. They don’t understand the research and they don’t understand the Oregon program. And so in addition to the lack of that understanding, they make some assumptions. The biggest assumption is that this is just the same thing as cannabis. They assume this is for retail sales, which is not true,” Chapman said.
Healing Advocacy Fund, a nonprofit in Oregon and Colorado, will continue to push for the programs to grow, with state-regulated access to psychedelic healing. Heidi Pendergast, the group’s Oregon director, said the rollout in Oregon has been safe, with only four people needing emergency services out of thousands served.
“So while there may be some concerns, we haven’t seen that play out right now whatsoever in the program,” Pendergast said.
Oregon was the first state to decriminalize psilocybin in licensed settings and Colorado has followed suit. Massachusetts voters rejected a proposal to legalize the mushrooms and allow people to grow small quantities at their homes, National Public Radio reported.
Oregon Capital Chronicle is part of States Newsroom, a nonprofit news network supported by grants and a coalition of donors as a 501c(3) public charity.
Source: The Lund Report – Latest Headlines | November 7, 2024
November 6, 2024 10:45 am
Voters in the 2024 election dealt a rebuke to drug legalization efforts in four states, a major political development that will shape the future of both marijuana and psychedelic drug policy across the country:
The legalization effort was dealt a decisive blow in mid-October by the Boston Globe, whose editorial board wrote that the measure “goes too far” despite the therapeutic promise of psychedelics for treating PTSD and other mental health conditions.
“Voters by wide margins rejected the legalization of drugs like marijuana and psychedelics from red Florida to blue Massachusetts,” Foundation for Drug Policy Solutions and Smart Approaches to Marijuana President Kevin Sabet said in a statement on the elections. “We expect this Administration to listen to this message loud and clear: More drugs are not good for any community.”
Nebraska medical marijuana is only victory
The two interrelated ballot initiatives for Nebraska were the only drug legalization amendments to pass on Tuesday night.
The Associated Press declared victory for the ballot measure to legalize medical marijuana, Initiative 437, 70.2%-29.3% with 99% of the votes counted as of 6:52 a.m.
The accompanying amendment, Initiative 438, which established the Nebraska Medical Cannabis Commission to regulate the medical marijuana program, passed with 67% of the vote, according to Ballotpedia. Results for Initiative 438 were not tracked by the Associated Press.
Nebraska is now one of 39 states that have legalized medical marijuana, which in the past has signaled that a recreational use policy will be introduced in the coming years.
Future of federal drug policy
Cannabis is still classified as a Schedule I drug under the Controlled Substances Act, along with heroin and ecstasy. Schedule I drugs are determined to have no accepted medical use and a high potential for abuse, and federal penalties for possession and intent to distribute can be severe.
President Joe Biden issued a directive to executive branch agencies in 2022 to begin a review of federal marijuana statutes. The Drug Enforcement Agency this spring started the process of reclassifying marijuana to a Schedule III substance, on par with ketamine and certain anabolic steroids.
Although it was not a major issue in the presidential campaigns, both Vice President Kamala Harris and President-Elect Donald Trump promised to continue with this spirit of drug reform at the federal level.
Trump, a resident of Florida, posted on Truth Social in September that he planned to vote in favor of Amendment 3 because he supported “smart regulations” for cannabis at the state level.
“As President, we will continue to focus on research to unlock the medical uses of marijuana to a Schedule 3 drug, and work with Congress to pass common sense laws, including safe banking for state authorized companies, and supporting states rights to pass marijuana laws, like in Florida, that work so well for their citizens,” Trump said in September.
Trump’s perspective on psychedelic drugs has not been as clear, but he has been a strong supporter of increasing access to clinical trials for experimental treatments for potentially fatal diseases.
Over the past two years, there has been strong bipartisan support in Congress for improving funding for the mental health benefits of psychedelic drug use for patients with severe PTSD, particularly combat veterans at risk of suicide.
Source: CLICK HERE TO READ MORE FROM THE WASHINGTON EXAMINER
November 6, 2024 by Our Reporter
This proposed strategy prioritizes reducing drug use while establishing a supportive legal framework to empower health interventions.
With roughly 14.4 percent of the population or about 14.3 million Nigerians, affected by drug use, public health experts argued that a comprehensive legal structure is critical for the Federal Ministry of Health to address this crisis effectively.
At a one-day media sensitization workshop in Abuja, themed ‘Public Health Approach to Drug Control Response in Nigeria’ and organized by the Federal Ministry of Health and Social Welfare in partnership with Youth Rise Nigeria, experts advocated for treating drug dependency as a health issue rather than a criminal offence.
They stressed that many individuals struggling with drug dependency are dealing with health-related challenges.
The workshop highlighted the urgent need for a health-oriented approach to tackle what experts now view as a national drug dependency epidemic and the crucial role of the media in shaping public perception and reaction to drug abuse.
Chukwuma Anyaike, the Director of Public Health at the Federal Ministry of Health, argued that a public health approach is crucial for controlling drug issues in Nigeria.
He noted that existing supply-focused measures have limited access to treatment and prevention services, which has led to increased rates of HIV, tuberculosis, and hepatitis among people who inject drugs.
Anyaike called for a multidisciplinary approach integrating public health, legal, and social welfare frameworks and urged Nigeria to align with international standards such as the World Health Organization’s guidelines, the 2016 UN General Assembly Special Session on Drugs UNGASS), and the African Union (AU) Plan of Action to improve its response to drug abuse.
“This approach includes preventing drug use, providing treatment and care for individuals with substance use disorders, implementing harm reduction strategies, and ensuring access to controlled medications,” Anyaike explained.
Echoing these sentiments, Nonso Maduka, a Consultant with Youth Rise Nigeria, stressed the need for legislation that would facilitate a health-centered response to drug control.
Maduka argued that a supportive legal framework would help provide better resources and care for individuals, families, and communities affected by drug dependency, shifting away from the current punitive focus.
“Unfortunately, we have an unbalanced approach that targets mainly supply reduction, and the health sector lacks the legal authority to address demand, prevention, treatment, and harm reduction,” Maduka noted.
He highlighted that Nigeria’s current drug laws treat drug use as a criminal issue, which restricts health interventions and puts more strain on affected communities.
A public health perspective, he noted, could help curb drug dependency and reduce associated health risks like HIV and hepatitis.
Maduka also emphasized the importance of empowering local health initiatives and granting States authority to address drug challenges in their communities.
A health-focused legal framework, he noted, would allow targeted responses, including treatment, rehabilitation, and palliative care.
Such a framework, according to him, would create a balanced approach that not only reduces drug abuse but also mitigates its harmful effects, ultimately supporting a healthier future for the nation.
“If you want to solve it, it must be driven by evidence,” Maduka added, calling for an evidence-based approach that balances criminal justice with health-focused interventions, which includes drug demand reduction, harm reduction, and access to necessary medications.
“Understanding underlying causes, such as pain management needs and rural challenges, is essential for developing compassionate and comprehensive responses,” he added.
Oluwafisayo Alao, the Executive Director of Youth Rise Nigeria, underscored the crucial role of the media in changing public perceptions around drug dependency, saying, “The way we approach substance use in Nigeria impacts the lives of millions of people.
“This media partnership is a vital step toward a compassionate, health-focused response. By creating a framework that prioritizes health over punishment, we aim to protect individuals, families, and communities”.
Source: https://thenationonlineng.net/experts-propose-all-inclusive-approach-legal-framework-to-combat-drug-abuse/
Counties will approach enforcement differently, providing yet another large-scale experiment in drug policy.
by Troy Brynelson|Oregon Public Broadcasting
October 17, 2024
Days after Oregon officially recriminalized drug possession, Douglas County Sheriff’s Deputy Ryan Gomez found himself helping with an arrest.
Officers in the town of Sutherlin stopped a car near a park, he recalled. They spotted fentanyl and methamphetamine inside. He and the officers arrested the man for misdemeanor drug possession.
Recriminalization went into effect Sept. 1. Before that date, drugs would have resulted in far less punishment. Officers would have ticketed the man.
“Now, there’s consequences to the actions,” Gomez said. “He has to face the judge and explain his actions.”
It may have been a different story for the man had he been stopped in a county deploying a new state program called “deflection.” It aims to get people criminally charged for possessing small amounts of drugs into treatment, in lieu of going to court.
Lawmakers over the summer offered counties state dollars in exchange for creating their own deflection programs. More than 20 counties applied, submitting plans that involved activities like establishing shelters and pairing police with substance use experts.
For example, a person in Multnomah County who has drugs, but no outstanding warrants, may be deflected away from the justice system. They go to treatment instead. A successful trip could result in the person never facing a criminal charge.
Other counties, like Douglas, didn’t apply at all.
What’s left is a patchwork of drug enforcement policies across the state. The contrasting approaches may look starkest at the border of Douglas and Lane counties. Both counties straddle Interstate 5 and are planning widely different approaches.
Lane County officials tell OPB they are planning a robust deflection program. Douglas County, on the other hand, plans to try policing illicit substances like the old days.
‘By golly, he‘s going to prosecute them’
In opting out of the state’s deflection program, Douglas County Sheriff John Hanlin is conscious that the county may look severe. He believes jail and the justice system can turn lives around.
To him, Measure 110, the voter-approved decriminalization of drugs in 2020, failed in its aim to improve drug users’ lives. He and his deputies had few means to get people into treatment without criminal charges looming over their heads.
“Don’t get me wrong; I believe treatment is an extremely important component to this drug problem that we’re dealing with,” Hanlin said. “Treatment works, but only if there are consequences that go along with that.”
While every deflection program will be different, criminal charges can still be leveled against a person if they don’t comply.
Hanlin noted that landing in jail for a drunken incident when he was a teenager proved a wakeup call. He also brought up his 31-year-old son’s ongoing addiction, which has led to a lengthy rap sheet of misdemeanors and felonies in Douglas County.
“If he got arrested and spent a day in jail and got out the next, that wasn’t even long enough for him to realize that he’d done anything wrong,” Hanlin said. Jail is “a necessity if you want to wake them up and get them to think, ‘You know what? I think this problem is getting out of hand.’”
Deputies made nine arrests in September under the new recriminalization statutes, according to a sheriff’s department spokesperson.
Overdose deaths have been rising. According to data from the Centers for Disease Control and Prevention, overdose deaths rose from 23 in 2020 to 43 in 2023. That’s less than 4 for every 10,000 people.
The sheriff, first elected in 2008, said it was a joint decision not to participate between himself, District Attorney Rick Wesenberg and the county’s Board of Commissioners. Wesenberg and the county commissioners did not respond to multiple requests for interviews.
Hanlin said he wanted to take a wait-and-see approach with deflection: Let other counties go first with their experiments. He added that the county worried about using one-time state grant dollars without assurances of ongoing funding.
He doubted empowering his deputies to enforce stricter penalties would lead to unintended consequences, such as crowding the jail.
“Most of these cases are going to be cite and release cases,” he said. “But the DA assures me that, by golly, he’s going to prosecute them.”
A drug user’s fate is then up to the courts, Hanlin said. Douglas County does offer diversion programs and a drug court that aim to soften punishment and help drug users get clean.
“I don’t think we can arrest our way out of the drug addiction problem,” Hanlin said. “But I know that, obviously, doing nothing isn’t going to cause the problem to go away either.”
‘A lot of folks just want to see people get help’
Crossing the county line north into Lane County, one will find a completely different approach. Officials there hope to get more people into treatment and keep them away from jail cells and courtrooms as much as possible.
Oregon gave Lane County $2.1 million to assist. That will help pay for housing, officials said, and for a team of substance use specialists, known as navigators, who work with police and decide if a person should be deflected.
Clint Riley, who is leading the program, said he has traveled to the county’s various police agencies to help train them on when to call a navigator.
“That’s a different training that most of us have never been to before,” Riley said. “Maybe five years ago, you would have taken this person to jail. Now, we’re using a different approach. So it’s crucial that the relationship between navigators and law enforcement is good.”
Law enforcement agencies seem to have bought in. Chris Parosa, the Lane County District Attorney, said officers are glad drug laws have more teeth yet they aren’t necessarily being asked to make many more arrests.
“That’s where the opportunity lies for them,” Parosa said. “Instead of having to – prior to ballot Measure 110 – have those people arrested, take them down to jail, fill out probable cause affidavits and immediately begin writing reports because that person is in custody, they can call out a person who is detached from the criminal justice system to take custody and control.”
Lane County is already home to one innovative first-responder program. CAHOOTS launched in the 1970s as one of the first-ever services dispatching mental health specialists through 9-1-1 to help people in crises.
Their deflection plans will effectively turn Riley and the navigator into case managers for low-level drug offenders. Parosa said the navigators will keep informing the county if people are actively pursuing treatment and not skirting responsibility.
“I’m not trained in the realm of substance abuse treatment,” Parosa said. “I’m a criminal attorney. It would be highly inappropriate for me as a criminal attorney to ultimately tell a substance abuse or behavioral health specialist how to do their job or what a person needs.”
Many of the navigators themselves will be ex-addicts, Riley said.
“Some law enforcement in our community might have arrested that navigator 15 years ago, when they were in that situation, and now they’ve completely changed their life,” he said. “They got help, got treatment, and now they’re working as a professional in our community with credentials.”
Lane County saw overdose deaths rise recently, too. From 2020 to 2023, deaths rose from 97 to 212, according to CDC figures. That’s about five-and-a-half deaths per 10,000 people.
The navigator program has not launched yet, according to Riley, but he envisions a system with wide latitude. A person facing criminal charges that aren’t inherently drug related – such as trespassing or theft, for example – may be able to get those charges deflected, too. The victim of a crime would have to agree, too.
“A lot of folks just want to see people get help, if they think it’s going to stop,” Riley said.
He doesn’t criticize counties like Douglas that are not participating in deflection. He acknowledged that many perceive Oregon’s drug decriminalization efforts to have failed. Another experiment can be daunting.
Riley formerly commanded the Lane County Sheriff’s Office jail. He said he saw firsthand that it was treatment, not jail in and of itself, that helped people. He said he helped launch new programs to get people medication and counseling.
“We started seeing people leave the jail in a better space, in a better place,” Riley said. “I’ve seen a lot of people spend a lot of time in jail and prison due to their addiction and, at some point, what stopped their addiction? For most people, they got treatment.”
Hanlin, the Douglas County Sheriff, said they are willing to learn from other counties if their programs succeed.
Source: This article was originally published by Oregon Public Broadcasting.
This is the opening of a submission by Dr Stuart Reece to the FDA relating to the re-scheduling of cannabis:
“I am very concerned about the potential for increased cannabis availability in USA implied by full drug legalization; however, a comprehensive and authoritative submission of the evidence would take weeks and months to prepare. Knowing what we know now and indeed, what has been available in the scientific literature for a growing number of years concerning a myriad of harmful effects of marijuana, marijuana containing THC should not be reclassified. These effects that are now well documented in the scientific literature include, alarmingly, harm involving reproductive function and birth anomalies as a result of exposure to or use of marijuana with THC.
In addition to all of the usual concerns which you will have heard from many sources including the following I have further particular concerns:
1) Effect on developing brains
2) Effect on driving
3) Effect as a Gateway drug to other drug use including the opioid epidemic
4) Effect on developmental trajectory and failure to attain normal adult goals(stable relationship, work, education)
5) Effect on IQ and IQ regression
6) Effect to increase numerous psychiatric and psychological disorders
7) Effect on respiratory system
8) Effect on reproductive system
9) Effect in relation to immunity and immunosuppression
10) Effect of now very concentrated forms of cannabis, THC and CBD which are widely available
11) Outdated epidemiological studies which apply only to the era before cannabis became so potent and so concentrated
These issues are all well covered by a rich recent literature including reviews from such major international authorities as Dr Nora Volkow Director of NIDA at NIH, Professor Wayne Hall and others “
The full text can be read here
Source: Letter from Dr Stuart Reece to FDA April 2018
With the increasing legalization of recreational marijuana across various states, employers need to proactively prepare for the changes and their implications on the workplace. As more states allow adults to legally purchase and possess marijuana, it’s essential for employers to review and update their workplace policies to ensure compliance and maintain a safe work environment.
Despite legalization, employers can still prohibit marijuana use that leads to impairment at work, akin to alcohol restrictions. Recent legal decisions, such as White v. Timken Gears & Servs., Inc. in Illinois, reinforce that a positive drug test for marijuana while working, even if used recreationally off-duty, can justify termination if it violates a reasonable and consistently applied workplace policy. This underscores the importance of clear, fair, and legally sound drug and alcohol policies to ensure workplace safety.
The increasing state legalization of recreational marijuana marks a significant change for employers. By proactively updating your drug testing protocols, policies, training programs, and communication strategies, you can effectively manage the impact of this new legislation on your workplace. Staying informed and prepared will help you navigate this evolving landscape while ensuring a safe and compliant work environment.
Sources:
Federal court rules employer did not violate Illinois privacy law for firing worker testing positive for cannabis. (2024, July 30). JD Supra. https://www.jdsupra.com/legalnews/federal-court-rules-employer-did-not-4849901/
NATIONAL DRUG-FREE WORKPLACE ALLIANCE
As the workplace division of Drug Free America Foundation, NDWA’s mission is to be a national leader in the drug-free workplace industry by directly assisting employers and stakeholders, providing drug-free workplace program resources and assistance, and supporting a national coalition of drug-free workplace service providers.
Source: www.ndwa.org
![]()
With the increasing legalization of recreational marijuana across various states, employers need to proactively prepare for the changes and their implications on the workplace. As more states allow adults to legally purchase and possess marijuana, it’s essential for employers to review and update their workplace policies to ensure compliance and maintain a safe work environment.
Despite legalization, employers can still prohibit marijuana use that leads to impairment at work, akin to alcohol restrictions. Recent legal decisions, such as White v. Timken Gears & Servs., Inc. in Illinois, reinforce that a positive drug test for marijuana while working, even if used recreationally off-duty, can justify termination if it violates a reasonable and consistently applied workplace policy. This underscores the importance of clear, fair, and legally sound drug and alcohol policies to ensure workplace safety.
The increasing state legalization of recreational marijuana marks a significant change for employers. By proactively updating your drug testing protocols, policies, training programs, and communication strategies, you can effectively manage the impact of this new legislation on your workplace. Staying informed and prepared will help you navigate this evolving landscape while ensuring a safe and compliant work environment.
Source:
PUBLISHED: June 30, 2024 at 6:00 a.m.
This month, Gov. Wes Moore pardoned more than 175,000 prior marijuana convictions, impacting more than 100,000 individuals. This comes 18 months after the Old Line State voted to legalize recreational marijuana, which went on sale exactly one year ago on July 1. While the pordons were a good move, the move was a too-little-too-late acknowledgement that marijuana legalization isn’t about social justice, and pot profiteers aren’t necessary to end the criminalization of small possession of marijuana.
Moore’s decision to pardon these prior marijuana convictions should be commended. The charges related to low-level possession and paraphernalia. He followed in the steps of President Joe Biden, who in 2022 pardoned federal convictions for the low-level possession of marijuana.
Moore called it “the most sweeping state level pardon in any state in American history.” Yet nobody will be released from prison, just as nobody was released from federal prison because of Biden’s pardons. The pardons in Maryland will also not expunge the criminal records of those with prior convictions.
These recent steps highlight the false dichotomy between the criminalization of marijuana and the legalization of today’s highly potent THC drugs. While nobody should be in jail for the use of marijuana, the alternative policy need not legalize dangerous psychoactive drugs and usher in a for-profit marijuana industry, as was done in Maryland. Removing criminal penalties could address concerns related to the criminal justice system, while not giving the marijuana industry free rein to do as it pleases.
Indeed, when polls ask voters about the specific policy they prefer for marijuana, they do not come out in support of a full-scale commercial industry. A national poll in 2022 from Emerson College found that only 38% of Americans prefer full legalization, with the remaining 62% majority favoring decriminalization of marijuana, or continued prohibition — among other options. Americans remain wary of legalization.
This trend is also playing out in Maryland, with some voters having second thoughts about legalization. According to a Washington Post/University of Maryland poll, only 31% of voters have a positive view of legalization. Notably, Black Marylanders were more likely to say it’s been bad than good, at 32% vs 28%, respectively. Opposition comes across party lines, with 63% of Democrats and 76% of Republicans saying legalization has not been good for the state.
The same poll also asked people whether they support allowing a dispensary to open in their community. Statewide, half of Marylanders opposed this proposition. In Prince George’s County specifically 59% of poll respondents opposed it. Voters recognize the difference between the harms of criminalization and the harms of the addiction-for-profit industry. Marylanders don’t want people in prison for marijuana, but they also don’t want pot shops in their neighborhood.
Moore’s pardons come amid calls for a shift in national marijuana policy. The Biden Administration is actively working to reclassify marijuana as a Schedule III substance, a move that would be a boon for the industry. Politicians should know better by now. They should know to distrust the industry and prioritize public health and public safety — they’ve gone through the same routine with the tobacco industry.
Despite promises that commercial pot sales would improve racial equity, we have seen that Black Americans continue to be disproportionately harmed, now by a predatory industry and its mind-altering products. Black Americans were 4x more like to have marijuana-related emergency department visits than white Americans. Additionally, in 2022, Black minors between the ages of 12 and 17 were 25% more likely to have used marijuana in the past month, compared to white minors and they were 31% more likely to have a cannabis use disorder. Pot shops are disproportionately concentrated in low-income communities and communities of color, helping to explain the concentration of these harms.
The marijuana industry uses arguments about racial equity as a guise to advance its financial interests. It’s a myth not supported by an honest assessment of the industry and its practices.
Moore’s actions are proof positive it is possible to advance racial equity without legalizing marijuana, a drug associated with numerous mental health harms, including anxiety, depression and schizophrenia. A good first step to protect Marylanders would be curbing public use, educating young people about the risks, requiring product labels with science-based warnings, and enacting strong regulations on the industry. The governor should turn his pulpit to these real concerns before more Marylanders get hurt.
Dr. Kevin Sabet (info@learnaboutsam.org) is the president of Smart Approaches to Marijuana (SAM), the nation’s leading nonpartisan voice for health and safety-based marijuana policy, and a three-time White House drug policy advisor.
In a dramatic example of government yielding to public opinion the Senate has introduced legislation to legalize cannabis on the federal level. Though passage before the November election is unlikely, this long overdue legislative action seeks to update a statute stemming [pun intended] from marijuana’s demonized image as depicted in the 1936 documentary film “Reefer Madness” and better reflect public opinion and liberal social trends. Currently, under the Federal Controlled Substances Act (CSA) of 1970, cannabis is considered to have “no accepted medical use” and a high potential for abuse and physical or psychological dependence. This Federal statute contrasts with the claims of therapeutic benefits of cannabis’ biochemical constituents such as cannabidiol and THC (tetra-hydro-cannabinol) when the sole FDA indication for their use is a rare childhood (Lennox-Gasteau) seizure disorder.
While the scientific information to officially endorse cannabis products as having therapeutic benefits is lacking, a recent Pew Research Center Survey found that 88 percent of Americans felt that marijuana should be legal for medical or recreational use. This wave of popular opinion has led to marijuana’s approval in 38 states for medical use, in 24 states for recreational use and decriminalization in an additional seven states.
Americans now have access to a recreational intoxicant that is arguably no more dangerous than alcohol or tobacco without fear of the disproportionately severe punishments previously meted out to those apprehended for possession and use. But at the same time, there are numerous inconsistencies and cross-purposes integral to the legalization and commercialization of cannabis products. The most obvious of these is the fact that Federal law considers the use, sale, and possession of cannabis illegal.
The consequence of the latter was not just that the exaggerated therapeutic claims were not born out by scientific research, but that it served as a “Trojan Horse” to galvanize public opinion and advance cannabis advocates ultimate goal of unfettered access. This came to fruition when the state legislatures of Colorado and Washington voted to legalize the commercial production and sale of cannabis products in 2012. This triggered a stunning demonstration of states’ rights in which a majority of states followed suit by liberalizing their cannabis laws despite Federal prohibitions.
In a glaring recent example of governmental missteps, on March 17, Gov. Kathy Hochul declared New York State’s commercialized cannabis licensing and distribution system “a disaster” and announced “a top-to-bottom review of the NYS Cannabis Control Board and its system for regulating legalized cannabis products.” The main purpose of the review was to process applications faster and enable more cannabis vendors to open. Just weeks before Hochul’s executive order which was intended to give New Yorkers greater access to cannabis, the American Heart Association had issued a warning on the higher risks of cardiovascular events associated with heavy cannabis use. This was based on a National Institutes of Health (NIH)-funded study of nearly 435,000 American adults reported last November which found that “Daily use of cannabis –– was associated with a 25% increased likelihood of heart attack and a 42% increased likelihood of stroke when compared to non-use of the drug.”
Such health hazards are not some abstract possibility or unconfirmed scientific speculation, but a growing current reality. As a practicing psychiatrist I have witnessed these effects first-hand as a burgeoning number of cannabis-induced medical and mental disturbances—particularly in young people—show up in our hospital emergency rooms and are referred to me for consultation. And while the rising numbers of adverse effects occurring in the wake of legislative reform are disturbing, they are not surprising. Rather, they were anticipated.
This was revealed in an NBC News report on states enacting legislation to legalize cannabis in April 2022: “We were not aware when we were voting [in 2012] that we were voting on anything but the plant,” said Dr. Beatriz Carlini, a research scientist at the University of Washington’s Addictions, Drug & Alcohol Institute. She has led the effort in Washington state to research high-potency pot and is now exploring policy options to limit access. Her team concluded in 2020 that “high-potency cannabis can have lifelong mental health consequences.”
So while possible therapeutic value has been the lever, tax revenue for states and profits for new industries—resulting from broad access—has clearly become the goal with unsuspecting users as the potential victims. This is the template now driving rapid legalization of a host of previously prohibited recreational drugs including MDMA (ecstasy) and psychedelics.
Source: https://time.com/6973962/health-hazards-of-legalizing-marijuana/
Supporting anti-corruption efforts in Hong Kong was a major focus during Ms. Waly’s mission. In a speech delivered at the 8th Symposium of the Independent Commission Against Corruption (ICAC) of Hong Kong on the occasion of the Commission’s 50th anniversary, Ms. Waly said that “In this era of uncertainty, as crises rage and threats simmer, we need to re-think and revitalize anti-corruption efforts,” adding that “corruption underpins many of the biggest challenges facing humanity today.”
In her remarks, Ms. Waly outlined four key priorities that UNODC considers essential to pave a new path for anti-corruption efforts, namely to 1) future-proof responses to corruption by leveraging the positive role of technology and unleashing the potential of youth; 2) unlock the full potential of international and regional anti-corruption frameworks, and to streamline cross border cooperation; 3) addressing gaps in capacities through partnerships; and 4) better understand corruption and its trends, through robust measurement, research, and analysis.
“Corruption is undermining everything we fight for, and empowering everything we fight against,” she said. “As we stand at this historic crossroads of challenges and opportunities, we need to seize every chance […] to innovate in the face of growing corruption challenges, together.”
On the sidelines of the Symposium, Ms. Waly signed a Memorandum of Understanding with ICAC Commissioner Woo Ying-ming to solidify their partnership and expand joint technical assistance to advance anti-corruption efforts in Asia.
Ms. Waly also met with the Chief Executive of Hong Kong, Mr. John KC Lee, to discuss the importance of coordinated regional action in the fight against organized crime.
Ms. Waly later visited the Hong Kong Jockey Club (HKJC) where she met its Executive Director of Racing and the Secretary General of the Asian Racing Federation (ARF).
Illegal betting in sports has become a global problem, helping to drive corruption and money-laundering in sports. By running the ARF and Anti-Illegal Betting and Related Financial Crime Council, HKJC is working to address issues like illegal betting and financial crimes that affect the integrity of sports and racing.
Ms. Waly invited the HKJC and ARF to support UNODC’s GlobE4Sport initiative, which will be launched this year. The initiative will create a global network which will support anti-corruption efforts in sport through the informal sharing of information between criminal justice authorities and sports organizations.
Ms. Waly also visited Hong Kong customs facilities, where she was briefed by Commissioner Louise Ho Pui-shan on the equipment and measures used by law enforcement to inspect cargo shipments and tackle trafficking in drugs and wildlife.
With fewer than 20 per cent of people with drug use disorders in treatment globally, UNODC is committed to supporting non-stigmatizing and people-centred health and social services to people who use drugs, as reflected by Ms. Waly’s visit to the Association of Rehabilitation of Drug Abusers of Macau (ARTM).
ARTM is a civil society organization offering voluntary, evidence-based prevention, treatment and harm reduction services to affected communities in Macau, China. Civil society organizations (CSOs) play a vital role in tackling drug related issues, including by combating stigma and delivering essential services to affected communities.
During the visit, Ms. Waly met with people in rehabilitation for drug use and learned about the work of ARTM in providing new life skills, such as painting, baking and ceramics classes, as well as treatment for women and classes for children.
ARTM was itself founded by a former user of drugs, Augusto Nogueira, whose experience helps the organization provide compassionate and inclusive rehabilitation. Augusto says that his main struggle when he was using drugs was not being able to identify a solution for his problem.
“My addiction was stronger than my will to stop using,” he said.
After undergoing his own challenging rehabilitation process, Augusto had ideas on how to professionalize the existing prevention and treatment activities in Macau. With the goal of providing evidence-based, personalized approaches to drug treatment and rehabilitation services, he founded ARTM in 2000.
ARTM belongs to the Asia-Pacific Civil Society Working Group on Drugs, supported by UNODC. Convened by the Vienna NGO Committee on Drugs (VNGOC), the Working Group aims to strengthen civil society action on drug related matters and the implementation of joint international commitments in the Asia-Pacific region.
ARTM also works to bring the voices of civil society to the international stage, including by presenting civil society recommendations on how best to implement drug policies at the Commission on Narcotic Drugs.
During her visit, Ms. Waly acknowledged the call from grassroot civil society organizations like ARTM for greater investment in evidence-based prevention, including through the implementation of the CHAMPS initiative. Ms. Waly praised ARTM’s cooperation with UNODC, including by delivering a training workshop on UNODC’s family-based prevention programme, Strong Families.
Ms. Waly also met with the Secretary of Security of Macau to discuss how Macau’s experience can help inform regional responses in tackling organized crime, illegal online gambling, and drug trafficking.
Source: https://www.unodc.org/unodc/en/frontpage/2024/May/unodc-executive-director-highlights-anti-corruption–fight-against-organized-crime–and-drug-prevention-on-visit-to-hong-kong-and-macau–china.html
Australia won’t see any cannabis cafes selling brownies anytime soon, despite agreement that the use of marijuana should be prioritised as a health issue.
https://www.dailytelegraph.com.au
A push to legalise the recreational use of cannabis on a national scale has been knocked back after experts expressed concerns it would lead to more use of the drug among young people.
A Senate committee rejected a bill introduced by Greens senator David Shoebridge on Friday, which calls to allow for cannabis possession for personal use in Australia, as well as the establishment of a national agency to regulate the growing of plants.
After receiving over 200 submissions the committee noted evidence from peak medical bodies including the Australian Medical Association (AMA) that warned wider access could exacerbate health risks, particularly for adolescents.
“Ultimately, the committee is concerned that the legalisation of cannabis for adult recreational use would create as many, if not more, problems than the bill is attempting to resolve,” the report said.
“While endeavouring to do so, the bill does not address several significant concerns, for example, ensuring that children and young people cannot access cannabis (particularly home-grow), managing risky cannabis use, and effective oversight of THC content.”
Multiple countries, including half of all US states have legalised recreational marijuana use. Picture: Ethan Miller/Getty Images/AFP
The committee report noted that the majority of submissions agreed that cannabis use “should be treated first and foremost as a health issue instead of a criminal issue.”
Cannabis remains the most commonly used illicit drug in Australia, according to the latest National Drug Strategy Household Survey, with more than 2.5 million people having used it recently.
In 2019, about 11.7 per cent of people aged 14 years reported having had used the drug at least once it in the past 12 months. The figure was higher for Aboriginal and Torres Strait Islander young people, at 16 per cent.
Under the Greens model, adults in Australia could legally grow six cannabis plants but it would remain a crime to sell the drug to anyone under the age of 18.
The bill also proposes the creation of licensed Amsterdam-style ‘cannabis cafes’ that sell marijuana products, such as edibles.
In his dissenting report, Senator Shoebridge argued the creation of a national cannabis market would generate thousands of jobs and remove “billions” from the black market.
“This inquiry shows clearly how evidence-based and human-centred reforms like this, we will need to break the stranglehold of politics as usual,” he said.
He said despite the committee’s findings the Greens plan to introduce the bill into parliament this year.
Senator Shoebridge claims up to 80,000 Australians could be flushed out of the criminal justice system if his Bill passed. Picture: NewsWire / Martin Ollman.
“The majority report in this inquiry reasonably fairly covers the evidence we had in the inquiry, although it does not detail the hundreds of individual submissions to the inquiry that, almost unanimously, asked us to vote this into law and to finally legalise cannabis,” he added.
Medical cannabis was legalised in Australia in 2016 and last year around 700,000 people reported having used cannabis for medical purposes.
Penalties for illicit use of marijuana, which remains illegal in all states and territories, vary based on jurisdiction.
In NSW, a first-time offender caught with a small amount of cannabis could be issued with a formal caution.
Offenders caught with up to 50 grams of cannabis in Queensland must be first offered a drug diversion program as an alternative to criminal prosecution.
In Western Australia, maximum fines can range from $2,000 to $20,000 and up to two years in prison.
Source: NCA NewsWire June 3, 2024 – 5:10PM
The communication below was issued by John Coleman, Chairman of DrugWatch International, to summarise the position with CBD and its legal status, as reported on in May 2020.
The format, as an email, has been retained in this version.
From: drug-watch-international@googlegroups.com <drug-watch-international@googlegroups.com> On Behalf Of John J. Coleman, PhD
Sent: 21 May 2020 17:30
To: drug-watch-international@googlegroups.com
Subject: Is CBD a controlled substance? DEA: Yes- FDA: No
In April 2020, the FDA approved a labelling for Epidiolex that specifically stated (at sect. 9.1) “EPIDIOLEX is not a controlled substance.” (see attachment). The DEA’s list of controlled substances as of May 2020 shows “APPROVED CANNABIDIOL DRUGS, AS DEFINED IN 21 CFR 1308.15(f)” as Schedule V controlled substance. The Code of Federal Regulations section referred to defines this as: “(f) Approved cannabidiol drugs. (1) A drug product in finished dosage formulation that has been approved by the U.S. Food and Drug Administration that contains cannabidiol (2-[1R-3-methyl- 6R-(1-methylethenyl)-2-cyclohexen-1-yl]-5-pentyl-1,3- benzenediol) derived from cannabis and no more than 0.1 percent (w/w) residual tetrahydrocannabinols.” (See attachment)
It should be noted that the scheduling of Epidiolex and CBD was not done in the usual manner by both FDA and DEA performing medical and scientific evaluations and assessments of abuse potential but, instead, the placement of CBD in the Epidiolex formulation is Schedule V was done upon an Order by the Attorney General pursuant to notification by the Secretary of State that the drug is required to be controlled (i.e., scheduled) by virtue of its scheduling status in the 1961 Single Convention on Narcotic Drugs. The U.S. ratified this treaty and, as a result, the Constitution requires that treaty obligations be enforceable as domestic law. The Attorney General could undo the scheduling by simply rescinding his Order or issuing a replacement Order setting forth the removal of CBD and the approved formulation of Epidiolex from Schedule V.
I’ve checked the Federal Register and there is nothing indicating that the Attorney General has removed CBD or Epidiolex from Schedule V as of May 20, 2020. I will make additional inquiries to see what’s going on here. The FDA’s label (prescribing information) is a legal certification of an approved drug’s uses and indications – as is the Attorney General’s Order (delegated to DEA) of 9/28/2018, described in 83 FR 48953. (See attachment)
John Coleman
Source: www.drugwatch.org
<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<DEA>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
Links to view the articles related to the above presentation:
First click on the link, then click on the image that appears:
Ricky Klausmeyer-Garcia’s friends struggled to get him addiction treatment, leading to the creation of a law in his name. A year after his death, profound questions remain about how best to help those with substance use disorder
by Katia Riddle in Seattle
Mon 13 May 2024 15.00 BST
Sitting at his dining room table, Kelsey Klausmeyer, 41, looks at a picture of his late husband, Enrique Klausmeyer-Garcia, known to most as Ricky. He died almost exactly a year ago, at the age of 37.
Kelsey can’t make sense of it.
When they met, Kelsey was awed by Ricky’s story: his long battle with addiction, his years of sobriety, his advocacy for recovery.
Now, after his death and in the midst of a nationwide addiction crisis, the narrative around Ricky’s life is less tidy.
Ricky is the inspiration for a Washington state law – known as Ricky’s law – passed in 2017 that enables loved ones and public safety officials to compel people experiencing substance abuse to undergo treatment, even if they are unable or unwilling to do it themselves.
The US has been experimenting with these forced-commitment laws for decades. The debate over their efficacy, practicality and ethicality is seeing renewed urgency in states such as New York, California and Washington, where addiction and severe mental health disorders have become a highly visible and highly political issue.
Ricky’s story brings into sharp relief one of the fundamental and difficult questions that officials in these places are grappling with: to what extent should society override an individual’s rights in the name of saving their life and protecting public safety?
I thought so highly of Ricky, to suffer with that disease and then turn around and do something for the greater good
Kelsey Klausmeyer, Ricky’s husband
For Kelsey, Ricky’s story is not primarily about public policy. It’s a story of immense personal joy and loss, laid before him in a handful of pictures. Here they are with their dog, Otis, whom Ricky “treated like our child”, chuckles Kelsey. Here they are in 2022 on their wedding day, both smiling, fit and handsome at a sunny mountain resort 90 minutes from their home in Seattle. Two hundred of their friends and family came to spend three days celebrating.
Here is Ricky with members of his sprawling family. When the couple first started dating, they discovered, remarkably, that they were both from families of nine siblings, both raised Catholic. “We always thought we were kind of destined in a way,” says Kelsey.
Kelsey grew up in Kansas; Ricky’s family immigrated from Mexico. They met online. Ricky was direct about what he wanted, a quality Kelsey, a naturopathic doctor, found attractive. “He shared that his dream was to have a family, to have kids, have a dog, have a house, have a husband,” remembers Kelsey. Those were prizes neither of them had felt certain were winnable. Together, they brought that picture into focus.
In those early, heady weeks of dating, Ricky was candid with Kelsey about his history with substance use disorder and his journey of recovery. Kelsey was undaunted.
“I just thought so highly of that, for somebody to have suffered with that disease as much as Ricky did, and then to turn around and do something for the greater good like he did,” remembers Kelsey. “That got me. That was the moment I fell in love with Ricky.”
But within the first year of their marriage, and despite Kelsey’s relentless attempts to help him, Ricky would be gone.
With his good looks, his authenticity, his goofy enthusiasm for life and willingness to be vulnerable, Ricky was a charmer. Kelsey wasn’t the first person to fall for him.
More than a decade before he met his future husband, Ricky met Lauren Davis. Their friendship would become one of the most important relationships in his life, and the driving force behind the involuntary-commitment law created in his name.
The two were in their late teens in 2004, working as assistant preschool teachers in Redmond, Washington. “I had an enormous crush on Ricky and spent several failed years attempting to woo him,” says Davis of their early friendship. Once they’d established she wasn’t his type, Davis became his “wing woman” and accompanied him to gay clubs. “I’m a white girl who grew up in Washington,” she says. “I can’t dance to save my life, but I sure tried.”
In the next few years, as the two grew into young adults, Davis would become a different kind of wing woman for her friend. Ricky spiraled into a serious problem with alcohol and occasional opioids. “I knew I was feeling depressed,” he recalled years later, in a public radio interview with the Seattle station KNKX. “I was feeling really anxious; most of the time I just wanted to escape all that. I just started to self-medicate and take whatever it took to escape reality.”
The first time Davis called 911 and had her friend taken to the hospital, she remembers his blood alcohol was dangerously high – she would find out it was at a near fatal level. He was admitted to the hospital’s psychiatric unit. Davis sat with him in his room from 8am to 8pm. She described trying to leave Ricky’s hospital room, “hugging him and he wouldn’t let me go”.
Davis and Ricky hiking on Mt Rainier in the summer of 2007. They two met in their early 20s and quickly became friends. Photograph: Courtesy of Lauren Davis
This episode set off a corrosive cycle of hospitalization, brief sobriety and relapse. Eventually, Ricky became suicidal.
“I found myself consistently in a position of trying to catch him, before he died, essentially,” says Davis. “In the course of those two years, he was in the emergency department over 75 times. I was at his bedside for most of those visits.” Numerous doctors told her to plan for his funeral. Davis refused. She would not stand by and watch her friend die.
Ricky’s father had terminal cancer during this period and despite family members’ efforts to help Ricky, his addiction stressed relationships. Davis became his primary advocate and champion.
Watching Ricky’s struggle, Davis was horrified at how little she could do to help him. What she wanted was to put her friend into an addiction treatment facility, because he was too sick to do it himself.
But at that time, in 2011, Washington law only allowed for involuntary commitment based on a psychiatric diagnosis, not for a substance abuse disorder. Other states had more expansive criteria.
Davis remembers Ricky on his sixth psychiatric hospitalization. “He had this young psychiatrist who looked across at him and said, ‘You know, if we were in another state and I could involuntarily commit you for your addiction, I would.’”
But in Washington state, the doctor said, “his hands were tied”.
American public policy has grappled with the concept of involuntary commitment since at least the 1850s. As many as 14 states had laws on the books before the turn of the 20th century allowing for civil commitment for “habitual drunkenness”. Often, offenders would be locked in asylums.
Over time, enthusiasm for this approach began to fade “because of the lack of evidence that the facilities were really able to cure substance abuse”, says psychiatrist and historian Paul Appelbaum, who teaches at Columbia University and studies medicine and ethics. Legislators – and the public – stopped supporting the investment. The country saw another wave of these statutes in the 1960s. Today, though roughly two-thirds of states have civil commitment laws that specifically include substance use, many are rarely used.
In part, that’s because there is still little consensus about the efficacy of committing someone to treatment against their will. “There are almost no data indicating whether it works or for whom it works,” says Appelbaum. Policymakers, he says – chronically guilty of short-term thinking – have been reluctant to invest in meaningful efforts to evaluate these kinds of programs. Those that have tried have shown mixed outcomes, and they often don’t measure long-term results.
Many who study addiction and substance use have ethical concerns. Holding someone long enough for treatment to possibly be effective, say some, is immoral.
Dr Liz Frye, who practices addiction medicine in Pittsburgh, explains that substances such as alcohol and opioids hijack the brain’s decision-making abilities. Regaining them can take months. “I have not seen an involuntary hold that would be long enough to help people regain their choice about substances,” she says. “I have a hard time with involuntarily committing someone for that length of time.”
Another complicating factor is that treatment and recovery itself can vary widely. “A lot of times, the perception is that everybody needs residential treatment,” says Michael Langer, who works in behavioral health for the state of Washington. “That’s not true.” Often the best course of treatment, says Langer, is outpatient, or medication-based.
Ordering someone into treatment is just based on a delusion that there’s somewhere for them to go
Keith Humphreys, addiction researcher
But staffing and funding for treatment facilities of all kinds is in short supply, and getting someone to a short-term treatment facility, with or without their consent, is only a first step on a successful path to recovery. Incentivizing and supporting the individual’s choice to maintain treatment is an equally critical part of the process. That can only happen with a robust and well-funded system that includes many different pathways and interventions.
“I think people imagine there’s this whole massive treatment system,” says Keith Humphreys, who studies addiction and public health at Stanford University. The truth is, he says, most systems across the country – privately and publicly funded – for treatment of addiction are frail and underfunded and can’t accommodate the demand, even from those who are pursuing it voluntarily.
In the United States, a recent report shows that 43% of people willingly seeking treatment for substance use were unable to access it. “Ordering them into treatment is just based on a delusion that there’s somewhere for them to go,” says Humphreys.
Police check on a man who said he has been smoking fentanyl in downtown Seattle. The addiction crisis sweeping US cities has raised complex questions about how to get people treatment. Photograph: John Moore/Getty Images
Lauren Davis helped to save her friend. In turn, he laid out the path for what would become her life’s work.
“I started to tell his story to anyone who would listen to me,” says Davis. Some of the people she demanded listen to her were legislators. They helped her introduce a bill for what became Ricky’s law.
After he eventually found his own way into treatment and long-term recovery, Ricky too became an advocate for his bill and Davis’s work. “If this law would have been in place back when I was in active addiction, I believe that my journey would have been cut that much shorter,” he would say in the interview with KNKX. “For a lot of addicts, they want to stop but they can’t. You could have loved ones tell you to stop. You could have all these consequences being behind your actions, and yet you won’t and can’t stop.”
The law amended Washington’s existing rule to allow for short-term, involuntary commitment not only for psychiatric disorders but also for those related to substance use. That meant people “gravely disabled” by addiction – and considered a danger to themselves – could now be committed against their will.
It designated tens of millions of dollars to creating a kind of holding place for detaining people under the law; there are now close to 50 “Ricky’s law” beds in four treatment facilities across the state.
But today, who needs these beds – and how to get them there – is not always clear.
“Someone who comes into the emergency department intoxicated on any substance who is a danger to themselves could be referred right off the bat under Ricky’s law,” says Paul Borghesani, medical director of psychiatric emergency services at Harborview medical center, Seattle’s public hospital. “Practically, that doesn’t happen.”
The reasons are numerous, says Borghesani. Often after 12-36 hours in detox, people who were previously at risk of great harm to themselves “appear much calmer”. Many even say they plan to quit using. This puts the clinicians in a bind, he explains, forcing them to reckon with a philosophical question: is someone a danger to themselves if they claim not to be?
The law is also dependent on a team of mental health professionals called designated crisis responders, employed through state contracts with regional behavioral health agencies and counties. These responders are deployed when someone – often a loved one, community member or medical provider, though it can be anyone – requests an evaluation of an individual in a substance use-related crisis. It’s at the discretion of these crisis responders to decide whether that individual is in enough danger, or endangering others enough, to commit them to a treatment facility – sometimes for just a few days but up to several weeks.
But waits are long for these responders; some advocates for those struggling with substance use disorders report enduring weeks before a designated crisis responder arrives. Sometimes that’s time they don’t have.
Another reason Borghesani says the law isn’t used: hospitals are busy. “Physicians are rightfully very eager to keep people flowing through the emergency departments,” he explains. “So they might look at this as something that would just take a lot of time and not be beneficial.”
Despite these obstacles, Ricky’s law is put to regular use in Washington. According to the Washington health authority, the state has been admitting roughly 700 people annually to substance-use facilities under Ricky’s law.
That number does not reveal how many people have elected to stay in recovery after their forced detention – a fact that makes it hard to say with certainty how effective it has been in galvanizing sustained recovery.
In 2024, the complex questions raised by Ricky’s law – and what helpful, compassionate addiction policy actually looks like – are more relevant than ever across the country. Recent CDC data shows a stunning national rise in alcohol-related deaths; more than 11% of adults had alcohol use disorder at some point in 2022, according to the National Institutes of Health.
A far more visible catastrophe of addiction is playing out in US cities overwhelmed in recent years by cheap, synthetic fentanyl. In Washington’s King county, home of Seattle, there were more than 1,000 overdose deaths in 2023, a nearly 50% increase from the previous year. Whole blocks are taken over by people buying, using and selling fentanyl. Arguably any one of these people is a grave danger to themselves.
Some outreach workers and medical providers on the frontlines of this problem would like to use the law to help this population, but say it’s not currently possible.
“We get stuck in this place of: what do we do?” says Cyn Kotarski, the medical director with a program called CoLead that helps people with housing and treatment. Kotarski often sees people with abscess wounds, days away from becoming septic. But with long waitlists for designated crisis responders, there’s no way to reach people in these crisis moments. “The option quite literally becomes: they stay outside until they die,” she says.
Frye, the addiction-medicine expert, says the problem is one of more than resources. The US, she says, needs an entirely new orientation to addiction treatment to underpin public policy, one that embraces methods such as harm reduction. “We have to stop being the moral police of people,” says Frye.
Public health addiction crises like the one that Seattle is battling, she argues, would be better addressed by tackling the surrounding problems – housing crises, trauma and mental health issues that give rise to substance use disorders. She imagines coupling this approach with accessible, compassionate therapeutic outpatient settings.
“The best way to help people reduce or stop using substances is to put the patient in the driver’s seat,” she says. “And we as healthcare providers are working towards helping them identify their own reasons to want to come back and quit.” Forced captivity, she argues, doesn’t meet that criterion.
But even Frye acknowledges a utility to saving a person’s life in certain circumstances without their consent. Sometimes her own patients are facing imminent death otherwise. “Transporting someone to the hospital involuntarily, getting that condition assessed, and helping make the hospital stay tolerable for the person – that’s warranted,” she says.
The exact circumstances in which to make this call are hard to define. Maybe impossible.
We get stuck in this place of: what do we do? The option quite literally becomes: they stay outside until they die
Cyn Kotarski, medical director with CoLead
Inspired by her work creating Ricky’s law, Lauren Davis decided to run for office, and was elected as a state representative in 2018. She has focused her policy efforts on expanding the state’s fragile system of treatment for substance abuse, an endeavor she continues today.
Davis acknowledges Ricky’s law needs course correction to be more useful, and she agrees that even if it’s improved, the law is not enough to adequately address the scope of addiction in places like Seattle.
“Do we just massively scale up Ricky’s law to address the scourge of fentanyl on the streets of Seattle?” she says. “No.”
Instead she’s focusing her current efforts on building a robust system of treatment that addresses comprehensive needs including housing and access to medications like methadone and Suboxone that can be provided over the counter to treat addiction. This effort also includes expanding a recovery navigator program, in which outreach workers build trust with people on the street and help them access resources – willingly.
Still, she firmly believes in the potential and power of Ricky’s law in certain circumstances. She’s seen it work first-hand, saying: “At the end of the day, I believe without a doubt that it has saved lives, that it has changed lives, that it has restored families.”
By late 2020, Ricky had been sober nine years. Then came an episode that would test both Ricky’s relationship with Kelsey and the law created in his name.
Kelsey recalls coming home one day from work and finding his then boyfriend passed out in the stairwell of their condo. Kelsey believes the pandemic triggered the relapse. Ricky had built a network of friends and family in the world of recovery, support that quickly dissolved in social isolation.
“I had heard him talk about what active disease looked like,” says Kelsey. “When it showed up, I was like: ‘Oh my God, what is happening?’”
During that event, according to both Davis and Kelsey, Ricky’s law worked the way it was supposed to. He was put in a temporary, involuntary hold. After a number of days of sobriety, says Davis, her friend re-emerged. “His brain came back online. He was able to make healthy choices,” Davis recounts.
Kelsey says: “He chose our life together.” Kelsey worked to help Ricky gain access to a residential treatment program.
It was more than two years later, after he and Kelsey were married, that relapse came again for Ricky. To Kelsey, it seemed out of the blue. Ricky had gone back to school and had a new job working for an organization supporting recovery for others. “We were really living the dream we always wanted,” he says.
He wonders if his husband was suffering from a kind of existential vertigo. “The only way that I can make sense out of it is that sometimes when things are so good, it’s the fear of losing it,” he says. “That’s what Ricky would talk to me about sometimes.”
This time, in post-pandemic 2023, systems of emergency and crisis support were stressed. Kelsey spent hours on the phone trying to make the legal and healthcare wheels turn in his favor. One night, worried that Ricky was literally going to drink himself to death, he drove his husband to the emergency room. The following day, when there was a staff change, says Kelsey, “the attending physician was going to just release him back out onto the street”.
“I would beg and plead with healthcare staff, police officers. I would say: ‘Ricky’s law is literally named after him,’” says Kelsey.
After Kelsey finally had him committed, Ricky became far less reachable, even after days of forced withdrawal and sobriety. At one point, he fled all the way to Oregon, out of the reach of his own law. Kelsey spent nights with no idea where he was. “I really can’t see anyone living on the side of the street or under an overpass without thinking about Ricky,” he says.
Eventually, Ricky ended up in a residential treatment facility in a Seattle suburb. He went there willingly; Kelsey was expecting to see his husband the next day. Instead, Ricky was found dead.
The cause of Ricky’s death is under investigation. Kelsey is now suing the facility, alleging wrongful death.
Kelsey’s faith in the law named for his husband remains steadfast, as does his belief in the power of recovery. “For anyone dealing with this,” he says, “please know there is hope.”
That optimism has not made his first year as a widower easier. It’s been “hell”, as Kelsey describes it. “I just miss him.”
This story is part of a reporting fellowship sponsored by the Association of Health Care Journalists and supported by the Commonwealth Fund
Source: https://www.theguardian.com/society/article/2024/may/13/rehab-forced-addiction-treatment#navigation
This is the Executive Summary of the DEA’s 2024 National Drug Threat Assessment
Fentanyl is the deadliest drug threat the United States has ever faced, killing nearly 38,000 Americans in the first six months of 2023 alone. Fentanyl and other synthetic drugs, like methamphetamine, are responsible for nearly all of the fatal drug overdoses and poisonings in our country. In pill form, fentanyl is made to resemble a genuine prescription drug tablet, with potentially fatal outcomes for users who take a pill from someone other than a doctor or pharmacist. Users of other illegal drugs risk taking already dangerous drugs like cocaine, heroin, or methamphetamine laced or replaced with powder fentanyl. Synthetic drugs have transformed not only the drug landscape in the United States, with deadly consequences to public health and safety; synthetic drugs have also transformed the criminal landscape in the United States, as the drug cartels who make these drugs reap huge profits from their sale.
Mexican cartels profit by producing synthetic drugs, such as fentanyl (a synthetic opioid) and methamphetamine (a synthetic stimulant), that are not subject to the same production challenges as traditional plant-based drugs like cocaine and heroin – such as weather, crop cycles, or government eradication efforts. Synthetic drugs pose an increasing threat to U.S. communities because they can be made anywhere, at any time, given the required chemicals and equipment and basic know-how. Health officials, regulators, and law enforcement are constantly challenged to quickly identify and act against the fentanyl threat, and the threat of new synthetic drugs appearing on the market. The deadly reach of the Mexican Sinaloa and Jalisco cartels into U.S. communities is extended by the wholesale-level traffickers and street dealers bringing the cartels’ drugs to market, sometimes creating their own deadly drug mixtures, and exploiting social media and messaging applications to advertise and sell to customers.
The Sinaloa Cartel and the Cartel Jalisco Nueva Generación (also known as CJNG or the Jalisco Cartel) are the main criminal organizations in Mexico, and the most dangerous. They control clandestine drug production sites and transportation routes inside Mexico and smuggling corridors into the United States and maintain large network “hubs” in U.S. cities along the Southwest Border and other key locations across the United States. The Sinaloa and Jalisco cartels are called “transnational criminal organizations” because they are not just drug manufacturers and traffickers; they are organized crime groups, involved in arms trafficking, money laundering, migrant smuggling, sex trafficking, bribery, extortion, and a host of other crimes – and have a global reach extending into strategic transportation zones and profitable drug markets in Europe, Africa, Asia, and Oceania.
Source: https://www.dea.gov/sites/default/files/2024-05/NDTA_2024.pdf May 2024

Nearly half of all U.S. citizens now live in a state where they can purchase cannabis from a recreational market, and all but 13 states have legalized medical use. These state-level policies have all been developed and adopted under a federal prohibition, which may be changing soon as lawmakers in both the House and the Senate are developing federal proposals to legalize cannabis.
A new USC Schaeffer Center white paper shows how state-level cannabis regulations have weak public health parameters compared to other countries, leaving consumers vulnerable. Federal legalization is an opportunity to implement regulations that better protect consumers and promote reasonable use. Regulations policymakers should consider include placing caps on the amount of the main intoxicant (THC) allowed in products sold in the marketplace and placing purchase limits on popular high-potency cannabis products, like edibles and vape cartridges, as has been done in other legalized jurisdictions abroad.
“Allowing the industry to self-regulate in the U.S. has generated products that are more potent and diverse than in other countries and has led to a variety of youth-oriented products, including cannabis-infused ice cream, gummies and pot tarts,” says Rosalie Liccardo Pacula, a senior fellow at the USC Schaeffer Center and Elizabeth Garrett Chair in Health Policy, Economics & Law at the USC Price School of Public Policy. “Current state regulations and public advisories are inadequate for protecting vulnerable populations who are more susceptible to addiction and other harm.”
High-potency cannabis products have been linked to short-term memory and coordination issues, impaired cognitive functions, cannabis hyperemesis syndrome, psychosis, and increased risks of anxiety, depression and dependence when used for prolonged periods. Acute health effects associated with high-potency products include unexpected poisonings and acute psychosis.
Product innovation within the legal cannabis industry has outpaced state regulations and our knowledge of health impacts of nonmedical, adult-use cannabis, write Pacula and her colleagues. Cannabis concentrates and extracts can reach concentrated THC levels of 90% in certain cases – many, many times more potent than dried flower that ranges between 15-21%. These products are also increasingly popular – sales for concentrates like vape pens rose 145% during the first two years of legalization in Washington state.
But state approaches to regulation have insufficiently considered quantity and potency limits. Just two states, Vermont and Connecticut, have set potency limits on both flower and concentrates. Most states base sales limits on product weight and product type, an approach that allows individuals to purchase excessive amounts of high-potency products in a single transaction.
An individual in most states can purchase 500 10-milligram servings of concentrates in a single transaction. Six states allow purchases that exceed 1,000 servings. By comparison, a full keg of beer, which usually requires registration, provides 165 servings of alcohol.
“Voters in many of these states supported legalization because they were told we would regulate cannabis like alcohol, but in reality, when it comes to product innovation, contents and standard serving sizes, the cannabis market has largely been left on its own,” says Seema Pessar, a senior health policy project associate at the USC Schaeffer Center. “And that is what is concerning for public health.”
“We are seeing evidence of real health consequences from this approach, especially among young adults,” explains Pacula. For example, studies show a rise cannabis-related emergency department visits for acute psychiatric symptoms and cyclical vomiting in states that legalize recreational cannabis.
To better regulate legal cannabis markets and products, researchers find four policy areas in which state laws and federal proposals can do more to encourage responsible use.
While generating tax revenue and reversing damages from prohibition are important, so is prioritizing public health — and prolonged use of high-potency cannabis products has health consequences, the researchers write.
“It is difficult to implement restrictive health regulations in markets that are already operating, generating jobs and revenue,” Pacula says. “Now is when the federal government has the best chance of ensuring a market that fully considers public health.”
Source: Cannabis Regulations Inadequate Given Rising Health Risks of High-Potency Products – USC Schaeffer July 2022
Alex Azar
Secretary of Health and Human Services
US Department of Health and Human Services
200 Independence Avenue SW
Washington D.C, 20201
November 5, 2019
Dear Secretary Azar:
This letter is to bring to your attention a study underway at the University of Washington referred to as the “Moms and Marijuana Study” and granted under the title: “Olfactory Activation and Brain Development in Infants with Prenatal Cannabis Exposure.” The Office of Human Research Protections issued a decision against opening a case on this research, and we are asking you, as the Secretary of Health and Human Services, to overturn that decision based on the scientific concerns we outline in this letter.
Women who are in their first trimester of a pregnancy, who are frequent users of marijuana for morning sickness, are being recruited. The study seeks to assess the damage marijuana prenatal exposure may have on the babies by means of various testing, including an MRI scan of the infants at six months of age. The recruited women will receive $300.00 + for their participation. The study is solely funded by NIDA. This study calls into question serious issues over human rights and raises ethical questions, including mandatory reporting pertaining to substance abuse in pregnancy. This open letter seeks to gather support from you in seeing that this study is re-evaluated at the federal level. The study’s website is at the following link: https://depts.washington.edu/klab/infoMM.html
We are of the view that the Kleinhans study does not meet the requirements set forth by the Office of Human Research Protections (https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr46/ ): “Subpart B presumption that pregnant women may be included in research, provided certain conditions are met. According to Subpart B, the permissibility of research with pregnant women hinges on a judgment of the potential benefits and risks of the research. Approval of proposed research carrying no “prospect of direct benefit” to the woman or fetus requires that the risk to the fetus be judged “not greater than minimal”. Fetal risk that exceeds that standard is permissible only when the proposed research offers a prospect of direct benefit to the pregnant woman, the fetus, or both.
Notably, if the proposed research does not fit within either of those two parameters, Subpart B offers an additional mechanism at the national level for approval by the Secretary of Health and Human Services.”
The federal definition of minimum risk reads: “That the magnitude and probability of harm or discomfort anticipated in the research are not greater in and of themselves than those ordinarily encountered in daily life or during the performance of routine physical or psychological examinations or tests.” Although the primary harm at issue is exposure to marijuana, the use of MRI or fMRI has not yet been proven safe for otherwise healthy infants, where an unknown risk would come with no benefit, as there is no diagnosis being sought. The UW study consent form reads on page 3:“There are no known side effects associated with MRI or fMRI when earphones are used to protect your hearing.” …. “There may be risks associated with the use of magnetic resonance which are not known at this time.” It is precisely questions about the potential for MRI risks that should be investigated in an animal model first. In principle, any study that recruits subjects and then tracks the consequences of drug transfer to a developing fetus should be carried out in animal models first, and not in humans until the animal results point towards safety. The evidence of decades of research on marijuana in pregnancy does not point to safety but rather to risk and harm.
Two basic principles in bioethics are relied upon to determine the merit of research that involves human subjects: Is the study necessary and can the research be done without the use of human subjects? There now exists a significant body of scientific evidence that warrants and justifies warning women not to use marijuana products at pre-conception, while pregnant, or breast-feeding. The University of Washington study is not necessary to conclude that marijuana use is associated with risk to the child (and also the mother). The National Academies, a lead authority, concluded in a scientific literature review in 2017: There is substantial evidence of a statistical association between maternal cannabis smoking and lower birth weight of the offspring. Studies have already shown that prenatal use is associated with a 50 percent increased likelihood of low birth weight. The Surgeon General’s advisory of August 29, 2019 is also relied upon here. What is the “necessity” that this study addresses? The conclusion has already been made by the findings of science – pregnant women should refrain from marijuana use in order to protect the life and health of their child.
Yet, in spite of existing scientific literature of concern, a highly misleading recruitment statement appears on the University of Washington study’s website introductory page: “We do not expect to find anything of medical concern during the infant MRI scans…If you’re interested in helping us learn more about whether cannabis is safe to use for morning sickness, click the Sign Up button and let us know!” Their lack of concern about the potential for adverse medical outcomes directly contradicts the findings of Grewen et al. (2015) which similarly evaluated postnatal outcomes using MRI scans on infants that had been exposed to marijuana in utero. As compared to controls, the exposed infants showed hypoconnectivity between brain regions: ” Marijuana-specific differences were observed in insula and three striatal connections: anterior insula–cerebellum, right caudate–cerebellum, right caudate–right fusiform gyrus/inferior occipital, left caudate–cerebellum. +MJ neonates had hypo-connectivity in all clusters compared with −MJ and CTR groups.” While an imperfect study because the cases included a proportion of women in the case group who used not only marijuana but also alcohol, tobacco, opiates and SSRIs, one of the two control groups was matched to the cases for use of those drugs, while the other was completely drug free. Notably, work in an animal model by Tortoriello et al. (2014) presents a plausible mechanism for the observed effect of marijuana seen between cases and controls. The combined evidence points towards harm, and confirmation could easily be sought in an animal model that parallels the intent of the University of Washington study.
Furthermore, the ethics are clearly different between the Kleinhans et al. and Grewen et al. studies, because unlike the protocol for the former, the study of Grewen et al. did not recruit women while the fetus was developing but recruited shortly before or after the time of birth. Being unaware of marijuana use until the time of birth, the researchers could not intervene to encourage abstinence for the sake of the fetus, whereas the University of Washington team could intervene, but their protocols do not allow them to. As a further point of distinction, the University of Washington protocol states that infants enrolled in the study will be screened and excluded if they have been in an NICU for 24 hours. This will, for obvious reasons, result in a biased outcome in reporting overall harm from marijuana use during pregnancy.
Typical morning sickness affects up to 91% of pregnancies (Castillo and Phillippi, 2015), and is regarded by many medical practitioners as being a reflex protecting against consumption of dangerous foods or beverages, as well as a sign of a healthy pregnancy because the absence of morning sickness is associated with a higher rate of miscarriage (reviewed by Sherman and Flaxman, 2002). The rare condition when morning sickness becomes pathologic, hyperemesis gravidarum, affects on average 1.1% of pregnancies, and is defined as a loss of 5% or more of the pre-pregnancy weight (Castillo and Phillippi, 2015). Maintenance of fluid and electrolyte balance may become problematic in this situation and pharmacologic intervention may become necessary, both for the health of the mother and the baby. To date, the serious documented outcomes include an increased risk for preterm births and low birth weight (Dodds et al., 2006).
Thus, if the Kleinhans study were to be proposing to recruit only those with hyperemesis gravidarum, the ethics might be more favorable. They would, however, have to exclude women whose marijuana use may have triggered the hyperemesis, which may occur in a subset of pregnant users (Alaniz et al., 2015). The study recruitment website is definitely remiss in not making that possibility clear to those interested in enrolling, and the research protocol describes no effort to ascertain if marijuana might be triggering hyperemesis in their study subjects.
In summary, there is already sufficient scientific evidence to answer the question as to whether or not marijuana is safe to use for typical morning sickness. That answer is no. Please see additional references for numerous research publications showing harm at the end of this letter.
Complaints have been filed with NIDA, The University of Washington, The World Medical Association regarding the Helsinki Declaration, The Office of Human Research Protections, and two doctors have filed a human rights complaint on behalf of the children involved. Complaint documents will be forwarded on request.
Thank you for your time in reviewing this serious situation.
Best regards,
Pamela McColl
Child Rights Activist
pjmccoll@shaw.ca
and
Christine L. Miller, Ph.D.
Neuroscientist
MillerBio
6508 Beverly Rd
Baltimore, Maryland 21239
cmiller@millerbio.com
et al.
Correspondence with the OHRP in regards to the University of Washington study began in September
of 2019. On October an email was received from the OHRP to Pamela McColl:
October 25, 2019
Hello,
OHRP has reviewed the study and will not be opening a case.
Sincerely,
Division of Compliance Oversight OHRP
September 25, 2019
“OHRP is now reviewing your complaint and this study. We are currently gathering the information about the research being conducted before a full review is started. Once OHRP completes a full review of the study, the research conducted and the study’s approval process, we will contact you with our findings. Please remember, this does not mean you can’t contact OHRP again before we finish the full review. You can contact us using this email address to update your complaint at any time.
Thank-you,
Division of Compliance Oversight (OHRP)
September 17, 2019
Thank you for contacting the Office for Human Research Protections (OHRP). OHRP has responsibility for oversight of compliance with the U.S. Department of Health and Human Services (HHS) regulations for the protection of human research subjects (see 45 CFR Part 46 at
www.hhs.gov/ohrp/regulations-and-policy/guidance/index.html
In carrying out this responsibility, OHRP reviews allegations of noncompliance involving human subject research projects conducted or supported by HHS or that are otherwise subject to the regulations, and determines whether to conduct a for-cause compliance evaluation. For further details see OHRP’s guidance, “Compliance Oversight Procedures for Evaluating Institutions,” at www.hhs.gov/ohrp/compliance-and-reporting/evaluating-institutions/index.html.
OHRP has jurisdiction only if the allegations involve human subject research (a) conducted or supported by HHS, or (b) conducted at an institution that voluntarily applies its Assurance of Compliance to all research regardless of source of support. Since this requirement appears to be met by the circumstances described in your email, OHRP appears to have jurisdiction.
Sincerely,
Division of Compliance Oversight
cc. Surgeon General Jerome Adams
cc. Director NIDA Dr. Nora Volkow
In-text citations:
Alaniz VI, Liss J, Metz TD, Stickrath E. Cannabinoid hyperemesis syndrome: a cause of refractory nausea and vomiting in pregnancy. Obstet Gynecol. 2015 Jun;125(6):1484-6.
Castillo MJ, Phillippi JC. Hyperemesis gravidarum: a holistic overview and approach to clinical assessment and management. J Perinat Neonatal Nurs. 2015;29(1):12-22.
Dodds L, Fell DB, Joseph KS, Allen VM, Butler B. Outcomes of pregnancies complicated by hyperemesis gravidarum. Obstet Gynecol. 2006;107(2, pt 1):285–292.
Grewen K, Salzwedel AP, Gao W. Functional Connectivity Disruption in Neonates with Prenatal Marijuana Exposure. Front Hum Neurosci. 2015;9:601.
Sherman PW, Flaxman SM. Nausea and vomiting of pregnancy in an evolutionary perspective. Am J Obstet Gynecol. 2002;186(5 Suppl Understanding):S190-7.
The National Academies of Sciences, Engineering, and Medicine, 2017, The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. National Academies Press, Washington, D.C. 20001
Tortoriello G, et al. Miswiring the brain: Δ9-tetrahydrocannabinol disrupts cortical development by inducing an SCG10/stathmin-2 degradation pathway. EMBO J. 2014;33(7):668-85.
Additional references on specific neonatal outcomes:
Lower birth weight, animal studies
Benevenuto SG et al., Recreational use of marijuana during pregnancy and negative gestational and fetal outcomes: An experimental study in mice. Toxicology. 2017;376:94-101.
“Five minutes of daily (low dose) exposure during pregnancy resulted in reduced birthweight…..females from the Cannabis group presented reduced maternal net body weight gain, despite a slight increase in their daily food intake compared to the control group”
Lower birth weight, human studies
Gunn,JKL, Rosales CB, Center KE, Nunez A, Gibson SJ, Christ C, and Ehiri EJ. Prenatal exposure to cannabis and maternal and child health outcomes: A systematic review and meta-analysis. BMJ Open 2016; 6(4):e009986.
“Infants exposed to cannabis in utero had a decrease in birth weight (low birth weight pOR=1.77: 95% CI 1.04 to 3.01; pooled mean difference (pMD) for birth weight=109.42 g: 38.72 to 180.12) compared with infants whose mothers did not use cannabis during pregnancy. Infants exposed to cannabis in utero were also more likely to need placement in the neonatal intensive care unit compared with infants whose mothers did not use cannabis during pregnancy (pOR=2.02: 1.27 to 3.21).”
Brown SJ, Mensah FK, Ah Kit J, Stuart-Butler D, Glover K, Leane C, Weetra D, Gartland D, Newbury J, Yelland J. Use of cannabis during pregnancy and birth outcomes in an Aboriginal birth cohort: a crosssectional, population-based study. BMJ Open. 2016;6(2):e010286.
“Controlling for education and other social characteristics, including stressful events/social health issues did not alter the conclusion that mothers using cannabis experience a higher risk of negative birth outcomes (adjusted OR for odds of low birth weight 3.9, 95% CI 1.4 to 11.2).”
Fergusson, D. M., L. J. Horwood, and K. Northstone. 2002. Maternal use of cannabis and pregnancy outcome. British Journal of Obstetrics and Gynaecology 109(1):21–27.
“Over 12,000 women expecting singletons at 18 to 20 weeks of gestation who were enrolled in the Avon Longitudinal Study of Pregnancy and Childhood……the babies of women who used cannabis at least once per week before and throughout pregnancy were 216g lighter than those of non-users.”
Preterm birth, animal studies
Wang H, Xie H, Dey SK. Loss of cannabinoid receptor CB1 induces preterm birth. PLoS One. 2008;3(10):e3320.
“CB1 deficiency altering normal progesterone and estrogen levels induces preterm birth in mice…. CB1 regulates labor by interacting with the corticotrophin-releasing hormone-driven endocrine axis.”
Preterm birth, human studies
Luke S, Hutcheon J, Kendall T. Cannabis Use in Pregnancy in British Columbia and Selected Birth Outcomes. J Obstet Gynaecol Can. 2019;41(9):1311-1317.
“Using cannabis in pregnancy was associated with a 47% increased risk of SGA (adjusted OR 1.47; 95% CI 1.33–1.61), a 27% increased risk of spontaneous preterm birth (adjusted OR 1.27; 95% CI 1.14–1.42), and a 184% increased risk of intrapartum stillbirth (adjusted HR [aHR] 2.84; 95% CI 1.18–6.82).”
Corsi DJ, Walsh L, Weiss D, Hsu H, El-Chaar D, Hawken S, Fell DB, Walker M. Association Between Selfreported Prenatal Cannabis Use and Maternal, Perinatal, and Neonatal Outcomes. JAMA. 2019;322(2):145-152.
“In a cohort of 661 617 women…. The crude rate of preterm birth less than 37 weeks’ gestation was 6.1%among women who did not report cannabis use and 12.0% among those reporting use in the unmatched cohort (RD, 5.88% [95%CI, 5.22%-6.54%]). In the matched cohort, reported cannabis exposure was significantly associated with an RD of 2.98%(95%CI, 2.63%-3.34%) and an RR of 1.41 (95% CI, 1.36-1.47) for preterm birth. Compared with no reported use, cannabis exposure was significantly associated with greater frequency of small for gestational age (third percentile, 6.1% vs 4.0%; RR, 1.53 [95%CI, 1.45-1.61]), placental abruption (1.6%vs 0.9%; RR, 1.72 [95% CI, 1.54-1.92]), transfer to neonatal intensive care (19.3%vs 13.8%; RR, 1.40 [95%CI, 1.36-1.44]), and 5-minute Apgar score less than 4 (1.1% vs 0.9%; RR, 1.28 [95%CI, 1.13-1.45]).”
Saurel-Cubizolles MJ, Prunet C, Blondel B. Cannabis use during pregnancy in France in 2010. BJOG. 2014;121(8):971-7.
“Cannabis users had higher rates of spontaneous preterm births: 6.4 versus 2.8%, for an adjusted odds ratio (aOR) of 2.15 (95% CI 1.10–4.18).”
Leemaqz SY, Dekker GA, McCowan LM, Kenny LC, Myers JE, Simpson NA, Poston L, Roberts CT;
SCOPE Consortium. Maternal marijuana use has independent effects on risk for spontaneous preterm birth but not other common late pregnancy complications. Reprod Toxicol. 2016;62:77-86. “continued maternal marijuana use at 20 weeks’ gestation was associated with” spontaneous preterm birth “independent of cigarette smoking status [adj OR2.28 (95% CI:1.45–3.59)] and socioeconomic index (SEI) [adj OR 2.17 (95% CI:1.41–3.34)]. When adjusted for maternal age, cigarette smoking, alcohol and SEI, continued maternal marijuana use at 20 weeks’ gestation had a greater effect size [adj OR 5.44 (95% CI 2.44–12.11)].”
Impacts on the neonatal immune system, animal study
Zumbrun EE et al. Epigenetic Regulation of Immunological Alterations Following Prenatal Exposure to Marijuana Cannabinoids and its Long Term Consequences in Offspring. J Neuroimmune Pharmacol. 2015; 10(2):245-54.
“Data from various animal models suggests that in utero exposure to cannabinoids results in profound T cell dysfunction and a greatly reduced immune response to viral antigens
Impacts on cortical wiring and development, animal studies
Tortoriello G, et al. Miswiring the brain: Δ9-tetrahydrocannabinol disrupts cortical development by inducing an SCG10/stathmin-2 degradation pathway. EMBO J. 2014;33(7):668-85.
“Here, we show that repeated THC exposure disrupts endocannabinoid signaling, particularly the temporal dynamics of CB1 cannabinoid receptor, to rewire the fetal cortical circuitry….these data highlight the maintenance of cytoskeletal dynamics as a molecular target for cannabis”
DiNieri JA, Wang X, Szutorisz H, Spano SM, Kaur J, Casaccia P, Dow-Edwards D, Hurd YL. Maternal cannabis use alters ventral striatal dopamine D2 gene regulation in the offspring. Biol Psychiatry. 2011 Oct 15;70(8):763-9.
“we exposed pregnant rats to THC and examined the epigenetic regulation of the NAc Drd2 gene in their offspring at postnatal day 2, comparable to the human fetal period studied, and in adulthood…. Decreased Drd2 expression was accompanied by reduced D2R binding sites and increased sensitivity to opiate reward in adulthood”
Rodríguez de Fonseca F, Cebeira M, Fernández-Ruiz JJ, Navarro M, Ramos JA. Effects of pre- and perinatal exposure to hashish extracts on the ontogeny of brain dopaminergic neurons. Neuroscience. 1991;43(2-3):713-23.
“Perinatal exposure to cannabinoids altered the normal development of nigrostriatal, mesolimbic and tuberoinfundibular dopaminergic neurons, as reflected by changes in several indices of their activity”.
Impacts on cortical wiring and development, human studies
Grewen K, Salzwedel AP, Gao W. Functional Connectivity Disruption in Neonates with Prenatal Marijuana Exposure. Front Hum Neurosci. 2015;9:601.
“+MJ (marijuana-exposed) neonates had hypo-connectivity in all clusters compared with –MJ (marijuana unexposed) and CTR (control) groups. Altered striatal connectivity to areas involved in visual spatial and motor learning, attention, and in fine-tuning of motor outputs
involved in movement and language production may contribute to neurobehavioral deficits reported in this at-risk group. Disrupted anterior insula connectivity may contribute to altered integration of interoceptive signals with salience estimates, motivation, decision-making, and later drug use.”
El Marroun H, Tiemeier H, Franken IH, Jaddoe VW, van der Lugt A, Verhulst FC, Lahey BB, White T. Prenatal Cannabis and Tobacco Exposure in Relation to Brain Morphology: A Prospective Neuroimaging Study in Young Children. Biol Psychiatry. 2016;79(12):971-9.
“prenatal cannabis exposure was associated with differences in cortical thickness….. it may be possible that the frontal cortex in cannabis-exposed children undergoes altered neurodevelopmental maturation (i.e., having differences in cortical trajectories) as compared with
nonexposed control subjects”
Wang X, Dow-Edwards D, Anderson V, Minkoff H, Hurd YL. In utero marijuana exposure associated with abnormal amygdala dopamine D2 gene expression in the human fetus. Biol Psychiatry. 2004; 56:909–915.
“Adjusting for various covariates, we found a specific reduction, particularly in male fetuses, of the D(2) mRNA expression levels in the amygdala basal nucleus in association with maternal marijuana use. The reduction was positively correlated with the amount of maternal marijuana intake during pregnancy.”
Received by email
Police forces in the province collected 795 blood samples from motorists suspected of driving while under the influence.
One year after the legalization of recreational use of cannabis in Canada, the black market for the drug — as well as its use behind the wheel — continues to keep Quebec police forces busy.
In 2018, police collected 795 blood samples from motorists suspected of driving while under the influence, and sent them to Quebec’s medical legal centre for processing. That’s 254 more than in the previous year.
The presence of cannabis was detected in 46 per cent of those cases.
The Sûreté du Québec says cannabis is the most commonly detected drug in its traffic stops.
The provincial force said that since legalization, cannabis was detected in the systems of 113 persons pulled over for impaired driving, compared with 73 cases a year earlier — an increase of 54 per cent.
More than 670 officers trained in drug use evaluation have been deployed across the province.
In a statement issued Thursday detailing its operations over the past year, the SQ said it had opened 1,409 investigations into the illegal production, supply and distribution of cannabis, which led to 1,458 warrants being executed and charges filed against 1,403 individuals.
Meanwhile, raids on illegal outdoor cannabis fields were carried out in August and September, and saw 37,000 plants seized.
Over the past year, the SQ seized 71,500 cannabis plants, 161 kilograms of cannabis, 15.8 kilograms of cannabis oil and resin, 23,460 units of edible cannabis and $180,000 in cash.
Source: https://montrealgazette.com/news/local-news/quebec-pot-arrests-behind-the-wheel-up-54-since-legalization October 2019
INTRODUCTION
In 2013, Uruguay became the first country in fully regulating the marijuana market that now operates under state control.
In a Washington Post feature article on Uruguay’s cannabis laws, they reported that Uruguay is socially liberal and has a wide separation of church and state. Gambling and prostitution are legal and regulated. Uruguay is also the only Latin American nation outside Cuba that has broadly legalised abortion, and it was one of the first to recognize civil unions and adoption by same-sex couples. Uruguay also is accustomed to relatively high levels of regulation and a big state role in the economy, with an array of government-owned banks, gas stations and utilities. Over the years, activists began to argue: Why not weed?
As early as 1974, Uruguay decriminalised possession of “a minimum quantity [of illicit substances], intended solely for personal use.” Exactly what constituted a “minimum quantity” was never clarified, giving judges broad discretion in its interpretation.
The initiative of marijuana regulation was by the then president José Mujica. Lawmakers in Uruguay (population: 3.3m) signed the country’s cannabis bill into law in December 2013 and pharmacies began selling two strains of legal marijuana cultivated by two government-authorised firms in July 2017.
The text of the law expresses its goals through three main objectives, which included reducing drug trafficking-related violence by taking cannabis off the black market, and promoting public health through education and prevention campaigns, thereby “minimising the risks and reducing the harm of cannabis use”.
Uruguay was the first country to leave behind the global ban on non-medical cannabis that began with the United Nations’ 1961 Single Convention on Narcotic Drugs, and despite repeated criticisms from the International Narcotics Control Board (INCB), as in the Board’s report for 2016, which states:
The Board notes the continued implementation by the Government of Uruguay of measures aimed at creating a regulated market for the non-medical use of cannabis… [T]he Board wishes to reiterate its position that such legislation is contrary to the provisions of the international drug control conventions… according to which States parties are obliged to ‘limit exclusively to medical and scientific purposes the production, manufacture, export, import, distribution of, trade in, use and possession of drugs.’
Concerned that their policy would come under intense scrutiny from their neighbours and from the broader international community, Uruguayan authorities deliberately opted for a strict approach to regulation, such as a user registry and monthly sales limits.
In an attempt to reassure the international public opinion, President José Mujica, said that his government would not allow unlimited use of marijuana and illicit drug dealing: “And if somebody buys 20 marijuana cigarettes, he will have to smoke them. He won’t be able to sell them“.
And in order to convince the majority of the Uruguayan population, the President Mujica promised to launch at the same time “a campaign aimed at young people on how to consume marijuana. Avoid, for example, to smoke to not damage the lungs but inhale or consume it with food“.
In response to public opposition, the Open Society Foundation headed by the financier George Soros announced the launch of a massive media campaign across the nation to manipulate the public consensus. Time magazine (5 Aug 2013) reported that “a massive media campaign, with television ads funded partly by Soros’ Open Society Foundations group, were required to convince opponents of legalisation”.
STATE CONTROL – HOW IT WORKS
There are three ways to legally obtain cannabis in Uruguay. The first alternative is autocultivo, which allows individuals to grow up to six marijuana plants per household and yield an annual crop of 480 grams per year, or 40 grams per month. All individuals must register with the government agency for the regulation and control of cannabis—called the Instituto de Regulación y Control de Cannabis (Cannabis Regulation and Control Institute) to grow these plants in their home and no person may register more than one location for domestic growth. The second alternative is the Cannabis Club, which allows between 15 to 45 members of a duly-registered civil association to farm up to 99 marijuana plants in specific locations. Each club may not supply any individual with more than 480 grams of marijuana per year. The third alternative is sale through pharmacies. This alternative will allow a registered consumer to buy up to 40 grams of marijuana per month and 480 per year in person from pharmacies that are registered with the IRCCA and the Ministry of Public Health. On July 19, 2017, Uruguay launched the last remaining stage of the cannabis law, with sales finally beginning in 16 pharmacies across the country.
PUBLIC DISAPPROVAL
Public opinion surveys have consistently shown most Uruguayans to be doubtful about the government’s initiative.
According to the results of the 2014 AmericasBarometer survey in Uruguay, only 34% of Uruguayans approved the new regulations regarding the liberalization of marijuana use, while 60.7% showed their disapproval to the new policies. Perhaps not surprisingly, approval for the new regulation of cannabis is closely related to previous personal experimentation with marijuana and a history of marijuana consumption among relatives and close friends.

PUBLIC SKEPTICISM
As of 2014, most Uruguayans remained skeptical about the benefits the new regulation will bring. For instance, 42% of Uruguayans considered that the general situation of the country would worsen as a result of regulation, while only 19% believed that the situation would improve. Among the most negative opinions expressed, 70% of Uruguayans stated that public safety and public health conditions would either worsen or remain the same. The issue that seemed to generate the most positive opinions was related to the fight against drug trafficking organisations.

PUBLIC USAGE
In 2001, 5.3% of the population admitted to having consumed marijuana.
By 2014, life prevalence had quadrupled with 22.1% of Uruguayans acknowledging some consumption.

Since Uruguay legalised the sale of marijuana, underage use increased from 14% to 21%. Use by those aged 19 to 24 increased from 23% to 36% Those aged 25 to 34 increased from 15% to 25%.

TEENS
Prevalence doubled among secondary school students from 2003 to 2014. In 2003, 8.4% of students had consumed marijuana during the previous twelve months. in 2014, 17% had.
Almost a quarter of the high-frequency users of Montevideo had their first experience with marijuana before age turning 15 (24.1%).
Prevalence is also higher among 18-25 year-olds than other age categories.

NON-COMPLIANCE
As at February 2018, 8,125 individuals and 78 cannabis clubs with a total of 2,049 members were registered in addition to the 20,900 people registered through pharmacy sales for cannabis. The system potentially provides cannabis to around 30,000 of the 140,000 past-month cannabis users estimated in Uruguay in 2014.
A recent survey found that almost 40% said they would probably or definitely flout the law which requires registration. (19.6% state that it is not probable that they will register, and another 19.6% said that they are certain that they will not register.)
MONITORING AND EVALUATION
A 2018 Brookings Institute report details how the Ministerio de Salud Pública is required to submit an annual report on the impacts of the legalization since 2014 – but the ministry has only submitted such a report once, in 2016, and the findings were not made public.
According to a report by WOLA (funded by Open Society Foundations – aka George Soros) and posted on the Monitor Cannabis Uruguay site, in spite of President Vázquez’s support for monitoring and evaluation, his administration has provided the public with relatively little in the way of hard data on the early effects of initial implementation of the cannabis measure.
The IRCCA’s limited staff – it has a team of six inspectors who are responsible for ensuring compliance – does not realistically allow the institute to check the annual plant yields for all 8,000+ homegrowers and approximately 80 registered clubs.
PRODUCTS
A recent study of marijuana consumers in Montevideo found that users had consumed it in several different ways during the past year, including vaporizers (15.7%), edibles, such as brownies, cakes, cookies (26.4%), and drinks, such as mate, milkshakes, daiquiris (9.4%).
PERCEPTION OF RISK
The study of marijuana consumers in Montevideo also found that users had a very low perception of risk associated with undertaking several activities while under the influence of marijuana. For instance: 21.4% of respondents drove a car under the influence of marijuana; 28.4% rode a motorcycle; 11.2% operated heavy equipment. More than half of the respondents (55.4%) declared that they consumed marijuana and went to work before four hours had passed.
More than one in every four of those women who were pregnant (26.1%) reported to having continued consuming marijuana while pregnant.
BLACK MARKET
Three years after legalisation, seven out of every ten cannabis consumers still acquire the product on the black market. Authorities admit that “street selling points have multiplied in recent years, along with criminal acts related to micro trafficking.”
Marcos Baudeán, a member of the study group Monitor Cannabis Uruguay, suggests it may be worse than that: “Consider the fact that there are 55,000 regular consumers who are responsible for 80% of the marijuana consumption in the country, but currently only 10% are consuming from the legal market, the rest are buying the drug off the illegal market.”
Others have pointed to the very low concentration of THC in the legal drug as another reason why some users may turn to the black market. Though the price may be higher — a gram of high-potency illegal marijuana can cost as much as $20— some users may be willing to pay this premium in exchange for access to a more powerful drug.
Because sales to tourists are prohibited, some Uruguayan homegrowers and clubs have attempted to get around the ban by offering ‘cannabis tours’, which are framed more as social and educational experiences, in which participants are free to sample cannabis while on a paid tour. Others simply sell directly to tourists behind closed doors, a grey market quietly operating via word of mouth.
FINANCIAL IMPLICATIONS
An unexpected consequence of Uruguay’s marijuana law is that the U.S. government invoked the Patriot Act which prohibits U.S. banks from handling funds for distributors of marijuana. In Uruguay, this is by way of the pharmacies only. International banks – both those with U.S. headquarters such as Citibank and European banks such as Santander have advised their Uruguayan branches that they are prohibited from providing services to the distributors of marijuana.
As a result, pharmacies tasked with the sale and distribution of marijuana have been cut off from the entire financial services market because the banks in Uruguay announced that every business associated with the newly legal marijuana industry risked being in violation of the U.S. drug laws and would lose their access to U.S. banks and dollar transactions.
SUMMARY
What we have learned from the data so far indicates that frequency of consumption has significantly increased, especially in the 15-24 age group. The perception of risk with drug use is low, and risky behaviours have increased with the frequency of consumption, including use of marijuana during pregnancy. The black market is alive and well. And the overwhelming support for the regulation among high-frequency marijuana users does not immediately translate into willingness to comply with it. Of most concern is that monitoring and reporting of the effects of legalisation is minimal, and not made public.
The drug-friendly website CannabisWire in July 2018 summed it up perfectly. “What Have We Learned From the First Nation to Legalize Cannabis? Not Enough.”
Source: Uruguay – Say Nope to Dope 2019

(Image Credit: 7raysmarketing via Pixabay)
Contrary to advocates’ promises, legalizing pot has spurred new illegal enterprises. https://t.co/1k9twTCrmg via @cjstevempic.twitter.com/VKND92hjl5
— City Journal (@CityJournal) June 12, 2019
Unintended consequences of legislation are more commonplace than they should be, but minimizing them would require more nuanced political debate and that option has probably left us forever.
A new article in City Journal details just how legal marijuana is the gateway drug to illegal marijuana enterprises:
Though advocates claim that one of the benefits of legalizing recreational marijuana is that the black market will disappear and thus end the destructive war on drugs, the opposite is happening. States that have legalized pot have some of the most thriving black markets, creating new headaches for law enforcement and prompting some legalization advocates to call for a crackdown—in effect, a new war on drugs.
Unlicensed pot businesses have already become a problem for Los Angeles just a year and a half after legalization. The city is devoting police resources that are already stretched thin to address the situation.
City Journal notes that it’s not just mom and pop scofflaws that are problematic:
Legal-pot states are attracting international criminal cartels. Mexican drug gangs have smuggled illegals into Colorado to set up growing operations, former U.S. prosecutor Bob Troyer wrote last September, explaining why his office was stepping up enforcement. Rather than smuggle pot from Mexico, the cartels grow it in Colorado and smuggle it elsewhere—spurring violence. In 2017, seven homicides in Denver were directly connected to marijuana growers. “I would love to be able to shift some of my resources away from marijuana to other things,” Denver lieutenant Andrew Howard said last year. “But right now, the violence is marijuana or marijuana-related.”
More cartel violence and more illegal immigration…yay legal weed!
I’m no anti-pot Puritan, but I am on record as always having been frustrated by the discussions surrounding legalization efforts. They are rarely in-depth and mostly focus on marijuana’s medicinal uses. It is often portrayed as harmless, which is nonsensical. It’s not heroin, but it’s also not baby aspirin.
What were almost never discussed pre-Colorado were the consequences of legalizing a black market drug. It’s a bit naive to think that the major players from the black market would flee into the shadows once their commodity became legit.
Cartels may be illegal enterprises, but they are still businesses. They can adapt to changing markets. It would appear they are also adept at outreach:
Legal-marijuana businesses are getting in on the game, too. Last year, Denver authorities arrested the owners of a licensed chain of pot shops that employed 350 people for supplying the black market. In January, three owners of the business pled guilty to drug and racketeering charges. In Oregon, federal prosecutors arrested six individuals in 2018 and charged them with “vast” interstate-trafficking schemes that supplied black-market pot to Texas, Virginia, and Florida. Some of the suspects were also charged with kidnapping, money-laundering, and use of a firearm in a drug-trafficking crime.
So much for the harmless stoner sales pitch.
None of this is surprising for advocates of smaller government. Legalization and regulation were supposed to make the marijuana black market and its problems go away. Instead, as the City Journal conclusion observes, it’s merely created “Black Market 2.0.”
High times indeed.
Source: https://pjmedia.com/trending/legal-marijuana-a-boon-to-illegal-cartels/ June 2019
The title of “Cannabis in Medicine: An Evidence-Based Approach” contains an irony. In chapter after chapter in this multi-authored book written predominately by providers associated with mainstream medical facilities in Colorado, the authors point out the inadequacy of the evidence we have and the absence of the evidence we need to determine how – or even if – cannabis has medical legitimacy. The foreword’s title, “Losing Ground: The Rise of Cannabis Culture,” sets the tone. David Murray, a senior fellow at the Hudson Institute, argues convincingly that “the current experiment with cannabis, underway nationwide [is] leading us towards a future of unanticipated consequences, a future already established in the patterns of use ‘seeded’ in the population but as yet unmanifested.” In other words, the cannabis horse has not only fled the barn but has been breeding prolifically to the point that we couldn’t get rid of it and its progeny if we wanted to!
The 20 chapters following the foreword are divided into basic science (three chapters) and clinical evidence (17 chapters) sections. Over and over in the clinical evidence chapters, individual authors remind the reader of the lack of quality control in production, the dearth of strong evidence from adequately designed research trials, and the intensifying potency of cannabis with attendant dangers, particularly for youth. The organization of this section lacks consistency in that some chapters focus on specialty (e.g. pulmonary medicine), others on patient groups (e.g. the pediatric and adolescent population), others on physiological implications (e.g. clinical cardiovascular effects; neuropsychiatric effects), others on specific diseases (e.g. gastrointestinal disorders; ocular conditions), and still others on public health topics (e.g. cannabis-impaired driving). While all are relevant, a specialty or organ system focus, with a separate public health section might lend the book more coherence. It would also be worth exploring how “cannabis culture” has become in essence a parallel medical system, with many of cannabis’s most ardent proponents as dropouts from establishment medicine after its nostrums for diagnoses like chronic pain, anxiety, and depression have failed to bring them relief.

I would have liked a chapter specifically grappling with the porous boundary between federal and state jurisdictions over cannabis as medicine and marijuana as recreational substance. Lawyer David G. Evans’ admirable chapter on “The Legal Aspects of Marijuana as Medicine” moves in that direction when he writes that, “‘medical marijuana’ is not a ‘states’ rights’ issue.” To wit, for no other drug than cannabis has the federal government ceded regulatory responsibility to states that are variably (but mostly not) equipped to handle it. The truth, complex in its contradictions and inconsistencies, is that in the United States, marijuana remains a Schedule I drug without recognized medical value; the Federal Drug Administration overseeing American pharmaceuticals throws roadblocks in the way of studying it, thereby interfering with the development of a robust evidence base; the federal government has looked the other way and even colluded with the states as one after another has legalized cannabis medically, recreationally, or both; and physicians risk their federal licenses to prescribe if they do more than recommend this drug. In a nutshell, any effort to impose logic is doomed because the American scene vis-à-vis cannabis is seemingly irretrievably illogical.
The editor of this volume, Kenneth Finn, MD, a PMR and pain management specialist in Colorado Springs, Colorado, is to be commended for encouraging individual chapter authors to develop encyclopedic bibliographies. The book can thus serve as a resource for practitioners wishing to delve into a vast and growing literature that continues to offer little that is conclusive. The book can also serve as a primer on what is known about cannabis as medicine, keeping in mind a slant throughout – not necessarily unjustified, at least from an allopathic or osteopathic perspective – that cannabis is neither legitimate as medicine nor safe, even for recreational use.
Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7723137/ Sept-Oct 2020

Hemp plants are visible inside several structures on Sept. 16, 2020, in Shiprock, New Mexico.
NOEL LYN SMITH/THE FARMINGTON DAILY TIMES USA TODAY NETWORK – NEW MEXICO
Leaders on the Navajo Nation have cracked down on one of its members who they say has used immigrant labor to transform 400 acres of crop land into hemp farms in the reservation’s northeastern corner.
The crops — illegal under Navajo law — have pitted residents and reservation officials against entrepreneur Dineh Benally, who has formed a partnership with a Las Vegas company that says it develops hemp and cannabis businesses on Native American lands.
Navajo Nation leaders took Benally to court and got an initial victory last week: District of Shiprock Judge Genevieve Woody granted a temporary restraining order halting the hemp farming.
Navajo Nation President Jonathan Nez said the order grants tribal law enforcement officers’ authority to stop hemp production. Navajo Nation police have begun asking some workers on the hemp farms — people law enforcement officials claim are immigrant workers from Asia — to leave tribal land.
The ruling appears to provide a brief break in the dispute that came to a head this summer over the legality of Benally’s operation, which he claims has also provided employment for more than 200 members of the tribal nation.
The hemp farms are located around Shiprock on the Navajo Nation, which encompasses northeastern Arizona, northwest New Mexico and a sliver of southeastern Utah.
The farms have prompted protests and allegations that Benally is illegally growing marijuana under the guise of a hemp farm with the help of foreign nationals.
Both crops are illegal on tribal land. “The hemp will not stay here,” Nez said.
A few hundred Navajo tribal members also work on the farms, officials say.
The battle over the farms has resulted in protests and last week’s showdown in the District Court of the Navajo Nation Judicial District of Shiprock.
“We strongly urge everyone to respect the ruling of the court and move forward peacefully to ensure the safety of community members, police officers and everyone in the impacted area,” Nez said after the hearing.
Benally said in a statement that he was disappointed by the court’s decision, saying it will have a “chilling effect” on Navajo business and economic development.
But residents like Beatrice Redfeather, 75, said the hemp farms have made her fear opening her front door.
“I see marijuana plants. I see a bunch of foreign workers, armed security guards. I see a security patrol 32 feet from my front door,” Redfeather said during a court hearing last week. “Those security guards have made it known they will attack, and they have shown their guns to our family. We are mentally afraid to walk outside … The smell of marijuana is so strong that I have had to go to the hospital because of my severe headaches.”
In an investigation published Wednesday by Searchlight New Mexico, people who said they had worked on the farms described growing marijuana, and said some people who worked there were teenagers or younger.
Legal marijuana: Pros and cons
An attorney for Benally says his client is growing hemp, a less potent form of cannabis. Products made from it are commonly used and sold across the United States at major supermarkets and convenience stores.
Benally argued in court filings that the 2018 Farm Bill, signed into law by President Donald Trump, allows him to grow hemp on reservation land.
But tribal leaders say harvesting both hemp and marijuana is illegal on the Navajo Nation — except for a government-backed pilot project. Navajo law, however, has no penalty for growing hemp, Nez said, so the nation took Benally to court.
Navajo Nation Attorney General Doreen McPaul filed a lawsuit against Benally in June, charging Benally and his company of illegally growing industrial hemp and unlawfully issuing land use permits.
Nez said tribal leaders believe the potency of Benally’s crops is well above the federal threshold that defines hemp as no more than 0.3% tetrahydrocannabinol. or THC, the main active ingredient of cannabis.
Regardless, the controversy has prompted heated skirmishes in recent months.
Benally has hired guards who patrol the farms wearing bulletproof vests and body cameras, according to court testimony that claimed arsonists torched at least one farm. Benally’s top security officer, Duane Billey, said in court that protesters have attacked him, but his force doesn’t carry guns. Locals say otherwise.
Officials also are critical of the use of what they believe are Asian migrants who have come to the reservation during a global pandemic and camped on the farms, where they work in greenhouses.
Sonya Sengthong, a Glendale resident whose family lives near Shiprock, said relatives have told her vans and sport utility vehicles with California and Texas license plates continually drop off what she believes are workers for the farms.

The volcanic spire, seen from town in New Mexico.
MEGAN FINNERTY/THE REPUBLIC
“We are concerned some of these visitors may be mistreating our people,” Nez said in an interview with The Arizona Republic. “There are large areas that they are using to put up housing on these farms.”
Nez said the laborers also are breaking the law as visitors have been banned from the reservation during the COVID-19 pandemic, which has ravaged the Navajo Nation.
Nez said he does not know when scores of workers started arriving on the reservation, adding that some live in nearby Farmington.
“Workers are coming in and they are not citizens. They are from other areas,” Navajo Nation police Chief Philip Francisco said during last week’s hearing. “There’s a general worry about a criminal element coming in, and there’s a belief that the hemp is not hemp but marijuana.”
“We have seen a lot of Asian people working on the farms, and there’s a law in place to not allow visitors on the Navajo Nation,” Nez said in an interview. “Because of the high population of these visitors, there are concerns about human waste.”
Nez and other Navajo officials confronted some of the workers during an unannounced visit to one of the farms on Sept. 3. “They claim they don’t speak English, so we started talking back to them in Navajo,” Nez said.
Benally and his attorney, David Jordan, have declined to answer questions about how employees came to work on the farms. But Jordan claims the Asian workers have been racially profiled and attacked by Navajos who oppose Benally’s business venture.
“They want to blame my client for the violent protests and that they threaten the safety of the Navajo Nation,” Jordan said in court. “But they have a fear of other people who are different.”
‘Blatant disregard’
Benally has used his position on the San Juan River Farm Board, which represents a half-dozen or so communities or chapters on the Navajo Nation, to grant land use permits to grow hemp, and his ownership of the Native American Agricultural Company to produce the crops.
The farm board on which Benally sits is composed of elected members from various chapters or communities within the Navajo Nation. Its purpose is to develop and sustain farmland and water systems for economic development.
The initial lawsuit filed against Benally says farm boards are not authorized to issue agricultural land use permits for hemp. Instead, according to Navajo law, it only is authorized to review and recommend approval of permits to the Resources Committee of the Navajo Nation Council, the legislative branch of the reservation’s government.
Tracy Raymond, a former farm board member, stated in a court filing that Benally has used his farm board position to “serve his personal interests without approval or authorization.” “It is a great disappointment to me to have to watch those growing hemp openly flouting the law just to make a quick profit,” Raymond, a corn farmer, said.
He added the farm board never took a vote to authorize the issuance of hemp licenses.
Benally, on his personal website, said he’s used his leadership position to “collaborate with government delegates, grazing officials, and chapter officials to protect native water rights and improve the economy and livelihood of the Navajo People.”
Benally’s business partners
His company partnered with One World Ventures, a Las Vegas-based penny-stock company with shares worth about 2 cents each, to operate the farms, financial records show.
Some financing came from SPI Energy Co., a Hong Kong-based firm that specializes in solar panels but has diversified its portfolio. One World Ventures placed Benally on its board in March 2019.
One World Ventures CEO DaMu Lin last year issued a news release lauding One World’s relationship with Benally’s company and the San Juan River Farm Board, stating the company was well positioned for the upcoming hemp growing season. Calls to the company and Lin were not returned.
One World Ventures has posted combined losses of $1.48 million the past two years, financial records show. After Benally and Lin struck a deal, they obtained financing from SPI Energy Co., a publicly traded company on the NASDAQ.
SPI launched a hemp business last year and agreed to invest $1.1 million into the Shiprock farms. But investments from SPI dried up last year after Benally’s company failed “to deliver any of the hemp plants” and refused to return an initial instalment of $324,125, SPI financial records show.
SPI officials visited the Shiprock farms after making their first payment by the July 31, 2019, deadline and found “the plants and growing operations appeared to be deficient and not up to industry standards,” according to a company filing. Further, SPI alleges Benally didn’t deliver updates or financial reports as required.
“Finally, NAAC failed to deliver any of the hemp plants by Nov. 30, 2019 … and refused to return the company’s down payment and to make whole the damages the company has suffered,” a filing says.
SPI said Benally’s company also did not respond to two demand letters late last year.
‘Crisis situation’
Benally — whose Facebook page describes him as a “politician” despite his losing races for Navajo Nation president and Congress — claims he’s become a political target.
Benally declined to be interviewed. Benally was scheduled to be a witness during last week’s hearing but didn’t testify. His attorney had a farm owner and a security guard to testify.
Redfeather was among those who testified against Benally. Others included Navajo Nation Environmental Protection Agency Director Oliver Whaley and the tribal police chief. Whaley said in court that during a Sept. 9 visit to one of Benally’s farms, he found septic tanks discharging sewer water into soil and groundwater, pesticides not being properly applied and petroleum leakage. He also said Benally didn’t have permits to operate.
Francisco, the police chief, testified after Whaley and said about a year ago a “crisis situation” began in the community, noting his office has been flooded with calls to maintain peace on the Shiprock farms. All of the calls have taken officers from other emergencies, he said.
Francisco has previously said his agency was working with the Navajo Department of Criminal Investigation and the Bureau of Indian Affairs Division of Drug Enforcement regarding potential criminal violations on the farms.
“It’s a disruption to the community, and the smell is causing problems. And there’s encroachment on people’s land,” Francisco said in court. “There has been discord and unrest.” Residents near the farms said in court that Benally’s crews have flooded their fields, making it impossible to harvest, and destroyed a corn crop with constant dust from Benally’s operation. Loretta Bennett, a 69-year-old farmer, said in court that the workers on Benally’s farms also don’t wear masks, and she’s concerned about the spread of COVID-19.
Arlando Teller, an Arizona state representative from Chinle, said in an interview that while the hemp farms are in New Mexico, he’s concerned about “how the operation has taken place as far as the transparency of a business operation.”
Hemp farms may remain
Benally, a 43-year-old father of four, has said in press releases and on his website that he brought hemp farms to Shiprock as an economic driver, and he’s been successful in partnering with tribal members on his website.
He has paid $2,000 a month to childhood friend and farmer Farley Blueyes to use up to 150 acres of his farm for hemp production.
Blueyes said his land was fallow until Benally put people to work. Security officers were needed because residents have become confrontational.

Hoop houses at a hemp farm are visible from U.S. Highway 64 in Hogback, New Mexico, on Sept. 16, 2020.
NOEL LYN SMITH/THE FARMINGTON DAILY TIMES
Despite Friday’s ruling, the battle is likely not over. Attorneys for Benally say they will pursue “all legal channels” to keep fighting, and many Asian workers remained on the farms after Friday’s ruling.
Sengthong, the Glendale resident, said she went to visit her relatives near Shiprock on Saturday after learning about the court order.
She told The Republic that a hemp farm on a relative’s property, about 10 miles west of Shiprock, was still operating this past weekend. She said when Navajo Nation police visited the site, workers fled the farm. Sengthong was taking pictures of the activity and said after police left, one of the workers tried to “smack” her cellphone and other workers were confrontational. “I’ve been intimidated for what I did,” she said. “They are still working and the camp is huge.”
Benally’s attorneys said the court decision violated their client’s civil rights and put many tribal members out of work. Jordan, Benally’s attorney, declined to say how his client would respond to the court order. Jordan said in court filings that such an order would destroy the “entire crop
Source: https://eu.azcentral.com/story/news/local/arizona/2020/09/22 September 24, 2020
Three decades ago, I would have been over the moon to see marijuana legalized. It would have saved me a lot of effort spent trying to avoid detection, constantly looking for places to hide a joint. I smoked throughout my teens and early 20s. During this period, upon landing in a new city, my first order of business was to score a quarter-ounce. The thought of a concert or a vacation without weed was simply too bleak.
These days it’s hard to find anybody critical of marijuana.
The drug enjoys broad acceptance by most Americans — 63 percent favoured ending cannabis prohibition in a recent Quinnipiac poll — and legislators on both sides of the aisle are becoming more likely to endorse than condemn it. After years of loosening restrictions on the state level, there are signs that the federal government could follow suit: In April, Senate Minority Leader Charles E. Schumer (D-N.Y.) became the first leader of either party to support decriminalizing marijuana at the federal level, and President Trump (his attorney general notwithstanding) promised a Republican senator from Colorado that he would protect states that have legalized pot.
And why not? The drug is widely thought to be either benign or beneficial. Even many of those apathetic toward its potential health benefits are ecstatic about its commercial appeal, whether for personal profit or state tax revenue. Legalization in many cases, and for many reasons, can be a good thing. I’m sympathetic.
But I am also a neuroscientist, and I can see that the story is being oversimplified. The debate around legalization — which often focuses on the history of racist drug laws and their selective enforcement — is astoundingly naive about how the widespread use of pot will affect communities and individuals, particularly teenagers. In our rush to throw open the gate, we might want to pause to consider how well the political movement matches up with the science, which is producing inconveniently alarming studies about what pot does to the adolescent brain.

Marijuana for sale at a Colorado dispensary. (Matthew Staver/Bloomberg Creative Photos)
I took a back-door route to the science of marijuana, starting with a personal investigation of the plant’s effects. When I was growing up in South Florida in the 1980s, pot was readily available, and my appreciation quickly formed the basis for an avid habit. Weed seemed an antidote to my adolescent angst and ennui, without the sloppiness of alcohol or the jaw-grinding intensity of stimulants.
Of the many things I loved about getting high, the one I loved best was that it commuted the voice in my head — usually peevish or bored — to one full of curiosity and delight. Marijuana transformed the mundane into something dramatic: family outings, school, work or just sitting on the couch became endlessly entertaining when I was stoned.
Like any mind-altering substance, marijuana produces its effects by changing the rate of what is already going on in the brain. In this case, the active ingredient delta-9-THC substitutes for your own natural endocannabinoids and mimics their effects. It activates the same chemical processes the brain employs to modulate thoughts, emotions and experiences. These specific neurotransmitters, used in a targeted and judicious way, help us sort the relentless stream of inputs and flag the ones that should stand out from the torrent of neural activity coding stray thoughts, urges and experience. By flooding the entire brain, as opposed to select synapses, marijuana can make everything, including the most boring activities, take on a sparkling transcendence.
Why object to this enhancement? As one new father told me, imbibing made caring for his toddler much more engrossing and thus made him, he thought, a better parent. Unfortunately, there are two important caveats from a neurobiological perspective.
As watering a flooded field is moot, widespread cannabinoid activity, by highlighting everything, conveys nothing. And amid the flood induced by regular marijuana use, the brain dampens its intrinsic machinery to compensate for excessive stimulation. Chronic exposure ultimately impairs our ability to imbue value or importance to experiences that truly warrant it.
In adults, such neuro-adjustment may hamper or derail a successful and otherwise fulfilling life, though these capacities will probably recover with abstinence. But the consequences of this desensitization are more profound, perhaps even permanent, for adolescent brains. Adolescence is a critical period of development, when brain cells are primed to undergo significant organizational changes: Some neural connections are proliferating and strengthening, while others are pared away.
Although studies have not found that legalizing or decriminalizing marijuana leads to increased use among adolescents, perhaps this is because it is already so popular. More teenagers now smoke marijuana than smoke products with nicotine; between 30 and 40 percent of high school seniors report smoking pot in the past year, about 20 percent got high in the past month, and about 6 percent admit to using virtually every day. The potential consequences are unlikely to be rare or trivial.
The decade or so between puberty and brain maturation is a critical period of enhanced sensitivity to internal and external stimuli. Noticing and appreciating new ideas and experiences helps teens develop a sense of personal identity that will influence vocational, romantic and other decisions — and guide their life’s trajectory. Though a boring life is undoubtedly more tolerable when high, with repeated use of marijuana, natural stimuli, like those associated with goals or relationships, are unlikely to be as compelling.
It’s not surprising, then, that heavy-smoking teens show evidence of reduced activity in brain circuits critical for flagging newsworthy experiences, are 60 percent less likely to graduate from high school, and are at substantially increased risk for heroin addiction and alcoholism. They show alterations in cortical structures associated with impulsivity and negative moods; they’re seven times more likely to attempt suicide.
Recent data is even more alarming: The offspring of partying adolescents, specifically those who used THC, may be at increased risk for mental illness and addiction as a result of changes to the epigenome — even if those children are years away from being conceived. The epigenome is a record of molecular imprints of potent experiences, including cannabis exposure, that lead to persistent changes in gene expression and behavior, even across generations. Though the critical studies are only now beginning, many neuroscientists prophesize a social version of Rachel Carson’s “Silent Spring,” in which we learn we’ve burdened our heirs only generations hence.
Might the relationship between marijuana exposure and changes in brain and behavior be coincidence, as tobacco companies asserted about the link between cancer and smoking, or does THC cause these effects? Unfortunately, we can’t assign people to smoking and nonsmoking groups in experiments, but efforts are underway to follow a large sample of children across the course of adolescent development to study the effects of drug exposure, along with a host of other factors, on brain structure and function, so future studies will probably be able to answer this question.
In the same way someone who habitually increases the volume in their headphones reduces their sensitivity to birdsong, I followed the “gateway” pattern from pot and alcohol to harder drugs, leaping into the undertow that eventually swept away much of what mattered in my life. I began and ended each day with the bong on my nightstand as I floundered in school, at work and in my relationships. It took years of abstinence, probably mirroring the duration and intensity of my exposure, but my motivation for adventure seems largely restored. I’ve been sober since 1986 and went on to become a teacher and scholar. The single-mindedness I once directed toward getting high came in handy as I worked on my dissertation. I suspect, though, that my pharmacologic adventures left their mark.
Now, as a scientist, I’m unimpressed with many of the widely used arguments for the legalization of marijuana. “It’s natural!” So is arsenic. “It’s beneficial!” The best-documented medicinal effects of marijuana are achieved without the chemical compound that gets users high. “It’s not addictive!” This is false, because the brain adapts to marijuana as it does to all abused drugs, and these neural adjustments lead to tolerance, dependence and craving — the hallmarks of addiction.
It’s true that a lack of benefit, or even a risk for addiction, hasn’t stopped other drugs like alcohol or nicotine from being legal, used and abused. The long U.S. history of legislative hypocrisy and selective enforcement surrounding mind-altering substances is plain to see. The Marihuana Tax Act of 1937, the first legislation designed to regulate pot, was passed amid anti-Mexican sentiment (as well as efforts to restrict cultivation of hemp, which threatened timber production); it had nothing do with scientific evidence of harm. That’s true of most drug legislation in this country. Were it not the case, LSD would be less regulated than alcohol, since the health, economic and social costs of the latter far outweigh those of the former. (Most neuroscientists don’t believe that LSD is addictive; its potential benefits are being studied at Johns Hopkins and New York University, among other places.)
Still, I’m not against legalization. I simply object to the astounding lack of scepticism about pot in our current debate. Whether or not to legalize weed is the wrong question. The right one is: How will growing use of delta-9-THC affect individuals and communities?
Though the evidence is far from complete, wishful thinking and widespread enthusiasm are no substitutes for careful consideration. Instead of rushing to enact new laws that are as nonsensical as the ones they replace, let’s sort out the costs and benefits, using current scientific knowledge, while supporting the research needed to clarify the neural and social consequences of frequent use of THC. Perhaps then we’ll avoid practices that inure future generations to what’s really important.
By Judith Grisel, May 25, 2018
(Denver, CO) – Today, a new study on the impact of marijuana legalization in Colorado conducted by the Centennial Institute found that for every one dollar in tax revenue from marijuana, the state spends $4.50 as a result of the effects of the consequences of legalization.
This study used all available data from the state on hospitalizations, treatment for Cannabis Use Disorder (CUD), impaired driving, black market activity, and other parameters to determine the cost of legalization. Of course, calculating the human cost of addiction is nearly impossible, we can assume the cost estimated for treating CUD is a gross underestimate due to the fact that it is widely believed among health officials that CUD goes largely untreated…yet rates have been increasing significantly in the past decade.
That, in conjunction with the fact that there is no way of quantifying the environmental impact the proliferation of single use plastic packaging common within the marijuana industry, leads us to believe this is indeed a very conservative estimate.
“Studies such as this show that the only people making money off the commercialization of marijuana are those in the industry who profit at the expense of public health and safety,” said Dr. Kevin Sabet, president of Smart Approaches to Marijuana (SAM). “The wealthy men in suits behind Big Marijuana will laugh all the way to the bank while minority communities continue to suffer, black markets continue to thrive, and taxpayers are left to foot the bill.”
“The data collected in this study, as in similar studies before it, continues to show the scope of the cost of commercialization. The effects of legalization are far and wide, and affect just about every resident in the state directly and indirectly,” said Jeff Hunt, Vice President of Public Policy for Colorado Christian University.
“The pot industry doesn’t want this dirty truth to be seen by law makers and the taxpayers, who were promised a windfall in tax revenue,” said Justin Luke Riley, president of the Marijuana Accountability Coalition. “The MAC will continue to shine a light on the industry and urge our lawmakers to reign in Big Pot before it brings more harm on Coloradans.”
Source: New Colorado Report: Cost of Marijuana Legalization Far Outweighs Tax Revenues – Smart Approaches to Marijuana (learnaboutsam.org) November 2018
DRP0013
1.Aims Cannabis Skunk Sense (also known as CanSS Ltd) provides straight-forward facts and research-based advice on cannabis. We raise awareness of the continued and growing dangers to children, teenagers and their families of cannabis use.
2.We provide educational materials and information for community groups, schools, colleges and universities; and guidance to wide range of professions, Parliament and the general public – with a strong message of prevention not harm reduction.
3.The Inquiry document says: ‘Government’s stated intention in its 2017 drug strategy is to reduce all illicit and other harmful drug use…….’
4.Missing from this Inquiry document is the following 2017 Strategy statement: ‘preventing people – particularly young people – from becoming drug users in the first place’. Prevention should be first and foremost in any statement as well as in the minds of us all. FRANK was mentioned just once in this strategy; ‘develop our Talk to FRANK service so that it remains a trusted and credible source of information and advice for young people and concerned others’. This claim will be challenged in this report.
5.If prevention (pre-event) were to be successful, there would be little need for a policy of reducing harmful use. Unfortunately, for fifteen or sixteen years now, prevention has taken a back seat.
6.In 1995 Prime Minister John Major’s government produced ‘Tackling Drugs Together’ saying, ‘The new programme strengthens our efforts to reduce the demand for illegal drugs through prevention, education and treatment’.
7.Objectives included: ‘to discourage young people from taking drugs’ and to ensure that schools offer effective programmes of drug education, giving pupils the facts, warning them of risks, and helping them to develop the skills and attitudes to resist drug use – all good common sense.
8.On harm reduction, the government said, ‘The ultimate goal is to ensure people do not take drugs in the first place, but if they do, they should be helped to become and remain drug-free. Abstinence is the ultimate goal and harm reduction should be a means to that end, not an end in itself’.
9.In 1998 the Second National Plan for 2001-2, ‘Tackling Drugs to Build a Better Britain’ was published. Although prevention was still the aim, the phrase ‘informed choice’ appeared, the downhill slide from prevention had started.
10.The` Updated Strategy in 2002 contained the first high-profile mention of ‘Harm Minimisation (Reduction)’. David Blunkett in the Foreword said, ‘Prevention, education, harm minimisation, treatment and effective policing are our most powerful tools in dealing with drugs’.
Some bizarre statements appeared, e.g.: ‘To reduce the proportion of people under 25 reporting use of illegal drugs in the last month and previous year substantially’. Is infrequent use of drugs acceptable?
In October 2002 at a European Drugs Conference, Ashford, Kent, Bob Ainsworth, drugs spokesman for the Labour government, said that harm reduction was being moved to the centre of their strategy. Prevention was abandoned, ‘informed choice’ and ‘harm reduction’ ruled.
The official government website for information on drugs is FRANK set up in 2003. It continued with the harm reduction policy of the Labour Government.
From the beginning, FRANK was heavily criticised. The Centre for Social Justice (CSJ), founded by Iain Duncan-Smith MP in 2004, consistently criticised FRANK for being ill-informed, ineffective, inappropriate and shamefully inadequate, whilst citing a survey conducted by national treatment provider Addaction who found that only one in ten children would call the FRANK helpline to talk about drugs. Quite recently, when asked about sources where they had obtained helpful information about alcohol or smoking cigarettes, young people put FRANK at the bottom.
The CSJ recommended that FRANK be scrapped, and an effective replacement programme developed to inform young people about the dangers of drug and alcohol abuse based on prevention rather than harm reduction.
The IHRA (International Harm Reduction Alliance) gives the following definition of harm reduction:
Harm reduction refers to policies, programmes and practices that aim to minimise negative health, social and legal impacts associated with drug use, drug policies and drug laws. Harm reduction is grounded in justice and human rights – it focuses on positive change and on working with people without judgement, coercion, discrimination, or requiring that they stop using drugs as a precondition of support.
The use of Harm reduction instead of Prevention is tantamount to condoning drug use – a criminal activity. The legitimate place for harm reduction is with ‘known users’ on a one to one basis as part of a treatment programme to wean them off completely and attain abstinence in a safer manner than abrupt stoppage which can be very dangerous. One example of this is to inhale the fumes of heroin rather than injection, thus avoiding blood-borne diseases such as AIDS, hepatitis and septicaemia.
An opioid substitute drug for heroin addiction, methadone has the advantage of being taken orally and only once/day. As the dosage is reduced, abstinence will be attained more safely. However, methadone users are often ‘parked’ for months on this highly addictive drug without proper supervision or monitoring. In 2008 in Edinburgh, more addicts died of methadone than heroin.
Harm reduction is a green light. If children are encouraged to use drugs by being given tips on how to use them more safely, many will do it. The son of a friend told his mother. ‘It’s OK we go on to the FRANK website and find out how to take skunk safely by cutting our use and inhaling less deeply’. He is now psychotic!
Prevention works. Between 1997 and 1991 America saw drug use numbers plummet from 23 to 14 million, cocaine and cannabis use halved, daily cannabis use dropped by 75%.
In 2005, Jonathan Akwue of In-Volve writing in Drink and Drugs News, criticised the campaign for lacking authenticity; its ill-judged attempts at humour which try to engage with youth culture; and diluting the truth to accommodate more socially acceptable messages.
The conservatives regained power under David Cameron. FRANK did not change.
In 2005, Mr Iain Duncan Smith again criticised FRANK, saying “Drugs education programmes, such as Talk to FRANK, have failed on prevention and intervention, instead progressively focussing on harm reduction and risk minimisation, which can be counter-productive”
In 2011 it was announced FRANK would be re-launched and the team commissioned ‘A Summary of Health Harms of Drugs’ from The John Moore’s University Liverpool, a hotbed of harm reduction. A psychiatrist from The FRANK Team was involved. Their section on cannabis is totally inadequate, out of date, no recognition of deaths, brain shrinkage, violence, homicides, suicides, the huge increase of strength of THC etc. Professor Sir Robin Murray’s research on mental illness (2009) and the discovery that CBD is virtually absent from skunk are of vital importance.
Many worrying papers have been written since, especially about brain development, all of which are ignored. CanSS met with the FRANK team prior to their re-launch in 2011 where it was agreed that the cannabis section would, with their assistance, be re-written. All but two very small points were ignored, one about driving after taking alcohol with cannabis and the effect on exam results. The harm reduction advice about cannabis was removed at the request of CanSS.
Scientific evidence detailing FRANK’s inaccuracies was given to the Government by CanSS and other drug experts over the years – all of it ignored. Complaints and oral evidence were submitted to the HASC in April and September 2012 and the Education Select Committee in 2014. Government drugs spokesmen have also been contacted with concerns about FRANK.
As the official government source of information on drugs for the UK public, the FRANK site must be regularly updated and contain the many new accurate findings from current scientific research. The public is owed a duty of care and protection from the harm of drugs, especially cannabis, the most commonly used.
The following list contains some of the glaring omissions and vital details from the FRANK website:
Deaths from cancers except lung, road fatalities, heart attacks/strokes, violent crime, homicides, suicides. Tobacco doesn’t cause immediate deaths either.
Alcohol with cannabis can be fatal. An alcohol overdose can be avoided by vomiting but cannabis suppresses the vomiting reflex.
Cases of severe poisoning in the USA in toddlers are increasing, mostly due to ‘edibles’ left within reach. Accidental ingestion by children should be highlighted.
Hyperemesis (violent vomiting) is on the increase.
Abnormally high levels of dopamine in the brain cause psychosis (the first paper on this was written in 1845) and schizophrenia, especially in those with genetic vulnerabilities, causing violence, homicides and suicides. Skunk-induced schizophrenia costs the country around £2 billion/year to treat.
Young people should understand how THC damps down the activities of the whole brain by suppressing the chemical messages for several weeks. It is fat soluble and remains in the cells. Messages to the hippocampus (learning and memory) fail to reach its cells, some die, causing permanent brain damage. IQ points are lost. Few children using cannabis even occasionally will achieve their full potential.
Serotonin is depleted, causing depression and suicides. The huge increase in the strength of THC in cannabis due to the prevalence of skunk (anything from 16% to over 20%) and the almost total lack of CBD is ignored as is the gateway theory, medical cannabis, passive smoking and lower bone mineral density, bronchitis, emphysema and COPD.
They need to be taught that there is reduced ability to process information, self-criticise and think logically. Users lack attention and concentration, can’t find words, plan or achieve routines, have fixed opinions, whilst constantly feeling lonely and misunderstood. They should know of the risk of miscarriages and ectopic pregnancies.
Amazingly, the fact THC damages our DNA is virtually unknown among the public. In the 1990s, scientists found new cells being made in the adult body (white blood, sperm and foetal cells), suffered premature ‘apoptosis’ (programmed cell death) so were fewer in number. Impotence, infertility and suppressed immune systems were reported. This is important.
In 2016 an Australian paper discovered THC badly interferes with cell division i.e. where chromosomes replicate to form new cells. They fail to segregate properly causing numerous mutations as chromosomes shatter and randomly rejoin. Many cells die (about 50% of fertilized eggs (zygotes). Any affected developing foetus will suffer damage. Resultant foetal defects include gastroschisis (babies born with intestines outside the body), now rising in areas of legalisation, anencephaly (absence of brain parts) and shortened limbs (boys are about 4 inches shorter). Oncogenes (cancer-causing) can be switched on. Bladder, testicle and childhood cancers like neuroblastoma have all been reported. The DNA in mitochondria (energy producers in cells) can also be damaged.
Parliament controls the drug laws, so why are the police able to decide for themselves how to deal with cannabis possession?
Proof of the liberalisation of the law on cannabis possession appeared in the new Police Crime Harm Index in April 2016, where it appeared 2nd bottom of the list of priorities. In the following November it fell to the bottom. Class ‘A’ drug possession was immediately above. Possession has clearly become a very low priority. In 2015, Durham Police decided they would no longer prosecute those smoking the drug and growing it ‘for their own use’. Instead, officers will issue a warning or a caution. Then Durham Chief Constable Mike Barton announced that his force will stop prosecuting all drug addicts from December 2017 and plans to use police money to give free heroin to addicts to inject themselves twice a day in a supervised ‘shooting gallery’. This surely constitutes dealing. The police can it seems, alter and ‘soften’ laws at will.
Several weeks ago, I happened to check the FRANK website. Quietly, stealthily and without fanfare, a new version had appeared – completely changed. Absent were the patronising videos, games and jokes. Left were A to Z of Drugs, News, Help and Advice (e.g. local harm reduction information) and Contact.
There is poor grammar, i.e. ‘are’ instead of ‘is’ and ‘effect’ where it should be ‘affect’. Mistakes like these do not enhance its credibility.
The drug information is still inadequate with scant essential detail, little explanation and still out of date. This is especially true of cannabis. THC can stay in the brain for many weeks – still sending out its damping-down signals.
What shocked me though were the following:
Our organisation recently received an email about a call to FRANK requesting advice. A friend, a user who also encouraged others to use as well, had lied in a court case where her drug use was a significant factor. He contacted FRANK about her disregard for the law for a substance that was illegal. The advisor raised his voice whilst stating the friend has the right to do what she wants in her own home and mocked him about calling the police. He was shocked and upset by the response.
Ecstasy – Physical health risks
The ‘NEWS’ consisted of 8 pictures with text. In 2 of the 8 items, opportunity is taken to give more ecstasy harm reduction advice. One is titled, ‘Heading out this weekend with Mandy or Molly?’ This is blatant normalisation. The others aren’t ‘news’ items either, but more information about problems.
The section on each drug entitled, ‘Worried about drug x’ mostly consists of giving FRANK’s number. ‘If you are worried about your use, you can call FRANK on 0300 1236600 for friendly, confidential advice’. Any perceptions that FRANK is anything but a Harm Reduction advice site are dispelled completely.
Mentor International is a highly respected worldwide Prevention Charity. Government-funded Mentor UK is in charge of school drug-education with their programme, ADEPIS (Alcohol and Drug Education and Prevention Information Service). Mentor UK masquerades as a ‘Prevention’ charity but practices ‘Harm Reduction’ and has done so from its inception in 1998. A founding member, Lord Benjamin Mancroft, is currently prominent in the APPG: Drug Policy Reform, partly funded by legaliser George Soros’s Open Society Foundation.
Professor Harry Sumnall of John Moores University Liverpool, a trustee on Mentor UK’s board, signed a ‘Legalisation’ letter in The Telegraph 23rd November 2016 along with the university, Professor David Nutt, The Beckley Foundation, Nick Clegg, Peter Lilley, Transform, Volte-face and other well-known legalisation advocates. Eric Carlin, former Mentor UK CEO (2000-2009), is now a member of Professor David Nutt’s Independent Scientific Committee on Drugs (ISCD). At a July 2008 conference in Vienna, he said “we are not about preventing drug use, we are about preventing harmful drug use”.
Examples of their activities:
The ‘Street Talk’ programme, funded by the Home Office, carried out by the charities Mentor UK and Addaction and completed in March 2012 was aimed to help vulnerable young people aged 10 – 19, to reduce or stop alcohol and drug misuse. Following the intervention, the majority of young people demonstrated a positive intention to change behaviour as follows: “I am confident that I know more about drugs and alcohol and can use them more safely in the future” – 70% agreed, 7% disagreed’.
Two CanSS members attended a Mentor UK meeting on 7th January 2014 at Kent University, where Professor Alex Stevens, a sociology professor favouring the opening of a ‘coffee shop’ in Kent and supporting ‘grow your own’ was the main speaker. The audience consisted mainly of young primary school teachers. He became increasingly irritated as CanSS challenged his views, becoming incandescent when told knowledge of drug harms is the most important factor in drug education. The only mention of illegality (by CanSS) was met by mirth!
In a Mentor UK project ‘Safer at school’ (2013), the greatest number of requests from pupils, by 5 to 6 times, were: – effects of drugs, side-effects, what drugs do to your body and consequences. Clearly it had been ignored. Coggans 2003 said that, ‘the life skills elements used by Mentor UK may actually be less important than changing knowledge, attitudes and norms by high quality interactive learning’.
Paul Tuohy, the Director of Mentor UK in February 2013 emailed CanSS, ‘Harm reduction approaches are proven and should be part of the armoury for prevention……..there are many young people harming their life chances who are already using and need encouragement to stop, or where they won’t, to use more safely’.
In 2015 Mentor incorporated CAYT (Centre for Analysis of Youth Transitions) with their ‘The Climate Schools programmes’. Expected Outcomes: ‘To show that alcohol and drug prevention programmes, which are based on a harm minimisation approach and delivered through the internet, can offer a user-friendly, curriculum-based and commercially-attractive teaching method’.
In November 2016, Angelus and Mentor UK merged, ‘The Mentor-Angelus merger gives us the opportunity to reach a wider audience through the delivery of harm-prevention programs that informs young people of the harms associated with illicit and NPS drug-taking, to help support them in making conscientious healthy choices in the future’.
The under-developed brains in young people are quite incapable of making reasoned choices. Nor should they. Drug-taking is illegal.
Michael O’Toole (CEO 2014 –2018) said in an ACMD Briefing paper.
‘Harm reduction may be considered a form of selective prevention – reducing frequency of use or supporting a narrowing range of drugs used’. “It is possible to reduce adverse long-term health and social outcomes through prevention without necessarily abstaining from drugs”.
It is a puzzle that any organisation, including the Government, can condone drug-taking, an illegal activity, either by testing drugs or dishing out harm reduction advice, without being charged with ‘aiding and abetting’ a crime.
Mary Brett, Chair CanSS and Lucy Dawe,Administrator CanSS www.cannabisskunksense.co.uk
Source: http://data.parliament.uk/writtenevidence/committeeevidence.svc/evidencedocument/health-and-social-care-committee/drugs-policy/written/97965.html March 2019


More than 1 million packets of a dangerous, unpredictable new breed of drug were seized in the Houston area by the DEA in the past two years, yet criminal charges are rare for those who make, sell or use them.
The packets, sold as potpourri or incense, are among the more popular brands of so-called synthetic marijuana taking center stage in a new front in the war on drugs.
On a recent afternoon, glossy packets of strawberry-flavored “Kush” lay side by side in a lighted glass display case, just past the bongs and pipes, at a Houston-area shop. The mixture inside looks like dried, finely crushed green leaves. It is smoked like pot but packs a far different punch – and is fueling the never-ending search for ways to get high.
“This is a new frontier for drugs and drug traffickers,” said Rusty Payne, a spokesman for the Drug Enforcement Administration. “I want to shout it from the roof tops: This is nasty stuff.”
Despite pressure from law enforcement, users still don’t have to go to underground dealers to score. Instead, they just visit smoke shops and convenience stores that sell the products.
Houston has a key role in the popularity of the drugs. It is not only a large marketplace for them, but they are covertly made here and shipped to other regions, according to court documents.
Doctors said the substances – technically classified as synthetic cannabinoids – can be aggressive, unstable and damaging.
Hearts race. Blood pressure soars. Seizures can be unleashed.
Paranoia is known to grip some users, as well as agitation and suicidal tendencies that can last five or six hours and land them in emergency rooms.
“They come in, and they are wild and psychotic and sometimes have a distinct smell,” said Dr. Spencer Greene, director of medical toxicology for Baylor College of Medicine. “They are going to be kind of wild and kind of crazy, and potentially very sick.”
Part of the problem is that the potency of the drugs can vary so greatly, and that users can never be sure what they are smoking.
Emily Bauer, a 17-year-old former user who lives in Cypress, learned just how bad they can be on a Friday night in 2012.
She smoked a packet, as she had done many times before, and ended up suffering what her family has been told was a series of strokes.
“I am improving constantly, and my vision is getting better,” she said, noting that she continues with high school thanks to people who read textbooks aloud to her and help her write.
Bauer and her parents have been sharing her story publicly in hopes that others will avoid the drugs. She said it just is not accurate to compare what she smoked to marijuana.
“It is more like smoking bleach,” she said.
Banned at trade shows
They come in colorful packets with dozens of other brand names, including Scooby Snax and Hello Kitty. The packages look like packets of candy and cost from $6 to $20, depending on the size.
They carry warnings that the contents are not for human consumption and sometimes incorrectly note contents are legal.
Authorities contend the language is just an attempt to dodge state and federal laws.
In schemes reminiscent of the popular crime drama “Breaking Bad,” rogue chemists repeatedly tweak compounds to create new generations of designer drugs faster than laws can catch them.
“Trained chemists know exactly what they are doing,” said Jeff Walterscheid, a toxicologist with the Harris County Institute of Forensic Sciences.
He noted that tweaking one molecule can make a new drug.
Dozens of such deviations of synthetic cannabinoids have been identified in the past few years, according to the DEA, and the list of what is out there is believed to be growing weekly.
To prepare the drugs for consumption, chemicals – usually white powdery mixtures – are often imported from China where they were prepared by chemists who keep an eye on U.S. laws, according to the DEA.
After U.S.-based manufacturers get those chemicals, they are often dissolved in acetone and then sprayed over leafy material, dried and spritzed with flavors such as grape, strawberry or cherry. Then they are poured into packages that are delivered in bulk to stock the shelves of retailers.
A manufacturing operation in Stafford was shut down by police in September after five day laborers staggered to an ambulance company looking for help. They had been overcome by fumes.
The factory was in an industrial park and a few hundred yards from a day care center. All that was left behind on a recent visit to the site was a scattering of crushed leaves in a carpeted office and a small black and blue packet labeled Amsterdam Dreams Potpourri.
Manufacturers of these substances aren’t considered nearly as violent as drug-cartel gangsters, but turf wars flare up.
Authorities point to a brutal dispute between two manufacturers. One stormed into the other’s business on Harwin, doused him with gasoline, and threatened to set him ablaze if he didn’t stop stealing a brand name.
The dispute faded. No one was arrested.
Jeff Hirschfeld, president of Champs, which holds national trade shows for thousands of smoke shop owners, said two years ago he decided to ban synthetic marijuana vendors from his events.
“There are so many states that don’t allow it, we just did not think it was proper,” he said.
“I am a grandfather of six, and I would not really recommend it for my grandkids,” he said. “I have not tried it, but I know people who have. Some say good, some say bad, but I’m not comfortable with it.”
Users vary from high school kids to working professionals. The drug also doesn’t show up in urine tests for marijuana, which might appeal to people on parole or job applicants.
Not meant for humans
In the past two years in Houston, synthetic cannabinoids were in the system of a person who hanged himself, another who was hit by an allegedly drunken driver while walking along a tollway, and another who was shot to death, according to the Harris County Institute of Forensic Sciences.
Users are playing roulette with their lives, said Walterscheid, the Harris County toxicologist.
“You cannot look at a container of Kush Apple and know what is in it,” he said. “When buying a package that looks the same every day for a year, you could be getting something different every single time.”
John Huffman, a South Carolina chemist who years ago led a team that developed synthetic cannabinoids while researching under a federal grant, said some strains now being copied could easily be 50 times more potent than marijuana.
“They are all dangerous. Don’t use them,” said Huffman, who retired four years ago. “They were never designed for this.”
The substances were tested on animals but were never to be used by humans.
Criminal charges rarely are filed as cases involving these emerging drugs bring on a host of new scientific, medical and legal complexities.
Clinical tests have not yet been conducted on humans on any of these drugs, so it can be tough to prove the extent of their harm. Experts could also clash over whether the ingredients of a given drug make it illegal, among other issues.
People who knowingly make or sell synthetic cannabinoids for human consumption can face federal charges. Possession of some of those substances, regardless of weight, can in some cases be a misdemeanor in Texas.
“We have been taking an active role trying to classify more of these, make more of them fall in the penal code,” said Marcy McCorvey, division chief of the major narcotics division of the Harris County District Attorney’s Office.
She said that prosecutors are handcuffed by insufficient laws, but if they can make a case, they will take it to court.
“It is very frustrating. I know of police officers who are out there trying to combat the problem,” McCorvey said. “I understand parents who want it off the shelves. I wish I could prosecute sellers and suppliers in a more harsh manner, but the state law does not allow for a harsher penalty as it is written.”
Few criminal charges
Despite the DEA seizing more than 1 million packets of the drugs, as well as the pending forfeitures of more than $8 million, federal prosecutors in Houston have yet to charge anyone, according to officials.
The U.S. Attorney for the Southern District of Texas, who is based in Houston, declined to comment.
In June, federal authorities in San Antonio announced Operation Synergy. At least 17 people were arrested in San Antonio, Houston and elsewhere for alleged roles in a synthetic cannabinod ring.
In another case, Houston resident Issa Baba was charged federally in Pennsylvania with using the Web to sell synthetic pot and other designer drugs. More than $5 million was seized from his bank accounts. Baba has signed a guilty plea.
Another Houston-area man has not been charged with a crime, but more than $2 million was taken from him in May on the grounds that it was proceeds from making synthetic cannabinoids. Bundles of $100 bills wrapped in rubber bands were stashed at his ex-wife’s home in La Marque.
Lawyer Chip Lewis, who represents Baba and the other man, said the cases against his clients come at a tricky time, as the Department of Justice has decided not to challenge laws that permit the medical and recreational use of marijuana.
“It is a slippery slope we are on here,” Lewis said. “Yes, we will prosecute you for this. No, we are not going to prosecute you for something else on the books.”
Javier Pena, chief of the DEA’s Houston Division, said getting this breed of drugs off the streets has become a moral mission as much as a legal one.
“We are trying to say to store owners: You know who you are. You need to stop selling this poison.”
Source: https://www.houstonchronicle.com/news/investigations/article/Houston-gains-key-role-in-synthetic-marijuana-5024607.php November 2013
An investor in a major Canadian cannabis company has had longstanding ties, including business dealings, with influential Mafia members and drug traffickers, Radio-Canada has learned.
Another investor in the same company has links with a prominent member of the Rizzutos, the powerful Montreal crime family.
In still another case, an individual managed to sell his cannabis business to one of the big players in the industry, despite his connections to drug traffickers. In return, he received shares in the company and rented out space for a cannabis grow-op.
Prime Minister Justin Trudeau’s legalization plan was supposed to cut out organized crime, but an investigation by Radio-Canada’s Enquête shows Health Canada has granted production licences to companies with individuals with links to the criminal underworld.
Enquête examined hundreds of documents as part of its investigation, including reviews conducted by Canadian securities oversight bodies. Enquête is not naming the companies or individuals involved.
For its part, Health Canada says it has not seen any cases of organized crime infiltration of more than 130 licensed cannabis producers since 2013.
To produce cannabis, those who hold certain positions in companies must first obtain a permit from Health Canada by taking a security screening.
Any past connections with individuals related to organized crime are part of the analyzed information.
To secure a licence, Health Canada first checks if the individual has a criminal record.
Second, the RCMP consults police databases to review information that may indicate an applicant’s links to criminals.
Health Canada makes its final decision with the information provided by the RCMP.
The RCMP says it raised red flags on about 10 per cent of the applicants it was asked to check out in 2016 and 2017.
“It’s really criminal associations,” says Supt. Yves Goupil, who gives the example of a person “associated with individuals who have criminal records.”
In a statement, Health Canada said it can “categorically confirm” that it didn’t issue “security clearance to an individual when the RCMP provided evidence to the department that it was associated with organized crime.”
“Health Canada has found no evidence that organized crime has infiltrated one of more than 130 federally registered producers,” spokesperson Eric Morrissette said in an email.
Throughout the period in which Canada’s cannabis industry was developing, primarily for medical purposes, only individuals who directly ran the companies were required to obtain a security clearance.
This approach, says Conservative Senator Claude Carignan, demonstrates a naiveté about the workings of high-level organized crime.
“If there is someone who has a criminal record, it is not that person they will put to apply for the licence,” Carignan said. “It would be completely naive to think that.”
Last spring, Carignan and his Senate colleagues tried, unsuccessfully, to amend Bill C-45 on the legalization of cannabis in order to demand more transparency from companies entering the industry.
Several companies have opaque and complex structures.
“You never see who the real licence holders are,” said lawyer and tax expert Marwah Rizqy, who raised the issue before a Senate committee last spring and has since been elected Liberal MNA for the Quebec riding of Saint-Laurent.
It’s not uncommon for cannabis companies to be funded through family trusts.
Originally designed for estate and tax planning, trusts are an ideal way to hide individuals with interests in a business, said Marie-Pierre Allard, who studies tax policy at the Université de Sherbrooke.
“The beneficiaries of the trust are not disclosed publicly. It’s anonymous,” she said, adding that it is “one of the great vulnerabilities of the Canadian legal system.”
“If we want to eliminate the Mafia cannabis market, we cannot allow them to use tax havens or trusts to enter indirectly through the back door,” Carignan said.
A report by the federal Department of Finance and several international organizations identifies trusts as one of the vehicles most at risk for money-laundering in Canada.
In a Senate appearance last April, Rizqy suggested refusing to grant production licences to companies financed through trusts.
“Maybe it would be wise to deny the licence outright because you are not able to unequivocally establish that the security clearance is really valid,” said Rizqy.
The recommendation was not accepted. The federal cannabis legislation adopted this summer, however, did include more extensive background checks into individuals who back cannabis companies.
Carignan has faced criticism for his efforts to make cannabis companies more transparent.
Line Beauchesne, a criminologist at the University of Ottawa, believes Health Canada’s investigations are adequate and consistent with the government’s desire to ensure the quality of the product and to prevent smuggling.
“Why especially for the cannabis industry?” Beauchesne asked.
If there were to be new rules of transparency, “all industries moving into Canada” should be affected, she said.
She acknowledged, however, that Health Canada “is absolutely not equipped to conduct financial investigations.”
Its traditional role is to ensure a product meets certain standards.
“Health Canada’s job is to make sure that when I eat cheese, it’s cheese. When it’s eggs, it’s eggs. And when [it comes to] cannabis, it’s cannabis.”
The number of audits to be conducted in the cannabis industry is so great investigators have to make choices, said the RCMP’s Goupil.
The work of police is complicated considerably when the sources of financing for businesses come from abroad, including from tax havens.
“Technically, there is nothing illegal there. But it’s hard for [the RCMP] and for Health Canada to go out and check in those countries,” he said.
“Often, it’s going to be the janitor who will sign the company documents or a law firm in country X. At some point, we cannot do the research. It’s a lot of investment, a lot of time, a lot of money,” Goupil said.
“We cannot have a fully bulletproof system. If organized crime has an opportunity to make a profit, it will exploit it. “
Tax havens are not the only barrier to police work. Secrecy also exists in some companies in Canada.
“We need to use other more advanced techniques such as physical surveillance and wiretapping that will help us identify who is behind the company and who operates it,” he said.
These survey techniques, however, require considerable resources and cannot be deployed for all cannabis companies.
“We cannot afford it.”
Source: Licensed cannabis growers have ties to organized crime, Enquête investigation finds | CBC News November 2018
The fact that 1 in 6 infants and toddlers admitted to a Colorado hospital with symptoms of bronchiolitis tested positive for marijuana exposure should concern Canadians as they move to legalization on 17 October. The dangers of 2nd-hand, carcinogenic and psychoactive chemically-laden marijuana smoke were ignored by the Trudeau government in its push to legalize pot, Pamela McColl writes.
PAMELA McCOLL’S STATEMENT IN FULL…
What About Us? October 17 2018
No amount of second-hand smoke is safe. Children exposed to second-hand smoke are more likely to develop lung diseases and other health problems. Second hand-smoke is a cause of sudden infant death syndrome (SIDS). The fact that one in six infants and toddlers admitted to a Colorado hospital with symptoms of bronchiolitis tested positive for marijuana exposure should be of grave to Canadians as they too have moved to legalization.
The dangers of second-hand, carcinogenic and psychoactive chemically-laden marijuana smoke were ignored by the Trudeau government in their push to legalize pot. This government in fact sanctioned the smoking of marijuana in the presence of children.
The government did not commission an in-depth child risk assessment of the draft legalization framework, a study called for by child advocates across the country.
The Alberta Ministry of Children’s Services’ – Child, Youth and Family Enhancement Act Placement Resource Policy on Environmental Safety states; that a foster parent must be aware of, and committed to provide a non-smoking environment by not allowing smoking in the home when a foster child is placed; not allowing smoking in a vehicle when a foster child is present; and not allowing use of smokeless tobacco when a foster child is present. As the Alberta government’s policy contains all-inclusive language of “non-smoking environment,” the same rules have been extend to legalized marijuana. Some children in the province of Alberta have been protected under policy while the majority of Albertan children and other children in Canada should rightly ask: “What About Us?”
The Canadian Charter of Rights and Freedoms secures the safety of children from threats to their health and their life. Section 15 of the Charter prohibits discrimination perpetrated by the governments of Canada. The Equality Rights section states that every individual is equal before and under the law and has the right to the equal protection and equal benefit of the law without discrimination. The provisions that protect children in foster care should extend to every child.
Section 7 of the Charter is a constitutional provision that protects an individual’s personal legal rights from actions of the government of Canada, the right to life, liberty and security of the person. The Cannabis Act fails to protect Canadian children’s right to security of the self. The right to security of the person consists of the rights to privacy of the body and its health and of the right protecting the “psychological integrity” of an individual. Exposure to marijuana in poorly ventilated spaces exposes the non-user to the impact of a psychotropic high, including the distortion of one’s sense of reality.
Canada is a party to the Rights of the Child Treaty, the most widely ratified piece of human rights law in history. The treaty establishes the human rights of children to health and to protection under law. Placing marijuana products and plants into children’s homes fails to protect their rights under international treaty obligations.
A petition, before the BC Government Legislative Assembly via the Minister of Municipal Affairs and Housing, seeks to make all multi-unit dwellings in BC smoke-free. Smoke-free housing is needed to protect the non-user’s health. Smoke travels, it escapes and contaminates beyond a single unit. Law consists, primarily, in preserving a person from death and violence and in securing their free enjoyment of their property. The Cannabis Act fails to preserve the rights of non-users of marijuana. It rests with citizens to stand up for their rights and those of children. Be prepared this will be an ugly, costly and lengthy process.
“We think that the true rule of law is, that the person who for his own purposes brings on his land and collects and keeps there anything likely to do mischief if it escapes, must keep it at his peril, and, if he does not do so, is prima facia answerable for all the damage which is the natural consequence of its escape. “ House of Lords Rule. Doctrine of Strict Liability of Dangerous Conditions Rylands versus Fletcher – 1868. Successful argued in Delta, Canada 1983. Individual prevented from smoking in his residence.
Provincial governments can correct the mistakes made by the federal government. Concerned citizens must see that they do.
Pamela McColl – www.cleartheairnow.org
Source: What about the children? | DB Recovery Resources October 2018
This Notice of Liability Memo and attached Affidavit of Harms give formal notification to all addressees that they are morally, if not legally liable in cases of harm caused by making toxic marijuana products legally available, or knowingly withholding accurate information about the multiple risks of hemp/marijuana products to the Canadian consumer. This memo further gives notice that those elected or appointed as representatives of the people of Canada, by voting affirmatively for Bill C45, do so with the knowledge that they are breaching international treaties, conventions and law. They do so also with the knowledge that Canadian law enforcement have declared that they are not ready for implementation of marijuana legalization, and as they will not be ready to protect the lives of Canadians, there may arise grounds for a Charter of Rights challenge as all Canadian citizens are afforded a the right to security of self.
Scientific researchers and health organizations raise serious questions about the safety of ingesting even small amounts of cannabinoids. Adverse effects include risk of harm to the cardio-vascular system, respiratory tract, immune system, reproductive and endocrine systems, gastrointestinal system and the liver, hyperemesis, cognition, psychomotor performance, psychiatric effects including depression, anxiety and bipolar disorder, schizophrenia and psychosis, a-motivational syndrome, and addiction. The scientific literature also warns of teratogenicity (causing birth deformities) and epigenetic damage (affecting genetic development) and clearly establishes the need for further study. The attached affidavit cites statements made by Health Canada that are grounded in scientific evidence that documents many harms caused by smoking or ingesting marijuana.
Putting innocent citizens in “harm’s way” has been a costly bureaucratic mistake as evidenced by the 2015 Canadian $168 million payout to victims of exposure to the drug thalidomide. Health Canada approved thalidomide in 1961 to treat morning sickness in pregnant women but it caused catastrophic birth defects and death.
It would be instructive to reflect on “big tobacco” and their multi-billion-dollar liability in cases of misinformed sick and dead tobacco cigarette smokers. Litigants won lawsuits for harm done by smoking cigarettes even when it was the user’s own choice to obtain and smoke tobacco. In Minnesota during the 1930’s and up to the 1970’s tobacco cigarettes were given to generally healthy “juvenile delinquents’ incarcerated in a facility run by the state. One of the juveniles, now an adult, who received the state’s tobacco cigarettes, sued the state for addicting him. He won.
The marijuana industry, in making public, unsubstantiated claims of marijuana safety, is placing itself in the same position, in terms of liability, as the tobacco companies.
In 1954, the tobacco industry published a statement that came to be known during Minnesota’s tobacco trial as the “Frank Statement.” Tobacco companies then formed an industry group for the purposes of deceiving and confusing the public.
In the Frank Statement, tobacco industry spokesmen asserted that experiments linking smoking with lung cancer were “inconclusive,” and that there was no proof that cigarette smoking was one of the causes of lung cancer. They stated, “We believe the products we make are not injurious to health.” Judge Kenneth Fitzpatrick instructed the Minnesota jurors: “Jurors should assume in their deliberations that tobacco companies assumed a “special duty” by publishing the ad (Frank Statement), and that jurors will have to determine whether the industry fulfilled that duty.” The verdict ruled against the tobacco industry.
Effective June 19, 2009, marijuana smoke was added to the California Prop 65 list of chemicals known to cause cancer. The Carcinogen Identification Committee (CIC) of the Office of Environmental Health Hazard Assessment (OEHHA) “determined that marijuana smoke was clearly shown, through scientifically valid testing according to generally accepted principles, to cause cancer.”
Products liability and its application to marijuana businesses is a topic that was not discussed in the Senate committee hearings. Proposition 65, requires the State to publish a list of chemicals known to cause cancer, birth defects or other types of reproductive harm. Proposition 65 requires businesses to provide their customers with notice of these cancerous causing chemicals when present in consumer products and provides for both a public and private right of action.
The similarities between the tactics of “Big Tobacco” and the “Canadian Cannabis Trade Alliance Institute” and individual marijuana producers would seem to demand very close scrutiny. On May 23, a witness testified before the Canadian Senate claimed that marijuana is not carcinogenic. This evidence was not challenged.
The International Narcotics Control Board Report for 2017 reads: “Bill C-45, introduced by the Minister of Justice and Attorney General of Canada on 13 April 2017, would permit the non-medical use of cannabis. If the bill is enacted, adults aged 18 years or older will legally be allowed to possess up to 30 grams of dried cannabis or an equivalent amount in non-dried form. It will also become legal to grow a maximum of four cannabis plants, simultaneously for personal use, buy cannabis from licensed retailers, and produce edible cannabis products. The Board wishes to reiterate that article 4 (c) of the 1961 Convention restricts the use of controlled narcotic drugs to medical and scientific purposes and that legislative measures providing for non-medical use are in contravention of that Convention….
The situation pertaining to cannabis cultivation and trafficking in North America continues to be in flux owing to the widening scope of personal non-medical use schemes in force in certain constituent states of the United States. The decriminalization of cannabis has apparently led organized criminal groups to focus on manufacturing and trafficking other illegal drugs, such as heroin. This could explain why, for example, Canada saw a 32 per cent increase from 2015 to 2016 in criminal incidents involving heroin possession….The Canadian Research Initiative in Substance Misuse issued “Lower-risk cannabis use guidelines” in 2017. The document is a health education and prevention tool that acknowledges that cannabis use carries both immediate and long-term health risks.”
Upon receipt of this Memo and Affidavit, the addressees can no longer say they are ignorant or unaware that promoting and/or distributing marijuana cigarettes for recreational purposes is an endangerment to citizens. Receipt of this Memo and Affidavit removes from the addressees any claim of ignorance as a defense in potential, future litigation.
Pamela McColl www.cleartheairnow.org
AFFIDAVIT May 27, 2018
I, Pamela McColl, wish to inform agencies and individuals of known and potential harm done/caused by the use of marijuana (especially marijuana cigarettes) and of the acknowledgement the risk of harm by Health Canada.
Marijuana is a complex, unstable mixture of over four hundred chemicals that, when smoked, produces over two thousand chemicals. Among those two thousand chemicals are many pollutants and cancer-causing substances. Some cannabinoids are psychoactive, all are bioactive, and all may remain in the body’s fatty tissues for long periods of times with unknown consequences. Marijuana smoke contains carcinogenic (cancer-causing) substances such as benzo(a)pyrene, benz(a)anthracene, and benzene in higher concentrations than are present in tobacco smoke. The mechanism by which benzo(a)pyrene causes cancer in smokers was demonstrated scientifically by Denissenko MF et al. Science 274:430-432, 1996.
Health Canada Consumer Information on Cannabis reads as follows: “The courts in Canada have ruled that the federal government must provide reasonable access to a legal source of marijuana for medical purposes.”
“Cannabis is not an approved therapeutic product and the provision of this information should not be interpreted as an endorsement of the use of cannabis for therapeutic purposes, or of marijuana generally, by Health Canada.”
“Serious Warnings and Precautions: Cannabis (marihuana, marijuana) contains hundreds of substances, some of which can affect the proper functioning of the brain and central nervous system.”
“The use of this product involves risks to health, some of which may not be known or fully understood. Studies supporting the safety and efficacy of cannabis for therapeutic purposes are limited and do not meet the standard required by the Food and Drug Regulations for marketed drugs in Canada.”
Health Canada – “When the product should not be used: Cannabis should not be used if you:-are under the age of 25 -are allergic to any cannabinoid or to smoke-have serious liver, kidney, heart or lung disease -have a personal or family history of serious mental disorders such as schizophrenia, psychosis, depression, or bipolar disorder-are pregnant, are planning to get pregnant, or are breast-feeding -are a man who wishes to start a family-have a history of alcohol or drug abuse or substance dependence Talk to your health care practitioner if you have any of these conditions. There may be other conditions where this product should not be used, but which are unknown due to limited scientific information.
Cannabis is not an approved therapeutic product and the provision of this information should not be interpreted as an endorsement of the use of this product, or cannabis generally, by Health Canada.”
Prepared by Health Canada Date of latest version: February 2013, accessed May 2018. https://www.canada.ca/en/health-canada/services/drugs-health-products/medical-use-marijuana/information-medical-practitioners/information-health-care-professionals-cannabis-marihuana-marijuana-cannabinoids.html
A report published by survey company RIWI Corp. (RIWI.com) can be found at: https://riwi.com/case-study/measuringcanadians-awareness-of-marijuanas-health-effects-may-2018
The report measures Canadians’ awareness of marijuana’s health effects as determined by Health Canada and published on Health Canada’s website. RIWI data indicates: 1. More than 40% of those under age 25 are unaware that marijuana impacts safe driving. Further, 21% of respondents are not aware that marijuana can negatively impact one’s ability to drive safely. Health Canada: “Using cannabis can impair your concentration, your ability to make decisions, and your reaction time and coordination. This can affect your motor skills, including your ability to drive.” 2. One in five women aged 25-34 believes marijuana is safe during pregnancy, while trying to get pregnant, or breastfeeding. • RIWI: “For women of prime childbearing age (25-34), roughly one in five believe smoking marijuana is safe during pregnancy, planning to get pregnant, and breastfeeding.” • Health Canada: “Marijuana should not be used if you are pregnant, are planning to get pregnant, or are breastfeeding. … Long-term use may negatively impact the behavioural and cognitive development of children born to mothers who used cannabis during pregnancy.” 3. One in three Canadians do not think that marijuana is addictive. • Health Canada: “Long term use may result in psychological dependence (addiction).” 4. One in three Canadians believe marijuana aids mental health. • Health Canada: “Long term use may increase the risk of triggering or aggravating psychiatric and/or mood disorders (schizophrenia, psychosis, anxiety, depression, bipolar disorder).” 5. One in two males were unaware that marijuana could harm a man’s fertility • “Marijuana should not be used if you are a man who wishes to start a family.”
ClearTheAirNow.org, a coalition of concerned Canadians commissioned the survey.
Affiant is willing to provide further sources of information about the toxicity of marijuana.
Pamela McColl
Source: From email sent to Drug Watch International May 2018
The Internet hosts many unregulated marketplaces for otherwise regulated products. If extended to marijuana (or cannabis), online markets can undermine both the U.S. Controlled Substances Act, which bans marijuana sales, and the regulatory regimes of states that have legalized marijuana. Consequently, regardless of the regulatory regime, understanding the online marijuana market should be a public health
priority. Herein, the scale and growth trajectory of the online marijuana marketplace was assessed for the first time by analyzing aggregate Internet searches and the links searchers typically find.
METHODS
First, the fraction of U.S. Google searches including the terms marijuana, weed, pot, or cannabis relative to all searches was described monthly from January 2005 through June 2017 using data obtained from Google. Searches were also geotagged by state (omitting Alaska, Montana, North Dakota, South Dakota, Vermont, West Virginia, and Wyoming because of data access restrictions). The subset of shopping searches was then monitored by tracking queries that also included buy, shop, and order (e.g., buy marijuana) in aggregate. Searches that included killer, cooking, or clay (e.g., weed killer) were considered unrelated and excluded from all analyses.
Linear regressions were used to compute pooled means to compare between time periods and log-linear regressions were used to compute average growth. Raw search volumes were estimated based on total Google search volume using comScore (www.comscore.com).
Searches in a Google Chrome browser without cached data were executed during July 2017 using the 12 combinations of marijuana and shopping root terms (i.e., buy marijuana). The results would be indicative of a Google user’s typical search results. The first two pages of links, including duplicates (N¼279, with seven to 12 links per page), were analyzed (because nearly all searchers click a link on the first two pages, with as much as 42% selecting the first link). Investigators recorded whether each linked site advertised mail-order marijuana (excluding local deliveries in legal marijuana states) and its order in the search results. Two authors agreed on all labels. Analyses were computed using R, version 3.4.1.
RESULTS
Marijuana searches grew 98% (95% CI¼84%, 113%) as a proportion of all searches from 2005 through the partial 2017 year (Figure 1). The subset of marijuana searches indicative of shopping grew more rapidly over the same period (199%, 95% CI¼165%, 243%), with 1.4–2.4
million marijuana shopping searches during June 2017. Marijuana shopping searches were highest in Washington, Oregon, Colorado, and Nevada. The compounding annual growth rate for marijuana shopping searches since 2005 was significantly positive (po0.05) in 42 of
the 44 studied locations (all but Alabama and Mississippi), suggesting demand is growing across the nation. Forty-one percent (95% CI¼35%, 47%) of shopping search results linked to retailers promising mail-order marijuana (Table 1). Retailers occupied 50% (95% CI¼42%, 59%) of the first page results and for eight (of 12) searches, the first link led to a mail-order marijuana retailer. For some searches (e.g., order marijuana), all of the first-page links were marijuana retailers.
Table 1: Online Mail-Order Marijuana Retailers on Internet Search Engines, 2017
| Search results | ||||
| Retailer | First link | First page | Second page | Total |
| Yes | 8 (67) | 66 (50) | 48 (32) | 114 (41) |
| No | 4 (33) | 65 (50) | 100 (68) | 165 (59) |
Note: Data were collected by executing searches in July 2017. Cells show the frequency and percent of links (by column) in the first two
pages of Google search results that claim to sell mail-order marijuana in response to 12 searches that contained unique combinations of the
following terms: cannabis, marijuana, pot, or weed with buy, order, or shop, such as buy cannabis, buy marijuana, buy pot, or buy weed.
Searches were executed on a new Google browser without cached data. Two authors agreed on the labels 100% of the time.
DISCUSSION
Millions of Americans search for marijuana online, and websites where marijuana can be purchased are often the top search result.
If only a fraction of the millions of searches and thousands of retailers are legitimate, this online marketplace poses a number of potential public health consequences. Children could purchase marijuana online. Marijuana could be sold in states that do not currently allow it.
 Initiation and marijuana dependence could increase. Products may have inconsistent potency or be contaminated. State and local tax revenue (which can fund public health programs) could be negatively impacted.
Initiation and marijuana dependence could increase. Products may have inconsistent potency or be contaminated. State and local tax revenue (which can fund public health programs) could be negatively impacted.
Regulations governing online marijuana markets (even if policy changes favor legalized marijuana) need to be developed and enforced. Policing online regulations will require careful coordination across jurisdictions at the local, state, and federal level with agreements on how to implement regulations where enforcement regimes conflict. Online sales are already prohibited under virtually every regulatory regime—all sales are illegal under federal statute and legal marijuana states like Colorado ban online sales—yet the market appears to be thriving.
Government agencies might work with Internet providers to purge illicit marijuana retailers from search engines, similar to how Facebook removes drug-related pages. Moreover, online payment facilitators could refuse to support marijuana-related online transactions.
This study was limited in that who is buying/selling and the quantity of marijuana exchanged cannot be measured. Further, some searches may be unrelated to seeking marijuana retailers, and some retailers may be illegitimate, including scams or law enforcement bait. The volume of searches and placement of marijuana retailers in search results is a definitive call for public health leaders to address the previously unrecognized dilemma of online marijuana.
ACKNOWLEDGMENTS
This work was supported by a grant from the National Institutes of Mental Health (R21MH103603). Mr. Caputi acknowledges scholarships from the Joseph Wharton Scholars and the George J. Mitchell Scholarship programs. Dr. Leas acknowledges a training grant from the National Heart, Lung, and Blood Institute (T32HL007034). No other financial disclosures were reported by the authors of this paper.
Source: Online Sales of Marijuana: An Unrecognized Public Health Dilemma – American Journal of Preventive Medicine (ajpmonline.org) March 2018
National Drug Intelligence Center
North Carolina Drug Threat Assessment
April 2003
Marijuana is the most readily available and widely abused drug in North Carolina. Marijuana is abused by individuals of various ages in North Carolina. Outdoor cannabis cultivation is widespread in the state. Indoor cultivation occurs to a lesser extent. Mexican criminal groups, the dominant wholesale distributors of marijuana in the state, transport multiton shipments of Mexico-produced marijuana into North Carolina in tractor-trailers, primarily from Mexico and southwestern states. African American, Caucasian, and Jamaican criminal groups and OMGs also transport marijuana produced in Mexico into North Carolina and distribute wholesale quantities. Caucasian and Mexican criminal groups also distribute wholesale quantities of marijuana produced in large outdoor grows in North Carolina. At the retail level marijuana is distributed by African American, Caucasian, and Hispanic gangs; OMGs; and local independent producers and dealers including students, homemakers, and business people.
Marijuana is the most widely abused illicit drug in North Carolina, and the drug is abused by individuals of all ages. According to the 1999 NHSDA, 4.7 percent of North Carolina residents reported having abused marijuana in the 30 days prior to the survey. The same figure was reported nationwide. The survey data also indicate that rates of marijuana abuse are highest among teenagers and young adults. Nearly 14 percent of North Carolina residents aged 18 to 25 surveyed reported having abused marijuana in the past month, while 6.8 percent of residents aged 12 to 17 surveyed reported the same. Of North Carolina residents aged 26 and older, 3.1 percent reported past month marijuana abuse.
The number of marijuana-related treatment admissions in North Carolina ranked second to the number of cocaine-related admissions each year from FY1996 through FY1999. Marijuana-related treatment admissions increased 70 percent from 7,285 in FY1996 to 12,382 in FY1999, according to the North Carolina Department of Health and Human Services. (See Table 3.)
| Fiscal Year | Admissions |
|---|---|
| 1996 | 7,285 |
| 1997 | 9,382 |
| 1998 | 11,150 |
| 1999 | 12,382 |
Source: North Carolina Department of Health and Human Services.
According to 2000 ADAM data, 44.2 percent of adult male arrestees tested positive for marijuana. Marijuana abuse was highest among male arrestees under 21 years of age; 84.4 percent of arrestees under 21 tested positive for marijuana.
Marijuana produced in Mexico or in North Carolina is readily available. Mexico-produced marijuana is relatively inexpensive and has a low THC (tetrahydrocannabinol) content (average 3.3%). According to local law enforcement, in 2001 a pound of Mexico-produced marijuana sold for $600 to $1,000 in North Carolina. A pound of marijuana produced from cannabis cultivated outdoors in North Carolina sold for $600 to $900. In North Carolina cannabis plants cultivated indoors using hydroponic operations usually yield marijuana with a higher THC content that is significantly more expensive. A pound generally sold for $2,400 in 2001.
The number of marijuana-related arrests was dramatically higher in 1999 than in 1994, particularly among juveniles. According to the North Carolina State Bureau of Investigation, juvenile arrests for marijuana possession likewise were significantly higher in 1999 than in 1994.
| Year | Arrests |
|---|---|
| 1994 | 15,476 |
| 1995 | 17,462 |
| 1996 | 19,266 |
| 1997 | 22,924 |
| 1998 | 22,662 |
| 1999 | 22,728 |
Source: North Carolina State Bureau of Investigation.
Note: Includes possession or sale/manufacturing.
| Year | Arrests |
|---|---|
| 1994 | 1,532 |
| 1995 | 2,286 |
| 1996 | 2,684 |
| 1997 | 3,173 |
| 1998 | 2,932 |
| 1999 | 3,004 |
Source: North Carolina State Bureau of Investigation.
Note: Includes possession.
The amount of marijuana seized in the state increased dramatically from 1998 through 2001. Federal law enforcement authorities in North Carolina seized 801 kilograms of marijuana in 1998, 2,301 kilograms in 1999, 4,885 kilograms in 2000, and 3,826.8 kilograms in 2001, according to FDSS data. Additionally, the number of cannabis plants seized by state and local authorities increased 36 percent from 29,753 in 1999 to 40,464 in 2000.
The number of marijuana-related federal sentences in North Carolina ranked second to cocaine-related federal sentences from FY1996 through FY2000. According to USSC data, the number of marijuana-related federal sentences fluctuated from FY1996 through FY2000, with 113 in FY1996, 72 in FY1997, 79 in FY1998, 124 in FY1999, and 81 in FY2000
Cannabis growers take extreme measures intended to injure or kill intruders on cultivation sites. Cannabis growers frequently protect their grows by booby trapping them with explosives, trip-wired firing devices, and pits dug in the ground. The perimeters of cultivation sites frequently are littered with shards of glass and wooden boards with upright nails. Cultivation sites may also be guarded by aggressive dogs such as pit bulls. Law enforcement authorities report that weapons, usually firearms, are seized frequently from the homes of cannabis growers. Officials from the Asheville Buncombe Metropolitan Enforcement Group, in response to the NDIC National Drug Threat Survey 2001, report that cannabis growers frequently place animal traps among cannabis plants.
Cannabis cultivation is widespread in North Carolina. Outdoor cannabis cultivation is more common than indoor cultivation because of the state’s long growing season, temperate climate, and rural areas that allow growers to conceal cultivation sites. Cannabis growers frequently use federal forest land, particularly in western North Carolina, to minimize the risk of personal property seizures if the plots are seized by law enforcement. Mexican and Caucasian criminal groups are the primary cultivators of outdoor cannabis. Reporting from law enforcement officials indicates that cannabis cultivation is widespread in areas including the Pisgah and Nantahala National Forests in the western part of the state. Outdoor cultivation sites in North Carolina are larger than before, according to law enforcement authorities. In July 2001 state and local law enforcement authorities seized more than 23,000 cannabis plants, ranging in size from seedlings to 9-foot-tall plants, from a large field that covered nearly 2 acres in Chatham County. This cannabis cultivation site was one of the largest ever seized in North Carolina.
Growers also cultivate high potency cannabis in indoor hydroponic operations. Indoor grows vary in size and number from dozens to several hundred cannabis plants. Indoor cultivation requires the grower to regulate light, heat, humidity, and fertilizer. Caucasian and African American independent producers are the primary cultivators of cannabis using hydroponic techniques.
|
Four Illegal Immigrants Arrested
|
Mexican criminal groups are the dominant transporters of Mexico-produced marijuana into North Carolina. They primarily use tractor-trailers to transport multiton quantities of marijuana concealed among legitimate goods such as produce, furniture, and other items from Mexico and southwestern states. Law enforcement officials report that tractor-trailers carrying 1,000 pounds or more of marijuana are increasingly common. In March 2001 law enforcement authorities in Rowan County seized over 4 tons of marijuana from a tractor-trailer that was destined for a farmhouse in the county. The seizure was one of the largest marijuana seizures in North Carolina history.
|
North Carolina Legislators Stiffen Marijuana Laws
|
Mexican, African American, Caucasian, and Jamaican criminal groups also transport marijuana in private vehicles. These criminal groups transport Mexico-produced marijuana directly from Mexico and southwestern states. They also transport marijuana from Georgia, South Carolina, and Tennessee. Transporters conceal marijuana in luggage or in false compartments and sometimes smear marijuana packages with food or liquid soap to conceal the distinctive odor. In May 2001 a sheriff’s deputy in Harrison County, Mississippi, seized 35 pounds of marijuana from a private vehicle and arrested two Mexican individuals who claimed to be traveling from Edinburg, Texas, to Charlotte. The marijuana was wrapped in packing tape and concealed in the gas tank, which contained two compartments: one for gasoline and one for contraband. In April 2001 a Louisiana state trooper arrested an individual driving a vehicle from Texas to North Carolina and seized 62 pounds of marijuana hidden in luggage in the trunk. The marijuana was wrapped in clear cellophane, smeared with mustard, and wrapped again with fabric softener sheets.
|
Marijuana Smuggled Through South Carolina Port
|
Criminal groups, particularly Jamaican, also transport marijuana into North Carolina on commercial airlines, employing couriers who conceal the drug in their luggage or strap packages of it under their clothing. The DEA San Diego Division reports that San Diego is a principal distribution hub for marijuana produced in Mexico supplied to Jamaican criminal groups in the southeastern United States. Mexican DTOs based in Mexico supply marijuana to Jamaican criminal groups in San Diego who then distribute the drug to other Jamaican criminal groups in North Carolina and other southeastern states. Jamaican criminal groups in North Carolina often falsely market Mexico-produced marijuana as Jamaican marijuana because Jamaican marijuana is reputed to be more potent and is, therefore, more expensive. Marijuana produced in Mexico sells for about $400 per pound in San Diego but sells for as much as $2,400 per pound as Jamaican marijuana in North Carolina.
Mexican, African American, and Caucasian criminal groups also transport marijuana into North Carolina from southwestern states via package delivery services. According to 2000 Operation Jetway data, law enforcement authorities in North Carolina seized at least 19 packages that contained multipound quantities of marijuana. The packages were sent from Texas and California, and most were destined for Charlotte. According to the Charlotte-Mecklenburg Police Department, approximately one-half of the packages were sent to members of Mexican criminal groups, and approximately one-half were sent to members of African American criminal groups.
Mexican, African American, and Caucasian criminal groups also transport marijuana into the state on buses and passenger trains. In December 2000 Davidson County sheriff’s deputies stopped a bus traveling from Texas to North Carolina and seized 80 pounds of marijuana in a duffel bag. None of the passengers admitted to owning the bag. According to law enforcement authorities, the passengers were Mexican migrant workers traveling from Texas to North Carolina for employment.
Unknown quantities of marijuana produced in North Carolina are transported out of the state in private vehicles and via package delivery services into urban and rural areas in Georgia, South Carolina, Tennessee, and Virginia.
In North Carolina Mexican criminal groups are the primary wholesale distributors of marijuana produced in Mexico. African American, Caucasian, and Jamaican criminal groups also distribute wholesale quantities of Mexico-produced marijuana. All of these criminal groups distribute marijuana to gang members and local independent dealers; they also distribute some marijuana at the retail level. These criminal groups sell marijuana to dealers of other races and ethnicities; however, in a small number of communities, they distribute marijuana only within their own ethnic group because they distrust outsiders. OMG members sell wholesale quantities to members of smaller motorcycle gangs and female associates who handle retail distribution.
Cannabis growers who cultivate large outdoor plots–usually Caucasian and Mexican criminal groups–sell wholesale quantities of locally produced marijuana to gang members and local independent dealers and occasionally sell retail quantities. Growers who cultivate small amounts of cannabis in their homes or tend small plots–usually Caucasian and African American independent dealers–abuse the drug themselves or sell it to friends, family members, and associates.
At the retail level marijuana is distributed by African American, Caucasian, and Hispanic gangs; OMGs; and local independent producers and dealers including students, homemakers, and businesspeople. Law enforcement authorities report that marijuana is sold at various locations such as open-air drug markets; parking lots; bars and nightclubs; college, high school, and middle school campuses; and businesses and private homes. Law enforcement authorities report that high school students, in particular, are becoming increasingly involved in retail marijuana distribution on and near school grounds. In April 2001, law enforcement officers in Chapel Hill arrested a high school student who had concealed small plastic bags of marijuana in a sock that he had hidden in his pants. Law enforcement officers report that the student intended to sell the marijuana to other students on school grounds.
Source: Marijuana – North Carolina Drug Threat Assessment (justice.gov) April 2003
Oregon farmers have grown three times what their customers can smoke in a year, causing bud prices to plummet and panic to set in
A recent Sunday afternoon at the Bridge City Collective
Little wonder: a gram of weed was selling for less than the price of a glass of wine.
The $4 and $5 grams enticed Scotty Saunders, a 24-year-old sporting a gray hoodie, to spend $88 picking out new products to try with a friend. “We’ve definitely seen a huge drop in prices,” he says.
Across the wood and glass counter, Bridge City owner David Alport was less delighted. He says he’s never sold marijuana this cheap before.
“We have standard grams on the shelf at $4,” Alport says. “Before, we didn’t see a gram below $8.”
The scene at Bridge City Collective is playing out across the city and state. Three years into Oregon’s era of recreational cannabis, the state is inundated with legal weed.
It turns out Oregonians are good at growing cannabis – too good.
In February, state officials announced that 1.1m pounds of cannabis flower were logged in the state’s database.
If a million pounds sounds like a lot of pot, that’s because it is: last year, Oregonians smoked, vaped or otherwise consumed just under 340,000lb of legal bud.
That means Oregon farmers have grown three times what their clientele can smoke in a year.
Yet state documents show the number of Oregon weed farmers is poised to double this summer – without much regard to whether there’s demand to fill.
The result? Prices are dropping to unprecedented lows in auction houses and on dispensary counters across the state.
Wholesale sun-grown weed fell from $1,500 a pound last summer to as low as $700 by mid-October. On store shelves, that means the price of sun-grown flower has been sliced in half to those four-buck grams.
For Oregon customers, this is a bonanza. A gram of the beloved Girl Scout Cookies strain now sells for little more than two boxes of actual Girl Scout cookies.
But it has left growers and sellers with a high-cost product that’s a financial loser. And a new feeling has descended on the once-confident Oregon cannabis industry: panic.
“The business has been up and down and up and down,” says Don Morse, who closed his Human Collective II dispensary in south-west Portland four months ago. “But in a lot of ways it has just been down and down for dispensaries.”
This month, WW spoke to two dozen people across Oregon’s cannabis industry. They describe a bleak scene: small businesses laying off employees and shrinking operations. Farms shuttering. People losing their life’s savings are unable to declare bankruptcy because marijuana is still a federally scheduled narcotic.
To be sure, every new market creates winners and losers. But the glut of legal weed places Oregon’s young industry in a precarious position, and could swiftly reshape it.
Oregon’s wineries, breweries and distilleries have experienced some of the same kind of shakeout over time. But the timetable is faster with pot: for many businesses, it’s boom to bust within months.
Mom-and-pop farms are accepting lowball offers to sell to out-of-state investors, and what was once a diverse – and local – market is increasingly owned by a few big players. And frantic growers face an even greater temptation to illegally leak excess grass across state lines – and into the crosshairs of US attorney general Jeff Sessions’ justice department.
“If somebody has got thousands of pounds that they can’t sell, they are desperate,” says Myron Chadowitz, who owns the Eugene farm Cannassentials. “Desperate people do desperate things.”
In March, Robin Cordell posted a distress signal on Instagram.
“The prices are so low,” she wrote, “and without hustling all day, hoping to find the odd shop with an empty jar, it doesn’t seem to move at any price.”
Cordell has a rare level of visibility for a cannabis grower. Her Oregon City farm, Oregon Girl Gardens, received glowing profiles from Dope Magazine and Oregon Leaf. She has 12 years of experience in the medical marijuana system, a plot of family land in Clackamas county, and branding as one of the state’s leaders in organic and women-led cannabis horticulture.
She fears she’ll be out of business by the end of the year.
“The prices just never went back up,” she says.
Cordell ran headlong into Oregon’s catastrophically bountiful cannabis crop.
The Oregon Liquor Control Commission (OLCC) handed out dozens of licenses to new farmers who planted their first crop last spring. Mild weather blessed the summer of 2017 and stretched generously into the fall. And growers going into their second summer season planted extra seeds to make up for flower lost to a 2016 storm, the last vestige of a brutal typhoon blown across the Pacific from Asia.
“That storm naturally constrained the supply even though there were a lot of cultivators,” says Beau Whitney, senior economist for New Frontier Data, which studies the cannabis industry.
It kept supply low and prices high in 2017 – even though the state was handing out licenses at an alarming rate.
“It was a hot new market,” Whitney says. “There weren’t a whole lot of barriers to entry. The OLCC basically issued a license to anyone who qualified.”
Chadowitz blames out-of-state money for flooding the Oregon system. In 2016, state lawmakers decided to lift a restriction that barred out-of-state investors from owning controlling shares of local farms and dispensaries.
It was a controversial choice – one that many longtime growers still resent.
“The root of the entire thing was allowance of outside money into Oregon,” Chadowitz says. “Anyone could get the money they needed. Unlimited money and unlimited licenses, you’re going to get unlimited flower and crash the market.”
As of 1 April, Oregon had licensed 963 recreational cannabis grows, while another 910 awaited OLCC approval.
That means oversupply is only going to increase as more farms start harvesting bud.
The OLCC has said repeatedly that it has no authority to limit the number of licenses it grants to growers, wholesalers and dispensaries (although by contrast, the number of liquor stores in Oregon is strictly limited).
Since voters legalized recreational marijuana in 2014, many industry veterans from the medical marijuana years have chafed at the entrance of new money, warning it would destroy a carefully crafted farm ecosystem.
The same problem has plagued cannabis industries in other states that have legalized recreational weed. In 2016, Colorado saw wholesale prices for recreational flower drop 38%. Washington saw its pot drop in value at the same time Oregon did.
The OLCC remains committed to facilitating a free market for recreational marijuana in which anyone can try their hand at growing or selling.
“[The law] has to be explicit that we have that authority to limit or put a cap on licenses,” says OLCC spokesman Mark Pettinger. “It doesn’t say that we could put a cap on licenses. The only thing that we can regulate is canopy size.”
The demand for weed in Oregon is robust – the state reeled in $68m in cannabis sales taxes last year – but it can’t keep pace with supply.

Whitney says it’s not unusual for a new industry to attract speculators and people without much business savvy.
“Whenever you have these emerging markets, there’s going to be a lot of people entering the market looking for profit,” he says. “Once it becomes saturated, it becomes more competitive. This is not a phenomenon that is unique to cannabis. There used to be a lot of computer companies, but there’s not so many anymore.”
Across rolling hills of Oregon farmland and in Portland dispensaries as sleek as designer eyewear shops, the story plays out the same: Business owners can’t make the low prices pencil out.
Nick Duyck is a second-generation farmer and owner of 3D Blueberry Farms in Washington county. “I was born and raised on blueberries,” he says.
But last June, Duyck launched Private Reserve Cannabis, a weed grow designed to create permanent jobs for seasonal workers.
“By starting up the cannabis business,” says Duyck, “it keeps my guys busy on a year-round basis.”
He invested $250,000 in the structural build-outs, lighting, environmental controls and other initial costs to achieve a 5,000 sq ft, Tier I, OLCC-approved indoor canopy.
Ongoing labor and operational costs added another $20,000 a month.
Weed prices were high: Duyck forecast a $1,500 return per pound. If Duyck could produce 20lb of flower a week, he’d make back his money and start banking profits in just three months.
October’s bumper crop tore those plans apart.
“We got in at the wrong time,” Duyck says. “The outdoor harvest flooded the market.”
By the start of the new year, Duyck was sitting on 100lb of ready-to-sell flower – an inventory trickling out to dispensaries in single-pound increments.
So he turned to a wholesaler, Cannabis Auctions LLC, which holds monthly fire sales in various undisclosed locations throughout Oregon.
Weed auctions operate under a traditional model: sellers submit their wares, and buyers – dispensary owners, intake managers and extract manufacturers – are given an opportunity to inspect products before bidding on parcels awarded to the highest dollar.
Duyck sent 60lb of pot to the auction block in December. He had adjusted his expectations downward: he hoped to see something in the ballpark of $400 a pound.
It sold for $100 a pound.
“The price per pound that it costs us to raise this product is significantly higher than the hundred dollars a pound,” says Duyck. (A little light math points to a $250-per-unit production cost.) “Currently, we’re operating at a $15,000-per-month loss,” Duyck says.
If prices don’t improve soon, Duyck says he won’t be able to justify renewing his OLCC license for another year.
“The dispensaries that are out there, a lot of them have their own farms, so they don’t buy a lot of product from small farms like us’” Duyck says. “If you really want to grow the product, you almost have to own the store also.”
Middlemen – store owners without farms – are also suffering. Take Don Morse, who gave up selling weed on New Year’s Eve.
Morse ran Human Collective II, one of the earliest recreational shops in the city, which first opened as a medical marijuana supplier in 2010. At times, Morse stocked 100 strains in his Multnomah Village location.

Morse lobbied for legal recreational weed and founded the Oregon Cannabis Business Council.
The shift to recreational was costly. With his business partner Sarah Bennett, Morse says he invested more than $100,000 in equipment to meet state regulations.
By last summer, new stores were popping up at a rapid pace. Morse’s company wasn’t vertically integrated, which means it did not grow any of its own pot or run a wholesaler that might have subsidized low sales.
“Competition around us was fierce, and the company started losing money, and it wasn’t worth it anymore,” Morse says. “At our peak, we had 20 employees. When we closed, we had six.”
Prices went into free fall in October: the average retail price dropped 40%.
Morse couldn’t see a way to make the numbers work. Human Collective priced grams as low as $6 to compete with large chains like Nectar and Chalice, but it struggled to turn a profit.
“When you’re the little guy buying the product from wholesalers, you can’t afford to compete,” he says. “There’s only so far you can lower the price. There’s too much of everything and too many people in the industry.”
So Morse closed his shop: “We paid our creditors and that was that. That was the end of it.”
Despite losing his business, Morse stands behind Oregon’s light touch when it comes to regulating the industry.
“It’s just commercialism at its finest,” he says. “Let the best survive. That’s just the way it goes in capitalism. That’s just the way it goes.”
Just as mom-and-pop grocery stores gave way to big chains, people like Morse are losing out to bigger operations.
Chalice Farms has five stores in the Portland area and is opening a sixth in Happy Valley. La Mota has 15 dispensaries. Nectar has 11 storefronts in Oregon, with four more slated to open soon.
Despite the record-low prices in the cannabis industry, these chains are hiring and opening new locations, sometimes after buying failed mom-and-pop shops.
The home page on Nectar’s website prominently declares: “Now buying dispensaries! Please contact us if you are a dispensary owner interested in selling your business.”
Nectar representatives did not respond to a request for comment.
Because the federal government does not recognize legal marijuana, the industry cannot access traditional banking systems or even federal courts. That means business owners can’t declare bankruptcy to dissolve a failed dispensary or farm, leaving them with few options. They can try to liquidate their assets, destroy the product they have on hand and eat the losses.
Or they can sell the business to a company like Nectar, often for a fraction of what they’ve invested.
“This time last year, it was basically all mom-and-pop shops,” says Mason Walker, CEO of Cave Junction cannabis farm East Fork Cultivars. “Now there are five or six companies that own 25 or 30%. Stores are selling for pennies on the dollar, and people are losing their life savings in the process.”
Deep-pocketed companies can survive the crash and wait for the market to contract again.
“What this means is, the market is now in a position where only the large [businesses] or the ones that can produce at the lower cost can survive,” Whitney says. “A lot of the craft growers, a lot of the small-capacity cultivators, will go out of business.”
Oregon faces another consequence of pot businesses closing up shop: leftover weed could end up on the black market.
Already, Oregon has a thriving illegal market shipping to other states.
US attorney for Oregon, Billy Williams, has said he has little interest in cracking down on legal marijuana businesses, but will prosecute those shipping marijuana to other states.
“That kind of thing is what’s going to shut down our industry,” Chadowitz says. “Anything we can do to prevent Jeff Sessions from being right, we have to do.”
Ask someone in the cannabis industry what to do about Oregon’s weed surplus, and you’re likely to get one of three answers.
The first is to cap the number of licenses awarded by the OLCC. The second is to reduce the canopy size allotted to each license – Massachusetts is trying that. And the last, equally common answer is to simply do nothing. Let the market sort itself out.

Farmers, such as Walker of East Fork Cultivars, argue that limiting the number of licensed farms in Oregon would stunt the state’s ability to compete on the national stage in the years ahead.
“We’re in this sort of painful moment right now,” says Walker, “but I think if we let it be a painful moment, and not try to cover it up, we’re going to be better off for it.”
Walker and other growers hope selling across state lines will someday become legal.
Every farmer, wholesaler, dispensary owner and economist WW talked to for this story said that if interstate weed sales became legal, Oregon’s oversupply problem would go away.
Under the current presidential administration, that might seem a long shot. But legalization is sweeping the country, Donald Trump is signaling a looser approach, and experts say Oregon will benefit when the feds stop fighting.
“The thing about Oregon is that it is known for its cannabis, in a similar way to Oregon pinot noir,” Whitney says. “For those who are able to survive, they are positioned extremely well not only to survive in the Oregon market but also to take advantage of a larger market – assuming things open up on a federal level.”
Source: How do you move mountains of unwanted weed? | Cannabis | The Guardian May 2018
SEPARATING MARIJUANA FACT FROM FICTION IN NEW YORK RESPONSE TO THE “ASSESSMENT OF THE POTENTIAL IMPACT OF REGULATED MARIJUANA IN NEW YORK STATE”
AUGUST 2018
Executive Summary
Recently, New York State (NYS) released what they claimed to be “an extensive assessment of current research and literature to evaluate the cost-risk benefit of legalizing the recreational adult use of marijuana.”
The overall conclusion of this assessment was that marijuana poses little public health risk and should be considered for legalization. But a closer look finds several flaws in the report that questions its purpose and conclusions. Unfortunately, it appears that the conclusion of the NYS report was written before the data were analyzed. The legalization of recreational marijuana is presented in the introduction as a fait accompli: “It has become less a question of whether to legalize but how to do so responsibly.” Much of the report discusses how to decrease the dangers of legal recreational marijuana. The best way to lessen the danger is to keep it from being commercialized, normalized, promoted – and legalized.
The report conflates the issues of medical marijuana and commercial sales of recreational marijuana. The potential medical benefits of medical cannabis are already available in New York. Adding indiscriminate recreational use does not increase any health benefit to New Yorkers.
Smart Approaches to Marijuana (SAM) is advised by a scientific advisory board of researchers from institutions such as Harvard and Johns Hopkins. SAM believes in the need for rational, well-informed public policy – legislation that maximizes public health benefits and minimizes harms.
This state-issued report reads more like a marijuana lobbyist’s manifesto, as we found no credible opposing evidence cited.
Based on our findings, the reference to unlisted “subject-matter experts” that the report apparently relied on, and the fact that state medical groups like the New York Society for Addiction Medicine (NYSAM) were not consulted with, we are formally requesting that the state of New York publicly disclose all sources that were consulted and those that contributed to creation of the document. We believe that National Institute of Health (NIH) scientists, NYSAM physicians, and other experts should have the chance to review these findings.
Below are the top claims from the report and rebuttals.
CLAIM: “A 2017 Marist Poll showed that 52 percent of Americans 18 years of age or older have tried marijuana at some point in their lives, and 44 percent of these individuals currently use it.”
CORRECTION:
The best usage data are not found in polls, but rather scientific studies conducted by the National Institutes of Health. According to the most recent National Survey on Drug Use and Health (NSDUH) data, 10.58% of Americans 12 or older and 10.84% of New York State residents reported being current users and 44% of Americans have tried marijuana at some point in their life (NSDUH, 2016).
CLAIM: “In 1999 the Institute of Medicine (IOM) found a base of evidence to support the benefits of marijuana for medical purposes.”
CORRECTION:
This report is supposed to be about non-medical marijuana. We should not conflate the two issues. Still, there have been several reviews since this was published almost twenty years ago. The 1999 IOM report stated: “Because of the health risks associated with smoking, smoked marijuana should generally not be recommended for long-term medical use” and called for a “heavier investment in research.”
Released at the beginning of 2017, the most recent National Academy of Sciences report said: “Despite increased cannabis use and a changing state-level policy landscape, conclusive evidence regarding the short- and long-term health effects—both harms and benefits—of cannabis use remains elusive.” The July 24, 2018 issue of the Annals of Internal Medicine stated that “Americans’ view of marijuana use is more favorable than existing evidence supports.”
Again, this NYS report recommended recreational legalization, and we should separate the issue of the possible therapeutic benefits from this study.
CLAIM: “Most women who use marijuana stop or reduce their use during pregnancy.”
CORRECTION:
Dr. Nora Volkow, NIH’s drug abuse director, published a report last year in response to an alarming trend being seen across the country of increased cannabis use during pregnancy and warned of the detrimental health risks of in utero cannabis exposure (Volkow et al., 2017).
Even more alarming is a recent study that was not included in this report where researchers found nearly 70% of 400 Colorado dispensaries surveyed in a scientific, undercover study were recommending cannabis products to mothers experiencing morning-sickness in the first trimester (Dickson et al., 2018).
A clinically-controlled study published this year found that mothers vulnerable to mental illness who smoked during pregnancy put their child at higher risk to develop significantly more psychotic symptoms earlier in life compared to mothers who didn’t smoke marijuana, but had similar vulnerabilities (Bolhuis et al., 2018).
CLAIM: “Data from multiple sources indicate that legalization in Colorado had no substantive impact on youth marijuana use.”
CORRECTION:
Despite widely publicized reports by the state of Colorado, pro-legalization lobbyists, and others with revenue-producing interests; reliable data sources say otherwise. According to NSDUH state estimates, Colorado now leads the nation in the percentage of 12- to 17-year olds who have tried marijuana for the first time (NSDUH, State Estimates, 2017). In adolescents and adults, Colorado is well above the national average.
All state-collected data related to adolescent substance use is done via the Healthy Kids Colorado Survey – a state sponsored assessment to replace all other national and state surveys administered in school. Until 2017, these data have not met the CDC’s standard qualifications for sampling methodology since 2011 – the year before recreational marijuana became legal in Colorado. The 2015 HKCS has been widely criticized for misrepresenting and promoting misleading messages surrounding adolescent drug use (Murray, 2016).

As a result of questionable reports publicized by the state of Colorado and pro-legalization activists, local investigative journalists at the Denver Post interviewed numerous law enforcement officers, educators and advocates; in addition to analyzing databases. They ultimately concluded that state-produced data appears to be unreliable (Migoya, 2017). “Records do not account for many young offenders who either are not reported to police, are not ticketed because police say there’s too little to cite or have infractions that are not tabulated because of programs designed to protect minors from blemished records.”
CLAIM: “There has been no increase in violent crime or property crime rates around medical marijuana dispensaries.”
CORRECTION:
The relationship between marijuana establishments and crime is mixed at best. A study funded by the National Institutes of Health showed that the density of marijuana dispensaries was linked to increased property crimes in nearby areas (Freisthler, et al., 2017). Colorado Public Radio reported similar findings – particularly in Denver and Pueblo – and noted the visible association with increased gang violence seen in both cities likely due to a high density of dispensaries and illegal activity, including the black market (Markus, 2017).
CLAIM: “Marijuana is an effective treatment for pain, greatly reduces the chance of dependence, and eliminates the risk of fatal overdose compared to most opioid-based medications.”
CORRECTION:
This is inaccurate and is confounding medical and recreational use. This statement was based on a survey that 17 medical marijuana patients took while being prescribed opioids. Self-report data can be useful but have no value in informing serious public health risks. Several recent and widely-circulated studies show strong contradictory evidence to this claim.
Researchers found that patients reporting marijuana use actually experienced more pain on average when admitted to the hospital following a traumatic injury than those that did not. Compared to non-users, they required more opioid medication to cope with the pain and consistently rated their pain higher during the duration of their stay (Salottolo et al., 2018).
A 4-year prospective study in the highly respected Lancet journal followed medical marijuana patients with a dual opioid prescription and found that marijuana use did not reduce opioid use or prescribing. Users reported greater pain severity and more day-to-day interference than those that did not use marijuana (Campbell et al., 2018).
CLAIM: “Regulated marijuana introduces an opportunity to reduce harm for consumers through labeling.”
CORRECTION:
Non-FDA approved commercially-produced products have received only minimal regulatory attention. Recent studies have shown rampant mislabeling of the active cannabinoid ingredients in concentrates and edibles (Peace et al., 2016).
The FDA has published warning letters on the severe mislabeling of commercial products consistently seen on the market since 2015 (FDA, 2015-17). This claim was cited from the Drug Policy Alliance website. The DPA and its affiliates have directly funded campaigns to legalize all forms of marijuana including edible products throughout the US. They also call for the legalization of all drugs. This is not a credible source.
CLAIM: “The status quo (i.e., criminalization of marijuana) has not curbed marijuana use.”
CORRECTION:
Non-public, personal use of Marijuana is not criminalized in NYS nor are possession of small amounts for personal amounts – often a reason for imprisonment. In 2016 23.5% Americans reported using legal drugs compared to 10.6% using illegal ones – signaling that the law matters in preventing drug use (NSDUH, 2016). In 2017 in New York State, marijuana made up 0.003% of non youthful-offender felony sentences to prison. There were no youthful offender felony marijuana sentences for prison. Misdemeanor marijuana arrests made up 8.5% of all state
misdemeanor arrests (NY State Division of Criminal Services, 2018). The recent rush to legalization across the country has pushed marijuana to the number one spot for recent first-time drug users aged 12 or older in 2016 compared to any other illicit drug (NSDUH, 2016).
CLAIM: “Legalizing marijuana results in a reduction in the use of synthetic cannabinoids.”
CORRECTION:
This claim is inaccurately attributed to the report Global Drug Survey which indicates that countries that decriminalize marijuana have lower rates of synthetic marijuana use. The claim cannot be found in that reference. And, even if there is an association between decreased synthetic use and decriminalized marijuana, it does not follow that legalizing marijuana will cause a reduction in synthetic use. We emailed Professor Adam R Winstock, Founder & CEO of the Global Drug Survey, to ask his opinion. He replied, ”It’s not clear cut,” indicating uncertainty. There is not much data on decreased synthetic use in countries with decriminalization (Zucker doesn’t even say “countries with legalization” which is actually the issue at hand because only Uruguay would fall into that category).
CLAIM: “The over-prosecution of marijuana has had significant negative economic, health, and safety impacts that have disproportionately affected low-income communities of color.”
CORRECTION:
Marijuana does not need to be legalized to address valid social justice concerns. Although overall drug-related offenses have decreased in states that have legalized; minorities have still disproportionately been targeted for the arrests that do still occur. Such as in 2014, two years after legalization in Colorado, the marijuana arrest rates for African‐ Americans (348 per 100,000) was almost triple that of Whites (123 per 100,000) (Co. Dept. of Public of Safety, 2016).
Colorado has seen an increase in crime in regions that attract recreational users. Although the rise in crime cannot be attributed to legalization of marijuana alone, much of the violence has been attributed to increased gang violence where dispensaries are densest (Markus, 2017). Current drug policies can be changed without legalization.
CLAIM: “The negative health consequences of marijuana have been found to be lower than alcohol, tobacco, and illicit drugs including heroin and cocaine.”
CORRECTION:
This statement is questionable because it was based on a theoretical model that estimated human consumption averages for each substance and calculated a risk ratio using lethal doses reported in animal studies. Basic research is necessary for understanding the biology underlying addiction; however, the transferability of dosing schedules between species has not been conclusively established. Much of the reason alcohol and tobacco exert more costs to society than many illegal drugs is because those two drugs are legalized and commercialized. As Dr. Nora Volkow, head of NIH’s drug abuse institute stated, “Repeated marijuana use during adolescence may result in long-lasting changes in brain function that can jeopardize educational, professional, and social achievements.
“However, the effects of a drug (legal or illegal) on individual health are determined not only by its pharmacologic properties but also by its availability and social acceptability.” “In this respect, legal drugs (alcohol and tobacco) offer a sobering perspective, accounting for the greatest burden of disease associated with drugs not because they are more dangerous than illegal drugs but because their legal status allows for more widespread exposure.”
CLAIM: “The impact of legalization in surrounding states has accelerated the need for NYS to address legalization.”
CORRECTION:
This statement reads as if two wrongs somehow make a right. NYS should not be forced into legalizing marijuana because other states are considering it (several surrounding states, it should be noted, have considered and then defeated proposals to legalize marijuana). Even if a surrounding state or two legalizes marijuana, NYS can stand out as the state promoting health, well-being, family-centered tourism – not more drug use.
This statement totally ignores newer polls such as the 2018 Emerson College poll that found that the majority of New Yorkers do not support the legalization of marijuana. A plurality support either decriminalization or the current policy.
“The poll — conducted by the same college that recently conducted a poll for pro-marijuana groups Marijuana Policy Project (MPP) and the Drug Policy Alliance (DPA) — reported that 56% of respondents did not favor legalizing the recreational sales of marijuana.”
REFERENCES
Bolhuis, K., Kushner, S. A., Yalniz, S., Hillegers, M. H., Jaddoe, V. W., Tiemeier, H., & El Marroun, H. (2018). Maternal and paternal cannabis use during pregnancy and the risk of psychotic-like experiences in the offspring. Schizophrenia research.
Campbell, G., Hall, W. D., Peacock, A., Lintzeris, N., Bruno, R., Larance, B., … & Blyth, F. (2018). Effect of cannabis use in people with chronic non-cancer pain prescribed opioids: findings from a 4-year prospective cohort study. The Lancet Public Health, 3(7), e341-e350.
Center for Behavioral Health Statistics and Quality. (2017). 2016 National Survey on Drug Use and Health: Detailed Tables. Substance Abuse and Mental Health Services Administration, Rockville, MD.
Commissioner, O. O. (n.d.). Public Health Focus – Warning Letters and Test Results for Cannabidiol-Related Products. Retrieved from https://www.fda.gov/newsevents/publichealthfocus/ucm484109.htm
Colorado Dept. Public Safety. (2016, March). Marijuana Legalization in Colorado: Early Findings. Retrieved from https://cdpsdocs.state.co.us/ors/docs/reports/2016-SB13-283-Rpt.pdf
Copyright © 2018 National Academy of Sciences. All Rights Reserved. (2017, November 08). Retrieved from http://nationalacademies.org/hmd/Activities/PublicHealth/MarijuanaHealthEffects.aspx
Dickson, B., Mansfield, C., Guiahi, M., Allshouse, A. A., Borgelt, L., Sheeder, J., … & Metz, T. D. (2018). 931: Recommendations from cannabis dispensaries on first trimester marijuana use. American Journal of Obstetrics and Gynecology, 218(1), S551.
Emerson College. (2018, June). June 2018 Public Opinion Survey of New York Registered Voters Attitudes on Marijuana Policy. Retrieved from https://learnaboutsam.org/wp-content/uploads/2018/06/nyspoll-1.pdf Commissioned by Smart Approaches to Marijuana
Freisthler, B., Ponicki, W. R., Gaidus, A., & Gruenewald, P. J. (2016). A micro‐temporal geospatial analysis of medical marijuana dispensaries and crime in Long Beach, California. Addiction, 111(6), 1027-1035.
Green, M. C. (2018, June). Criminal Justice Case Processing Arrest through Disposition New York State January – December 2017. Retrieved from http://www.criminaljustice.ny.gov/crimnet/ojsa/dar/DAR-4Q-2017-NewYorkState.pdf
Keyhani, S., Steigerwald, S., Ishida, J., Vali, M., Cerdá, M., Hasin, D., . . . Cohen, B. E. (2018). Risks and Benefits of Marijuana Use. Annals of Internal Medicine. doi:10.7326/m18-0810
Markus, B. (2017, July 31). A Dive Into Colorado Crime Data In 5 Charts. Retrieved from http://www.cpr.org/news/story/a-dive-into-colorado-crime-data-in-5-charts
Migoya, D. (2017, December 22). Police across Colorado questioning whether youths are using marijuana less. Retrieved from https://www.denverpost.com/2017/12/22/police-across-colorado-questioning-youth-marijuana-use/
Murray, D. W. (2016, July 2). Misrepresenting Colorado Marijuana – by David W. Murray. Retrieved from https://www.hudson.org/research/12615-misrepresenting-colorado-marijuana
National Families in Action. (n.d.). Colorado | The Marijuana Report.org. Retrieved from http://themarijuanareport.org/colorado/.
Peace, M. R., Butler, K. E., Wolf, C. E., Poklis, J. L., & Poklis, A. (2016). Evaluation of two commercially available cannabidiol formulations for use in electronic cigarettes. Frontiers in pharmacology, 7, 279.
Salottolo, K., Peck, L., Tanner II, A., Carrick, M. M., Madayag, R., McGuire, E., & Bar-Or, D. (2018). The grass is not always greener: a multi-institutional pilot study of marijuana use and acute pain management following traumatic injury. Patient Safety in Surgery, 12(1), 16.
Volkow, N. D., Compton, W. M., & Wargo, E. M. (2017). The risks of marijuana use during pregnancy. Jama, 317(2), 129-130.
Smart Approaches to Marijuana (SAM) is a nonpartisan, non-profit alliance of physicians, policy makers, prevention workers, treatment and recovery professionals, scientists, and other concerned citizens opposed to marijuana legalization who want health and scientific evidence to guide marijuana policies. SAM was co-founded by former Congressman Patrick Kennedy and former Obama Administration senior drug policy advisor, Dr. Kevin Sabet. SAM has affiliates in more than 30 states.
Source: NY-Rebuttal-Absolute-Final.pdf (learnaboutsam.org) August 2018
America’s largest drug companies saturated the country with 76 billion oxycodone and hydrocodone pain pills from 2006 through 2012 as the nation’s deadliest drug epidemic spun out of control, according to previously undisclosed company data released as part of the largest civil action in U.S. history.
The information comes from a database maintained by the Drug Enforcement Administration that tracks the path of every single pain pill sold in the United States — from manufacturers and distributors to pharmacies in every town and city. The data provides an unprecedented look at the surge of legal pain pills that fueled the prescription opioid epidemic, which has resulted in nearly 100,000 deaths from 2006 through 2012.
Just six companies distributed 75 percent of the pills during this period: McKesson Corp., Walgreens, Cardinal Health, AmerisourceBergen, CVS and Walmart, according to an analysis of the database by WAPO. Three companies manufactured 88 percent of the opioids: SpecGx, a subsidiary of Mallinckrodt; Actavis Pharma; and Par Pharmaceutical, a subsidiary of Endo Pharmaceuticals.
[Top takeaways from The Post’s analysis of the DEA database]
Purdue Pharma, which the plaintiffs allege sparked the epidemic in the 1990s with its introduction of OxyContin, its version of oxycodone, was ranked fourth among manufacturers with about 3 percent of the market.
The volume of the pills handled by the companies skyrocketed as the epidemic surged, increasing about 51 percent from 8.4 billion in 2006 to 12.6 billion in 2012. By contrast, doses of morphine, a well-known treatment for severe pain, averaged slightly more than 500 million a year during the period.
Those 10 companies along with about a dozen others are now being sued in federal court in Cleveland by nearly 2,000 cities, towns and counties alleging that they conspired to flood the nation with opioids. The companies, in turn, have blamed the epidemic on overprescribing by doctors and pharmacies and on customers who abused the drugs. The companies say they were working to supply the needs of patients with legitimate prescriptions desperate for pain relief.
The database reveals what each company knew about the number of pills it was shipping and dispensing and precisely when they were aware of those volumes, year by year, town by town. In case after case, the companies allowed the drugs to reach the streets of communities large and small, despite persistent red flags that those pills were being sold in apparent violation of federal law and diverted to the black market, according to the lawsuits.
Plaintiffs have long accused drug manufacturers and wholesalers of fueling the opioid epidemic by producing and distributing billions of pain pills while making billions of dollars. The companies have paid more than $1 billion in fines to the Justice Department and Food and Drug Administration over opioid-related issues, and hundreds of millions more to settle state lawsuits. But the previous cases addressed only a portion of the problem, never allowing the public to see the size and scope of the behavior underlying the epidemic. Monetary settlements by the companies were accompanied by agreements that kept such information hidden.
The drug companies, along with the DEA and the Justice Department, have fought furiously against the public release of the database, the Automation of Reports and Consolidated Order System, known as ARCOS. The companies argued that the release of the “transactional data” could give competitors an unfair advantage in the marketplace. The Justice Department argued that the release of the information could compromise ongoing DEA investigations. Until now, the litigation has proceeded in unusual secrecy. Many filings and exhibits in the case have been sealed under a judicial protective order. The secrecy finally lifted after The Post and HD Media, which publishes the Charleston Gazette-Mail in West Virginia, waged a year-long legal battle for access to documents and data from the case.
On Monday evening, U.S. District Judge Dan Polster removed the protective order for part of the ARCOS database. Lawyers for the local governments suing the companies hailed the release of the data. “The data provides statistical insights that help pinpoint the origins and spread of the opioid epidemic — an epidemic that thousands of communities across the country argue was both sparked and inflamed by opioid manufacturers, distributors, and pharmacies,” said Paul T. Farrell Jr. of West Virginia, co-lead counsel for the plaintiffs.
In statements emailed to The Post on Tuesday, the drug distributors stressed that the ARCOS data would not exist unless they had accurately reported shipments and questioned why the government had not done more to address the crisis. “For decades, DEA has had exclusive access to this data, which can identify the total volumes of controlled substances being ordered, pharmacy-by-pharmacy, across the country,” McKesson spokeswoman Kristin Chasen said. A DEA spokeswoman declined to comment Tuesday “due to ongoing litigation.”
Cardinal Health said that it has learned from its experience, increasing training and doing a better job to “spot, stop and report suspicious orders,” company spokeswoman Brandi Martin wrote.
AmerisourceBergen derided the release of the ARCOS data, saying it “offers a very misleading picture” of the problem. The company said its internal “controls played an important role in enabling us to, as best we could, walk the tight rope of creating appropriate access to FDA approved medications while combating prescription drug diversion.”
While Walgreens still dispenses opioids, the company said it has not distributed prescription-controlled substances to its stores since 2014. “Walgreens has been an industry leader in combatting this crisis in the communities where our pharmacists live and work, ” said Phil Caruso, a Walgreens spokesman.
Mike DeAngelis, a spokesman for CVS, said the plaintiffs’ allegations about the company have no merit and CVS is aggressively defending against them. Walmart, Purdue and Endo declined to comment about the ARCOS database. A Mallinckrodt spokesman said in a statement that the company produced opioids only within a government-controlled quota and sold only to DEA-approved distributors.Actavis Pharma was acquired by Teva Pharmaceutical Industries in 2016, and a spokeswoman there said the company “cannot speak to any systems in place beforehand.”
A virtual road map – The Post has been trying to gain access to the ARCOS database since 2016, when the news organization filed a Freedom of Information Act request with the DEA. The agency denied the request, saying some of the data was available on its website. But that data did not contain the transactional information the companies are required to report to the DEA every time they sell a controlled substance such as oxycodone and hydrocodone.
The drug companies and pharmacies themselves provided the sales data to the DEA. Company officials have testified before Congress that they bear no responsibility for the nation’s opioid epidemic. The numbers of pills the companies sold during the seven-year time frame are staggering, far exceeding what has been previously disclosed in limited court filings and news stories. Three companies distributed nearly half of the pills: McKesson with 14.1 billion, Walgreens with 12.6 billion and Cardinal Health with 10.7 billion. The leading manufacturer was Mallinckrodt’s SpecGx with nearly 28.9 billion pills, or nearly 38 percent of the market.
The states that received the highest concentrations of pills per person per year were: West Virginia with 66.5, Kentucky with 63.3, South Carolina with 58, Tennessee with 57.7 and Nevada with 54.7. West Virginia also had the highest opioid death rate during this period. Rural areas were hit particularly hard: Norton, Va., with 306 pills per person; Martinsville, Va., with 242; Mingo County, W.Va., with 203; and Perry County, Ky., with 175. In that time, the companies distributed enough pills to supply every adult and child in the country with 36 each year.
The database is a virtual road map to the nation’s opioid epidemic that began with prescription pills, spawned increased heroin use and resulted in the current fentanyl crisis, which added more than 67,000 to the death toll from 2013 to 2017. The transactional data kept by ARCOS is highly detailed. It includes the name, DEA registration number, address and business activity of every seller and buyer of a controlled substance in the United States. The database also includes drug codes, transaction dates, and total dosage units and grams of narcotics sold. The data tracks a dozen different opioids, including oxycodone and hydrocodone, which make up three-quarters of the total pill shipments to pharmacies.
Under federal law, drug manufacturers, distributors and pharmacies must report each transaction of a narcotic to the DEA, where it is logged into the ARCOS database. If company officials notice orders of drugs that appear to be suspicious because of their unusual size or frequency, they must report those sales to the DEA and hold back the shipments. As more and more towns and cities became inundated by pain pills, they fought back. They filed federal lawsuits against the drug industry, alleging that opioids from the companies were devastating their communities. They alleged the companies not only failed to report suspicious orders, but they also filled those orders to maximize profits. As the hundreds of lawsuits began to pile up, they were consolidated into the one centralized case in U.S. District Court in Cleveland. The opioid litigation is now larger in scope than the tobacco litigation of the 1980s, which resulted in a $246 billion settlement over 25 years.
Judge Polster is now overseeing the consolidated case of nearly 2,000 lawsuits. The case is among a wave of actions that includes other lawsuits filed by more than 40 state attorneys general and tribal nations. In May, Purdue settled with the Oklahoma attorney general for $270 million. In the Cleveland case, Polster has been pressing the drug companies and the plaintiffs to reach a global settlement so communities can start receiving financial assistance to mitigate the damage that has been done by the opioid epidemic. To facilitate a settlement, Polster had permitted the drug companies and the towns and cities to review the ARCOS database under a protective order while barring public access to the material. He also permitted some court filings to be made under seal and excluded the public and press from a global settlement conference at the outset of the case. Last June, The Post and the Charleston Gazette-Mail asked Polster to lift the protective order covering the ARCOS database and the court filings. A month later, Polster denied the requests, even though he had said earlier that “the vast oversupply of opioid drugs in the United States has caused a plague on its citizens” and the ARCOS database reveals “how and where the virus grew.” He also said disclosure of the ARCOS data “is a reasonable step toward defeating the disease.”
Lawyers for The Post and the Gazette-Mail appealed Polster’s ruling. They argued that the ARCOS material would not harm companies or investigations because the judge had already decided to allow the local government plaintiffs to collect information from 2006 through 2014, withholding the most recent years beginning with 2015 from the lawsuit. “Access to the ARCOS Data can only enhance the public’s confidence that the epidemic and the ensuing litigation are being handled appropriately now — even if they might not have been handled appropriately earlier,” The Post’s lawyer, Karen C. Lefton, wrote in her Jan. 17 appeal. The lawyers also noted the DEA did not object when the West Virginia attorney general’s office provided partial ARCOS data to the Gazette-Mail in 2016. That data showed that drug distribution companies shipped 780 million doses of oxycodone and hydrocodone into the state between 2007 and 2012.
On June 20, the 6th Circuit Court of Appeals in Ohio sided with the news organizations. A three-judge panel reversed Polster, ruling that the protective order sealing the ARCOS database be lifted with reasonable redactions and directed the judge to reconsider whether any of the records in the case should be sealed. On Monday, Polster lifted the protective order on the database, ruling that all the data from 2006 through 2012 should be released to the public, withholding the 2013 and 2014 data.
‘Prescription tourists’ – The pain pill epidemic began nearly three decades ago, shortly after Purdue Pharma introduced what it marketed as a less addictive form of opioid it called OxyContin. Purdue paid doctors and nonprofit groups advocating for patients in pain to help market the drug as a safe and effective way to treat pain. But the new drug was highly addictive. As more and more people were hooked, more and more companies entered the market, manufacturing, distributing and dispensing massive quantities of pain pills. Purdue ending up paying a $634 million fine to the Food and Drug Administration for claiming OxyContin was less addictive than other pain medications.
Annual opioid sales nationwide rose from $6.1 billion in 2006 to $8.5 billion in 2012, according to industry data gathered by IQVIA, a health care information and consulting company. Individual drug company revenues ranged in single years at the epidemic’s peak from $403 million for opioids sold by Endo to $3.1 billion in OxyContin sales by Purdue Pharma, according to a 2018 lawsuit against multiple defendants by San Juan County in New Mexico.
During the past two decades, Florida became ground zero for pill mills — pain management clinics that served as fronts for corrupt doctors and drug dealers. They became so brazen that some clinics set up storefronts along I-75 and I-95, advertising their products on billboards by interstate exit ramps. So many people traveled to Florida to stock up on oxycodone and hydrocodone, they were sometimes referred to as “prescription tourists.” The route from Florida to Georgia, Kentucky, West Virginia and Ohio became known as the “Blue Highway.” It was named after the color of one of the most popular pills on the street — 30 mg oxycodone tablets made by Mallinckrodt, which shipped more than 500 million of the pills to Florida between 2008 and 2012.
When state troopers began pulling over and arresting out-of-state drivers for transporting narcotics, drug dealers took to the air. One airline offered nonstop flights to Florida from Ohio and other Appalachian states, and the route became known as the Oxy Express.
A decade ago, the DEA began cracking down on the industry. In 2005 and 2006, the agency sent letters to drug distributors, warning them that they were required to report suspicious orders of painkillers and halt sales until the red flags could be resolved. The letter also went to drug manufacturers. Even just one distributor that fails to follow the law “can cause enormous harm,” the 2006 DEA letter said. DEA officials said the companies paid little attention to the warnings and kept shipping millions of pills in the face of suspicious circumstances. As part of its crackdown, the DEA brought a series of civil enforcement cases against the largest distributors.
The corporations to date have paid nearly $500 million in fines to the Justice Department for failing to report and prevent suspicious drug orders, a number that is dwarfed by the revenue of the companies.
But the settlements of those cases revealed only limited details about the volume of pills that were being shipped.
In 2007, the DEA brought a case against McKesson. The DEA accused the company of shipping millions of doses of hydrocodone to Internet pharmacies after the agency had briefed the company about its obligations under the law to report suspicious orders. “By failing to report suspicious orders for controlled substances that it received from rogue Internet pharmacies, the McKesson Corporation fueled the explosive prescription drug abuse problem we have in this country,” the DEA’s administrator said at the time. In 2008, McKesson agreed to pay a $13.25 million fine to settle the case and pledged to more closely monitor suspicious orders from its customers.
That same year, the DEA brought a case against Cardinal Health, accusing the nation’s second-largest drug distributor of shipping millions of doses of painkillers to online and retail pharmacies without notifying the DEA of signs that the drugs were being diverted to the black market. Cardinal settled the case by paying a $34 million fine and promising to improve its suspicious monitoring program.
Some companies were repeat offenders. In 2012, the DEA began investigating McKesson again, this time for shipping suspiciously large orders of narcotics to pharmacies in Colorado. One store in Brighton, Colo., population 38,000, was ordering 2,000 pain pills per day. The DEA discovered that McKesson had filled 1.6 million orders from its Aurora, Colo., warehouse between 2008 and 2013 and reported just 16 as suspicious. None involved the Colorado store. DEA agents and investigators said they had amassed enough information to file criminal charges against McKesson and its officers but they were overruled by federal prosecutors. The company wound up paying a $150 million fine to settle, a record amount for a diversion case.
Also in 2012, Cardinal Health attracted renewed attention from the DEA when it discovered that the company was again shipping unusually large amounts of painkillers to its Florida customers. The company had sold 12 million oxycodone pills to four pharmacies over four years. In 2011, Cardinal shipped 2 million doses to a pharmacy in Fort Myers, Fla. Comparable pharmacies in Florida typically ordered 65,000 doses per year. The DEA also noticed that Cardinal was shipping unusually large amounts of oxycodone to a pair of CVS stores near Sanford, Fla. Between 2008 and 2011, Cardinal sold 2.2 million pills to one of the stores. In 2010, that store purchased 885,900 doses — a 748 percent increase over the previous year. Cardinal did not report any of those sales as suspicious. Cardinal later paid a $34 million fine to settle the case. The DEA suspended the company from selling narcotics from its warehouse in Lakeland, Fla. CVS paid a $22 million fine. As the companies paid fines and promised to do a better job of stopping suspicious orders, they continued to manufacture, ship and dispense large amounts of pills, according to the newly released data. “The depth and penetration of the opioid epidemic becomes readily apparent from the data,” said Peter J. Mougey, a lawyer for the plaintiffs from Pensacola, Fla. “This disclosure will serve as a wake up call to every community in the country. America should brace itself for the harsh reality of the scope of the opioid epidemic. Transparency will lead to accountability.”
Aaron Williams, Andrew Ba Tran, Jenn Abelson, Aaron C. Davis and Christopher Rowland contributed to this report.
Scott Higham is a Pulitzer-Prize winning investigative reporter at WAPO; has worked on Metro, National and Foreign projects since 2000.
Sari Horwitz is a Pulitzer-Prize winning reporter who covers DOJ, law enforcement & criminal justice issues for WAPO, where she has been a reporter for 34 years.
Steven Rich is the database editor for investigations at WAPO; has worked on investigations involving the NSA,, police shootings, tax liens & civil forfeiture; reporter on two teams to win Pulitzer Prizes, for public service in 2014 and national reporting in 2016.
Source: https://www.washingtonpost.com Feb. 4th 2019
When Californians voted in 2016 to allow the sale of recreational marijuana, advocates of the move envisioned thousands of pot shops and cannabis farms obtaining state licenses, making the drug easily available to all adults within a short drive.
But as the first year of licensed sales comes to a close, California’s legal market hasn’t performed as state officials and the cannabis industry had hoped. Retailers and growers say they’ve been stunted by complex regulations, high taxes and decisions by most cities to ban cannabis shops. At the same time, many residents are going to city halls and courts to fight pot businesses they see as nuisances, and police chiefs are raising concerns about crime triggered by the marijuana trade.
Gov.-elect Gavin Newsom, who played a large role in the legalization of cannabis, will inherit the numerous challenges when he takes office in January as legislators hope to send him a raft of bills next year to provide banking for the pot industry, ease the tax burden on retailers and crack down on sales to minors.
Hundreds of new California laws take effect Jan. 1. How will they affect you? »
“The cannabis industry is being choked by California’s penchant for over-regulation,” said Dale Gieringer, director of California NORML, a pro-legalization group. “It’s impossible to solve all of the problems without a drastic rewrite of the law, which is not in the cards for the foreseeable future.”
After voters legalized marijuana two years ago under Proposition 64, state officials estimated in there would be as many as 6,000 cannabis shops licensed in the first few years. But the state Bureau of Cannabis Control has issued just 547 temporary and annual licenses to marijuana retail stores and dispensaries. Some 1,790 stores and dispensaries were paying taxes on medicinal pot sales before licenses were required starting Jan. 1.
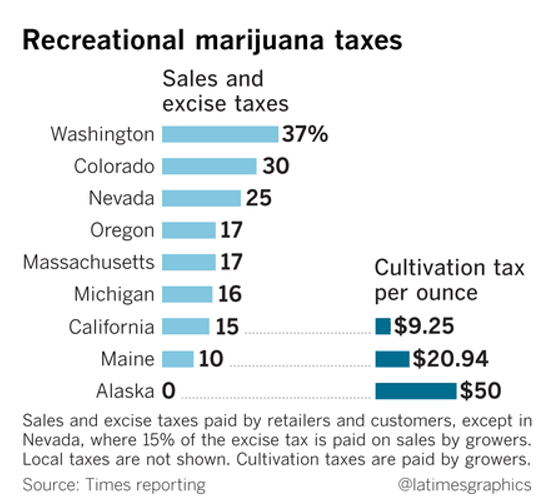
(Los Angeles Times)
State officials also predicted that legal cannabis would eventually bring in up to $1 billion in revenue a year. But with many cities banning pot sales, tax revenue is falling far short of estimates. Based on taxes collected since Jan. 1, the state is expected to bring in $471 million in revenue this fiscal year — much less than the $630 million projected in Gov. Jerry Brown’s budget.
“I think we all wish we could license more businesses, but our system is based on dual licensing and local control,” said Alex Traverso, a spokesman for the state Bureau of Cannabis Control, referring to the requirement that cannabis businesses get permission from the state and the city in which they want to operate.
Less than 20% of cities in California — 89 of 482 — allow retail shops to sell cannabis for recreational use, according to the California Cannabis Industry Assn. Cities that allow cannabis sales include Los Angeles, Oakland, San Francisco and San Diego.
Coverage of California politics »
Eighty-two of Los Angeles County’s 88 cities prohibit retail sales of recreational marijuana, according to Alexa Halloran, an attorney specializing in cannabis law for the firm Solomon, Saltsman & Jamieson. Pot shops are not allowed in cities including Burbank, Manhattan Beach, Alhambra, Beverly Hills, Inglewood, Compton, Redondo Beach, El Monte, Rancho Palos Verdes and Calabasas.
“While some cities have jumped in headfirst, we’ve taken a deliberate approach,” said Manhattan Beach Mayor Steve Napolitano, “to see how things shake out elsewhere before further consideration. I think that’s proven to be the smart approach.”
Voters have also been reluctant to allow cannabis stores in their communities.
Of the 64 California cities and counties that voted on cannabis ballot measures in the November midterm election, eight banned the sale of cannabis or turned down taxation measures, seven allowed sales and 49 approved taxes on pot businesses, said Hilary Bricken, an attorney who represents the industry. Among them, voters in Malibu approved pot shops while Simi Valley residents voted for an advisory measure against allowing retail sales.
Javier Montes, owner of Wilmington pot store Delta-9 THC, says he is struggling to compete with a large illicit market unburdened by the taxes he pays as a licensed business.
“Because we are up against high taxes and the proliferation of illegal shops, it is difficult right now,” Montes said. “We expected lines out of our doors, but unfortunately the underground market was already conducting commercial cannabis activity and are continuing to do so.”
Montes, who received his city and state licenses in January, says his business faces a 15% state excise tax, a 10% recreational marijuana tax by the city of Los Angeles and 9.5% in sales tax by the county and state — a markup of more than 34%.
He says there isn’t enough enforcement against illegal operators, and the hard times have caused him to cut the number of employees at his shop in half this year from 24 to 12.
“It’s very hard whenever I have to lay people off, because they are like a family to me,” said Montes, who is vice president of the United Cannabis Business Assn., which represents firms including the about 170 cannabis retailers licensed by the city of Los Angeles.
DELTA-9 faces a 15% state excise tax, a 10% recreational cannabis tax by the city of Los Angeles and 9.5% in sales tax by the county and state, the shop owner says. (Marcus Yam / Los Angeles Times)
Sky Siegel, who operates a cannabis business in Studio City, said he recently gave up trying to open another store in Santa Monica because of its restrictions on such businesses.
“It turns into this ‘Hunger Games’ to try to get a license,” said Siegel, who is general manager of Perennial Holistic Wellness Center, which has a dozen employees in Studio City and also operates a delivery service.
He says his firm is up against thousands of unlicensed delivery services going into cities where storefronts are banned.
“To me, it doesn’t make sense” that many cities have prohibited shops, he said. “Banning does nothing. It’s already there. Why not turn this into a legitimized business, which is what the people want.”
Marijuana use is rising among pregnant patients. Not so fast, doctors warn »
California has also issued fewer cultivation licenses than expected in the first year of legalization, with about 2,160 growers registered with the state; an estimated 50,000 commercial cannabis cultivation operations existed before Proposition 64, according to the California Growers Assn. Some have given up growing pot, but many others are continuing to operate illegally.
The trade group hoped to see at least 5,000 commercial growers licensed in the first year, said Hezekiah Allen, the group’s former executive director who is now chairman of Emerald Grown, a cooperative of 130 licensed cultivators.
“We are lagging far behind,” Allen said. “It’s woefully inadequate. Most of the people in California who are buying cannabis are still buying it from the unregulated market. There just isn’t a reason for most growers to make the transition.”
Patrick McGreevy Dec 27, 2018
(Marcus Yam / Los Angeles Times)
Source: http://www.latimes.com/politics/la-pol-ca-marijuana-year-anniversary-review-20181227-story.html
Abstract
Background—As an increasing number of states liberalize cannabis use and develop laws and local policies, it is essential to better understand the impacts of neighborhood ecology and marijuana dispensary density on marijuana use, abuse, and dependence. We investigated associations between marijuana abuse/dependence hospitalizations and community demographic and environmental conditions from 2001–2012 in California, as well as cross-sectional associations between local and adjacent marijuana dispensary densities and marijuana hospitalizations.
Source: Drug Alcohol Depend. 2015 September 1; 154: 111–116. doi:10.1016/j.drugalcdep.
|
Booker released a statement on the bill on July 21, saying this can undo the damage done by the War on Drugs.
Meanwhile anti-legalization advocates like Kevin A. Sabet are doing all they can to prevent the bill from passing the Senate and becoming law.
However, regardless of the outcome, this bill is likely to change the discourse around cannabis for years to come.
State legalization and subsequent commercialization of marijuana has given the drug a glow up. The drug, once associated with potheads, illicit dealings, and pungent herbal smells is fast becoming a legal, family-friendly, trendy, and Instagram-worthy herbal medicine.
The expectation was that after legalization, marijuana would become more controlled and safe. The states that have made moves to legalize first medical marijuana, then recreational marijuana, however, observed increases in illicit dealings, hospital admission rates, and cannabis addiction and use.
Potency and concentration of cannabis and its derivatives, car crashes involving cannabis and abuse, and use in young people have also met new highs.
Marijuana is getting a foothold into medicine and households. It has been the most-consumed illicit drug globally and in the United States (pdf) for decades, though marijuana use is still far behind alcohol and tobacco.
The two words cannabis and marijuana are often used interchangeably, but there are differences in nuance. Cannabis generally refers to the entire cannabis plant, while marijuana refers to products made from cannabis such as dried leaves, or flowers. The word marijuana also implies that it is a cannabis product high in tetrahydrocannabinol (THC), the main constituent and the psychoactive derivative of cannabis.
Since legalization and commercialization, the THC content of cannabis products has been increasing. It has gone up from less than 2 percent (prior to the 1990s) to the current levels of 17 percent, and possibly even 30 percent as consumers seek bigger highs.

Some parents’, grandparents’, and educators’ memory of recreational weed is that of its humbler eras of 2 to 4 percent THC. There is a mismatch in perception, as high-THC level products are being packaged into innocent-looking gummies, candies, vapes, drinks, and many more. Though these are only legal for adult consumption, younger people are using it more than ever. Teenagers and young adults, whose brains are still in development, are consuming marijuana at unprecedented potencies. Marijuana use is linked with mental disorders, and memory and cognitive decline, with younger people the most at risk.
To add the cherry on top, researchers such as psychiatrist and professor Dr. Deepak D’Souza from Yale University, believes the high potencies, longer periods of use, may make findings from studies in the ’70s, ’80s, ’90s irrelevant to the current marijuana landscape.
“It’s the potency…the weed that’s available now [is] so different from what it was in the 1960s,” D’Souza told The Epoch Times.
Back then, weed was less accessible, less potent, and most people used it sporadically. Today, marijuana is more accessible, easily obtained in both licensed and unlicensed stores, increasingly potent, with an increased demographic of people taking the drug in the long-term.
“Studies done in the past would suggest that only about one in 10 people would develop a cannabis use disorder (addiction to cannabis),” D’Souza said. “I think more recent studies … in the current landscape of marijuana would suggest that that number is actually a lot higher than we previously thought.”

Marijuana acts on the endocannabinoid system that exists in the brain and spinal cord.
Researchers are not exactly sure how marijuana creates its euphoric effects, but studies suggest that it is the binding of THC to the endocannabinoid receptors in the brain that creates euphoria. There are two endocannabinoid receptors, CB1 receptors are in the brain and CB2 receptors are in the spinal cord. THC and most cannabinoids can bind to both.
Apart from THC, there is also another common cannabinoid: cannabidiol (CBD).
CBD, the second most common cannabinoid, also interacts with the endocannabinoid system, though its actions are more complex. CBD, however, does not give users the high found in THC. CBD is generally the active ingredient in medicinal marijuana, and there are many studies linking the cannabinoid with therapeutic properties including pain and seizures.
Since the 1900s, the potency of THC in recreational marijuana has been increasing, while CBD percentage has decreased. One can find 99 percent THC oils being dispensed. Consumers can add this to their vapes, or for other forms of consumption.
Though the general advice for younger people is to stay off the drug until adulthood, D’Souza senses that an increasing number of younger people are using weed recreationally, often unaware of the exact implications of consumption.
“More and more young people … are using cannabis, and they are getting younger,” he said. “And they’re using more potent forms.”
He is not wrong. Cannabis use in young people is reaching record rates, increasing from 37 percent in 2014 to 43 percent in 2019. Teenagers of today are also more likely to consume marijuana than tobacco.
Many studies have suggested that cannabis, especially its THC component, may affect neurodevelopment in growing brains, as it disrupt processes in the brain. The brain only completes its full maturation at about the age of 25 to 26. Some studies suggest maturation may come even later than that. During adolescence, brains go through “pruning,” which is a process where necessary brain cells and connections are strengthened and the unnecessary neurons are removed.
“The process of pruning is important, it’s really important in preparing the brain for the demands of adulthood,” D’Souza said.
The endocannabinoid system is also important in neurodevelopment. In our bodies we produce two chemicals that can bind to CB1 and CB2 receptors.
“One is called anandamide, named after the Sanskrit word meaning bliss,” he said. “And the other is called 2-AG.”
When the endocannabinoid system is activated, these chemicals will be released and bind to the receptors. The chemicals are specific. They act on a small targeted area and “produce the effects for just milliseconds before…they are inactivated.”
Researchers believe that the binding of these chemicals allows the brain to select what neurons will be strengthened and what neurons will be removed in neurodevelopment, according to D’Souza.
Whilst these two natural chemicals act for a very short, transient time, THC does not.
THC in the body can last for minutes to hours, smoked joints give a quick and strong burst in minutes but consumed THC in gummies and other food start slow and last for hours. THC is also non-selective and will bind to all the areas of the brain with these receptors, distorting the targeted communication in the brain.
“The scientific term we use is that THC produces effects that are … non physiological effects, and those … effects may have far reaching consequences.”
If the endocannabinoid system is, as researchers believe, “really important in directing … neurodevelopmental processes, you could imagine that when an adolescent whose brain is still maturing smokes cannabis, it may disrupt that process,” said D’Souza.
The prefrontal cortex, the area of the brain in charge of critical thinking and decision making, is the last area to fully mature. Research suggests that the maturation in this area is what separates teenagers and young adults from fully matured adults.
Brain scans of drug abusers often show a decreased brain matter volume in the prefrontal cortex, suggesting increased in impulsivity and poor decision making.
Since younger people have immature prefrontal cortexes, this may be why early marijuana use increases risks of addiction and brain impairment. A study found 10.7 percent of teenagers between the age of 12 and 17 developed an addiction to cannabis within 12 months of use, and 20.1 percent developed addiction after 3 years. For young adults aged 18 to 25, 6.4 percent developed addiction in a year, and 10.9 percent in three years.
Cannabis use is also linked to mental health disorders, especially in younger people, particularly those at risk of certain mental health disorders, including depression, psychosis, and schizophrenia.
Though it should be noted that not everyone who uses cannabis will develop mental health disorders and other health conditions, studies in younger people have linked the drug with various mental disorders including psychosis, schizophrenia (some studies suggest a causal link), anxiety, and depression. Some studies also link cannabis consumption with an exacerbation of present psychiatric symptoms. Schizophrenia has lifelong consequences and patients will need to be treated or monitored over their lifetime.
The majority of endocannabinoid receptors in the brain reside in the hippocampus, a seahorse structure deep in the brain important for memory formation and storage. Studies on long-term and short-term effects of cannabis have both found that cannabis affects learning and episodic memory.
Studies on adolescents have also found that cannabis use was associated with a reduced brain matter volume, a 2021 study found that it has been linked with brain aging, especially in the prefrontal cortex. Persistent use of cannabis in adolescence has also been associated with permanently reduced IQ by 5 to 13 points.

Though parenting plays a role in preventing teens from abusing cannabis and severe adverse effects, it can be hard for parents and educators to make the connection when their image of cannabis is mostly benign.
The industry is also trying to make cannabis appealing to the younger generations despite regulations prohibiting minor use.
D’Souza argued that the age limit that has been set is “disingenuous,” due to the investment in products that are enticing to pre-teens and teenagers.
“Companies are making gummy bears, gummy bears, I would hardly think that adults would be interested in gummy bears. That’s just a disingenuous way of marketing to young adults below the age,” D’Souza said.
“We really have done a poor job at educating the public.”

Studies shown that medicinal cannabis does have therapeutic effects against pain, chemo-therapy induced nausea and vomiting, and spasticity from multiple sclerosis.
There is also anecdotal evidence of the drug’s effects against seizures in neurodegenerative diseases and epilepsy.
However, regulation of medicinal marijuana use varies drastically across different states.
Connecticut, for example, approves medicinal marijuana use for over 40 conditions including cancer, amyotrophic lateral sclerosis, cystic fibrosis, multiple sclerosis, and many others. New York sets no limit on the number and type of conditions.
There are also states with strict laws; Wyoming only approved CBD-oils in 2015 and limited its use to seizures only.
Some studies also suggest benefits in Alzheimer’s disease, cancer, and depression, but “for the overwhelming majority of those conditions, there is very little evidence to support the benefits of marijuana for these conditions, with some exceptions,” said D’Souza.
Studies also found that most (around 90 percent) people taking medical marijuana reported that it reduced their symptoms, and two-thirds of them used less prescription medicines.
For the medical marijuana users that report addiction, around 80 percent use recreational marijuana.
Medical marijuana has helped people, but D’Souza argued that there are political motivations behind medicinal marijuana legalization. “Those who wanted to legalize marijuana realized and planned very early on that if they could get the public at large to accept medical marijuana, then it would be a very short step from there to make marijuana completely legal.”
“And that is exactly what is happening.”
Currently, 38 states have approved medical marijuana and 18 of these states also approved recreational marijuana use in adults.
The states first to approve marijuana medically were often also the first to approve it recreationally, with some exceptions:
Colorado and California were leaders in approving medical marijuana, doing so long before the movement for legalization gained momentum. Recreational approval only came after the movement gained momentum, thus these two states took 12 and 20 years respectively to legalize recreational marijuana. There are also states that were late to the overall medical marijuana program, but quickly approved recreational use, such as Massachusetts, and the district Washington DC. They legalized medical marijuana just ahead of the push for legal recreational marijuana use, and it took these two states only around 4 years to approve recreational marijuana.
Full legalization of cannabis often opened doors to commercialization. Each new policy further opened the doors for cannabis access, but these are not without health implications.
A study on youths from 2008 to 2016 in four states that legalized recreational cannabis (Colorado, Washington, Alaska, and Oregon) found that cannabis addictions reported in teenagers 12 to 17 increased from 2.18 to 2.72 percent—a 25 percent increase.
Colorado legalized medical marijuana in 2000, and was the first state to legalize recreational marijuana in 2012, before commercializing it in 2014.
Since its legalization, it saw increases in marijuana-involved traffic accidents, use and abuse in teenagers, hospital presentation from cannabis adverse effects, and poison center presentation for children and pets who unwittingly ingested cannabis from medicinal cabinets.
Hospitalizations for cannabis related adverse effects increased by 45 percent (pdf) between 2006 and 2008 (pre-commercialization of medical marijuana) to 2009 to 2012.
From Colorado’s post-commercialization period to 2013 to 2014 (legalization and commercialization period for recreational marijuana), hospitalizations for cannabis-related conditions increased by another 66 percent (pdf).
These hospitalizations do not come without repercussions, and hospitals are reporting financial losses from cannabis-related treatments. A study (pdf) examining one hospital in a municipality in Colorado found that from 2009 to 2014, hospitalizations from cannabis-related bills increased by 375 percent and emergency department (ED) submissions increased from 9 percent to 15.3 percent.
It should be noted that the municipality did not legalize cannabis under Amendment 64, however the hospital saw an increasing presentation to the ED for people experiencing adverse effects from marijuana, with the majority of hospitalizations mental health involved, including suicide ideation, depression, and so on.
From 2009 to 2014, the hospital incurred at least $20 million in losses from cannabis patients not paying their bills. Other studies examining hospital presentations in Colorado found that from 2000 to 2015, hospitalization rates with marijuana-related billing codes doubled from 274 in 2000 to 593 per 100,000 hospitalizations in 2015. ED visits from mental illness were five times higher for bills that had marijuana-related codes than bills without.
A study on poison center reports in Colorado found that child reports of cannabis ingestion doubled from 1.2 per 100 000 population in 2009 to 2.3 per 100,000 population in 2015, and half of these reports were from children ingesting cannabis-containing gummies, and brownies, both of which are appealing to children. Though arguably, the reports are less than crayon poisoning reports every year, however as legalization invariably increases marijuana exposures, poisoning from cannabis in children is only going to increase as the drug becomes increasingly socially acceptable.
Additionally, traffic deaths involving drivers who tested positive for marijuana also increased since legalization of recreational marijuana. Traffic deaths involving marijuana more than doubled from 55 people killed in 2013 to 115 in 2018. In 2019, there were 163 alcohol-impaired traffic deaths in Colorado.
Cannabis use in teenagers and young adults in Colorado have also mostly showed an increasing trend. In 2019, 15.5 percent of teenagers aged 15 and younger consumed cannabis in the past 30 days, compared to 15.4 percent in 2013. Teenagers aged 16 to 17, and 18 and older also saw general increases, reaching 24.4 and 27.5 percent respectively as compared to 22.5 and 25.3 percent in 2013.
D’Souza likened the popularity among the younger generation and commercialism of cannabis with tobacco and alcohol. “Even though alcohol is supposed to be sold only to people over the age of 21, it’s very easy for young people, adolescents to get their hands on alcohol, and likewise I would expect no different…with cannabis.”
Correction: A previous version of this article marked the 2009 to 2012 period as “(post-commercialization)” under the section Colorado: A Case Study. The terminology quoted from the report caused confusion and has since been removed. Colorado legalized recreational marijuana use in 2012 and state-licensed retail sales, or commercialization, in 2014.
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of The Epoch Times. Epoch Health welcomes professional discussion and friendly debate. To submit an opinion piece, please follow these guidelines and submit through our form here.
Source: How Modern Marijuana Changes the Brain (theepochtimes.com)
BY AND TIMEAUGUST 1, 2022
Source: https://prescribeddrug.org/appg-for-prescribed-drug-dependence-press-release-new-nice-guidance-to-tackle-prescribed-drug-dependence-fails-to-listen-to-patient-evidence/
Date: April 2022
Medical marijuana in Florida was approved by Governor Rick Scott last month and now school districts statewide are struggling with one specific requirement of the legislation. Under the law, children with certain ailments can use cannabis while at school and the districts are obligated to make it available to students as needed.
While medical marijuana for children is legal in Florida, the schools are resistant to creating cannabis-use policy as the language used in the law is ambiguous and inconsistent. The law requires schools to store and manage cannabis like other medications but does not provide a clear definition as to who can administer it to students.
Only an authorized caregiver can give medical marijuana to a child, yet the law does not afford school employees the power to act as a caregiver. Mitch Teitelbaum, an attorney for the Manatee County School District, says making schools provide the drug to students makes no sense when the school has no legal power to do so.
“The district is compelled to adhere to all state and federal laws,” said Teitelbaum, as reported by the Bradenton Herald. “But how do we do so with such inconsistency?”
The original medical cannabis law approved by Florida voters in November did not contain the school requirement provision, but was later modified to include it. This added amendment is causing both confusion and controversy to the new marijuana law.
Most Florida school districts turn to consulting firm NEOLA for help creating school policy. Currently, the company is reviewing the law and deciding how to move forward before making any recommendations to district officials.
According to NEOLA CEO Dick Clapp, Florida’s medical marijuana law puts “schools in a real tough spot” by making them create a policy that potentially opens them up to lawsuits. Once one district comes up with solid guidelines regulating how cannabis will be given to students, other districts are likely to follow. However, Clapp says that isn’t likely to happen before the start of the 2017-18 school year.
As of now, not many children are affected by the medical marijuana law in Florida. Yet, the families that are impacted want the state’s school districts or the Florida Department of Education to make a decision.
“The number of people that will be impacted will be a small number, but they are in dire situations, so it is a tough human-relations thing,” Clapp said, per the report by the Bradenton Herald. “I don’t know what we do about that.”
It is likely the Florida school districts with the highest number of students will act first to create medical marijuana guidelines. For now, the most probable scenario will be treating medical cannabis like any other prescription medication.
The medical marijuana law in Florida allows children with severe epilepsy, cancer, and other qualifying conditions to be treated with cannabis oil, capsules, and edibles. Due to federal restrictions regarding prescribing weed for medical purposes, marijuana treatment is only available by recommendation from state-approved physicians to Florida patients.
Source: https://www.inquisitr.com/4399383/medical-marijuana-in-florida-creates-policy-smoky-challenge-for-states-school-districts/ July 2017
Question Are US state medical marijuana laws one of the underlying factors for increases in risk for adult cannabis use and cannabis use disorders seen since the early 1990s?
Findings In this analysis using US national survey data collected in 1991-1992, 2001-2002, and 2012-2013 from 118 497 participants, the risk for cannabis use and cannabis use disorders increased at a significantly greater rate in states that passed medical marijuana laws than in states that did not.
Meaning Possible adverse consequences of illicit cannabis use due to more permissive state cannabis laws should receive consideration by voters, legislators, and policy and health care professionals, with appropriate health care planning as such laws change.
Importance Over the last 25 years, illicit cannabis use and cannabis use disorders have increased among US adults, and 28 states have passed medical marijuana laws (MML). Little is known about MML and adult illicit cannabis use or cannabis use disorders considered over time.
Objective To present national data on state MML and degree of change in the prevalence of cannabis use and disorders.
Design, Participants, and Setting Differences in the degree of change between those living in MML states and other states were examined using 3 cross-sectional US adult surveys: the National Longitudinal Alcohol Epidemiologic Survey (NLAES; 1991-1992), the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC; 2001-2002), and the National Epidemiologic Survey on Alcohol and Related Conditions–III (NESARC-III; 2012-2013). Early-MML states passed MML between NLAES and NESARC (“earlier period”). Late-MML states passed MML between NESARC and NESARC-III (“later period”).
Main Outcomes and Measures Past-year illicit cannabis use and DSM–IV cannabis use disorder.
Results Overall, from 1991-1992 to 2012-2013, illicit cannabis use increased significantly more in states that passed MML than in other states (1.4–percentage point more; SE, 0.5; P = .004), as did cannabis use disorders (0.7–percentage point more; SE, 0.3; P = .03). In the earlier period, illicit cannabis use and disorders decreased similarly in non-MML states and in California (where prevalence was much higher to start with). In contrast, in remaining early-MML states, the prevalence of use and disorders increased. Remaining early-MML and non-MML states differed significantly for use (by 2.5 percentage points; SE, 0.9; P = .004) and disorder (1.1 percentage points; SE, 0.5; P = .02). In the later period, illicit use increased by the following percentage points: never-MML states, 3.5 (SE, 0.5); California, 5.3 (SE, 1.0); Colorado, 7.0 (SE, 1.6); other early-MML states, 2.6 (SE, 0.9); and late-MML states, 5.1 (SE, 0.8). Compared with never-MML states, increases in use were significantly greater in late-MML states (1.6–percentage point more; SE, 0.6; P = .01), California (1.8–percentage point more; SE, 0.9; P = .04), and Colorado (3.5–percentage point more; SE, 1.5; P = .03). Increases in cannabis use disorder, which was less prevalent, were smaller but followed similar patterns descriptively, with change greater than never-MML states in California (1.0–percentage point more; SE, 0.5; P = .06) and Colorado (1.6–percentage point more; SE, 0.8; P = .04).
Conclusions and Relevance Medical marijuana laws appear to have contributed to increased prevalence of illicit cannabis use and cannabis use disorders. State-specific policy changes may also have played a role. While medical marijuana may help some, cannabis-related health consequences associated with changes in state marijuana laws should receive consideration by health care professionals and the public.
Source: https://jamanetwork.com/journals/jamapsychiatry/article-abstract/2619522 June 2017
In California, the crop ranks between lettuce and grapes; total sales in the state, according the Los Angeles Times, will top $21 billion by 2021. In Colorado, where marijuana is also legal, revenues stood at just over $1 billion last year, adding $2.4 billion to the state’s economy.
Those numbers are for legal farms. Illegal marijuana cultivation is much larger. It is estimated that there may be as many as ten million illegal plants grown annually, yielding over $30 billion worth of product.
In California, illegal pot is being grown on literally thousands of acres of the state’s national and state forests and parks, including in Stanislaus National Forest adjacent to Yosemite National Park. A one acre illegal patch can produce well over $1 million worth of marijuana per year. Much of the illegal harvest is sold in states where marijuana remains illegal – but where there is also huge demand, jacking up prices. Commerce in illegal marijuana is often controlled by the same Mexican drug lords who sell cocaine, heroin and contraband opioids; to make things worse, their illegal plots are often tended by illegal immigrants who are virtual slaves, guarded by thugs with high-powered weapons.
Pot production may rake in billions of dollars, but at immense environmental cost. Research has documented that marijuana cultivation, legal and illegal, is polluting water, land and air at an alarming rate. Both legal and illegal growers use large amounts of pesticides, insecticides and other chemicals and fertilizers banned in the U.S., illegally divert streams, and discharge polluted waste into waterways, poisoning the water supply, fish and animals. Growers have also clear cut trees and excavated forests illegally creating vast wastelands. When they move on to another illegal site, the old one is often the equivalent of a toxic waste site, saturated with poisons and fertilizers.
Despite evidence of significant criminal toxic waste discharge and other environmental crimes, not surprisingly the Obama Justice Department largely ignored the problem. In the liberal mindset, marijuana, unlike coal, oil and gas, is sacred stuff and considered outside the reach of the law. And there is little noise from the environmental movement which, if oil and gas or timber were the product, would be all over the issue like a wet blanket. But not marijuana.
A good example of the problems is Calaveras County made famous by Mark Twain, in the foothills of California’s Sierra Mountains. About the size of Rhode Island, it has a population of some 44,000 people. The County Board recently voted to ban commercial marijuana production – a prerogative under California’s law legalizing it. Their sheriff estimates there are at least 1200 illegal farms scattered through the mountainous terrain, all discharging large quantities of chemical waste into the water supply (nearly 10% of California’s water originates in little Calaveras County) and fouling the surrounding land with illegal herbicides, insecticides and rodenticides. Cleaning up those sites – just in Calaveras County — will cost, according to U.S. Forest Service estimates, at least $240 million; perhaps much more. Expand Calaveras’s problems across 15 other Northern California counties and the problem becomes almost unimaginable.
Environmental groups such as the Sierra Club and the Natural Resources Defense Council are nowhere to be found. Ironically it was these very mountains where Sierra Club founder John Muir hiked and studied for decades. I spoke with Dennis Mills, a member of the Calaveras County Board of Supervisors, who told me he has begged local and national environmentalist groups to get involved, but his pleas are always met, he said, with a yawn. Mills documented the abuses in a study Cultivating Disaster conducted by The Communications Institute.
So where is the federal government? Illegal and many legal marijuana farmers are likely in flagrant violation of numerous federal environmental criminal laws ranging from pollution crimes, wildlife and animal welfare crimes, and could be subject to large fines and restitution as well as lengthy prison sentences.
The Environmental Protection Agency, the Interior Department and Agriculture Department all have jurisdiction, and the Justice Department, complete with an Environmental Crimes Unit, together with California’s U.S. Attorneys, should be actively investigating these crimes, empaneling grand juries, and issuing indictments against these criminals.
The Trump Administration would do well to unleash its environmental lawyers on this nasty problem. It would greatly assist local and state agencies in dealing with the serious environmental mess caused by pot cultivation. It might not gain much support from marijuana users, but an aggressive campaign would undoubtedly create plenty of good will among the rest of the population and deal with a serious environmental problem.
Mr. Regnery, an Attorney, served in the Reagan Justice Department. He is Chairman of the Law Enforcement Legal Defense Fund.
Source: https://www.breitbart.com/politics/2018/02/25/regnery-feds-prosecute-california-marijuana-farmers-devastating-environment/February 2018

Ontario’s proposal to allow people to consume marijuana in hotel rooms opens the door to a boom in cannabis tourism, says lawyer Matt Maurer.
Maurer heads the cannabis law group at Minden Gross in Toronto, and says he knows businesspeople who are interested in opening cannabis-friendly hotels and resorts.
Maurer says he was surprised by the province’s proposal to loosen up the ban on consuming cannabis anywhere other than private homes. The government has also asked for public comments on whether to allow cannabis lounges.

Maurer said he assumed the provincial government would eventually consider exemptions to the cannabis act passed in December, which bans consumption in public places.
“I was surprised that it happened so quickly.”
Maurer calls consumption in hotels “step No. 1” in the development of a cannabis tourism industry.
“You could come to Ontario, go to the government-owned retail store, pick up your cannabis, head out to the hotel room, consume it there and head out to where ever you are going that evening, to a show or an event.”
The provincial regulations unveiled last month propose that cannabis could be consumed by residents and their guests at rooms in hotels, motels and inns, as long as the drug is not smoked or vaped. Smoking and vaping marijuana would be allowed in designated smoking rooms.
The regulations have been posted for public comment. The government plans to put them into effect when recreational marijuana is legalized across the country, expected in July.
Ontario has also opened the door to cannabis consumption lounges, asking for public comments on the idea. There’s no time frame for the lounges, but rules won’t be in place be by July. The province says the comments it receives will “inform future policy development and consultations.”
Abi Roach, who runs a cannabis vaping lounge in Toronto called Hotbox Cafe, says she’s interested in opening more if they become legal. She dreams of the day when lounges will be allowed to sell single servings of cannabis, just like drinks are served in a bar or restaurant.
At the Hotbox (slogan: “serving potheads since … ahh I forget”), guests pay a $5 entry fee and bring their own pot.

If Ontario allows lounges, they probably won’t feature smoking inside because of concerns over the health dangers of second-hand smoke to both customers and employees, said Roach. “I don’t like to be in a big smoky room, either.”
At the Hotbox, only vaping is allowed inside. Pot smokers puff at an outdoor patio.
Roach also sees a demand for pot-friendly hotels. She’s helping design a cannabis-themed room at a hotel to be built in downtown Toronto. Each room in the hotel is owned by a private investor and offers a themed experience. If cannabis consumption is made legal in hotel rooms, they’ll go ahead with that project.
However, Roach said she doubts if Canada will see a big influx of cannabis tourists from the U.S. because we’ll be competing with a growing number of American states that are legalizing pot, some of which have taken a more creative, freewheeling approach. Ontario plans to sell cannabis from behind the counter at a restricted number of government-run stores. That won’t appeal to people who want convenience and innovative products from craft producers, said Roach.
“Canada really has to be careful in terms of blocking innovation in this industry.”
Roach said she recently drove from Vancouver to Washington State, where she stopped at a gas station and bought a joint. “To me as a tourist, it was like, ‘Wow, this is great!’ ”
In the lvillage of Embrun 40 kilometres southeast of Ottawa, Frank Medewar says he plans to open a lounge if they are made legal. He already runs InfoCannabis, a service that advises people about medical marijuana, and Seed 2 Weed, a store that sells growing equipment.
Medewar says his lounge will be modern and upscale, similar to an old-fashioned cigar lounge.
At the headquarters of the world’s largest medical marijuana company, Canopy Growth Corp. in Smiths Falls, spokesman Jordan Sinclair said the company would love to make the huge grow-op a tourist destination.

Canopy is in a former Hershey chocolate factory that was famous for tours taken by thousands of schoolchildren and tourists.
Canopy plans to have the plant open for public tours this summer, said Sinclair.
The company would also like to run a retail store on site, so the experience would be similar to a winery tour. However, the province has nixed that idea.
At Ottawa Tourism, spokesperson Jantine Van Kregten said the legalization of cannabis is on the radar. However, she hasn’t heard of any specific plans for hotels or other tourist ventures. “I think everybody is kind of taking a wait-and-see approach. I haven’t heard a lot of talk, a lot of scuttlebutt, in the industry of what their plans are. I think a lot of questions are unanswered about exactly how the legislation will roll out.”
Source: https://ottawacitizen.com/news/local-news/ontario-proposal-to-allow-cannabis-consumption-in-hotel-rooms-could-jump-start-pot-tourism February 2018

You’re aware America is under siege, fighting an opioid crisis that has exploded into a public-health emergency. You’ve heard of OxyContin, the pain medication to which countless patients have become addicted. But do you know that the company that makes Oxy and reaps the billions of dollars in profits it generates is owned by one family?
The newly installed Sackler Courtyard at London’s Victoria and Albert Museum is one of the most glittering places in the developed world. Eleven thousand white porcelain tiles, inlaid like a shattered backgammon board, cover a surface the size of six tennis courts. According to the V&A;’s director, the regal setting is intended to serve as a “living room for London,” by which he presumably means a living room for Kensington, the museum’s neighborhood, which is among the world’s wealthiest. In late June, Kate Middleton, the Duchess of Cambridge, was summoned to consecrate the courtyard, said to be the earth’s first outdoor space made of porcelain; stepping onto the ceramic expanse, she silently mouthed, “Wow.”
The Sackler Courtyard is the latest addition to an impressive portfolio. There’s the Sackler Wing at New York’s Metropolitan Museum of Art, which houses the majestic Temple of Dendur, a sandstone shrine from ancient Egypt; additional Sackler wings at the Louvre and the Royal Academy; stand-alone Sackler museums at Harvard and Peking Universities; and named Sackler galleries at the Smithsonian, the Serpentine, and Oxford’s Ashmolean. The Guggenheim in New York has a Sackler Center, and the American Museum of Natural History has a Sackler Educational Lab. Members of the family, legendary in museum circles for their pursuit of naming rights, have also underwritten projects of a more modest caliber—a Sackler Staircase at Berlin’s Jewish Museum; a Sackler Escalator at the Tate Modern; a Sackler Crossing in Kew Gardens. A popular species of pink rose is named after a Sackler. So is an asteroid.
The Sackler name is no less prominent among the emerald quads of higher education, where it’s possible to receive degrees from Sackler schools, participate in Sackler colloquiums, take courses from professors with endowed Sackler chairs, and attend annual Sackler lectures on topics such as theoretical astrophysics and human rights. The Sackler Institute for Nutrition Science supports research on obesity and micronutrient deficiencies. Meanwhile, the Sackler institutes at Cornell, Columbia, McGill, Edinburgh, Glasgow, Sussex, and King’s College London tackle psychobiology, with an emphasis on early childhood development.
The Sacklers’ philanthropy differs from that of civic populists like Andrew Carnegie, who built hundreds of libraries in small towns, and Bill Gates, whose foundation ministers to global masses. Instead, the family has donated its fortune to blue-chip brands, braiding the family name into the patronage network of the world’s most prestigious, well-endowed institutions. The Sackler name is everywhere, evoking automatic reverence; the Sacklers themselves, however, are rarely seen.
The descendants of Mortimer and Raymond Sackler, a pair of psychiatrist brothers from Brooklyn, are members of a billionaire clan with homes scattered across Connecticut, London, Utah, Gstaad, the Hamptons, and, especially, New York City. It was not until 2015 that they were noticed by Forbes, which added them to the list of America’s richest families. The magazine pegged their wealth, shared among twenty heirs, at a conservative $14 billion. (Descendants of Arthur Sackler, Mortimer and Raymond’s older brother, split off decades ago and are mere multi-millionaires.) To a remarkable degree, those who share in the billions appear to have abided by an oath of omertà: Never comment publicly on the source of the family’s wealth.
That may be because the greatest part of that $14 billion fortune tallied by Forbes came from OxyContin, the narcotic painkiller regarded by many public-health experts as among the most dangerous products ever sold on a mass scale. Since 1996, when the drug was brought to market by Purdue Pharma, the American branch of the Sacklers’ pharmaceutical empire, more than two hundred thousand people in the United States have died from overdoses of OxyContin and other prescription painkillers. Thousands more have died after starting on a prescription opioid and then switching to a drug with a cheaper street price, such as heroin. Not all of these deaths are related to OxyContin—dozens of other painkillers, including generics, have flooded the market in the past thirty years. Nevertheless, Purdue Pharma was the first to achieve a dominant share of the market for long-acting opioids, accounting for more than half of prescriptions by 2001.
According to the Centers for Disease Control, fifty-three thousand Americans died from opioid overdoses in 2016, more than the thirty-six thousand who died in car crashes in 2015 or the thirty-five thousand who died from gun violence that year. This past July, Donald Trump’s Commission on Combating Drug Addiction and the Opioid Crisis, led by New Jersey governor Chris Christie, declared that opioids were killing roughly 142 Americans each day, a tally vividly described as “September 11th every three weeks.” The epidemic has also exacted a crushing financial toll: According to a study published by the American Public Health Association, using data from 2013—before the epidemic entered its current, more virulent phase—the total economic burden from opioid use stood at about $80 billion, adding together health costs, criminal-justice costs, and GDP loss from drug-dependent Americans leaving the workforce. Tobacco remains, by a significant multiple, the country’s most lethal product, responsible for some 480,000 deaths per year. But although billions have been made from tobacco, cars, and firearms, it’s not clear that any of those enterprises has generated a family fortune from a single product that approaches the Sacklers’ haul from OxyContin.
Even so, hardly anyone associates the Sackler name with their company’s lone blockbuster drug. “The Fords, Hewletts, Packards, Johnsons—all those families put their name on their product because they were proud,” said Keith Humphreys, a professor of psychiatry at Stanford University School of Medicine who has written extensively about the opioid crisis. “The Sacklers have hidden their connection to their product. They don’t call it ‘Sackler Pharma.’ They don’t call their pills ‘Sackler pills.’ And when they’re questioned, they say, ‘Well, it’s a privately held firm, we’re a family, we like to keep our privacy, you understand.’ ”
To the extent that the Sacklers have cultivated a reputation, it’s for being earnest healers, judicious stewards of scientific progress, and connoisseurs of old and beautiful things. Few are aware that during the crucial period of OxyContin’s development and promotion, Sackler family members actively led Purdue’s day-to-day affairs, filling the majority of its board slots and supplying top executives. By any assessment, the family’s leaders have pulled off three of the great marketing triumphs of the modern era: The first is selling OxyContin; the second is promoting the Sackler name; and the third is ensuring that, as far as the public is aware, the first and the second have nothing to do with one another.
If you head north on I-95 through Stamford, Connecticut, you will spot, on the left, a giant misshapen glass cube. Along the building’s top edge, white lettering spells out ONE STAMFORD FORUM. No markings visible from the highway indicate the presence of the building’s owner and chief occupant, Purdue Pharma.
Originally known as Purdue Frederick, the first iteration of the company was founded in 1892 on New York’s Lower East Side as a peddler of patent medicines. For decades, it sustained itself with sales of Gray’s Glycerine Tonic, a sherry-based liquid of “broad application” marketed as a remedy for everything from anemia to tuberculosis. The company was purchased in 1952 by Arthur Sackler, thirty-nine, and was run by his brothers, Mortimer, thirty- six, and Raymond, thirty-two. The Sackler brothers came from a family of Jewish immigrants in Flatbush, Brooklyn. Arthur was a headstrong and ambitious provider, setting the tone—and often choosing the path—for his younger brothers. After attending medical school on Arthur’s dime, Mortimer and Raymond followed him to jobs at the Creedmoor psychiatric hospital in Queens. There, they coauthored more than one hundred studies on the biochemical roots of mental illness. The brothers’ research was promising—they were among the first to identify a link between psychosis and the hormone cortisone—but their findings were mostly ignored by their professional peers, who, in keeping with the era, favored a Freudian model of mental illness.
Concurrent with his psychiatric work, Arthur Sackler made his name in pharmaceutical advertising, which at the time consisted almost exclusively of pitches from so-called “detail men” who sold drugs to doctors door-to-door. Arthur intuited that print ads in medical journals could have a revolutionary effect on pharmaceutical sales, especially given the excitement surrounding the “miracle drugs” of the 1950s—steroids, antibiotics, antihistamines, and psychotropics. In 1952, the same year that he and his brothers acquired Purdue, Arthur became the first adman to convince The Journal of the American Medical Association, one of the profession’s most august publications, to include a color advertorial brochure.
In the 1960s, Arthur was contracted by Roche to develop an advertising strategy for a new antianxiety medication called Valium. This posed a challenge, because the effects of the medication were nearly indistinguishable from those of Librium, another Roche tranquilizer that was already on the market. Arthur differentiated Valium by audaciously inflating its range of indications. Whereas Librium was sold as a treatment for garden- variety anxiety, Valium was positioned as an elixir for a problem Arthur christened “psychic tension.” According to his ads, psychic tension, the forebear of today’s “stress,” was the secret culprit behind a host of somatic conditions, including heartburn, gastrointestinal issues, insomnia, and restless-leg syndrome. The campaign was such a success that for a time Valium became America’s most widely prescribed medication—the first to reach more than $100 million in sales. Arthur, whose compensation depended on the volume of pills sold, was richly rewarded, and he later became one of the first inductees into the Medical Advertising Hall of Fame.
As Arthur’s fortune grew, he turned his acquisitive instincts to the art market, quickly amassing the world’s largest private collection of ancient Chinese artifacts. According to a memoir by Marietta Lutze, his second wife, collecting, exhibiting, owning, and donating art fed Arthur’s “driving necessity for prestige and recognition.” Rewarding at first, collecting soon became a mania that took over his life. “Boxes of artifacts of tremendous value piled up in numerous storage locations,” she wrote, “there was too much to open, too much to appreciate; some objects known only by a packing list.” Under an avalanche of “ritual bronzes and weapons, mirrors and ceramics, inscribed bones and archaic jades,” their lives were “often in chaos.” “Addiction is a curse,” Lutze noted, “be it drugs, women, or collecting.”
When Arthur donated his art and money to museums, he often imposed onerous terms. According to a memoir written by Thomas Hoving, the Met director from 1967 to 1977, when Arthur established the Sackler Gallery at the Metropolitan Museum of Art to house Chinese antiquities, in 1963, he required the museum to collaborate on a byzantine tax-avoidance maneuver. In accordance with the scheme, the museum first soldArthur a large quantity of ancient artifacts at the deflated 1920s prices for which they had originally been acquired. Arthur then donated back the artifacts at 1960s prices, in the process taking a tax deduction so hefty that it likely exceeded the value of his initial donation. Three years later, in connection with another donation, Arthur negotiated an even more unusual arrangement. This time, the Met opened a secret chamber above the museum’s auditorium to provide Arthur with free storage for some five thousand objects from his private collection, relieving him of the substantial burden of fire protection and other insurance costs. (In an email exchange, Jillian Sackler, Arthur’s third wife, called Hoving’s tax-deduction story “fake news.” She also noted that New York’s attorney general conducted an investigation into Arthur’s dealings with the Met and cleared him of wrongdoing.)
In 1974, when Arthur and his brothers made a large gift to the Met—$3.5 million, to erect the Temple of Dendur—they stipulated that all museum signage, catalog entries, and bulletins referring to objects in the newly opened Sackler Wing had to include the names of all three brothers, each followed by “M.D.” (One museum official quipped, “All that was missing was a note of their office hours.”)
Hoving said that the Met hoped that Arthur would eventually donate his collection to the museum, but over time Arthur grew disgruntled over a series of rankling slights. For one, the Temple of Dendur was being rented out for parties, including a dinner for the designer Valentino, which Arthur called “disgusting.” According to Met chronicler Michael Gross, he was also denied that coveted ticket of arrival, a board seat. (Jillian Sackler said it was Arthur who rejected the board seat, after repeated offers by the museum.) In 1982, in a bad breakup with the Met, Arthur donated the best parts of his collection, plus $4 million, to the Smithsonian in Washington, D. C.
Arthur’s younger brothers, Mortimer and Raymond, looked so much alike that when they worked together at Creedmoor, they fooled the staff by pretending to be one another. Their physical similarities did not extend to their personalities, however. Tage Honore, Purdue’s vice-president of discovery of research from 2000 to 2005, described them as “like day and night.” Mortimer, said Honore, was “extroverted—a ‘world man,’ I would call it.” He acquired a reputation as a big-spending, transatlantic playboy, living most of the year in opulent homes in England, Switzerland, and France. (In 1974, he renounced his U. S. citizenship to become a citizen of Austria, which infuriated his patriotic older brother.) Like Arthur, Mortimer became a major museum donor and married three wives over the course of his life.
 Mortimer had his own feuds with the Met. On his seventieth birthday, in 1986, the museum agreed to make the Temple of Dendur available to him for a party but refused to allow him to redecorate the ancient shrine: Together with other improvements, Mortimer and his interior designer, flown in from Europe, had hoped to spiff up the temple by adding extra pillars. Also galling to Mortimer was the sale of naming rights for one of the Sackler Wing’s balconies to a donor from Japan. “They sold it twice,” Mortimer fumed to a reporter from New York magazine. Raymond, the youngest brother, cut a different figure—“a family man,” said Honore. Kind and mild-mannered, he stayed with the same woman his entire life. Lutze concluded that Raymond owed his comparatively serene nature to having missed the worst years of the Depression. “He had summer vacations in camp, which Arthur never had,” she wrote. “The feeling of the two older brothers about the youngest was, ‘Let the kid enjoy himself.’ ”
Mortimer had his own feuds with the Met. On his seventieth birthday, in 1986, the museum agreed to make the Temple of Dendur available to him for a party but refused to allow him to redecorate the ancient shrine: Together with other improvements, Mortimer and his interior designer, flown in from Europe, had hoped to spiff up the temple by adding extra pillars. Also galling to Mortimer was the sale of naming rights for one of the Sackler Wing’s balconies to a donor from Japan. “They sold it twice,” Mortimer fumed to a reporter from New York magazine. Raymond, the youngest brother, cut a different figure—“a family man,” said Honore. Kind and mild-mannered, he stayed with the same woman his entire life. Lutze concluded that Raymond owed his comparatively serene nature to having missed the worst years of the Depression. “He had summer vacations in camp, which Arthur never had,” she wrote. “The feeling of the two older brothers about the youngest was, ‘Let the kid enjoy himself.’ ”
Raymond led Purdue Frederick as its top executive for several decades, while Mortimer led Napp Pharmaceuticals, the family’s drug company in the UK. (In practice, a family spokesperson said, “the brothers worked closely together leading both companies.”) Arthur, the adman, had no official role in the family’s pharmaceutical operations. According to Barry Meier’s Pain Killer, a prescient account of the rise of OxyContin published in 2003, Raymond and Mortimer bought Arthur’s share in Purdue from his estate for $22.4 million after he died in 1987. In an email exchange, Arthur’s daughter Elizabeth Sackler, a historian of feminist art who sits on the board of the Brooklyn Museum and supports a variety of progressive causes, emphatically distanced her branch of the family from her cousins’ businesses. “Neither I, nor my siblings, nor my children have ever had ownership in or any benefit whatsoever from Purdue Pharma or OxyContin,” she wrote, while also praising “the breadth of my father’s brilliance and important works.” Jillian, Arthur’s widow, said her husband had died too soon: “His enemies have gotten the last word.”
The Sacklers have been millionaires for decades, but their real money—the painkiller money—is of comparatively recent vintage. The vehicle of that fortune was OxyContin, but its engine, the driving power that made them so many billions, was not so much the drug itself as it was Arthur’s original marketing insight, rehabbed for the era of chronic-pain management. That simple but profitable idea was to take a substance with addictive properties—in Arthur’s case, a benzo; in Raymond and Mortimer’s case, an opioid—and market it as a salve for a vast range of indications.
In the years before it swooped into the pain-management business, Purdue had been a small industry player, specializing in over-the-counter remedies like ear-wax remover and laxatives. Its most successful product, acquired in 1966, was Betadine, a powerful antiseptic purchased in industrial quantities by the U. S. government to prevent infection among wounded soldiers in Vietnam. The turning point, according to company lore, came in 1972, when a London doctor working for Cicely Saunders, the Florence Nightingale of the modern hospice movement, approached Napp with the idea of creating a timed-release morphine pill. A long-acting morphine pill, the doctor reasoned, would allow dying cancer patients to sleep through the night without an IV. At the time, treatment with opioids was stigmatized in the United States, owing in part to a heroin epidemic fueled by returning Vietnam veterans. “Opiophobia,” as it came to be called, prevented skittish doctors from treating most patients, including nearly all infants, with strong pain medication of any kind. In hospice care, though, addiction was not a concern: It didn’t matter whether terminal patients became hooked in their final days. Over the course of the seventies, building on a slow-release technology the company had already developed for an asthma medication, Napp created what came to be known as the “Contin” system. In 1981, Napp introduced a timed-release morphine pill in the UK; six years later, Purdue brought the same drug to market in the U. S. as MS Contin.
MS Contin quickly became the gold standard for pain relief in cancer care. At the same time, a number of clinicians associated with the burgeoning chronic-pain movement started advocating the use of powerful opioids for noncancer conditions like back pain and neuropathic pain, afflictions that at their worst could be debilitating. In 1986, two doctors from Memorial Sloan Kettering hospital in New York published a fateful article in a medical journal that purported to show, based on a study of thirty-eight patients, that long-term opioid treatment was safe and effective so long as patients had no history of drug abuse. Soon enough, opioid advocates dredged up a letter to the editor published in The New England Journal of Medicine in 1980 that suggested, based on a highly unrepresentative cohort, that the risk of addiction from long-term opioid use was less than 1 percent. Though ultimately disavowed by its author, the letter ended up getting cited in medical journals more than six hundred times.
 As the country was reexamining pain, Raymond’s eldest son, Richard Sackler, was searching for new applications for Purdue’s timed-release Contin system. “At all the meetings, that was a constant source of discussion—‘What else can we use the Contin system for?’ ” said Peter Lacouture, a senior director of clinical research at Purdue from 1991 to 2001. “And that’s where Richard would fire some ideas—maybe antibiotics, maybe chemotherapy—he was always out there digging.” Richard’s spitballing wasn’t idle blather. A trained physician, he treasured his role as a research scientist and appeared as an inventor on dozens of the company’s patents (though not on the patents for OxyContin). In the tradition of his uncle Arthur, Richard was also fascinated by sales messaging. “He was very interested in the commercial side and also very interested in marketing approaches,” said Sally Allen Riddle, Purdue’s former executive director for product management. “He didn’t always wait for the research results.” (A Purdue spokesperson said that Richard “always considered relevant scientific information when making decisions.”)
As the country was reexamining pain, Raymond’s eldest son, Richard Sackler, was searching for new applications for Purdue’s timed-release Contin system. “At all the meetings, that was a constant source of discussion—‘What else can we use the Contin system for?’ ” said Peter Lacouture, a senior director of clinical research at Purdue from 1991 to 2001. “And that’s where Richard would fire some ideas—maybe antibiotics, maybe chemotherapy—he was always out there digging.” Richard’s spitballing wasn’t idle blather. A trained physician, he treasured his role as a research scientist and appeared as an inventor on dozens of the company’s patents (though not on the patents for OxyContin). In the tradition of his uncle Arthur, Richard was also fascinated by sales messaging. “He was very interested in the commercial side and also very interested in marketing approaches,” said Sally Allen Riddle, Purdue’s former executive director for product management. “He didn’t always wait for the research results.” (A Purdue spokesperson said that Richard “always considered relevant scientific information when making decisions.”)
Perhaps the most private member of a generally secretive family, Richard appears nowhere on Purdue’s website. From public records and conversations with former employees, though, a rough portrait emerges of a testy eccentric with ardent, relentless ambitions. Born in 1945, he holds degrees from Columbia University and NYU Medical School. According to a bio on the website of the Koch Institute for Integrative Cancer Research at MIT, where Richard serves on the advisory board, he started working at Purdue as his father’s assistant at age twenty-six before eventually leading the firm’s R&D; division and, separately, its sales and marketing division. In 1999, while Mortimer and Raymond remained Purdue’s co-CEOs, Richard joined them at the top of the company as president, a position he relinquished in 2003 to become cochairman of the board. The few publicly available pictures of him are generic and sphinxlike—a white guy with a receding hairline. He is one of the few Sacklers to consistently smile for the camera. In a photo on what appears to be his Facebook profile, Richard is wearing a tan suit and a pink tie, his right hand casually scrunched into his pocket, projecting a jaunty charm. Divorced in 2013, he lists his relationship status on the profile as “It’s complicated.”
Richard’s political contributions have gone mostly to Republicans—including Strom Thurmond and Herman Cain—though at times he has also given to Democrats. (His ex-wife, Beth Sackler, has given almost exclusively to Democrats.) In 2008, he wrote a letter to the editor of The Wall Street Journaldenouncing Muslim support for suicide bombing, a concern that seems to persist: Since 2014, his charitable organization, the Richard and Beth Sackler Foundation, has donated to several anti-Muslim groups, including three organizations classified as hate groups by the Southern Poverty Law Center. (The family spokesperson said, “It was never Richard Sackler’s intention to donate to an anti-Muslim or hate group.”) The foundation has also donated to True the Vote, the “voter-fraud watchdog” that was the original source for Donald Trump’s inaccurate claim that three million illegal immigrants voted in the 2016 election.
Former employees describe Richard as a man with an unnerving intelligence, alternately detached and pouncing. In meetings, his face was often glued to his laptop. “This was pre-smartphone days,” said Riddle. “He’d be typing away and you would think he wasn’t even listening, and then all of the sudden his head would pop up and he’d be asking a very pointed question.” He was notorious for peppering subordinates with unexpected, rapid-fire queries, sometimes in the middle of the night. “Richard had the mind of someone who’s going two hundred miles an hour,” said Lacouture. “He could be a little bit disconnected in the way he would communicate. Whether it was on the weekend or a holiday or a Christmas party, you could always expect the unexpected.”
Richard also had an appetite for micromanagement. “I remember one time he mailed out a rambling sales bulletin,” said Shelby Sherman, a Purdue sales rep from 1974 to 1998. “And right in the middle, he put in, ‘If you’re reading this, then you must call my secretary at this number and give her this secret password.’ He wanted to check and see if the reps were reading this shit. We called it ‘Playin’ Passwords.’ ” According to Sherman, Richard started taking a more prominent role in the company during the early 1980s. “The shift was abrupt,” he said. “Raymond was just so nice and down-to-earth and calm and gentle.” When Richard came, “things got a lot harder. Richard really wanted Purdue to be big—I mean really big.”
 To effectively capitalize on the chronic-pain movement, Purdue knew it needed to move beyond MS Contin. “Morphine had a stigma,” said Riddle. “People hear the word and say, ‘Wait a minute, I’m not dying or anything.’ ” Aside from its terminal aura, MS Contin had a further handicap: Its patent was set to expire in the late nineties. In a 1990 memo addressed to Richard and other executives, Purdue’s VP of clinical research, Robert Kaiko, suggested that the company work on a pill containing oxycodone, a chemical similar to morphine that was also derived from the opium poppy. When it came to branding, oxycodone had a key advantage: Although it was 50 percent stronger than morphine, many doctors believed—wrongly—that it was substantially less powerful. They were deceived about its potency in part because oxycodone was widely known as one of the active ingredients in Percocet, a relatively weak opioid- acetaminophen combination that doctors often prescribed for painful injuries. “It really didn’t have the same connotation that morphine did in people’s minds,” said Riddle.
To effectively capitalize on the chronic-pain movement, Purdue knew it needed to move beyond MS Contin. “Morphine had a stigma,” said Riddle. “People hear the word and say, ‘Wait a minute, I’m not dying or anything.’ ” Aside from its terminal aura, MS Contin had a further handicap: Its patent was set to expire in the late nineties. In a 1990 memo addressed to Richard and other executives, Purdue’s VP of clinical research, Robert Kaiko, suggested that the company work on a pill containing oxycodone, a chemical similar to morphine that was also derived from the opium poppy. When it came to branding, oxycodone had a key advantage: Although it was 50 percent stronger than morphine, many doctors believed—wrongly—that it was substantially less powerful. They were deceived about its potency in part because oxycodone was widely known as one of the active ingredients in Percocet, a relatively weak opioid- acetaminophen combination that doctors often prescribed for painful injuries. “It really didn’t have the same connotation that morphine did in people’s minds,” said Riddle.
A common malapropism led to further advantage for Purdue. “Some people would call it oxy-codeine” instead of oxycodone, recalled Lacouture. “Codeine is very weak.” When Purdue eventually pleaded guilty to felony charges in 2007 for criminally “misbranding” OxyContin, it acknowledged exploiting doctors’ misconceptions about oxycodone’s strength. In court documents, the company said it was “well aware of the incorrect view held by many physicians that oxycodone was weaker than morphine” and “did not want to do anything ‘to make physicians think that oxycodone was stronger or equal to morphine’ or to ‘take any steps . . . that would affect the unique position that OxyContin’ ” held among physicians.
Purdue did not merely neglect to clear up confusion about the strength of OxyContin. As the company later admitted, it misleadingly promoted OxyContin as less addictive than older opioids on the market. In this deception, Purdue had a big assist from the FDA, which allowed the company to include an astonishing labeling claim in OxyContin’s package insert: “Delayed absorption, as provided by OxyContin tablets, is believed to reduce the abuse liability of a drug.”
 The theory was that addicts would shy away from timed-released drugs, preferring an immediate rush. In practice, OxyContin, which crammed a huge amount of pure narcotic into a single pill, became a lusted-after target for addicts, who quickly discovered that the timed-release mechanism in OxyContin was easy to circumvent—you could simply crush a pill and snort it to get most of the narcotic payload in a single inhalation. This wasn’t exactly news to the manufacturer: OxyContin’s own packaging warned that consuming broken pills would thwart the timed-release system and subject patients to a potentially fatal overdose. MS Contin had contended with similar vulnerabilities, and as a result commanded a hefty premium on the street. But the “reduced abuse liability” claim that added wings to the sales of OxyContin had not been approved for MS Contin. It was removed from OxyContin in 2001 and would never be approved again for any other opioid.
The theory was that addicts would shy away from timed-released drugs, preferring an immediate rush. In practice, OxyContin, which crammed a huge amount of pure narcotic into a single pill, became a lusted-after target for addicts, who quickly discovered that the timed-release mechanism in OxyContin was easy to circumvent—you could simply crush a pill and snort it to get most of the narcotic payload in a single inhalation. This wasn’t exactly news to the manufacturer: OxyContin’s own packaging warned that consuming broken pills would thwart the timed-release system and subject patients to a potentially fatal overdose. MS Contin had contended with similar vulnerabilities, and as a result commanded a hefty premium on the street. But the “reduced abuse liability” claim that added wings to the sales of OxyContin had not been approved for MS Contin. It was removed from OxyContin in 2001 and would never be approved again for any other opioid.
The year after OxyContin’s release, Curtis Wright, the FDA examiner who approved the pharmaceutical’s original application, quit. After a stint at another pharmaceutical company, he began working for Purdue. In an interview with Esquire, Wright defended his work at the FDA and at Purdue. “At the time, it was believed that extended-release formulations were intrinsically less abusable,” he insisted. “It came as a rather big shock to everybody—the government and Purdue—that people found ways to grind up, chew up, snort, dissolve, and inject the pills.” Preventing abuse, he said, had to be balanced against providing relief to chronic-pain sufferers. “In the mid-nineties,” he recalled, “the very best pain specialists told the medical community they were not prescribing opioids enough. That was not something generated by Purdue—that was not a secret plan, that was not a plot, that was not a clever marketing ploy. Chronic pain is horrible. In the right circumstances, opioid therapy is nothing short of miraculous; you give people their lives back.” In Wright’s account, the Sacklers were not just great employers, they were great people. “No company in the history of pharmaceuticals,” he said, “has worked harder to try to prevent abuse of their product than Purdue.”
Purdue did not invent the chronic-pain movement, but it used that movement to engineer a crucial shift. Wright is correct that in the nineties patients suffering from chronic pain often received inadequate treatment. But the call for clinical reforms also became a flexible alibi for overly aggressive prescribing practices. By the end of the decade, clinical proponents of opioid treatment, supported by millions in funding from Purdue and other pharmaceutical companies, had organized themselves into advocacy groups with names like the American Pain Society and the American Academy of Pain Medicine. (Purdue also launched its own group, called Partners Against Pain.) As the decade wore on, these organizations, which critics have characterized as front groups for the pharmaceutical industry, began pressuring health regulators to make pain “the fifth vital sign”—a number, measured on a subjective ten-point scale, to be asked and recorded at every doctor’s visit. As an internal strategy document put it, Purdue’s ambition was to “attach an emotional aspect to noncancer pain” so that doctors would feel pressure to “treat it more seriously and aggressively.” The company rebranded pain relief as a sacred right: a universal narcotic entitlement available not only to the terminally ill but to every American.
OxyContin’s sales started out small in 1996, in part because Purdue first focused on the cancer market to gain formulary acceptance from HMOs and state Medicaid programs. Over the next several years, though, the company doubled its sales force to six hundred—equal to the total number of DEA diversion agents employed to combat the sale of prescription drugs on the black market—and began targeting general practitioners, dentists, OB/GYNs, physician assistants, nurses, and residents. By 2001, annual OxyContin sales had surged past $1 billion. Sales reps were encouraged to downplay addiction risks. “It was sell, sell, sell,” recalled Sherman. “We were directed to lie. Why mince words about it? Greed took hold and overruled everything. They saw that potential for billions of dollars and just went after it.” Flush with cash, Purdue pioneered a high-cost promotion strategy, effectively providing kickbacks—which were legal under American law—to each part of the distribution chain. Wholesalers got rebates in exchange for keeping OxyContin off prior authorization lists. Pharmacists got refunds on their initial orders. Patients got coupons for thirty- day starter supplies. Academics got grants. Medical journals got millions in advertising. Senators and members of Congress on key committees got donations from Purdue and from members of the Sackler family.
 It was doctors, though, who received the most attention. “We used to fly doctors to these ‘seminars,’ ” said Sherman, which were, in practice, “just golf trips to Pebble Beach. It was graft.” Though offering perks and freebies to doctors was hardly uncommon in the industry, it was unprecedented in the marketing of a Schedule II narcotic. For some physicians, the junkets to sunny locales weren’t enough to persuade them to prescribe. To entice the holdouts—a group the company referred to internally as “problem doctors”—the reps would dangle the lure of Purdue’s lucrative speakers’ bureau. “Everybody was automatically approved,” said Sherman. “We would set up these little dinners, and they’d make their little fifteen-minute talk, and they’d get $500.”
It was doctors, though, who received the most attention. “We used to fly doctors to these ‘seminars,’ ” said Sherman, which were, in practice, “just golf trips to Pebble Beach. It was graft.” Though offering perks and freebies to doctors was hardly uncommon in the industry, it was unprecedented in the marketing of a Schedule II narcotic. For some physicians, the junkets to sunny locales weren’t enough to persuade them to prescribe. To entice the holdouts—a group the company referred to internally as “problem doctors”—the reps would dangle the lure of Purdue’s lucrative speakers’ bureau. “Everybody was automatically approved,” said Sherman. “We would set up these little dinners, and they’d make their little fifteen-minute talk, and they’d get $500.”
Between 1996 and 2001, the number of OxyContin prescriptions in the United States surged from about three hundred thousand to nearly six million, and reports of abuse started to bubble up in places like West Virginia, Florida, and Maine. (Research would later show a direct correlation between prescription volume in an area and rates of abuse and overdose.) Hundreds of doctors were eventually arrested for running pill mills. According to an investigation in the Los Angeles Times, even though Purdue kept an internal list of doctors it suspected of criminal diversion, it didn’t volunteer this information to law enforcement until years later.
As criticism of OxyContin mounted through the aughts, Purdue responded with symbolic concessions while retaining its volume-driven business model. To prevent addicts from forging prescriptions, the company gave doctors tamper-resistant prescription pads; to mollify pharmacists worried about robberies, Purdue offered to replace, free of charge, any stolen drugs; to gather data on drug abuse and diversion, the company launched a national monitoring program called RADARS.
Critics were not impressed. In a letter to Richard Sackler in July 2001, Richard Blumenthal, then Connecticut’s attorney general and now a U. S. senator, called the company’s efforts “cosmetic.” As Blumenthal had deduced, the root problem of the prescription-opioid epidemic was the high volume of prescriptions written for powerful opioids. “It is time for Purdue Pharma to change its practices,” Blumenthal warned Richard, “not just its public-relations strategy.”
It wasn’t just that doctors were writing huge numbers of prescriptions; it was also that the prescriptions were often for extraordinarily high doses. A single dose of Percocet contains between 2.5 and 10mg of oxycodone. OxyContin came in 10-, 20-, 30-, 40-, and 80mg formulations and, for a time, even 160mg. Purdue’s greatest competitive advantage in dominating the pain market, it had determined early on, was that OxyContin lasted twelve hours, enough to sleep through the night. But for many patients, the drug lasted only six or eight hours, creating a cycle of crash and euphoria that one academic called “a perfect recipe for addiction.” When confronted with complaints about “breakthrough pain”—meaning that the pills weren’t working as long as advertised—Purdue’s sales reps were given strict instructions to tell doctors to strengthen the dose rather than increase dosing frequency.
Over the next several years, dozens of class-action lawsuits were brought against Purdue. Many were dismissed, but in some cases Purdue wrote big checks to avoid going to trial. Several plaintiffs’ lawyers found that the company was willing to go to great lengths to prevent Richard Sackler from having to testify under oath. “They didn’t want him deposed, I can tell you that much,” recalled Marvin Masters, a lawyer who brought a class-action suit against Purdue in the early 2000s in West Virginia. “They were willing to sit down and settle the case to keep from doing that.” Purdue tried to get Richard removed from the suit, but when that didn’t work, the company settled with the plaintiffs for more than $20 million. Paul Hanly, a New York class-action lawyer who won a large settlement from Purdue in 2007, had a similar recollection. “We were attempting to take Richard Sackler’s deposition,” he said, “around the time that they agreed to a settlement.” (A spokesperson for the company said, “Purdue did not settle any cases to avoid the deposition of Dr. Richard Sackler, or any other individual.”)
When the federal government finally stepped in, in 2007, it extracted historic terms of surrender from the company. Purdue pleaded guilty to felony charges, admitting that it had lied to doctors about OxyContin’s abuse potential. (The technical charge was “misbranding a drug with intent to defraud or mislead.”) Under the agreement, the company paid $600 million in fines and its three top executives at the time—its medical director, general counsel, and Richard’s successor as president—pleaded guilty to misdemeanor charges. The executives paid $34.5 million out of their own pockets and performed four hundred hours of community service. It was one of the harshest penalties ever imposed on a pharmaceutical company. (In a statement to Esquire, Purdue said that it “abides by the highest ethical standards and legal requirements.” The statement went on: “We want physicians to use their professional judgment, and we were not trying to pressure them.”)
No Sacklers were named in the 2007 suit. Indeed, the Sackler name appeared nowhere in the plea agreement, even though Richard had been one of the company’s top executives during most of the period covered by the settlement. He did eventually have to give a deposition in 2015, in a case brought by Kentucky’s attorney general. Richard’s testimony—the only known record of a Sackler speaking about the crisis the family’s company helped create—was promptly sealed. (In 2016, STAT, an online magazine owned by Boston Globe Media that covers health and medicine, asked a court in Kentucky to unseal the deposition, which is said to have lasted several hours. STAT won a lower-court ruling in May 2016. As of press time, the matter was before an appeals court.)
In 2010, Purdue executed a breathtaking pivot: Embracing the arguments critics had been making for years about OxyContin’s susceptibility to abuse, the company released a new formulation of the medication that was harder to snort or inject. Purdue seized the occasion to rebrand itself as an industry leader in abuse-deterrent technology. The change of heart coincided with two developments: First, an increasing number of addicts, unable to afford OxyContin’s high street price, were turning to cheaper alternatives like heroin; second, OxyContin was nearing the end of its patents. Purdue suddenly argued that the drug it had been selling for nearly fifteen years was so prone to abuse that generic manufacturers should not be allowed to copy it.
On April 16, 2013, the day some of the key patents for OxyContin were scheduled to expire, the FDA followed Purdue’s lead, declaring that no generic versions of the original OxyContin formulation could be sold. The company had effectively won several additional years of patent protection for its golden goose.
Opioid withdrawal, which causes aches, vomiting, and restless anxiety, is a gruesome process to experience as an adult. It’s considerably worse for the twenty thousand or so American babies who emerge each year from opioid-soaked wombs. These infants, suddenly cut off from their supply, cry uncontrollably. Their skin is mottled. They cannot fall asleep. Their bodies are shaken by tremors and, in the worst cases, seizures. Bottles of milk leave them distraught, because they cannot maneuver their lips with enough precision to create suction. Treatment comes in the form of drops of morphine pushed from a syringe into the babies’ mouths. Weaning sometimes takes a week but can last as long as twelve. It’s a heartrending, expensive process, typically carried out in the neonatal ICU, where newborns have limited access to their mothers.
But the children of OxyContin, its heirs and legatees, are many and various. The second- and third-generation descendants of Raymond and Mortimer Sackler spend their money in the ways we have come to expect from the not-so-idle rich. Notably, several have made children a focus of their business and philanthropic endeavors. One Sackler heir helped start an iPhone app called RedRover, which generates ideas for child-friendly activities for urban parents; another runs a child- development center near Central Park; another is a donor to charter-school causes, as well as an investor in an education start-up called AltSchool. Yet another is the founder of Beespace, an “incubator for emerging nonprofits,” which provides resources and mentoring for initiatives like the Malala Fund, which invests in education programs for women in the developing world, and Yoga Foster, whose objective is to bring “accessible, sustainable yoga programs into schools across the country.” Other Sackler heirs get to do the fun stuff: One helps finance small, interesting films like The Witch; a second married a famous cricket player; a third is a sound artist; a fourth started a production company with Boyd Holbrook, star of the Netflix series Narcos; a fifth founded a small chain of gastropubs in New York called the Smith.
Pardes’s ostrichlike avoidance is not unusual. In 2008, Raymond and his wife donated an undisclosed amount to Yale to start the Raymond and Beverly Sackler Institute for Biological, Physical and Engineering Sciences. Lynne Regan, its current director, told me that neither students nor faculty have ever brought up the OxyContin connection. “Most people don’t know about that,” she said. “I think people are mainly oblivious.” A spokesperson for the university added, “Yale does not vet donors for controversies that may or may not arise.”
The controversy surrounding OxyContin shows little sign of receding. In 2016, the CDC issued a startling warning: There was no good evidence that opioids were an effective treatment for chronic pain beyond six weeks. There was, on the other hand, an abundance of evidence that long-term treatment with opioids had harmful effects. (A recent paper by Princeton economist Alan Krueger suggests that chronic opioid use may account for more than 20 percent of the decline in American labor-force participation from 1999 to 2015.) Millions of opioid prescriptions for chronic pain had been written in the preceding two decades, and the CDC was calling into question whether many of them should have been written at all. At least twenty-five government entities, ranging from states to small cities, have recently filed lawsuits against Purdue to recover damages associated with the opioid epidemic.
The Sacklers, though, will likely emerge untouched: Because of a sweeping non-prosecution agreement negotiated during the 2007 settlement, most new criminal litigation against Purdue can only address activity that occurred after that date. Neither Richard nor any other family members have occupied an executive position at the company since 2003.
The American market for OxyContin is dwindling. According to Purdue, prescriptions fell 33 percent between 2012 and 2016. But while the company’s primary product may be in eclipse in the United States, international markets for pain medications are expanding. According to an investigation last year in the Los Angeles Times, Mundipharma, the Sackler-owned company charged with developing new markets, is employing a suite of familiar tactics in countries like Mexico, Brazil, and China to stoke concern for as-yet-unheralded “silent epidemics” of untreated pain. In Colombia, according to the L.A. Times, the company went so far as to circulate a press release suggesting that 47 percent of the population suffered from chronic pain.

Napp is the family’s drug company in the UK. Mundipharma is their company charged with developing new markets.
In May, a dozen lawmakers in Congress, inspired by the L.A. Timesinvestigation, sent a bipartisan letter to the World Health Organization warning that Sackler-owned companies were preparing to flood foreign countries with legal narcotics. “Purdue began the opioid crisis that has devastated American communities,” the letter reads. “Today, Mundipharma is using many of the same deceptive and reckless practices to sell OxyContin abroad.” Significantly, the letter calls out the Sackler family by name, leaving no room for the public to wonder about the identities of the people who stood behind Mundipharma.
The final assessment of the Sacklers’ global impact will take years to work out. In some places, though, they have already left their mark. In July, Raymond, the last remaining of the original Sackler brothers, died at ninety-seven. Over the years, he had won a British knighthood, been made an Officer of France’s Légion d’Honneur, and received one of the highest possible honors from the royal house of the Netherlands. One of his final accolades came in June 2013, when Anthony Monaco, the president of Tufts University, traveled to Purdue Pharma’s headquarters in Stamford to bestow an honorary doctorate. The Sacklers had made a number of transformational donations to the university over the years—endowing, among other things, the Sackler School of Graduate Biomedical Sciences. At Tufts, as at most schools, honorary degrees are traditionally awarded on campus during commencement, but in consideration of Raymond’s advanced age, Monaco trekked to Purdue for a special ceremony. The audience that day was limited to family members, select university officials, and a scrum of employees. Addressing the crowd of intimates, Monaco praised his benefactor. “It would be impossible to calculate how many lives you have saved, how many scientific fields you have redefined, and how many new physicians, scientists, mathematicians, and engineers are doing important work as a result of your entrepreneurial spirit.” He concluded, “You are a world changer.”
Source: https://www.esquire.com/news-politics/a12775932/sackler-family-oxycontin/ October 2017
Illegal marijuana farms are taking over thousands of acres of land as toxic waste continues to corrupt ecosystems in areas along the West Coast.
According to a new report accessed by Reuters, the state of California, which is responsible for more than ’90 percent of illegal U.S. marijuana farming,’ has shown a drastic increase in the use of nationally restricted fertilizers and pesticides such as carbofuran and zinc phosphide, ecologists say.
‘Increasingly, dangerous, unregistered pesticides are being encountered by law enforcement officers who investigate illegal marijuana grows,’ Special Agent-in-Charge of the Environmental Protection Agency criminal enforcement program, Jay M. Green, announced in a public release.



‘Through their indiscriminate application, these unregistered pesticides pollute our lands and waters, create a significant safety risk to humans and animals, and present a mounting cleanup expense for taxpayers.’
Expert ecologist Mourad Gabriel, who reports over the issue for the U.S. Forest Service, said California is utilizing ’41 times more solid fertilizers and 80 times more liquid pesticides’ than the state’s initial reported cited in 2013.
Chemicals of these kind have been linked to health defects and death in both animals and humans.
The agency cited ‘a single swallow can be fatal to a small child, and carbofuran to be ‘highly toxic to vertebrates and birds. In granular form, a single grain will kill a bird; for humans, one quarter of a teaspoon is a sufficient dose to be fatal.’

The Environmental Protection Agency announced in 2011 the department would ban the inorganic chemical compound zinc phosphide.
Included in the unpublished data accessed by Reuters, Gabriel said federal land in California currently holds ‘731,000 pounds of solid fertilizer, 491,000 ounces of concentrated liquid fertilizer and 200,000 ounces of toxic pesticides.’
Illegal pot growers could face jail time and numerous charges for growing illegally, while taxpayers could expect to be left with hefty bills to aid in the sterilization of the toxic waste sites.


Since marijuana was legalized in the state of California, officials have been pushing to properly license growers and carefully supervise the production, testing and distribution of hemp.
Supervisor of Trinity County Keith Groves said there are roughly 4,000 illegal growers in the region currently.
‘I’ll be happy if we can get 500 of them to become licensed,’ he told Reuters.
The expense and danger of cleanup has created a backlog of 639 illegal marijuana farms awaiting restoration in California, according to U.S. Forest Service data compiled for Reuters. Each farm covers up to 50 acres.
‘We’re getting contamination over and over again at those locations,’ said Gabriel, as toxins move from unsafe containers into the soil and water.
At sites that state officials said they had cleaned up completely, his team found 30-50 percent of the chemicals were still there.
‘They are like superfund sites,’ said Assistant U.S. Attorney Karen Escobar,
Source: https://www.dailymail.co.uk/news/article-4768664/Marijuana-farms-forming-toxic-waste-dumps-California.html August 2017
Dear David,
I am sending you below a copy of a letter I have sent to the Premiers of Canada – and other members of the worldwide drug prevention community, plus an email to UN HQ in New York. Since they get so many letters I thought it would be sensible to send you a copy direct as it might take time for you to receive it through UN internal mail.
Dear Premiers,
As members of the worldwide drug prevention community we have been reading with increasing concern and disbelief the way that Canada seems to be bulldozing through legislation that can only damage the citizens of your country – not the least the children.
The Rights of the Child Treaty, under article 33 of the international drug conventions, would be breached if this legislation is allowed to be ratified.
Under the terms of the convention, governments are required to meet children’s basic needs and help them reach their full potential. Since it was adopted by the United Nations in November 1989, 194 countries have signed up to the UNCRC,
United Nations Convention on the Rights of the Child (CRC) is an important international legal instrument that obligates States Parties to protect children and youth from involvement with illicit drugs and the drug trade.
Canada is a signatory to the CRC – which is a legally binding document. Should your country go ahead with the decision to legalise marijuana – against all the evidence from respected scientists and Health authorities worldwide Canada would be an outcast by those 193 nations who have agreed and signed to Article 33.
We find it astonishing that the wealth of evidence and opinion in Canada and worldwide, on the harmfulness of marijuana would seem to have been totally ignored by your parliamentarians. Indeed new evidence relating to the epidemic of gastrochisis was submitted in good time by our Australian colleague Dr. Stuart Reece and was not allowed to be presented. Instead you have been persuaded by groups that want marijuana to be ‘the new tobacco’ – headed of course by George Soros, that this will not be harmful to your citizens, that it will bring in tax revenues and that it would destroy the black market.
However, there was a study done a few weeks ago by the Canadian Centre on Substance Abuse and Addiction finding that just in Canada alone, a much smaller country than the U.S. in population, marijuana-related car crashes cost a billion dollars. That’s just the car crashes, and those were directly related to marijuana. And the report came from a government think tank, not any kind of anti-drug group.
We heard many of these same promises in 2012 when Colorado legalized recreational marijuana. Yet in the years since, Colorado has seen an increase in marijuana related traffic deaths, poison control calls, and emergency room visits. The marijuana black market has increased in Colorado, not decreased. And, numerous Colorado marijuana regulators have been indicted for corruption.
New reports out of Colorado indicate that legal marijuana is posing real risks to the safety of young people. As Colorado rethinks marijuana, the rest of the nation should watch carefully this failing experiment.
Healthcare officials representing three hospitals in Pueblo, Colorado, issued a statement on April 27 in support of a ballot measure that would end Marijuana commercialization in the city and county of Pueblo. “We continue to see first-hand the increased patient harm caused by retail marijuana, and we want the Pueblo community to understand that the commercialization of marijuana is a significant public health and safety issue,” said Mike Baxter, president and CEO of Parkview Medical Center.
Among their concerns are a 51 percent increase in number of children under 18 being treated in Parkview Medical Center emergency rooms. Furthermore, of newborn babies at St. Mary-Corwin Hospital, drug tested due to suspected prenatal exposure, nearly half tested positive for marijuana.
Having read the above, how can Canadian legislators possibly believe that legalising marijuana would, in any way, be advantageous for their country ?
Yours faithfully,
Peter Stoker, Director, National Drug Prevention Alliance (UK)
Source: A letter forwarded by Peter Stoker to David Dadge, spokesperson for UN Office ON Drugs and Crime (UNODC), originally sent to the Premiers of Canada September 2017
WASHINGTON – The Drug Enforcement Administration today announced the establishment of six new enforcement teams focused on combatting the flow of heroin and illicit fentanyl.
“At a time when overdose deaths are at catastrophic levels, the DEA’s top priority is addressing the opioid epidemic and pursuing the criminal organizations that distribute their poison to our neighborhoods,” said DEA Acting Administrator Robert W. Patterson. “These teams will enhance DEA’s ability to combat trafficking in heroin, fentanyl, and fentanyl analogues and the violence associated with drug trafficking.”
The enforcement teams will be based in communities facing significant challenges with heroin and fentanyl, including New Bedford, Mass.; Charleston, W.Va.; Cincinnati, Ohio; Cleveland, Ohio; Raleigh, N.C.; and Long Island, N.Y.
In determining the locations for these teams, DEA considered multiple factors, including rates of opioid mortality, level of heroin and fentanyl seizures, and where additional resources would make the greatest impact in addressing the ongoing threat. While the teams are based in specific cities, their investigations will not be geographically limited. DEA will continue to pursue investigations wherever the evidence leads.
DEA received funding in its FY 2017 enacted appropriations to establish these teams, which will be comprised of DEA special agents and state and local task force officers.
The abuse of controlled prescription drugs is inextricably linked with the threat the United States faces from the trafficking of heroin, fentanyl and fentanyl analogues.
Drug overdoses are now the leading cause of injury-related death in the United States, eclipsing deaths from motor vehicle crashes or firearms. According to initial estimates provided by the Centers for Disease Control and Prevention, there were more than 64,000 overdose deaths in 2016, or approximately 175 per day. More than 34,500, or 54 percent, of these deaths were caused by opioids.
The DEA continues to aggressively pursue enforcement actions against international and domestic drug trafficking organizations manufacturing and distributing heroin, fentanyl and fentanyl analogues. Just last week, the Department of Justice announced indictments against two Chinese nationals and their North America-based traffickers and distributors for separate conspiracies to distribute large quantities of fentanyl and fentanyl analogues and other opiate substances in the United States.
Source: Email from U.S. Drug Enforcement Administration <dea@public.govdelivery.com> October 2017
These are very shocking videos with information about some of the effects of drug legalisation in the USA.
While writing, I wondered what kind of details I should publish about the previous lives of people in the marijuana industry. Virgil Grant, one of the article’s subjects, told me stories about how he would sell marijuana from his family grocery store in Compton in the 1980s and 1990s by putting the weed in empty boxes of Lucky Charms. He mentioned, without much elaboration, that would-be competitors in Compton regretted going up against him.
It’s an awkward and confusing transition period in the marijuana industry. What was illegal yesterday in California may be legal today, but that’s of course not the way the federal government sees it. Mr. Grant has spent time in both federal and state prisons.
Since legalization of recreational sales came into effect in California in January, there have been stories about cities and counties that banned marijuana. But I had never seen reporting on the bigger picture. So I reached out to a company called Weedmaps, a website that hosts online reviews of cannabis businesses. When they added it up, the data surprised me: Only 14 percent of California’s cities and towns authorize the sale of recreational marijuana. By contrast, Proposition 64, the ballot measure that allowed marijuana legalization, passed with 57 percent voter approval in 2016, a seemingly solid majority.
The low acceptance of marijuana businesses strikes me as part of the liberal, not-in-my-backyard paradox in California. Yes, Californians want shelters for the homeless, but just not across the street. Yes, Californians want more housing built, but not if it changes the character of the neighborhood. A marijuana dispensary? Sure, preferably in the next town.
A New York Times reporter wanted to find out why California cities are taking such different approaches to legal pot. Previously, he covered a story about why California growers are so reluctant to leave the black market and seek a state license to become legitimate. He found that only about 10 percent have done so. The other 90 percent remain in black market. California is the nation’s biggest producer and consumer of marijuana. One estimate projects the state produces seven times the amount of pot it consumes and exports the surplus to non-legal states. Pursuing this story took the reporter to Compton, in Los Angeles County, where residents voted in January to ban marijuana businesses by a 3-to-1 margin. He compared this to Oakland, near San Francisco, which has embraced the marijuana industry. It’s as if the two cities had been asked the same question and come up with completely different answers, he opined. To get a bigger picture, he consulted Weedmaps to find out how common industry bans are. He was surprised to find that only 14 percent of California’s cities and towns authorize marijuana sales, even though legalization passed in 2016 with 57 percent voter approval.
It’s still early days — it’s been less than three months since legal sales started — but for now the trend is that larger cities like Oakland, San Francisco, Los Angeles, Sacramento and San Diego are the hubs of the marijuana industry, while smaller cities and towns are ambivalent or outright hostile to the idea of opening marijuana dispensaries. Orange County, in Southern California, is a recreational marijuana desert, with only a handful of dispensaries allowed.
California has a reputation for very tolerant attitudes toward pot, and it’s the biggest consumer and producer of the drug in the United States by a wide margin. It is also the nation’s premier exporter to other states: By one estimate, the state produces seven times more than it consumes.
But the visit to Compton helped peel back another, more conservative set of attitudes toward marijuana.
At the Compton airport, Shawn Wildgoose, a former enlisted Marine who lives in Compton and works in the construction industry, told me he wanted to see the city focusing on its homeless problem and reducing crime, which is sharply down from previous decades.
Legal marijuana?
“Compton has other issues,” Mr. Wildgoose said. “We don’t need that distraction.”
Source: National Families in Action’s The Marijuana Report nfia@nationalfamilies.org 21st March 2018
For decades, attorney Richard Blau focused his legal savvy on the high-stakes business of booze. Alcohol-industry law was an attorney’s dream, full of unresolved questions and deep-pocketed players clawing their way to the top.
So when Florida’s talk turned to marijuana, another storied pastime with its own dubious history, Blau’s titan of a law firm, GrayRobinson, jumped at the opportunity. Blau now leads a special practice for clients wanting to capitalize on medical cannabis — and bend the laws to their advantage.
“The playbook is to get in and lend a hand in crafting those rules, so they read the way our clients want them to read,” Blau said. “The powerful people are the ones to get in on the ground floor.”
Months before the state’s November vote to legalize medical marijuana, some of Florida’s biggest law firms are already staking their claims to the lucrative legal minefield of the budding weed industry.
Orlando-based GrayRobinson, which employs 101 attorneys in Tampa Bay and nearly 300 across the state, will devote a core of its “regulated products” group to the nuances of marijuana law.
Attorneys with Holland & Knight, a prominent firm in Tampa with more than 1,000 lawyers across the world, last week released an alert for clients on the “legal landscape (and) complex marketplace for marijuana-related businesses.”
And Akerman, the Miami-based corporate-law giant and largest law firm in the state, recently launched a “regulated substances task force” with nearly two dozen senior attorneys and public-policy professionals ready to advise, among others, cultivators, private-equity groups and dispensaries.
“The shifting interplay between state and federal laws presents new challenges and unprecedented opportunities for Akerman clients,” managing partner Richard Spees said in a statement, “and we are positioned to help them capitalize.”
Groups with ostensible legal ties have filed for Florida business licenses with names like Medical Marijuana Business Lawyers and the Cannabis Law Group, joining a wave of “ganjapreneurs” grabbing for a piece of industry profits.
But the introduction of these powerhouse firms ups the ante, helping squash the images of two-bit, Breaking Bad-style “Better Call Saul” legal operations and legitimizing what could be a landslide of million-dollar corporate disputes.
“We’re not the ‘pot lawyers.’ This is not ‘reefer madness.’ It’s 100 percent professional, 100 percent legitimate . . . and we take it 100 percent seriously,” said Troy Kishbaugh, a health care specialist serving on GrayRobinson’s regulated-products group. “We have a large health care base . . . and they want their patients to get the best care possible. And if medical marijuana happens to be part of that medical regimen, they want to make sure they’re doing it right.”
The state’s biggest firms bolstered their practices this spring after Florida lawmakers passed a “Charlotte’s Web” bill legalizing a non-high-producing cannabis strain used to treat cancer and epilepsy.
An even bigger fight comes in November, when voters could pass Amendment 2 and legalize weed for a much broader slate of medical uses. Its prospects seem increasingly upbeat: A Quinnipiac University poll last week found 88 percent of Florida voters support adult medical-cannabis use.
If the vote passes, Florida could follow California in becoming America’s second-biggest medical-weed state, with around 400,000 patients spending an average of $3,000 a year, estimates from state regulators and a national cannabis-industry trade group show.
State regulators have several months to decide on the law’s little details, leaving a huge window for “cannabusiness” interests pushing to find an unserved niche. The state Department of Health’s Office of Compassionate Use, which is drafting the rules, discussed at a public hearing Friday a range of potential enterprises, from medical-cannabis testing to home delivery.
Lawyers wise to food and alcohol regulation are shoo-ins for the firms’ legal-weed practices: Many of the rules facing Big Pot, attorneys argue, could look a lot like those governing Big Tobacco, Big Food and Big Booze.
Joining them are lawyers with a vast range of expertise:
• Health care experts to address hospital and physician groups on how to protect themselves while administering, storing and suggesting the use of a drug still illegal under federal law.
• Banking and financial gurus to advise on securing investment, handling money and saving on taxes in what has long been an all-cash business.
• Land use attorneys who can help resolve zoning and landlord disputes over where growers and distributors can operate from seed to sale.
• Even intellectual-property specialists with knowledge on how to protect and preserve cannabis companies’ strains, brands and reputations, in much the same way consultants have long advised Budweiser or Marlboro.
For precedent, attorneys here are analyzing the legal laboratories of the 23 states, plus Washington D.C., that have legalized medical cannabis, and the two states, Washington and Colorado, that have okayed weed for personal use.
They also are following in the footsteps of nationwide firms versed in guiding the emerging trade. Seattle’s Canna Law Group, launched by international law firm Harris Moure in 2011, proved “profitable almost instantly,” partner Dan Harris told the Puget Sound Business Journal last year, adding, “We were shocked at the demand.” One of the group’s attorneys, a young University of Miami graduate, was voted “Marijuana Industry Attorney of the Year” in 2013 by Dope Magazine.
For the finer details, attorneys said, firms are following their clients’ requests to lobby their way into influence. Litigation seems likely: A proposed rule limiting Florida’s medical weed to five nurseries, chosen by lottery, has already stirred up legal wrath.
Attorneys have likened their legal timing to representing alcohol outfits near the sunset of prohibition, a potentially historical chance to mold law and make nice with the grateful captains of a new industry.
But GrayRobinson’s Blau, whose practice group is taking on three new clients a week, stops short of supporting the “green rush” of small-time entrepreneurs. He compares the early days of legal Florida weed to that of the American gold rush, in which organized business interests, not excited ground troops, ended up with the most to gain.
“All those individual wannabe miners thought (they’d strike it rich) when they pushed forward to mine the Klondike … but very few emerged out of that with anything,” Blau said. “In reality, it was the established gold-mining companies who took the ground, and made it their own.”
Source: www.tampabay.com 1st August 2014
Public Health and Safety Communities Applaud Move
DOJ Decision Will Dry Up Money To Marijuana Industry
(January 4, 2018 – Alexandria, VA) – The Department of Justice will announce today it will rescind lax marijuana policy guidance to US Attorneys (the so-called “Cole Memo”) and instead allow US Attorneys to exercise discretion in going after marijuana cases. The new memo will not call for arresting users or others with low-level involvement in marijuana, but instead makes investing in the marijuana industry a risky move.
“This is a good day for public health. The days of safe harbor for multi-million dollar pot investments are over,” said Kevin A. Sabet, a former Obama Administration drug policy adviser who is now head of the anti-legalization group Smart Approaches to Marijuana (SAM). “DOJ’s move will slow down the rise of Big Marijuana and stop the massive infusion of money going to fund pot candies, cookies, ice creams, and other kid-friendly pot edibles. Investor, banker, funder beware.”
The Cole Memo and its compliance was blasted by the nonpartisan Government Accountability Office (GAO) in a 2016 report. The lead GAO author stated that DOJ “has not documented its plan for monitoring the effects of the state marijuana legalization.” A recent poll also found that when voters had more choices than just legalization or prohibition, support for legalization fell by 30%. Most voters were comfortable with laws removing criminal penalties for use but not legalizing sales, which the Cole Memo permitted.
“The Cole Memo had been waived around by money-hungry pot executives for years, searching for legitimacy among investors and banks,” remarked former Congressman Patrick J. Kennedy, a SAM Honorary Advisor. “It’s time we put public health over profits. This is a sensible move that now must be followed up with action so we can avoid a repeat of the nightmare of Big Tobacco.”
“Marijuana, along with alcohol and tobacco, are the three drugs we need to stop our youth from trying,” said Dr. Robert DuPont, the first Director of the National Institute on Drug Abuse and second White House drug czar. “DOJ is doing the right thing by putting a stop to this wink and nod policy of allowing marijuana legalization.”
Corinne Gasper, who lost her daughter Jennifer to a driver high on marijuana, stated, “All too often, marijuana has been seen as benign. An industry not unlike Big Tobacco has downplayed its harms, aided by laws allowing officials to look the other way. For the sake of so many families, I hope those days are now over.”
SAM, a non-profit organization founded by a former member of Congress and a former Obama Administration drug policy advisor, applauded the news. SAM’s Science Advisory board consists of more than a dozen top researchers in the field of marijuana policy ranging from institutions such as Harvard and Johns Hopkins.
Dr. Stuart Gitlow, the former President of the American Society of Addiction Medicine, stated, “This is the right move by DOJ. To protect public health, we must choke the large amounts of funding spent by Big Marijuana to hook kids on highly potent THC products.”
Justin Luke Riley, the Denver-based leader of the Marijuana Accountability Coalition stated, “Recovery from addiction is so much harder when you are bombarded with the kind of pot commercialization we see here in Colorado. DOJ should be applauded for trying to put a stop to the shameless promotion and advertising that is killing our community.”
Ron Brooks, the former head of the National Narcotics Officers Association Coalition, stated, “This is the kind of leadership that will save lives. For too long law enforcement has been handcuffed by vague and unenforced policy guidance.”
Will Jones, a DC-resident who is fighting for social justice in minority communities commented, “Since the Cole Memo was released, the pot industry has relentlessly opened more pot shops in poorer, communities of color. Arrests are even higher now in many jurisdictions than before legalization.”
“Focusing enforcement resources on incarcerating low-level, nonviolent offenders will always be wrong and counterproductive,” said Kevin Sabet, President of SAM. “But there is an urgent need for Federal officials to reassert targeted control over an exploding industry that is undermining public health and safety in our communities.
This is a major blow to an industry that is corrupting our politics and lying to voters in a steadfast pursuit to put profit over public health and safety. Today’s policy change will undoubtedly extend a chilling effect we have seen on marijuana legalization initiatives across the nation this year, and – hopefully – encourage lawmakers to stop and look at what science tells us about the unintended consequences of legal marijuana.
Like the tobacco industry before it, well-heeled lobbyists from the marijuana industry have been touting marijuana commercialization as the panacea for every contemporary challenge we face in America, but the truth is, the health and safety costs caused by the commercialization of cannabis are outweighing any tax revenues collected.”
Source: Press Release from SAM: info@learnaboutsam.org. 4th January 2018
Kevin Sabet, the president and CEO of Virginia-based Smart Approaches to Marijuana, has become arguably the most influential critic of marijuana legalization in the United States. But in an extended interview on view below, he fights against the perception that he’s a one-dimensional prohibitionist along the lines of U.S. Attorney General Jeff Sessions.
Sabet stresses that he and his organization, shorthanded as SAM, take what he sees as a sensible approach to cannabis by arguing in favor of treatment rather than jail time for users in trouble and advocating for greater study of the substance to determine the best ways to utilize it medically.
We first spoke to Sabet in January 2013, just prior to SAM’s launch in Denver, when he appeared alongside co-founder Patrick Kennedy, a former congressman from Rhode Island and a member of the Kennedy political dynasty. Sabet’s background is similarly stocked with connections to heavyweights. The author of Reefer Sanity: Seven Great Myths About Marijuana, he served stints in the Clinton and Bush administrations and spent two years as senior adviser to President Barack Obama’s drug-control director before taking on the SAM cause.
In the more than four years since then, he’s made countless media appearances while lobbying behind the scenes to try and stop the momentum generated by the pot legalization bandwagon.
Sabet, who says SAM’s funding mainly comes from small donors and grants as opposed to hard-core drug-war groups or Big Pharma, doesn’t think it’s too late to accomplish this goal, in part because only a relatively small percentage of the populace actually uses marijuana. Moreover, he feels that plenty of those who abstain will more actively fight against pot’s normalization if public use (and its attendant smoke and scent) becomes more prevalent in cities such as Denver, which he sees as having been demonstrably harmed by legalization. He blames cannabis for turning the 16th Street Mall into a homeless haven that visitors actively avoid and suspects that in his heart of hearts, Governor John Hicklenlooper knows legalization was a terrible mistake but can’t admit it publicly because the right to toke is enshrined in the state constitution.
Likewise, Sabet considers it inarguable that the marijuana industry is targeting young people with colorfully packaged pot edibles and argues that simply keeping cannabis away from kids isn’t enough. He cites studies showing that the brains of 25-30 year olds are still developing — and can still be harmed by weed.
Continue to learn more about Sabet’s cause and the arguments he makes to support it.
Westword: SAM recently put out a release about the amount of tax revenue Colorado has collected as a result of the marijuana industry [in reference to a VS Strategies report estimating that the state has generated more than $500 million in cannabis revenue since legalization]. In it, you talk about how drug use and its consequences cost taxpayers $193 billion per year, with Colorado’s annual share being approximately $3.3 billion. But that’s for all drugs, correct?
Kevin Sabet: Oh, yeah, absolutely. But you need to look at the fact that marijuana is used far more than any of the other drugs, and look at the costs associated with driving, crashing, mental illness — and long-term costs we’re not able to account for. Marijuana isn’t correlated with mental illness overnight. If often takes time. And so the cost of that can’t be calculated in any way. There was a study done a few weeks ago by the Canadian Centre on Substance Abuse and Addiction finding that just in
Canada alone, a much smaller country than the U.S. in population, marijuana-related car crashes cost a billion dollars. That’s just the car crashes, and those were directly related to marijuana. And the report came from a government think tank, not any kind of anti-drug group.
I honestly think it isn’t surprising coming from this group [VS Strategies]. It’s an industry group that wants to basically make money from marijuana — much more money than the State of Colorado will make after you account for costs. When you look at the actual number and context of just education alone, the marijuana revenue is barely newsworthy. The Department of Education in Colorado says they need $18 billion in capital construction funds alone. The reality is, the Colorado budget deficit is actually rising, not falling. This isn’t plugging a hole in the deficit. It’s actually costing money. There’s one area where I’d agree with [former Colorado Director of Marijuana Coordination] Andrew Freedman: You don’t do this for the money. But it’s a great talking point, and it polls well, just like the talking point of it being safer than alcohol polls well. This polls well, too, so you’re going to have an industry group that thrives off commercialization touting the numbers. That’s not surprising at all.
SAM is usually described as an anti-marijuana organization. Is that an accurate description from your viewpoint? Or is it pejorative in some way?
I wouldn’t necessarily say it’s pejorative, but I think it’s overly simplistic. It’s true that we don’t want to see the legalization of another illegal substance. We think that our experience with pharmaceuticals, which are, of course, legal, as well as alcohol and tobacco, has been an utter disaster from a public cost and public-policy point of view. We’ve never regulated those drugs in a responsible way. Lobbyists and special interests own the rule-making when it comes to these drugs. And what we’re saying is, do we really want to repeat history once again? It just happens to be marijuana. It really could have been any substance. And we will be talking about the legalization of other drugs if marijuana goes through. Because it doesn’t stop with marijuana in terms of the policy goals of many of these organizations. So I think it is overly simplistic. And we’re very concerned about commercialization.
Also, we don’t want to see a return to an enforcement-heavy policy that throws everybody behind bars or saddles young people, especially, with criminal records that prevent them from getting a job or being able to access public benefits or being able to go to school. We want to see people given another chance. But we also want to see this treated as a health issue, and you don’t treat marijuana as a health issue by ignoring it or facilitating its use. You do brief interventions if they’re needed, treatment if it’s needed. I don’t think everyone who uses marijuana needs treatment, just like everyone who drinks or uses other drugs doesn’t need treatment. But some people are using it in a way that is problematic, and they need an early intervention, perhaps, to prevent them from moving on to a substance-use disorder — or they need more intense treatment. It really just depends.
We also want to see research into components of marijuana that may have therapeutic value. We don’t want to see people needlessly suffering. But if Perdue Pharma or Pfizer said tomorrow that they have a new blockbuster drug but they don’t want it to go through the FDA and instead want to put it up to a vote, we’d be up in arms. And rightfully so. Everybody would be up in arms. And we don’t think marijuana should get a free pass because there are stories of it helping people. I don’t doubt that it helps some people — things like cannabidiol oil, etc., or even smoking marijuana to relieve pain. I don’t doubt that it helps some people. But we don’t want to turn back the clock to pre-FDA days, where we had snake-oil salesmen and wild claims about drugs. We want to put it through the same system, and if that system is problematic and difficult, then let’s look at what those barriers are and resolve them.
So I think we are a sensible organization that takes our cues from science. That’s why, on our board, you don’t see people benefiting from the policy position that we take. If anything, people like the doctors from Boston Children’s Hospital who are on our advisory board, or Harvard professors, they’re going to have more business if marijuana is legal, because they’re going to have people with more problems. We’re working counter to their self-benefit, if you think about it. That’s why we’re led by the science. And the reason we started this…. I left the White House and saw there was a huge disconnect between the public’s understanding of marijuana and what was being told to them by various sources, and we’re trying to bridge that gap. Many of the things you just touched upon are on the four items in the “What We Do” section of your website. But some things, such as “To promote research on marijuana in order to obtain FDA-approved, pharmacy-based cannabis medications,” we don’t hear your organization talking about very often. Is that the fault of the media, because they’re only focusing on the legalization-is-bad angle? Are you giving equal weight to some of these other goals?
I think that’s just people looking through the glasses they want to look through. I think the legalization groups are threatened by a sensible organization led by Harvard doctors that doesn’t want to put people in prison, so they want to paint us as the most irrational dinosaurs from the Stone Age on these issues. The reality is, we spend a lot of our time on all of these issues. In fact, we have released the most comprehensive document that any policy organization has released, I think, on the hurdles of medical marijuana research. That’s right on our website — the six-point plan. And we’ve also done a CBD guide — everything you need to know about CBD. After the guide to everything you need to know about CBD, we did a report on research barriers, and we got a lot of people from both extremes that didn’t like it. John Walters, my former boss, wrote a scathing editorial, saying we were off the mark in calling for more research. When we get criticized from multiple angles, I think people can decide for themselves whether that’s credible or not….
It’s just not sexy, though. I can’t remember the last time that someone from USA Today or Huffington Post said, “Oh, we want to cover the fact that you released a wonky policy document aimed at FDA senior scientists with ten letters after their name.” They’re not banging on the door to get that story. Instead, they’re banging on the door to say, “The governor of Nevada has just declared a state of emergency on pot. What do you think?”
I’m not going to say it’s the fault of the media. I think that’s overused these days. But we’re doing our best, and whether it’s noticed by USA Today or the Huffington Post or the Washington Post or not, that doesn’t matter as much. We’re getting it out there, and I know that hundreds of lawmakers have read it. In fact, three out of our six recommendations have been adopted since we released that report. I don’t think we’re the only reason they’ve been adopted, but I think us pushing and prodding and putting it down on paper gave some political cover to some people who may not have supported it in the past, and I’m very proud of that. I know it doesn’t satisfy Medical Marijuana Inc. or these hundreds of CBD manufacturers who are selling God knows what because they don’t get it looked at by the FDA; they’re not going to be happy about that. But I think the science speaks for itself, and scientists and others have noticed. That’s why they’ve asked to join my advisory board — top researchers who want to be part of this team not because we’re zealots, but because we look at the science and are able to get it out there….
Another of the talking points on your website says, “Alcohol is legal. Why shouldn’t marijuana be legal?” How do you answer that question?
To me, saying, “Alcohol is bad and it’s legal, so why shouldn’t marijuana be legal?” is like saying, “My headlights are broken, so why don’t we break the taillights, too?” It doesn’t make much sense. First of all, alcohol and marijuana are apples and oranges in many ways. They’re different just because of their biology and their pharmacology, but they’re also different in their cultural acceptance and prevalence in Western society. Alcohol has been a fixed part in Western civilization since before the Old Testament. The reason alcohol prohibition didn’t work — and that’s debatable….
What’s the debate?
If you look at scholars who studied Prohibition much more than I have, there is a vigorous debate. Alcohol use fell during Prohibition, harm fell as well. Cirrhosis of the liver, which is a top-ten killer of white men, wasn’t a top-ten killer. Organized crime had been in place, and obviously it was strengthened from Prohibition, although it isn’t like it caused it, and it certainly didn’t go away when Prohibition ended…. But it’s very difficult to prohibit something that 60 to 70 percent of the population are doing on a regular basis. Marijuana is still used by fewer than 10 percent of the population monthly, and so the idea that it’s the same in terms of acceptance is wrong. Right now, those 10 percent of users have convinced 55 percent of Americans that this is a good idea. HOW
That also points to the fact that I think support for marijuana is very soft. I think the industry has overplayed its hand about things like public nuisance, public use, secondhand smoke, car crashes. Once these things become greater in prevalence, which they inevitably will if more states legalize and commercialize, then I think you’re going to have the backlash I think will come, and it will come because of the increased problems….
Alcohol is such an accepted part of society. We accept the negative consequences. Alcohol is not legal because it’s safe. Alcohol isn’t legal because it’s so good for you. Alcohol is legal because it’s been a fixed part of Western civilization for millennia. Marijuana has not been. Of course it was used thousands of years ago. Was it used by certain cultures? Absolutely. But there’s no comparison, complete apples and oranges, when it comes to alcohol’s culture acceptability. So that’s why alcohol is legal — not because we love the effects it has on society. No parent, no teacher, no police officer, says, “I’d be better if I was drinking all the time.” No police officer says, “Man, I wish more people drank.” No parent says, “I wish my kid drank more.” That’s not why it’s legal, because it’s so great.
And alcohol has done very little for our tax base. One of the reasons Prohibition was repealed was because the industrialists were convinced that it would help eliminate or mitigate the corporate tax or even the personal income tax. That’s laughable today. It doesn’t do that at all. Instead it costs us way more money than any revenue we bring in. I think marijuana would be the same story. It affects our bodies differently.
Alcohol affects the liver, marijuana affects the lungs. Alcohol is in and out of your system quite rapidly, but marijuana lingers in the system longer, and according to studies, the effects also linger for longer. They affect different parts of the brain. So they’re different in many ways, but in some respects, they’re the same. They’re both intoxicants, and unlike tobacco, they specifically cause changes in behavior. And that’s a difference with tobacco, another legal drug. Tobacco isn’t correlated with paranoia or obsessiveness or mental illness and car crashes, and obviously, marijuana is.
In some ways, legal drugs offer an interesting example. I think they offer an example of the sort of social and financial consequences that would come with legalizing other drugs.
Source: http://www.westword.com 14th August 2017
Introduction
On 31 July 2017 a court case commences in the Pretoria High Court about the constitutional legality of South Africa’s dagga legislation. The media is calling it the “Trial of the Plant”.
What is the “Trial of the Plant” about?
It is about the dagga plant and its prohibition in our society. Scientists have long since proven that the dagga plant is highly complex and dangerous and must be prohibited, but some believe it is not dangerous and even medicinal.
What does the law in SA say about dagga?
Except for medical and research exemptions, the possession, use, cultivation, transportation and distribution of dagga is criminalised in terms of the Drugs and drug trafficking act as well as the Medicines and related substances act.
Was the law not settled by the Constitutional court in 2002?
In 2002 a Rastafarian brought a case to the Constitutional Court about Dagga where he complained that the law prevented him smoking dagga as a religious observance and this violated his rights to religious freedom.
The court accepted that a Rastafarian’s religious rights were violated but dismissed the case as there is no objective way for law enforcement officials to distinguish between the possession or use of cannabis for religious or for recreational purposes.
The trial of the plant will in all likelihood be the final decider.
Why is that?
Because the Trial of the Plant will be the first and only case where there will be oral evidence given and tested, in the witness stand.
These other cases were fought and decided on affidavit evidence in a day or two.
The trial of the plant is very different and will take many days in court starting on 31 July and continuing through the month of August.
There are three legal teams comprising 6 attorneys, 11 advocates, 16 expert witnesses and as many as 12 other witnesses. The trial will probably be recorded by the media and will also probably go all the way to the Constitutional Court to be finally decided.
DFL’s lead counsel is Adv Reg Willis instructed by the University of Pretoria Law Clinic.
How did this case start?
In 2010 a couple were arrested with approximately R500 000.00 worth of dagga in their home. They became known as the dagga couple.
To avoid prosecution they obtained an interdict in the Pretoria High Court against their prosecution, pending the outcome of a case to declare that all the SA dagga legislation is unconstitutional.
The case is against various government departments and against Doctors for Life International.
DFL joined this case to be of assistance to the State.
So for example DFL will lead the evidence of Harvard Professor Bertha Madras who is one of the foremost authorities on cannabis in the world. She contends that the legalisation of cannabis has to be resisted in the interests of the human brain.
Who is Doctors for Life and what does it do?
DFL is a non-profit relief and civil society organisation of doctors who care and give voluntarily of their own time and money to the many needs of the poor.
DFL serve the needs of the underprivileged communities they serve in South Africa and Southern Africa. DFL also has an extensive track record of being involved in public interest cases predominantly as a friend of the court, especially to assist with scientific and similar evidence.
So then how is the dagga couple funding their case?
The dagga couple dragged the case out for some years, while they raised money. They started an organisation called “Fields of Green for All” “FOGFA” which now has over 45000 supporters who are funding the case.
How important is this case for South Africa?
Given the role of dagga in crime, women and child abuse and the future of our youth, this trial is one of the most important to ever reach our courts. If the dagga couple win their case as they want to, there will be no restriction on the possession, consumption, cultivation, transportation and distribution of cannabis. A free for all.
Read our dagga court case press releases and more info on cannabis Media Release: High Court Blunders into Dagga Minefield
Source: Letter from Johan Claassen www.doctorsforlife.co.za) sent to Drugwatch International 27th July 2017
Sirs,
I believe that a state’s Attorney General and Secretary of State have the obligation to reject any petition that is obviously in violation of any law.
Whether a ballot initiative is properly worded or not, if it proposes, facilitates or allows the violation of any law – it is illegal.
EXCERPT: “In an opinion dated Tuesday and released Wednesday, Rutledge said the ballot title of the proposal is ambiguous and “that a number of additions or changes” are needed “to more fully and correctly summarize” the proposal.
“The proposal [to legalize recreational marijuana use in the state] by Larry Morris of West Fork would allow for the cultivation, production, distribution, sale and possession of marijuana for recreational use in Arkansas.”:
As you can readily see, Mr. Morris’ proposal would violate federal law and place persons who engage in any of those activities at risk of federal prosecution or other liability.
I draw to your attention a LEGAL PRIMER(BELOW) ON: ENFORCING THE CONTROLLED SUBSTANCE ACT IN STATES THAT HAVE COMMERCIALIZED MARIJUANA by Mr. David Evans, Esq. in which he concludes that: “Anyone who participates in the growing, possession, manufacturing, distribution, or sales of marijuana under state law or aids or facilitates or finances such actions is at risk of federal prosecution or other liability.”
I ask that you continue to reject these illegal proposals to legalize marijuana in any form in our state of Arkansas.
I reiterate, it is your job to UPHOLD the LAW, not facilitate LAWBREAKING.
Jeanette McDougal
Board Member, Drug Watch, Intl.
Director, NAHAS – National Alliance of Health and Safety dems8692@aol.com
During the 2015 election, the Liberals campaigned on a plan to greenlight marijuana for recreational use to keep it out of the hands of children and the profits out of the hands of criminals.
The party’s election platform said Canada’s current approach — criminalizing people for possession and use — traps too many Canadians in the justice system for minor offences.
Last month, the government spelled out its plans in legislation, setting sweeping policy changes in motion. The new law proposes setting the national minimum age to legally buy cannabis at 18 years old. It will be up to the provinces should they want to restrict it further.
Is it true, as Wilson-Raybould and the Liberals suggest, that legalization will in fact keep cannabis out of the hands of kids?
Spoiler alert: The Canadian Press Baloney Meter is a dispassionate examination of political statements culminating in a ranking of accuracy on a scale of “no baloney” to “full of baloney” (complete methodology below)
This one earns a lot of baloney — the statement is mostly inaccurate but contains elements of truth. Here’s why:
THE FACTS
There is no doubt cannabis is in the hands of young people today.
In fact, Canada has one of the highest rates of teenage and early-age adulthood use of marijuana, says Dr. Mark Ware, the vice-chair of the federally-appointed task force on cannabis and a medicinal marijuana researcher at McGill University.
“We don’t anticipate that this is going to eliminate it; but the public health approach is to make it less easy for young adolescents, young kids, to access cannabis than it is at the moment,” he said.
Bonnie Leadbeater, a psychology professor at the University of Victoria who specializes in adolescent behaviour, said as many as 60 per cent of 18-year-olds have used marijuana at some point in their lives.
The aim of a regulated, controlled system of legalized cannabis is to make it more difficult for kids to access pot, Ware said, noting the principle goal is to delay the onset of use.
So will a recreational market for adults coupled with a regulatory regime really keep pot out of the hands of kids?
THE EXPERTS
Public health experts — including proponents of legalization — say that probably won’t happen.
“I don’t exactly know what they are planning to do to keep it out of the hands of young people and I think some elaboration of that might be helpful,” Leadbeater said. “It is unlikely that it will change … it has been very, very accessible to young people.”
Benedikt Fischer, a University of Toronto psychiatry professor and senior scientist with the Centre for Addiction and Mental Health, agrees the expectation that legalization will suddenly reduce or eliminate use among young people is counter-intuitive and unrealistic to a large extent.
“The only thing we could hope for is that maybe because it is legal, all of a sudden it is so much more boring for young people that they’re not interested in it anymore,” he said.
Increasing penalties for people who facilitate access to kids will help discourage law-abiding Canadians from doing so, says Steven Hoffman, director of a global strategy lab at the University of Ottawa Centre for health law, policy and ethics.
“That being said, when there’s a drug, there’s no foolproof way of keeping it out of the hands of all children,” Hoffman said. “For sure, there will still be children who are still consuming cannabis.”
Cannabis will not be legal for people of all ages under the legislation, he added, noting this means there may still be a market for criminal activity for cannabis in the form of selling it to children.
In Colorado, officials thought there would be an increase in use as a result of legalization, according to Dr. Larry Wolk, chief medical officer at the Department of Public Health and Environment, but he said there’s been no increase among either youth or adults. Nor has there been a noticeable decrease.
“What it looks like is folks who may have been using illicitly before are using legally now and teens or youth that were using illicitly before, it’s still the same rate of illicit use,” he said.
THE VERDICT
Donald MacPherson, executive director of the Canadian Drug Policy Coalition, said the Liberal government could provide a more nuanced, realistic message about its plans to legalize marijuana.
“To suddenly go over to the rhetoric … that strict regulation is going to keep it out of the hands of young people doesn’t work,” he said.
“There’s a better chance of reducing the harm to young people through a … public health, regulatory approach. That’s ideally what they should be saying.”
Careful messaging around legalized marijuana — like the approach taken by the Netherlands — could make cannabis less of a tempting forbidden fruit for young people, said Mark Haden, an adjunct professor at the University of British Columbia.
“What we know is that prohibition maximizes the engagement of youth, so if we did it well and skillfully and ended prohibition with a wise approach and made cannabis boring, it would keep it out of the hands of kids,” he said.
“It isn’t completely baloney, it just hasn’t gone far enough in terms of a rich, real discussion. It is just political soundbites.”
For this reason, Wilson-Raybould’s statement contains “a lot of baloney.”
METHODOLOGY
The Baloney Meter is a project of The Canadian Press that examines the level of accuracy in statements made by politicians. Each claim is researched and assigned a rating based on the following scale:
· No baloney – the statement is completely accurate
· A little baloney – the statement is mostly accurate but more information is required
· Some baloney – the statement is partly accurate but important details are missing
· A lot of baloney – the statement is mostly inaccurate but contains elements of truth
· Full of baloney – the statement is completely inaccurate
Source: http://www.ctvnews.ca/politics/fact-check-will-legalizing-pot-keep-it-out-of-the-hands-of-kids-1.3397542 4th May 2017
In 2014, an estimated 22.2 million Americans aged 12 years or older had used marijuana in the past month.1
Under federal law, marijuana is considered an illegal Schedule I drug. However, over the last 2 decades, more than half of the states have allowed limited access to marijuana or its components, Δ9-tetrahydrocannabinol (THC) and cannabidiol, for medical reasons.2 More recently, 4 states and the District of Columbia have legalized marijuana for recreational purposes.
Currently, evidence for the therapeutic benefits of marijuana are limited to treatment and improvements to certain health conditions (eg, chronic pain, spasticity, nausea).3 Recreational use of marijuana is established by patterns of individual behaviors and lifestyle choices. In either case, use of marijuana or any of its components, especially in younger populations, is associated with an increased risk of certain adverse health effects, such as problems with memory, attention, and learning, that can lead to poor school performance and reduced educational and career attainment, early-onset psychotic symptoms in those at elevated risk, addiction in some users, and altered brain development.4- 7
In September 2016, the Substance Abuse and Mental Health Services Administration and the Centers for Disease and Control and Prevention (CDC) released an issue of the CDC’s Morbidity and Mortality Weekly Report—Surveillance Summary describing historical trends in marijuana use and related indicators among the non-institutionalized civilian population aged 12 years or older using 2002-2014 data from the National Survey on Drug Use and Health (NSDUH).8
During the last 13 years, marijuana access (ie, perceived availability) and use (ie, past-month marijuana use) have steadily increased in the United States, particularly among people aged 26 years or older, increasing from 54.9% in 2002 to 59.2% in 2014 and from 4.0% in 2002 to 6.6% in 2014, respectively. The factors associated with the national behavior patterns of marijuana use cannot be attributed solely to the heterogeneous body of state laws and policies that vary considerably with respect to year of enactment, implementation lag time, and access stipulations.
However, as state laws and policies continue to evolve, these data will be useful as a baseline to monitor changes in patterns of use and associated variables. Monitoring behavioral patterns is important given the possible increased risk of adverse health consequences due to potency changes—higher concentrations of THC (the psychoactive compound)—of the cannabis plant in the United States in the last 2 decades.9
Estimates from NSDUH data suggest that in 2014, 2.5 million persons aged 12 years or older had used marijuana for the first time within the past 12 months; this projected estimate suggests that there is an average of about 7000 new users each day (approximately 1000 more new users each day in 2014 compared with in 2002). In 2014, mean age at first use of marijuana was 19 years among persons aged 12 years or older and was 15 years among persons aged 12 to 17 years.8
During 2002-2014, the estimated prevalence of marijuana use in the past month, in the past year, and daily or almost daily increased among persons aged 18 years or older but
not among those aged 12 to 17 years, while the perceived risk from smoking marijuana decreased across all age groups. Conversely, the estimated prevalence of past-year marijuana dependence decreased from 1.8% in 2002 to 1.6% in 2014 among all persons aged 12 years or older and from 16.7% in 2002 to 11.9% in 2014 among past-year marijuana users.
Overall, the perceived availability to obtain marijuana among persons aged 12 years or older increased, and acquiring marijuana by buying the drug and growing it increased vs obtaining marijuana for free and sharing the drug. The percentage of persons aged 12 years or older perceiving that the maximum legal penalty for the possession of 1 oz or less of marijuana in their state of residence is a fine and no penalty increased vs perceptions that penalties included probation, community service, possible prison sentence, and mandatory prison sentence.8
These findings on perceived availability to obtain marijuana and fewer punitive legal penalties (eg, no penalty) for the possession of marijuana for personal use may play a role in the observed increased prevalence in use among adults in the United States. However, surveillance data do not reveal causal relationships; therefore, more granular research is needed.
As states adopt policies that increase legal access to marijuana, new indicators will be needed to understand trends in marijuana use and the risk of health effects. Questions regarding mode of use (eg, smoked, vaped, dabbed, eaten, drunk), frequency of use, potency of marijuana consumed, and reasons for use (ie, medical use, recreational use, or both) could be added to existing surveillance systems or launched in new systems.
Traditionally, understanding factors underlying the trends in marijuana use have been assessed by looking at 1 or 2 indicators (eg, perception of harm risk or dependence or abuse). A multivariable approach that includes environmental (eg, law enforcement, laws/policies) and cultural (eg, religion, individual choice) factors might be required to understand the relationship between the perceptions and attitudes toward marijuana and use behavior.
The health effects associated with marijuana use are still widely debated. Nonetheless, marijuana use during early stages of life, when the brain is developing, poses potential public health concerns, including reduced educational attainment, addiction in some users, poor education outcomes, altered brain structure and function, and cognitive impairment.4- 7
Given these potential health and social consequences of marijuana use, additional data sources at the federal and state levels may be required to assess the public health effects of marijuana use. These sources may include data from sectors such as health care (eg, emergency department data), criminal justice (eg, law enforcement data), education (eg, school attendance and performance data), and transportation (eg, motor vehicle injury data).
Assessing the prevalence and public health effects of marijuana use in the United States remains important given the evolving policies for marijuana for medical or recreational use at the state level. Therefore, it is vital to continue to monitor key traditional marijuana indicators but also to enhance public health surveillance to include monitoring of indicators that assess emerging issues so that public health actions could prevent adverse health consequences.
Given that legislation, types of products, use patterns, and evidence for potential harms and benefits of marijuana and its compounds are all evolving, clinicians need to understand the magnitude of marijuana use and associated behaviors so they can provide informed answers to patient questions, screen, counsel, treat, and refer patients to community treatment or counseling centers if abuse or adverse effects are identified.
Source: JAMA. 2016;316(17):1765-1766. doi:10.1001/jama.2016.13696
The “bud tender” had shoulder length black hair, a deep well of patience and a connoisseur’s pride in his wares as he spread tray after tray of marijuana-based products on the glass counter top.
There were fruit gums, chocolate caramels, granola packets, medicated sugar to drop in your coffee or tea in the morning, Rosemary Cheddar Crackers for a savoury taste, a bath soak and even sensual oil for the bedroom, Charles Watson explained.
Then he moved on to his dozen jars of green, frosted-looking marijuana lumps for smoking, all grown legally in Denver and all named and labelled with a percentage breakdown of their chemical composition to indicate their potency and character.
How marijuana changed Colorado
Mr Watson, a salesman for the prominent Colorado marijuana chain Native Roots, explained that he had a higher tolerance than most users to his products’ effects. For a novice he suggested Harlequin, which would be similar to the cannabis you would have found in the Sixties or early Seventies. It was milder than something like Alien OG with its sky-high THC, or tetrahydrocannabinol, content. “Even smoking a tiny bit of that can get you nice and elevated,” Mr Watson said.
Almost anywhere else in the world Native Roots would be considered an unusually well-stocked drug den and Mr Watson could be facing time in jail. In Colorado, where sales of recreational marijuana to adults over 21 have been legal since January 2014, he is one of more than 27,000 people licensed to work in a booming new industry with global ambitions.
“We’re trying to show the world you can sell and regulate it in a responsible manner,” Mr Watson said. His clients are not only stereotypical stoners — they include everyone from the healthy guy that’s just run a marathon to wheelchair users who are inhaling oxygen.
Colorado’s governor, John Hickenlooper, opposed legalisation at the time of the vote in 2012 and subsequently said that he wished he could wave a magic wand and abolish it. In May, however, he changed his tune. “If I had that magic wand now, I don’t know if I would wave it,” he said. “It’s beginning to look like it might work.”
By the end of this year, if a series of state referendums fall in favour of legalisation, recreational marijuana could be approved in nine states, including California, whose economy was the sixth largest in the world last year.
Colorado raised $135 million from marijuana fees, licences and taxes last year, a fraction of the overall state budget of $27 billion but welcome revenue all the same.
Recreational and medical marijuana customers pay a 2.9 per cent regular Colorado sales tax charge and any local taxes. Recreational consumers are also charged an additional 10 per cent state marijuana sales tax and the price of their marijuana includes a 15 per cent excise tax paid by the retailer when purchasing his wares from the grower. The revenue feeds into a state schools building programme. If it is legalised in California, voters will decide whether a portion of the taxes from recreational marijuana sales will go towards tackling the state’s homelessness problem.
There are still marijuana-related crimes in Colorado, for example where the supplier is unlicensed or the customer is under 21 but there are far fewer than previously. The total number of marijuana-related prosecutions fell by more than 8,000 a year between 2012 and 2015, and was down 69 per cent among the 10-17 age group.
Violent crime fell by 6 per cent and property crime dropped by 3 per cent between 2009 and 2014, the first year of the experiment, debunking pessimistic forecasts made before legalisation.
The state’s senior law enforcement official, Stan Hilkey, the executive director of the Colorado Department of Public Safety, said he was surprised by the results. “During the debate there was a ‘sky is gonna fall’ mentality from a lot of us, including me,” he said. “I haven’t seen that.” He said, however, that after three decades as a police officer he found it difficult “to shed my cop glasses”. Asked if legalisation had brought any benefits to the public or to law enforcement, he said: “None that I’m aware of.”
In May the state’s county sheriffs, prosecutors and police chiefs wrote to Colorado legislators to complain about the extra workload foisted on them by legalisation. They called for a two-year break from the constant tweaks to the regulation of
medical and recreational marijuana. Their letter said that there had been 81 bills on the subject introduced in the previous four years.
They wrote: “Industry forces are working constantly to chip away at regulations put in place to protect public health and safety.”
Mr Hilkey added that legalisation had failed to defeat the black market, which continues to thrive because its product is cheaper and not restricted by age. It has also created new problems, including the illegal export of licensed and unlicensed marijuana to neighbouring states and almost certainly brought greater profits to organised crime activity in Colorado.
The ban on marijuana sales at national level means that officially at least, banks will not open accounts for marijuana growers or vendors, so the industry remained a cash business, he said. Therefore this made it ripe for criminals.
There were 2,538 licensed marijuana businesses in Colorado last December, many of which hire security to protect against armed robberies.
Last month a former Marine Corps veteran working as a guard at the Green Heart dispensary in Aurora, near Denver, was shot dead in a botched robbery, the first killing at a licensed marijuana business, though not the first robbery.
Two days later a small group of Republicans in Congress blocked a measure backed by both parties that would have effectively opened the banking system to marijuana businesses.
You get dirty looks if you smoke a cigarette in the street but people barely think twice if they smell weed
A spokesman for Blue Line Protection Group, one of the largest companies competing to provide security and compliance services to the new industry, said that it was a myth that there was no banking. In practice some local banks and credit agencies now feel comfortable offering services to the marijuana industry but the national chains are still waiting for approval from the federal government.
Andrew Freedman, the governor’s director of marijuana coordination, said that if California voters passed recreational legalisation, the federal government would feel compelled to step in to open up legitimate banking for the industry.
Mr Freedman, a lawyer who refuses to give a personal opinion on legalisation, said that Colorado had succeeded in creating a heavily regulated marijuana industry where consumers could safely buy a healthier product than was available on the black market.
He said that it was too early to answer many of the most pressing questions about legalisation, including what impact it had on alcohol, tobacco and opioid usage although he had been pleasantly surprised by how few tragedies there had been through marijuana overdoses.
His greatest worry is that over time people’s comfort with legalisation could make radically different patterns of marijuana use socially acceptable.
That may be happening already though. Evan Borman, 33, an architect who lives down the street from a medical marijuana shop, said attitudes in the state were shifting, though he claimed that he smoked “no less and no more” than he did before legalisation. He said: “You get dirty looks if you smoke a cigarette in the street but people barely even think twice if they smell weed.”
Source: http://www.thetimes.co.uk/article/yes-it-s-legal-but-the-law-s-still-a-drag-j8rdh3nbj August 22nd 2016
An ITV News investigation has uncovered how children as young as 12 are being ruthlessly groomed and exploited by organised crime groups who send them the length and breadth of the country to carry drugs and money.
Working round-the-clock as a 14-year-old drugs mule
ITV News has seen an internal Home Office document which describes this as a “new type of organised crime” that is “unreported”.
It also suggests the number of kids involved is “unrecorded”. And it contains a stark warning; suggesting that current government practice – including the inability of public services to work together – “might be making it easier for criminal gangs to exploit vulnerable people”.
Warning signs that your child may be involved in a gang
Speaking to ITV News, Children’s Commissioner Anne Longfield called for the same “mindset change” about these young adults being groomed to run drugs by gangs as that after child sex exploitation was uncovered across Britain in 2014.
One teenager described to ITV News how he was groomed by drug gangs. We spoke to one 15-year-old boy, caught up in this dangerous world since the age of 13.
Daniel described how drug dealers groomed him, gave him gifts and made him feel part of their group.
“They’d pick me up around the corner from my house. They’d give me a lift to school and I’d get out and you just felt like you were important getting out of a nice big car.”
“Anything I ever wanted I got given and I thought it was all for free,” Daniel added.
But he soon realised they wanted something in return. They asked him to deliver shoeboxes of class A drugs and bags of pills, often having to travel long distances from home.
Daniel is still trying to escape this life.
And he’s not alone. We’ve discovered that young boys and girls are being sent out from major cities including Liverpool, London, Manchester and Birmingham to towns and coastal resorts right across Britain.
Others are directed from the capital to Winchester, Peterborough and towns along the south coast.
Children as young as 12 are being sent out from major cities. Credit: ITV News
We heard of boys being sent from Manchester to Aberdeen and Grimsby and teens from Liverpool turning up in Essex and Exeter. The police call it “county lines”, the children call it “going country”.
Home Office documents seen by ITV News describe it a “new type of organised crime” that is “unreported” and “unrecorded”. The department said the number of kids involved is “unrecorded” but our research suggests it runs into thousands.
Stephen Moore, a former senior detective at Merseyside Police and an expert in organised crime, says the drug syndicates see this as a business and children represent cheap labour, easy to exploit and easy to replace if anything happens to them.
“This is like mill owners using kids in Victorian times or sending kids down mines – cheap, easily replaceable labour, ” Mr Moore said. The gangs prey on school children but the Home Office documents warn they particularly target vulnerable young people from children’s care homes, or those who have been excluded from mainstream education.
It’s a growing problem. In just one small area of Essex around Clacton-on-Sea, police say there are as many as 19 ‘county lines’ running from Liverpool, London and Manchester Caroline Shearer runs the charity Only Cowards Carry, which works with young people to keep them safe.
“Once a child is in a drug ring it’s very hard to get out,” she told ITV News.
Really there’s three ways. You can run away and hope that nobody ever finds you. You can go to prison, which is probably the best bet to help you get out of it, unfortunately. You can die because you will not get out of it. And unfortunately this is something that most people don’t understand.
– CAROLINE SHEARER, CHARITY OWNER
Experts think many of the children who go missing every year in this country may have actually have “gone country”. In one London borough, Lewisham, the local authority believes half of its missing children have been groomed to carry drugs.
Children’s Commissioner Anne Longfield said there are parallels with child sexual exploitation and action is urgently needed to protect boys and girls. The Children’s Commissioner said a mindset change is needed to tackle the issue.
“I think as a country we have had a very serious and overdue wake-up call about child sexual exploitation and saw that very starkly in areas such as Rotherham,” she said.
“There are youngsters involved in gangs who are in every other sense being groomed into that situation and being exploited and if we are going to protect them and prevent them being in those gangs and coming to harm we need that same scale of mindset change about them.”
It appears the UK’s drug trade has reinvented itself, expanding from inner cities to parts of the new country and exploiting children has allowed it to do this without detection.
In January we announced our Ending Gang Violence and Exploitation approach, which includes specific action to tackle county lines, protect vulnerable locations and safeguard gang-associated women and girls. The National Crime Agency published its first threat assessment of ‘County Lines’ in August 2015 and is working closely with the National Policing Lead for Gangs to ensure there is a national, coordinated response from law enforcement.
– HOME OFFICE STATEMENT
Source: http://www.itv.com/news/2016-09-29/going-country-itv-news-reveals-the-scale-of-children-being-exploited-and-sent-around-britain-to-carry-drugs/
States that have legalized marijuana are contending with a new criminal tactic — smugglers who grow and process it for export to states where it’s illegal and worth a lot more.
Colorado is the epicenter of the phenomenon, although it’s popping up in Oregon and Washington too. Now as Maine, Massachusetts and Canada consider legalizing recreational marijuana, the question arises — will the Northeast see a wave of new-age bootleggers?
During the Prohibition era, it was whiskey being run from Canada or Mexico to the U.S. Now it’s marijuana that’s being smuggled — from Colorado, where it has been fully legal since 2014, to neighboring states and beyond.
“It’s probably our No. 1 concern.” says Andrew Freedman, who directs marijuana policy for Colorado Gov. John Hickenlooper.
Freedman says organized criminals are exploiting legal loopholes by collecting home-grow licenses that allow for as many as 99 marijuana plants each. And more generally, he says, criminals are using the state’s fully legalized pot economy as cover.
“Different ways you can use Amendment 20 and 64, the medical and the recreational, to kind of cloak yourself in legitimate growing. Unfortunately there are a lot of people who want to do that in order to sell out of state because there’s a huge economic incentive to want to sell out of state right now,” he says.
As in, a pound of pot, worth, say, $1,500 at the counter of a legal Colorado marijuana shop is worth $3,000 or more when it crosses the state border, instantly transmuted into a prized black-market commodity. And criminal gangs are moving in, creating a headache for Colorado law enforcement, danger to public safety and a field day for the media.
The U.S. Drug Enforcement Administration says last year, state highway patrols intercepted more than 3,500 pounds of marijuana that was destined for states beyond Colorado’s border. That’s just a tenth, they estimate, of the actual cross-border market, making it, conservatively, a $100 million-plus proposition. Those numbers do not include busts of some pretty big syndicates, many of them recently involving Cuban nationals shipping product to Florida.
And for Colorado’s neighboring states, it’s a doubly-frustrating problem, because it’s not of their own making.
“In Nebraska, Colorado’s become ground zero for marijuana production and trafficking,” says Jon Bruning, Nebraska’s attorney general, who with his counterpart in Oklahoma is trying to sue Colorado and force it to overturn its marijuana laws. “This contraband has been heavily trafficked in our state. While Colorado reaps millions from the production and sale of pot, Nebraska taxpayers have to bear the cost. Virtually every aspect of Nebraska’s criminal justice system has experienced increased expense to deal with the interdiction and prosecution of Colorado marijuana trafficking.” One Nebraska study found that border counties saw gradual increases in pot-related arrests, jailings and costs since medicinal marijuana was legalized in Colorado, and a surge in 2014, when the recreational pot law went into effect. But the U.S. Supreme
Court recently declined to review the complaint by Colorado’s neighbors, which are looking for other venues to pursue their case.
Meanwhile, here on the East Coast, voters in Massachusetts and Maine are considering full legalization on the November ballot, and Canada Prime Minister Justin Trudeau is calling for legalization there. If those measures are all approved, police in New Hampshire are wondering what it would be like to be nearly surrounded by legal pot territory.
Andrew Shagoury is Tuftonboro’s chief of police, and the New Hampshire Chiefs of Police Association’s point-man on pot. If Maine or Massachusetts does go for legalization, he expects that at the least, problems such as small-scale smuggling and intoxicated driving will spill over the border.
“If more does spill over, the direct effect I suspect will be more accidents with people under the influence — obviously that would be a public safety concern. And I think politically you’d see more pressure for it to pass here too,” he says.
And Massachusetts Attorney General Maura Healy expects organized crime to open up new fields of operation.
“What’s going to stop a drug cartel from purchasing property, renting property here and running an operation at the property? And that’s something that could be situated next to a school, next to a hospital, in a suburban neighborhood. That’s a real problem,” she says.
But some note that Colorado neighbors such as Nebraska and Omaha have relatively strict marijuana laws, creating a strong incentive for smugglers there. In New England there is a more relaxed culture around marijuana — every state in the region, except for New Hampshire, has decriminalized possession of small amounts of pot and allowed use of medicinal marijuana, perhaps reducing potential black-market demand.
Essentially, says Vermont Attorney General William Sorrell, Vermonters are already growing enough pot to meet most of their smoking needs. But Sorrell is worried about the introduction of edible marijuana products into the regional marketplace.
“And I really think the regulators have to do a lot more effective work on quality control so that buyers know what is the THC content, what is a legitimate serving or portion because I think there has been and will continue to be a problem with over ingestion of marijuana,” he says.
There are specific parts of the measures in Maine and Massachusetts that could make it harder for criminals to aggregate licenses for big grow operations. And advocates of ending pot prohibition point to what they believe would be the most effective way to end the black market economy — to legalize marijuana in every state.
Source: http://mainepublic.org/post/will-legalizing-marijuana-create-modern-bootlegger 21st Sept.2016
More of the U.S. workforce is testing positive for drugs, according to lab tests at Quest Diagnostics.
For the fifth straight year, the detection rate of amphetamine and heroin rose, while marijuana increased by 47 percent since 2013.
The analysis of 11 million workforce drug test results from 2015 shows a steady increase or a 10-year high in positive results, Quest said in a statement.
Here are some of the insights from the test results:
* Positivity rate was 4 percent in 2015, compared to 3.9 percent in 2014 for urine tests.
* The last year that positivity rate for urine tests was at or more than 4 percent was 2005.
* Post-accident urine test have been increasingly positive for drugs, from 6.5 percent in 2014 to 6.9 percent in 2015.
* An increase from 6.7 percent to 9.1 percent in marijuana positivity.
* Almost 45 percent of workforce tests were positive for marijuana in 2015.
“This report shows a welcome decline in workplace drug test positives for certain prescription opiates but a disturbing increase in heroin positives. This rise in heroin should concern both policymakers and employers. Substance abuse is a safety risk for everyone. This new workplace evidence is an additional sign of the rising national heroin problem, this time in the workplace,” said Robert DuPont, former director of the National Institute on Drug Abuse, in a statement through Quest.
Mark de Bernardo, executive director of the Institute for a Drug-Free Workplace, said the numbers underscore the threat to employers and employees from drug abuse and should provide a wake-up call to all.
Source: http://www.njbiz.com/article/20160916/NJBIZ01/160919875/greater-number-of-us-workforce-is-testing-positive-for-illegal-drugs Sept.16 2016
By Christopher Ingraham
Source: Washington Post
USA — An appeals court ruled last week that a federal law prohibiting medical marijuana cardholders from purchasing guns does not violate their Second Amendment rights, because marijuana has been linked to “irrational or unpredictable behavior.”
The ruling came in the case of a Nevada woman who attempted to purchase a handgun in 2011, but was denied when the gun store owner recognized her as a medical marijuana cardholder, according to court documents. S. Rowan Wilson maintained that she didn’t actually use marijuana, but obtained a card to make a political statement in support of liberalizing marijuana law.
Federal law prohibits gun purchases by an “unlawful user and/or an addict of any controlled substance.” In 2011, the Bureau of Alcohol, Tobacco and Firearms clarified in a letter that the law applies to marijuana users “regardless of whether [their] State has passed legislation authorizing marijuana use for medicinal purposes.” Though a growing number of states are legalizing it for medical or recreational use, marijuana remains illegal for any purpose under federal law, which considers the drug to have a high potential for abuse and no accepted medical use.
The U.S. Circuit Court of Appeals for the 9th Circuit ruled that the federal law passes muster with the Constitution, as “it is beyond dispute that illegal drug users, including marijuana users, are likely as a consequence of that use to experience altered or impaired mental states that affect their judgment and that can lead to irrational or unpredictable behavior.”
The court then concluded that it is reasonable to assume that a medical marijuana cardholder is a marijuana user, and hence reasonable to deny their gun purchase on those grounds.
From a legal standpoint, the nexus between marijuana use and violence was established by the U.S. Court of Appeals for the 4th Circuit in Virginia, in the 2014 case of United States v. Carter. That case cited a number of studies suggesting “a significant link between drug use, including marijuana use, and violence,” according to the 9th Circuit’s summary.
In the words of the 4th Circuit, those studies found that: “Probationers who had perpetrated violence in the past were significantly more likely to have used a host of drugs — marijuana, hallucinogens, sedatives, and heroin — than probationers who had never been involved in a violent episode.”
“Almost 50% of all state and federal prisoners who had committed violent felonies were drug abusers or addicts in the year before their arrest, as compared to only 2% of the general population.”
“Individuals who used marijuana or marijuana and cocaine, in addition to alcohol, were significantly more likely to engage in violent crime than individuals who only used alcohol.”
Among adolescent males, “marijuana use in one year frequently predicted violence in the subsequent year.” The 4th Circuit argued that, on the link between drug use and violence, the question of correlation vs. causation doesn’t matter: “Government need not prove a causal link between drug use and violence” to block firearms purchases by drug users. A simple link between drug use and violence, regardless of which way the causality runs, is grounds enough. Still, the 9th Circuit did suggest causation was part of its decision, saying that irrational behavior can be “a consequence” of marijuana use.
This argument — that substance use increases risky behavior — applies to plenty of other drugs, too, and not just illegal ones. For instance, drug policy researchers Mark Kleiman, Jonathan Caulkins and Angela Hawken have pointed out that tobacco users also are more likely to engage in crime relative to the general population. “Compared with nonsmokers, cigarette smokers have a higher rate of criminality,” they wrote in their 2011 book Drugs and Drug Policy: What Everyone Needs to Know. “Smoking in and of itself does not lead to crime, but within the population of smokers we are more likely to find individuals engaged in illicit behavior.”
The authors also point out that there’s a much stronger link between violent behavior and alcohol than there is for many illegal drugs: “There is a good deal of evidence showing an association between alcohol intoxication and pharmacologically induced violent crime,” they write. They added: “There is little direct association between marijuana or opiate use and violent crime. … it is also possible that for some would-be offenders, the pharmacological effect of certain drugs (marijuana and heroin are often given as examples) may actually reduce violent tendencies.”
Christopher Ingraham writes about politics, drug policy and all things data. He previously worked at the Brookings Institution and the Pew Research Center.
Source: Washington Post (DC) September 7, 2016:
On July 28 and July 29, agents of the Humboldt County Sheriff’s Office assisted by the Campaign Against Marijuana Planting (CAMP) and the United States Forest Service (USFS) responded to USFS property on Brush Mountain, Gainor Peak and Oak Knob in eastern Humboldt County after sighting marijuana being cultivated on USFS land. The deputies were also accompanied by three scientists, two from Integral Ecology Research Center, and one associated with UC Davis and Hoopa Tribal Wildlife Ecologist.
During the two days deputies seized 3,760 marijuana plants ranging in size from 18 inches to four feet. Deputies and scientists located water diversion, mounds of trash and 24 pounds of rodenticides, of which nine pounds were peanut butter flavored and 15 pounds were second generation rodenticide. Malathion and fertilizers were also located at the scenes. No suspects were located in the area of the trespass marijuana grows, however deputies obtained evidence from the scenes that is being processed and the investigation is ongoing.
The spring fed water sources, which had been diverted and used to water marijuana plants, flow into the South Fork of the Trinity River. The springs were part of a network of subterranean water sources. The scientists reported that impacts from the water diversions and chemicals used on the grows could affect Coho salmon, Chinook salmon, steelhead, foothill yellow-legged frogs and the western pond turtles.
The scientists reported the rodenticides could potentially kill fishes, Northern spotted owls, American black bears, black tailed deer and Humboldt martens.
Below are some quotes from Dr. Mourad Gabriel of the UC Davis Wildlife Ecologist/Integral Ecology Research Center, who was present with the deputies and USFS agents.
“The removal of this massive amount of killing agents within prime spotted owl and fisher habitat is pertinent for the conservation of these species.”
“The illegal diversion of this amount of water prohibits the flow of cool water into tributaries that support our salmon populations.”
In light of the current drought and high water temperatures, this represents another blow to our already taxed watersheds.”
“The remediation efforts are crucial in protecting our forest ecosystems.”
Anyone with information for the Sheriff’s Office regarding this case or related criminal activity is encouraged to call the Sheriff’s Office at 707-445-7251 or the Sheriff’s Office crime tip line at 707-268-2539.
Redwood Times Posted: 08/11/2014
http://www.redwoodtimes.com/news/ci_26315593/trespass-grows-found-usfs-land
I continue to be puzzled by an attitude that if something is difficult to enforce then we should abandon attempts and just legalize it. That is apparently the attitude of Oregon’s politicians (Republican and Democrat alike) and is reflected in the comments of the official spokesman for the government elites – The Oregonian – in its August 23 edition:
“Oregon has had a wink-wink, nudge-nudge relationship with recreational marijuana use since 1998, when legalization for medical purposes created a wide, open system that distributes pot cards to just about anyone with a vague medical claim and the signature of a compliant physician. We’re not suggesting that marijuana has no palliative value to those with genuine medical problems. But let’s be honest: Recreational marijuana is all but legal in Oregon now and has been for years. Measure 91, which deserves Oregonians’ support, would eliminate the charade and give adults freer access to an intoxicant that should not have been prohibited in the first place.”
There it is. The marijuana advocates foisted a canard on Oregonians by exploiting the plight of those benefiting from the use of medical marijuana. Having convinced Oregonians that those is need should not be denied, they set up a system that guaranteed abuses and then urged others to look the other way when the abuses became obvious and widespread. Wink, wink, nod, nod. There’s a solid foundation for change. (For those of you forced to endure a teachers union led education in Portland public schools, that is what is meant by “sarcasm”.)
And now the second canard is upon us with the assertion that “everyone is already doing it” and that recreational marijuana is not harmful. When the push began, those supporting it chanted “nobody has ever died from marijuana.” And that folks, is just plain bulls—t.
A New York Times article on May 31, 2014, noted:
“Five months after Colorado became the first state to allow recreational marijuana sales, the battle over legalization is still raging.
“Law enforcement officers in Colorado and neighboring states, emergency room doctors and legalization opponents increasingly are highlighting a series of recent problems as cautionary lessons for other states flirting with loosening marijuana laws.
“There is the Denver man who, hours after buying a package of marijuana-infused Karma Kandy from one of Colorado’s new recreational marijuana shops, began raving about the end of the world and then pulled a handgun from the family safe and killed his wife, the authorities say. Some hospital officials say they are treating growing numbers of children and adults sickened by potent doses of edible marijuana. Sheriffs in neighboring states complain about stoned drivers streaming out of Colorado and through their towns.”
On May 24, 2014, Newsweek reported:
“Wednesday’s move in Colorado to tighten rules on edible goods made with pot comes after two adult deaths possibly linked to such products. Meanwhile, a Colorado children’s hospital said it has seen an uptick in the number of admissions of children who ingested marijuana-laced foods since the start of the year.
“’Since the … legalization of recreational marijuana sales, Children’s Colorado has treated nine children, six of whom became critically ill from edible marijuana,’ the statement from Colorado Children’s Hospital said.”
And The Raw Story reported on April 2, 2014:
“A Wyoming college student visiting Colorado on spring break is the first reported death related to the legal sale of recreational marijuana.
“Levy Thamba, a student at Northwest College, fell to his death last month from the balcony of a Holiday Inn in Denver.
“Autopsy results released Monday showed the 19-year-old Thamba, who was also known as Levi Thamba Pongi, died from multiple injuries caused by the fall. But the coroner also listed ‘marijuana intoxication’ from a pot-infused cookie as a significant contributor to the student’s death.”
And finally, CBS reported from Seattle on February 4, 2014:
“According to a recent study, fatal car crashes involving pot use have tripled in the U.S.
‘Currently, one of nine drivers involved in fatal crashes would test positive for marijuana,’ Dr. Guohua Li, director of the Center for Injury Epidemiology and Prevention at Columbia, and co-author of the study told HealthDay News.”
But the Oregonian is undeterred by the mounting evidence of harm:
“Opponents of the measure are right about a couple of things. Allowing retail sales of recreational marijuana inevitably will make it easier for kids to get their hands on the stuff, as will Measure 91′s provision allowing Oregonians to grow their own. It’s also true that outright legalization will increase the number of people driving under the influence, which is particularly problematic given the absence of a simple and reliable test for intoxication. There is no bong Breathalyzer.
“As real as these consequences are, Oregonians should support outright legalization. . .”
We have imposed safety requirements on a whole host of things including guns, automobiles, golf carts, children’s toys and food products that have a lower incident rate of death and injury than is being currently compiled by the unrestricted use of marijuana. Oregon is now tying itself in knots trying to eliminate the use of genetically modified organisms (GMO) with no scientific evidence of harm and only a speculation as to what might become. But there is no apparent concern about the modification of marijuana to increase its potency which has resulted in numerous adverse health issues with children and adults alike.
And while the Oregonian acknowledges that there is no “simple and reliable test for marijuana intoxication” it fails to note that there is similarly no simple and reliable test for testing potency. There are no labeling requirements and no guidelines as to the limits of consumption and impairment. Contrast that with the liquor industry that has defined limits and labeling on the alcohol content of various beers, wine and liquors. There are exacting studies that demonstrate the effects of alcohol on a person given weight variations.
And yet the Oregonian ignores that in favor of addressing it sometime in the future – maybe.
And Oregon’s politicians are even less helpful because they are fixated on tax revenue opportunities from the unrestricted use of marijuana. Little thought is
being given to the problems that will be caused. Their sole focus is upon using regression analysis to determine how high the tax can be without seriously reducing the volume of consumption – it is the same myopic view used when determining the tax on tobacco. That amount of tax will increase over time as the use becomes more widespread and the dependency becomes more pronounced and as state government becomes more dependent on the revenue generated, the ability to correct the abuses of marijuana will be marginalized – just like tobacco.
In the end, this is all about the “me generation” and that pervasive attitude that “if it feels good, do it.” It furthers the myth of life without consequences. The only upside is for those who eschew getting high in favor of getting hired – your prospects for getting a good job and routine promotion are greatly enhanced.
Source: www.oregoncatalyst.com 27th August 2014
I live in Denver, where marijuana dispensaries outnumber pharmacies, liquor stores, McDonald’s and Starbucks. When I walk and drive the streets of this beautiful Rocky Mountain city, I often encounter the smell of marijuana smoke. Marijuana users are not allowed to smoke openly and publicly, but a bench in the front yard is considered private property, allowing the smell to pollute the clean mountain air.
The problems in Colorado began 14 years ago with the passage of Amendment 20 legalizing medical marijuana. Abuse and fraud flourished under its provisions because medical marijuana became easily available for recreational use.
In November, Florida voters will be faced with the choice to legalize marijuana for “medical use.” Voters should instead ask themselves whether they want marijuana legalized in Florida for recreational use. That’s essentially what Amendment 2 will do. The amendment is so flawed that if it passes, medical marijuana will be readily available for anyone who wants to obtain it.
Like Colorado, Florida’s Amendment 2 allows “Medical Marijuana Treatment Centers” to develop edibles. These food products have been developed intentionally to allow discreet consumption of marijuana in public places, at schools and in the workplace, and to introduce the product to a larger – younger – consumer base.
In Colorado, marijuana is sold in soda, salty snacks like nuts, granola bars, breakfast cereals, cookies, rice cereal treats, cooking oil and even salad dressing. Some companies buy commercially available children’s candies like Swedish fish, Sour Patch Kids, lollipops or lemon drops and infuse them with marijuana. Others make chocolate bars, Tootsie Rolls and truffles. So now in Colorado, parents who once taught their children not to take candy from a stranger must tell their children not to take candy from a friend because it could very well contain marijuana. Our emergency rooms report a striking increase in children who have unintentionally ingested marijuana edibles and require medical treatment.
Florida’s Amendment 2 allows for any medical condition, not just terminal, chronic or debilitating conditions, to qualify for marijuana treatment, as long as “a physician believes that the medical use of marijuana would likely outweigh the potential health risks for a patient.” This exception will result in patients who use marijuana to get high, despite the stated intention of the amendment to prohibit such conduct.
Colorado’s marijuana patient registry statistics show that only 1 percent of patients list HIV/AIDS; 2 percent, seizures; and 3 percent, cancer. A whopping 94 percent of those using “medical marijuana” claim to have “severe pain,” a subjective and unverifiable condition.
Sixty-six percent of users are male with an average age of 41, despite severe pain being a condition more closely associated with older, female patients. In Denver, it is common to see young, 20-something able-bodied men flocking to medical marijuana centers Friday and Saturday nights to get their “medicine.” Since outright legalization in 2012 for all persons 21 or older, Colorado has seen an explosion of medical marijuana patients between 18-20 years old.
Moreover, the long-term health implications from youth marijuana use are troubling. A longitudinal study found an association between weekly marijuana use by persons under the age of 18 and permanent decline in IQ.
You might think Florida won’t go as far as Colorado and Washington, but it will be one step closer. Every state that passes medical marijuana laws believes they will be able to correct the errors of those who have paved the way. This has yet to be accomplished.
The Colorado experiment is failing our children, and so will Florida’s. Coloradans may not be able to go back in time, but you can stop yours before it starts.
Rachel O’Bryan is a Colorado resident and an attorney who spent 18 months serving at the request of Governor John Hickenlooper and the Colorado Department of Revenue to aid in the development of recreational marijuana legislation and regulation. She is a founding member of SMART Colorado, a citizen-led nonprofit that protects Colorado kids from the unintended negative consequences of legalizing marijuana for recreational use.
Powdered alcohol was approved by a government agency on Tuesday, The Washington Post reports. The product, called “Palcohol,” could arrive in stores this summer. Last year the Alcohol and Tobacco Tax and Trade Bureau (TTB) approved labels for powdered alcohol. It then said the approval had been a mistake.
Lipsmark, the company that makes Palcohol, plans to sell four powdered products: cosmopolitan, margarita, a vodka and a rum, the article notes. The product will be sold in foil pouches that can be used as a glass. A person pours in five ounces of water, zips up the bag and shakes it until the powder dissolves.
Several states, including Louisiana, South Carolina and Vermont, have banned the use/sale of powdered alcohol, and a number of other states are considering similar legislation.
U.S. Senator Charles Schumer of New York introduced a bill last year to ban powdered alcohol. Last May Schumer urged the Food and Drug Administration (FDA) to prevent federal approval of powdered alcohol. He said it could become “the Kool-Aid of teen binge drinking.” Schumer noted the product can be mixed with water, sprinkled on food or snorted. He asked the FDA to investigate the potential harmful effects of the product.
In a statement released last May, Mothers Against Drunk Driving (MADD) said it agreed with Schumer. “This product is the latest in a long list of specialty alcohol fads,” MADD said. “As with anything ‘new,’ this product may be attractive to youth. … In the case of Palcohol, we share Senator Schumer’s view that the U.S. Food and Drug Administration should carefully review this product as it would seem to have the potential to increase underage drinking.” The FDA approved powdered alcohol last summer, the article notes.
Source: www.drugfree.org 12th March 2015
For decades, the Netherlands has been known for its tolerant cannabis laws – the poster nation for pro-pot advocates. Cannabis users from across the world have flocked to Amsterdam to patronize its many cannabis-selling “coffee shops.” Throughout this time cannabis has remained illegal in the Netherlands; although, the Dutch have not prosecuted anyone in possession of less than five grams of cannabis for personal use. This distinctive drug policy of tolerance toward cannabis is called gedoogbeleid, and known as the “Dutch model.”
Now, the U.S. now is the first, and so far the only, nation in the world to have fully legal production, sale, promotion, and use of cannabis for people 21 an older. In stark contrast, the Dutch are moving in the opposite direction, limiting the growth, distribution, and use of cannabis and showing no interest in “medical marijuana.” Cannabis with a THC level of more than 15 percent is now under consideration to be reclassified as a “hard drug.” In the Netherlands, that designation comes with stiff criminal penalties. Furthermore, the nation once had more than 1,000 coffee shops, 300 in Amsterdam alone. Now, there are fewer than 200 in the city and 617 nationwide. This is the result of the government’s actions to force coffee shops to choose either to sell alcohol or marijuana. Notably, many are choosing to sell alcohol.
While it has always been illegal to grow cannabis in the Netherlands, for years police acted as if they didn’t know where the shops were getting the drug. This is no longer the case. Now, new laws target even the smallest cannabis growers. In the past, anyone could grow up to five plants without fear of penalty. In 2011, the government issued new police guidelines declaring that anyone who grew cannabis with electric lights, prepared soil, “selected” seeds or ventilation would be considered a “professional” grower. This is a significant change because professional growers risk major criminal penalties, including eviction and blacklisting from the government-provided housing in which more than half of the country’s citizens reside.
What made the Netherlands make such a strong shift in its cannabis policy? The overall drug policy of the Netherlands – not just for cannabis but including cannabis – has four major objectives:
1. To prevent recreational drug use and to treat and rehabilitate recreational drug users.
2. To reduce harm to users.
3. To diminish public nuisance by drug users (the disturbance of public order and safety in the neighborhoods).
4. To combat the production and trafficking of recreational drugs.
The Netherlands has determined that its relaxed cannabis laws were a threat to these expressed public health objectives. The nation’s new, more restrictive laws on cannabis, including the banning of cannabis with THC levels of 15 percent or more, demonstrate that the government wants to reduce cannabis sale and use for reasons of public health.
As the legalization of medical and recreational marijuana spreads to more states in the U.S., we need to look anew to the Netherlands. The U.S. can benefit from what the lessons the Netherlands has learned about cannabis over the past four decades. How surprising is it that the American media frequently praised the Dutch cannabis policy when it seemed permissive but now that Dutch have become more restrictive their new cannabis policy is ignored?
Robert L. DuPont, M.D.
President, Institute for Behavior and Health, Inc.
Former Director, National Institute on Drug Abuse (1973-1978) Former White House Drug Chief (1973-1977)
Source: www.ibhinc.org 15th March 2015
Should heavy drinking in pregnancy be a crime? A recent test case in the UK was thrown out, but in the US hundreds of women have been imprisoned. We meet women and children affected by foetal alcohol syndrome
I’d had problems all my life and I didn’t know why,’ says Stella, who found out at 19 that she has foetal alcohol syndrome.
Stella was 19 when she discovered she has foetal alcohol syndrome. “I found out in a horrible way, to be honest,” she says. She had taken her boyfriend to meet her father for the first time. Stella and her father had only limited contact, but her boyfriend hoped that he might help to explain some of Stella’s erratic, unreliable behaviour, and asked him upfront, “What’s wrong with your daughter? Why is she the way she is?”
“That’s when he paused, and he breathed, and he said it,” Stella says, still distressed at the memory of the conversation. “I was shocked. I asked, ‘Why wasn’t I told about it?’ He said he didn’t want me to dwell on something like that.
“My heart felt like it was jumping out of my mouth,” the 25-year-old remembers. “It killed me inside. Why have I lived all my life without knowing about it? It was a really bad time.”
Stella and I arrange to meet at her friend’s flat, and she arrives two hours late, hugely apologetic that she forgot all about it. She tells me she has struggled with timekeeping all her life. Articulate and thoughtful, she gives no real indication of having the disorder, aside from occasionally trailing off and losing her train of thought, asking, “What was I just saying there?” But she describes how catastrophically her life has been affected by the legacy of her mother’s drinking.
Foetal alcohol spectrum disorder (FASD) is the umbrella term for a range of birth defects associated with drinking in pregnancy. At the extreme end of the spectrum is foetal alcohol syndrome (FAS), a very rare condition caused by heavy or frequent alcohol consumption during pregnancy. FAS can cause a range of physical and cognitive problems. Some babies are born with facial abnormalities – thin upper lips, a flatter area between the lip and the nose, smaller eyes. Babies with both FAS and FASD are often smaller than other babies, and typically remain small throughout their lives. Some children may have no physical signs of the condition, but a range of developmental disorders – attention deficit, hyperactivity, poor coordination, language problems and learning disabilities. There is no reliable research on how common it is in the UK; some doctors believe FAS may affect one child in 1,000, and FASD between three and four times more. Adolescents and adults with FASD are overrepresented in the criminal justice system.
Stella spent much of her childhood in care, until she was 11, when her aunt took her in. Her mother died before her father broke the news, so she was never able to ask her about the past. Instead, she went to her GP, who looked at her files. “She said, ‘Yes, you do have this. Your mum was a heavy alcoholic.’” The GP printed out a document that said Stella had been diagnosed in 1993, aged three.
She took to researching the condition online. “It described things that made sense,” Stella says. “All my life, things had been happening to me, and it was suddenly explained. I’m not good with organisation, bills, day-to-day things. I can’t read and write. I’m not good at maths. I’d had these problems and I didn’t know why.” She has never had a job and wonders if she would manage. “I want everything to be simple. If it isn’t, my head feels scattered. I can’t focus. I can’t concentrate.”
Women shouldn’t be prosecuted – they should be given alcohol rehabilitation
At the end of last year, a controversial British court case hinged on whether a woman should be considered to be committing a crime if she drinks heavily during pregnancy. The case looked at whether the council caring for a seven-year-old girl with FAS was entitled to extract compensation from the Criminal Injuries Compensation Authority on her behalf. Lawyers examined the legal rights of an unborn child and asked whether alcohol consumption by the mother constituted the crime of poisoning.
The court of appeal ruled in December that the mother, who inflicted lifelong damage on her child by consuming large quantities of alcohol while pregnant, had not committed a criminal offence, and that her daughter was not, therefore, entitled to compensation. To date, no woman has been prosecuted under English law for harm she caused to her child in utero, but hundreds of women in the US have been imprisoned for drinking or taking drugs during pregnancy. And the legal battle here is far from over; lawyers representing the seven-year-old (who remains anonymous), and around 80 other children affected by FASD, are considering whether to pursue the case in the supreme court.
We’re not talking here about the effects of drinking a couple of glasses of wine at a friend’s wedding. The test case involved a woman who drank, by her own account, half a bottle of vodka and several cans of strong lager daily. But there is a growing sense among politicians and doctors that drinking during pregnancy is an issue that is not taken seriously enough. In Westminster, politicians have been debating whether official guidance over drinking in pregnancy is sufficiently clear. The Royal College of Obstetricians & Gynaecologists recently hardened its advice, saying women should avoid alcohol altogether in the first three months of pregnancy. NHS Choices, the government’s health advisory website, states that the UK chief medical officers’ advice is that abstinence is best, but adds, “If they do choose to drink, to minimise the risk to the baby, we recommend they should not drink more than one or two units once or twice a week and should not get drunk.” The chief medical officer for England is currently reviewing these guidelines.
Lost in all these discussions, however, have been the voices of adults affected by the condition, and those of mothers who have given birth to, and brought up, children with FAS. Among them, there is little appetite for further stigmatising of mothers. But there is agreement that pregnant women need clearer guidance and help, and that affected children need much more support.
Stella thinks she can identify in herself the facial characteristics that sometimes go with the condition (although they are not discernible to others, or me; she looks lovely). But, she says, “It is more mental. I am not capable of doing things. I was hyperactive when I was young. I never listened. I got picked on a lot at primary school; there was a lot of spiteful behaviour. I went to a special needs secondary school – that was better – but I should have had more support as a teenager.”
Although she finds it painful to talk about her childhood, Stella is determined to raise awareness of the syndrome. Recently, she has spoken at conferences arranged by support group the National Organisation for Foetal Alcohol Syndrome (Nofas), which has helped find a charity that provides regular support sessions, allowing her to live independently: “They help with finances and forms, things I am not capable of doing.”
Stella feels ambivalent towards her mother. “I feel some sort of hate and some sort of love,” she says. “I want to be able to go back and ask her questions – questions that will never be answered, because she is dead.” She wishes she had known earlier what the cause of her difficulties was, but she is clear that moving towards prosecuting women is not the right answer. “What difference will it make? She hasn’t committed a crime – she has an issue with alcohol.”
No woman I have met ever wants to harm her baby. This is an illness, not a choice
Laura has two sons with FASD: ‘I need to make sure this doesn’t happen to other people.’ Photograph: Sophia Spring for the Guardian
Laura has two teenage sons who were diagnosed with FASD a few years ago. She was pregnant with them in the 1990s, when – as she remembers it – there was real ambiguity about the levels of safe alcohol consumption for pregnant women, and she doesn’t remember being confronted by her midwives. Her partner was violent, she was beaten during the first pregnancy, and had panic attacks. “I was a social drinker, but increasingly I was using alcohol to cope. I went to all my appointments, they were aware that I drank – I was drinking beer, mainly, Holsten Pils. The midwife knew I was a four-times-a-week drinker.”
Laura’s first pregnancy progressed without any problems, and she “gave birth to a beautiful child”. Over the next few years, her relationship with the child’s father deteriorated, she lost her job and her home, and began to drink more and more. By the time she was pregnant with her second son, she was an alcoholic. “I had to go into hospital early, and by that time I was drinking 24/7 – mainly beer, a few cans a day, not massive binges. But nobody mentioned the drink: not the doctors, not the midwives. They didn’t advise about the risk of FAS. I had no suspicion that my child could be affected.”
Her second son was born a few weeks prematurely. Neither child had any of the physical features of FAS, and both went to mainstream schools, but their behaviour was very challenging. Gradually, as her life became more stable and she stopped drinking, Laura began to be aware that both her sons had serious issues.
Her younger son had learning difficulties and was diagnosed with ADHD. She had taken him to a hospital appointment and was carrying his notes from one doctor to another, when she spotted a note on his file that said: “Possible FAS.”
“I was devastated,” Laura says. “I knew in my gut that’s what it was.” Both children were later given a formal diagnosis at Great Ormond Street hospital.
Laura is dynamic and energetic; she has a good job now, as she did when she was first pregnant. We meet in a cafe near Hampstead Heath in London, at teatime, and it soon becomes obvious from the discreet twitching of other customers’ heads that her calm, powerful account of this rarely discussed subject has them all engrossed.
She knows people will blame her for her actions, and is very conscious of her own responsibility for her sons’ difficulties, but she is adamant that mothers need support, not criminalisation. “There is sometimes a witch-hunt to go after the mothers, but I am living with my guilt every day. That’s a real life sentence.” She has coped by devoting herself to making sure her sons get all the support they need, and by volunteering to help other mothers who also drank during pregnancy, through the European Birth Mother Network.
“I need to make sure this doesn’t happen to other people,” Laura says. “Women shouldn’t be prosecuted – they should be given alcohol-rehabilitation services. No woman I have ever met ever wants to harm her baby. This is an illness, not a choice. But people need to be told if they do drink, what will happen. There aren’t enough clear guidelines. I think midwives are scared sometimes to confront women.”
Although Laura drank more during her second pregnancy, she thinks her older child has struggled more with the consequences of his condition. “My younger son got support earlier. For the older one, it was harder – we didn’t understand, so he was always being told, ‘You are awful – why do you behave like that?’ He had an organic brain injury; he couldn’t read people’s facial expressions, he had problems with social skills, he was overwhelmed by noise. We didn’t understand that.”
“There is a witch-hunt to go after the mothers, but I am living with my guilt every day. That’s a real life sentence”
Twenty years on from Laura’s pregnancy, the medical guidance is still confusing and contradictory. There are those, such as paediatrician and former children’s commissioner Sir Al Aynsley-Green, who argue for total abstinence. “Exposure to alcohol before birth is the most important preventable cause of brain damage in children, that could affect up to one in every 100 babies in England,” he says. “Its effects range from devastating physical and learning disabilities to subtle damage causing bad behaviour, violence and criminality.”
At the other end of the spectrum are groups such as the British Pregnancy Advisory Service, who point out that most women are already very sensible and warn against demonising their behaviour. According to BPAS, the main consequence of publishing excessively frightening advice is that women come to its clinics unnecessarily considering abortions, concerned about damage they might have inflicted on their foetus before they knew they were pregnant.
In the submission made by BPAS to the court case last year, it was pointed out that there are a wide variety of substances that may cause damage to an unborn baby, from food to plastics and household products. Lawyers in the case questioned whether demanding criminal injuries compensation for alcohol poisoning could mean by extension that “a pregnant mother who eats unpasteurised cheese or a soft-boiled egg, knowing that there is a risk of harm to the foetus might also find herself accused of a crime”.
At the frontline, Jo Austin, a midwife who works with vulnerable mothers in London, says it’s easier to get women to talk about heroin or crack addiction than it is to get them to confront their drinking during pregnancy. “We have lots of leaflets for women who take heroin and crack, who are quite a small minority of the women we see. But alcohol is more socially acceptable and it is legal. A large proportion of society drinks, at least socially. Our feeling is that it is a problem that women don’t admit to, perhaps because of stigma, guilt or fear of social services involvement.”
Austin says most of the pregnant women she sees are better informed about the risks of smoking during pregnancy. “There has been so much health promotion done on smoking, but the effects of alcohol are potentially much worse.”
Gail Priddey, CEO of Haringey Advisory Group on Alcohol, which supports families affected by alcohol, says she is currently writing an advice leaflet for midwives that attempts to navigate a line between being straightforward with the facts without “scaring pregnant women witless”. “It is such an emotive and difficult subject,” Priddey says. “You say, ‘Best not to drink when you’re pregnant,’ then someone says, ‘Well, actually, I’ve been drinking heavily. I didn’t realise.’ Where do you go from there? Do you say, ‘You may have done some damage’? It’s an area professionals don’t want to touch.”
The flipside of this is that children with FAS and FASD are not diagnosed early enough, and often do not receive the help they need. Raja Mukherjee, a neurodevelopmental psychiatrist and lead clinician at the national FASD clinic, says awareness of the condition has risen dramatically in the 12 years he has worked in the area, but diagnosis remains complicated. He believes doctors are often unwilling to label a child as suffering from FASD because it is “too stigmatising”. “It is easier to say, ‘You have ADHD,’” he says.
Yet Mukherjee is uncomfortable about the fight for criminal injuries compensation for children, because “criminalisation just pushes it underground. We struggle already with people who tell us, ‘I didn’t drink at all in pregnancy’ – yet they were an alcoholic before and an alcoholic afterwards.”
Neil Sugarman, the lawyer for the unidentified local authority in the north-west that took the legal action, said they were motivated by a quest to get adequate funding for the girl’s care. “This wasn’t about trying to get women prosecuted,” he says. “My job as a lawyer is to look at the interests of terribly badly impaired children. We have a state scheme that if you can show you are a victim of a crime, you are entitled to compensation.
“The Criminal Injuries Compensation Scheme has never required someone to be prosecuted – no one needs to be taken to court, charged, sentenced or convicted. All it requires is that a judge has to be satisfied that what happened can be recognised as a crime. It is very difficult for young people to get access to their therapeutic needs on the NHS – the occupational therapy and speech therapy they need is not always readily available. The true benefit of compensation would be to open up access to private treatment for these children and enhance their lives.”
I didn’t know the kids’ mother was an alcoholic. She loved them, but couldn’t cope. It didn’t put me off adopting them
Kay Collins adopted three children, two of whom have foetal alcohol spectrum disorder. Photograph: Sophia Spring for the Guardian
Kay Collins, 61, would also like to see more funding for children with FASD, but not if it means prosecuting their mothers. Ten years ago, she adopted three children, two of whom have the condition. She knew them before she adopted them, because they lived in a flat upstairs in the west London mansion block where they still live.
“We’d meet on the stairs and say hello, and I got to know them – they were lovely kids. I didn’t know their mother was an alcoholic. It was only as time went on, I realised. She was somebody who needed help, not someone to abuse or to judge.
“You saw that she loved the kids, but she couldn’t manage. She was in her 20s, the children’s father was there on and off. She never harmed the kids in any way. She loved them – she just didn’t know how to care for them.”
Eventually, the children were taken into care. Collins, who was working as a teaching assistant and had four, much older children of her own, decided to adopt them – a girl of 17 months and boys of four and five. She knew nothing about FASD until she was called by a paediatrician who was helping to prepare the adoption papers. She was told the two younger children might have learning disabilities and was asked how she would cope. “I said, ‘If I knew that now, I would be a genius. I can only know when I am dealing with it.’ It didn’t put me off. I knew that the children just needed a lot of love and attention.”
Now that she knows more about the condition, she can see some of the facial characteristics of FASD in pictures of the youngest as a baby. These have become less noticeable as she has grown up, but her cognitive problems have become more evident over time. “When they were about seven, it was clear things were not happening as with normal children. They both didn’t speak very well for a long time, they didn’t understand a lot of things. The younger one still doesn’t. Her brother understands better, but his behaviour is worse. If you try to correct him, he gets very angry.”
Collins is fighting for the youngest, now 12, to be given a place in a special needs school. “She has language difficulties. If things are not explained to her at a slower pace, she is not going to understand them. At the moment, I’m at loggerheads with the local authority and in a tribunal because they don’t think that’s necessary. They don’t want to pay for it. It’s down to cost.”
Collins thinks her 12-year-old daughter won’t take GCSEs and knows that, long-term, life will be complicated for her. “She will live independently, but she will need a lot of support – she is quite vulnerable because she thinks everyone is her friend.” But she doesn’t like the idea of fighting for compensation through the Criminal Injuries Compensation Scheme. “It would be nice to have the money; we could use it to get them educated in the right environment,” she says, but she is uncomfortable with the idea that this might be a step in the direction of criminalising troubled women. “Mothers who drink when pregnant need more support and understanding. No one sits down and just starts drinking. There has to be something that triggered it.”
Meanwhile, she just tries to help her children understand. “My daughter keeps asking, ‘Is there something wrong with me?’ I say, ‘Yes, you have foetal alcohol spectrum disorder.’” The middle child is angry about his mother’s role in his condition. “He says, ‘I hate my mum’, but I try to explain: ‘She couldn’t look after you. It doesn’t mean she didn’t love you. She was never a bad mum.’”
• Some names have been changed. To contact Nofas UK, call 020-8458 5951 or go to nofas-uk.org.
Source: http://gu.com/p/475mq April 2015 http://www.theguardian.com/society/2015/apr/04
Roll Call Video Advises Law Enforcement to Exercise Extreme Caution
DEA has released a Roll Call video to all law enforcement nationwide about the dangers of improperly handling fentanyl and its deadly consequences. Acting Deputy Administrator Jack Riley and two local police detectives from New Jersey appear on the video to urge any law enforcement personnel who come in contact with fentanyl or fentanyl compounds to take the drugs directly to a lab.
“Fentanyl can kill you,” Riley said. “Fentanyl is being sold as heroin in virtually every corner of our country. It’s produced clandestinely in Mexico, and (also) comes directly from China. It is 40 to 50 times stronger than street-level heroin. A very small amount ingested, or absorbed through your skin, can kill you.”
Two Atlantic County, NJ detectives were recently exposed to a very small amount of fentanyl, and appeared on the video.
Said one detective: “I thought that was it. I thought I was dying. It felt like my body was shutting down.”
Riley also admonished police to skip testing on the scene, and encouraged them to also remember potential harm to police canines during the course of duties.
“Don’t field test it in your car, or on the street, or take if back to the office. Transport it directly to a laboratory, where it can be safely handled and tested.”
The video can be accessed at: http://go.usa.gov/chBWW
More on Fentanyl:
On March 18, 2015, DEA issued a nationwide alert on fentanyl as a threat to health and public safety.
Fentanyl is a dangerous, powerful Schedule II narcotic responsible for an epidemic of overdose deaths within the United States. During the last two years, the distribution of clandestinely manufactured fentanyl has been linked to an unprecedented outbreak of thousands of overdoses and deaths. The overdoses are occurring at an alarming rate and are the basis for this officer safety alert.
Fentanyl, up to 50 times more potent than heroin, is extremely dangerous to law enforcement and anyone else who may come into contact with it. As a result, it represents an unusual hazard for law enforcement.
Fentanyl, a synthetic opiate painkiller, is being mixed with heroin to increase its potency, but dealers and buyers may not know exactly what they are selling or ingesting. Many users underestimate the potency of fentanyl.
The dosage of fentanyl is a microgram, one millionth of a gram – similar to just a few granules of table salt. Fentanyl can be lethal and is deadly at very low doses.
Fentanyl and its analogues come in several forms including powder, blotter paper, tablets, and spray.
Risks to Law Enforcement
Fentanyl is not only dangerous for the drug’s users, but for law enforcement, public health workers and first responders who could unknowingly come into contact with it in
its different forms. Fentanyl can be absorbed through the skin or accidental inhalation of airborne powder can also occur. DEA is concerned about law enforcement coming in contact with fentanyl on the streets during the course of enforcement, such as a buy-walk, or buy-bust operation.
Just touching fentanyl or accidentally inhaling the substance during enforcement activity or field testing the substance can result in absorption through the skin and that is one of the biggest dangers with fentanyl. The onset of adverse health effects, such as disorientation, coughing, sedation, respiratory distress or cardiac arrest is very rapid and profound, usually occurring within minutes of exposure.
Canine units are particularly at risk of immediate death from inhaling fentanyl.
In August 2015, law enforcement officers in New Jersey doing a narcotics field test on a substance that later turned out to be a mix of heroin, cocaine and fentanyl, were exposed to the mixture and experienced dizziness, shortness of breath and respiratory problems.
If inhaled, move to fresh air, if ingested, wash out mouth with water provided the person is conscious and seek immediate medical attention.
Narcan (Naloxone), an overdose-reversing drug, is an antidote for opiate overdose and may be administered intravenously, intramuscularly, or subcutaneously. Immediately administering Narcan can reverse an accidental overdose of fentanyl exposure to officers. Continue to administer multiple doses of Narcan until the exposed person or overdose victim responds favorably.
Field Testing / Safety Precautions
Law enforcement officers should be aware that fentanyl and its compounds resemble powered cocaine or heroin, however, should not be treated as such.
If at all possible do not take samples if fentanyl is suspected. Taking samples or opening a package could stir up the powder. If you must take a sample, use gloves (no bare skin contact) and a dust mask or air purifying respirator (APR) if handling a sample, or a self-contained breathing apparatus (SCBA) for a suspected lab.
If you have reason to believe an exhibit contains fentanyl, it is prudent to not field test it. Submit the material directly to the laboratory for analysis and clearly indicate on the submission paperwork that the item is suspected of containing fentanyl. This will alert laboratory personnel to take the necessary safety precautions during the handling, processing, analysis, and storage of the evidence. Officers should be aware that while unadulterated fentanyl may resemble cocaine or heroin powder, it can be mixed with other substances which can alter its appearance. As such, officers should be aware that fentanyl may be smuggled, transported, and/or used as part of a mixture.
Universal precautions must be applied when conducting field testing on drugs that are not suspected of containing fentanyl. Despite color and appearance, you can never be certain what you are testing. In general, field testing of drugs should be conducted as appropriate, in a well ventilated area according to commercial test kit instructions and training received. Sampling of evidence should be performed very carefully to avoid spillage and release of powder into the air. At a minimum, gloves should be worn and the use of masks is recommended. After conducting the test, hands should be washed with copious amounts of soap and water. Never attempt to identify a substance by taste or odor.
Historically, this is not the first time fentanyl has posed such a threat to public health and safety. Between 2005 and 2007, over 1,000 U.S. deaths were attributed to fentanyl – many of which occurred in Chicago, Detroit, and Philadelphia.
The current outbreak involves not just fentanyl, but also fentanyl compounds. The current outbreak, resulting in thousands of deaths, is wider geographically and involves a wide array of individuals including new and experiences abusers.
In the last three years, DEA has seen a significant resurgence in fentanyl-related seizures. In addition, DEA has identified at least 15 other deadly, fentanyl-related compounds. Some fentanyl cases have been significant, particularly in the northeast and in California, including one 12 kilogram seizure. During May 2016, a traffic stop in the greater Atlanta, GA area resulted in the seizure of 40 kilograms of fentanyl – initially believed to be bricks of cocaine – wrapped into blocks hidden in buckets and immersed in a thick fluid. The fentanyl from these seizures originated from Mexican drug trafficking organizations.
Recent seizures of counterfeit or look-a-like hydrocodone or oxycodone tablets have occurred, wherein the tablets actually contain fentanyl. These fentanyl tablets are marked to mimic the authentic narcotic prescription medications and have led to multiple overdoses and deaths.
According to DEA’s National Forensic Lab Information System, 13,002 forensic exhibits of fentanyl were tested by labs nationwide in 2015, up 65 percent from the 2014 number of 7,864. The 2015 number is also about 8 times as many fentanyl exhibits than in 2006, when a single lab in Mexico caused a temporary spike in U.S. fentanyl availability. This is an unprecedented threat
Source: U.S. Drug Enforcement Administration dea@public.govdelivery.com 11th June 2016
April 20, 2015
For Immediate Release
For More Information Contact: Lana Beck (727) 828-0211 or (727) 403-7571
Weeds 3: A Documentary Showcasing Legitimate Scientific Research or an Infomercial to Legalize Marijuana?
(St. Petersburg, FL) Drug Free America Foundation stands with other major medical associations whose positions support the research into the medical efficacy of marijuana. These associations include: the American Medical Association, American Society of Addiction Medicine, American Academy of Pediatrics and the American Psychiatric Association. However, Dr. Sanjay Gupta’s documentary blurs the lines between legitimate research and propaganda. The important take-a-way from the show was that research on the potential benefits of marijuana is taking place today without the rescheduling of the drug. Unfortunately, the show failed to point out the multitude of harms of marijuana use and the impacts in states that have determined medicine by popular vote.
“Two things about the documentary that really upset me as a medical professional are that Sanjay Gupta had a chance to drive home the point that because research is underway on the potential benefits of components in marijuana, there is no need to legalize it through referenda where dosages can’t be controlled and various strains can’t be cloned. Nor is it necessary to reschedule the drug,” said Dr. Eric Voth, an expert on drug policy and Chair of the Institute on Global Drug Policy.
“The other disappointing aspect about this show is the lack of discussion about the myriad of scientific research out there that shows the other side of marijuana that is harmful and addictive,” continued Voth. “If we are going to have open dialogue about marijuana research, then Gupta shouldn’t muddy the water by sending an incomplete message to the public about the right and the wrong way to approach true scientific research. I think this was an intentionally missed opportunity by Gupta to further a less-than-scientific agenda,” concluded Voth.
“By ignoring the potential harms of marijuana use and not acknowledging the big problems that Colorado and California have experienced since marijuana has been legalized in those states, CNN and Dr. Gupta failed to cover this issue honestly,” said Amy Ronshausen, Deputy Director of Drug Free America Foundation, Inc. and Save Our Society From Drugs. “This show failed to cover Colorado’s increases in drugged driving fatalities and emergency room visits because of marijuana use. Nor did the show discuss the alarming trend surrounding high potency marijuana edibles sold as ‘medicine’ and marketed to be appealing to youth,” continued Ronshausen. “There was a lot of discussion about how marijuana may help PTSD symptoms, but none about the mounting research on how the drug exacerbates psychotic symptoms,” concluded Ronshausen.
Source: Press Release DFAF 20th April 2015
The impact that so-called medical marijuana and later the legalisation of marijuana in Colorado, USA has had serious consequences, a few are show in snippets below. The items shown are taken from the Rocky Mountain High Intensity Drug Trafficking Area Report. The complete report can be found at:
http://www.rmhidta.org/default.aspx/MenuItemID/687/MenuGroup/RMHIDTAHome.htm.
The Legalization of Marijuana in Colorado: The Impact Vol. 3 Preview 2015
Medical Marijuana Registry Identification Cards
December 31, 2009 – 41,039
December 31, 2010 – 116,198
December 31, 2011 – 82,089
December 31, 2012 – 108,526
December 31, 2013 – 110,979
December 31, 2014 – 115,467
Colorado:
505 medical marijuana centers (“dispensaries”)1
322 recreational marijuana stores1
405 Starbucks coffee shops2
227 McDonalds restaurants3
Denver:
198 licensed medical marijuana centers (“dispensaries”)1
117 pharmacies (as of February 12, 2015

Findings
There has been an upward trend of marijuana-related emergency room visits and hospitalizations since medical marijuana was commercialized in 2009.
There has also been a significant increase in both categories in the first six months of 2014 when retail marijuana businesses began operating

It is important to note that, for purposes of the debate on legalizing marijuana in Colorado, there are three distinct timeframes to consider. Those are:
The early medical marijuana era (2000 – 2008), the medical marijuana commercialization era (2009 – current) and the recreational marijuana era (2013 – current).
2000 – 2008: In November 2000, Colorado voters passed Amendment 20 which permitted a qualifying patient and/or caregiver of a patient to possess up to 2 ounces of marijuana and grow 6 marijuana plants for medical purposes. During that time there were between 1,000 and 4,800 medical marijuana cardholders and no known dispensaries operating in the state.
2009 – Current: Beginning in 2009 due to a number of events, marijuana became de facto legalized through the commercialization of the medical marijuana industry. By the end of 2012, there were over 100,000 medical marijuana cardholders and 500 licensed dispensaries operating in Colorado. There were also licensed cultivation operations and edible manufacturers.
2013 – Current: In November 2012, Colorado voters passed Constitutional Amendment 64 which legalized marijuana for recreational purposes for anyone over the age of 21. The amendment also allowed for licensed marijuana retail stores, cultivation operations and edible manufacturers.

Findings
Youth (ages 12 to 17 years) Past Month Marijuana Use,
2013 o National average for youth was 7.15 percent
o Colorado average for youth was 11.16 percent
Colorado was ranked 3rd in the nation for current marijuana use among youth (56.08 percent higher than the national average)
In 2006, Colorado ranked 14th in the nation for current marijuana use among youth
In just one year when Colorado legalized marijuana (2013), past month marijuana use among those ages 12 to 17 years increased 6.6 percent.

June 6th. 2015
Dear Jessica McDonald
President and CEO BC Hydro:
I am writing to bring to your attention the fact that there are 93+ illegal marijuana dispensaries operating in the City of Vancouver. If your company is supplying these illegal businesses with hydro power you should seriously consider seeking advice from your legal counsel for being in conflict with the drug laws of Canada and laws pertaining to and potential penalties for facilitating criminal enterprises.
You will find it of benefit to review several court cases that have been filed by plaintiffs in the State of Colorado. These pleadings advance claims for damages from parties who are engaged in aiding and abetting marijuana businesses operating in violation of federal law. The Canadian Federal Government has verified, and made well publicized public statements that the marijuana dispensaries in Vancouver are illegal enterprises. BC Hydro customers should not be known illegal operations.
In Parksville BC, the RCMP closed down a marijuana dispensary and issued a warning to the landlord that if they rent to the company or a company conducting illegal business they could face charges under the provisions of Canadian law that prohibit any business from profiting from crime.
It is the position of Smart Approaches to Marijuana Canada – a national organization with representation from the medical and legal sectors, that these illegal businesses should be closed and federal drug laws be respected, adhered to.
We ask BC Hydro to comply with Canadian Federal Drugs Laws. We ask that BC Hydro disconnect all hydro service to these illegal businesses immediately and a public statement be made of this action. We respectfully also request that a letter be sent to the Mayor and Council, and the Federal Minister of Health Rona Ambrose that clearly states your actions on this matter.
Pamela McColl
Member of the Advisory Council of Smart Approaches to Marijuana Canada
Smart Approaches to Marijuana Canada (SAMC) Mission:
The mission of Smart Approaches to Marijuana Canada (SAMC) is to promote a health-first approach to marijuana policy that neither legalizes marijuana, nor demonizes its users. SAMC’s commonsense, third-way approach to marijuana policy is based on reputable science and sound principles of public health and safety. At SAMC we reject dichotomies — such as “incarceration versus legalization” — that offer only simplistic solutions to the highly complex problems stemming from marijuana use. Our aim is to champion smart policies that decrease marijuana use, like prevention and early intervention. Yet in rejecting legalization, we also do not believe that low-level marijuana users should be saddled with criminal records that stigmatize them for life.
SAMC’s Vision is to:
SAMC Will Advocate For:
SAMC’s Actions Will Consist Of:
conducting information briefings for the public and decision makers about the science of today’s marijuana and the evidence of effectiveness for different law makers;
Marijuana and Public Health:
People often refer to their own experiences with marijuana, rather than to what science has taught us. No matter what people think about the drug and the policies surrounding it, it is vitally important to be well-versed in the science and public health and safety impacts of marijuana use and addiction:
Marijuana and the Criminal Justice System
Statistics show that very few people are actually in prison for simple marijuana-only possession. Majority of offenders in Canada who are sentenced to prison have a prior criminal history or are found in possession of marijuana while committing other serious offences such as impaired driving or domestic violence. For instance, in 2011 in British Columbia, only 3% of founded cases of marijuana possession were cleared by a charge. And of that 3%, only seven cases (1.3% of the 3%) resulted in a custody sentence.[5]
Marijuana and Big Business
Tobacco companies lied to Canada for more than a century about the dangers of smoking. They deliberately targeted kids and had doctors promote cigarettes as medicine. And today we are paying the price. Tobacco use is our nation’s top cause of preventable death and contributes to about 37,000 deaths each year. Tobacco use costs our country at least $17 billion annually — which is about 3 times the amount of money our state and federal governments collect from today’s taxes on cigarettes and other tobacco products. If it is legalized, marijuana will be commercialized just as tobacco was. The examples of tobacco and alcohol should teach us that legalizing any third substance would be a public health disaster.
Hall W & Degenhard L. (2009). Adverse health effects of non-medical cannabis use. Lancet, 374.
Andréasson S, et al. (1987). Cannabis and Schizophrenia: A longitudinal study of Swedish conscripts. Lancet, 2(8574).
Meier, M.H. (2012). Persistent cannabis users show neuropsychological decline from childhood to midlife. Proceedings of the National Academy of Sciences.
Pauls, K., et al. (2013). The nature and extent of marijuana possession in British Columbia. University of Fraser Valley Center for Public Safety and Criminal Justice Research.
Source: www.learnabout.ca June 2015
[1] Wagner, F.A. & Anthony, J.C. (2002). From first drug use to drug dependence; developmental periods of risk for dependence upon cannabis, cocaine, and alcohol. Neuropsychopharmacology 26.
[2] Hall W & Degenhard L. (2009). Adverse health effects of non-medical cannabis use. Lancet, 374.
[3] Andréasson S, et al. (1987). Cannabis and Schizophrenia: A longitudinal study of Swedish conscripts. Lancet, 2(8574).
[4] Meier, M.H. (2012). Persistent cannabis users show neuropsychological decline from childhood to midlife. Proceedings of the National Academy of Sciences.
[5] Pauls, K., et al. (2013). The nature and extent of marijuana possession in British Columbia. University of Fraser Valley Center for Public Safety and Criminal Justice Research.
Dakof G.A., Cohen J.B., Henderson C.E. et al.
Journal of Substance Abuse Treatment: 2010, 38, p. 263–274..
US researchers may have found a better way to support mothers at risk of losing custody of their children so they engage in and benefit from substance use treatment and meet family court requirements, meaning more children can safely stay with their parents.
SUMMARY The family environment of the children of problem substance users is often compromised by instability, neglect, and poor parenting. Improving parental functioning – especially reducing substance use – makes children safer and improves child welfare outcomes. However, substance use treatment completion rates among parents who come into contact with the child welfare system are low. For solutions to these problems, many communities have turned to family drug courts. Adapted from the adult drug court model, family drug courts were established to enhance the effectiveness of child welfare agencies by increasing enrolment and retention in substance use treatment, motivating parents to address their addiction, and coordinating the many services needed to stabilise families. Unlike typical drug courts, these courts do not operate in the criminal justice system, most participants are women, and the court addresses the dual issues of parental addiction/recovery and child safety and custody. Most family drug courts employ court counsellors who refer clients to substance use treatment and other services, develop a recovery plan, and monitor and report clients’ ongoing progress to the court.
Key points
Family drug courts aim to enhance the effectiveness of child welfare agencies by promoting engagement in substance use treatment, motivating parents to address their addiction, and coordinating the services needed to stabilise families.
To further promote treatment engagement and family court compliance of mothers facing loss of custody of their children, a programme was developed for court counsellors which involved the mother’s family and other significant figures in their lives.
Compared to a more typical case management role, the tested programme led to more mothers retaining their parental rights and greater improvements in substance use, health, family functioning, and risk of child abuse.
However, samples were small and by the end of the study several of the differences between the two sets of mothers were also small.
The Engaging Moms Program – the focus of this study – is a family-oriented intervention shown to have succeeded in its objectives of facilitating treatment entry and short-term retention among mothers of infants who have been exposed to parental substance use. It was then adapted for use in a family drug court context and (relative to usual case management services) found in a non-randomised trial to improve completion of the drug court programme (72% versus 38%) and the proportion of mothers reunited with their children (70% versus 40%). Although the results were encouraging, this study had several limitations, leading to the current randomised trial comparing in a family drug court context the effectiveness of the Engaging Moms Program versus intensive case management of the kind recommended for such courts.
During the recruitment period of the trial, 62 of the 69 mothers who attended a family drug court in Miami in the USA agreed to join the study. They averaged 30 years of age, were mainly black or Hispanic, poor, unemployed and poorly educated. Just 1 in 10 were married. As children, many had been victims of physical and sexual abuse and most currently suffered serious mental health problems. They used a mixture of drugs including alcohol and cocaine and averaged about three lifetime arrests.
Mothers in the study were subject to the usual 12–15 month regimen of court hearings, supervision and support. Additionally, court counsellors were specially trained and supervised to deliver one of the programmes being compared as alternative ways to engage and retain these mothers in substance treatment and improve child and parental outcomes. The 62 women were randomly selected such that equal numbers were allocated to the Engaging Moms option or the comparator.
Neither option was a treatment in its own right, but sought to promote treatment entry, retention and benefit, as well as satisfactory completion of the drug court programme. Intensive case management counsellors aimed to develop a strong therapeutic relationship with the mother, assess her needs, plan support, link her to services, monitor progress, and advocate on her behalf. In contrast, the Engaging Moms Program (based on multidimensional family therapy) engaged not just with the mother and with services but with the mother’s social network, especially her family. For example, in stage two of the programme focused on changing behaviour, counsellors conducted individual and joint sessions with the mother and her family and or partner. These dealt with: the mother’s motivation and commitment to succeed in drug court and to change her life; the emotional attachment between the mother and her children; her relationships with her family of origin; her parenting skills; her romantic relationships; and emotional regulation, problem solving, and communication skills. Considerable attention was devoted to repairing the mother’s relationship with her family, often damaged by hurts, betrayals, and resentments. Also the counsellor facilitated the mother’s relationship with court personnel and service providers and helped prepare her for court appearances, during which they advocated for the mother.
Regardless of the approach to which they had been allocated, during the trial mothers saw their counsellors for on average about 40 hours, but the Engaging Moms Program included seven hours of family sessions versus just under four in the case management option.
Research workers assessed the mothers several times up to 18 months following drug court intake (97% of assessments were completed), when information on child welfare status was extracted from court records. This primary outcome was defined as positive if the mother retained her parental rights, either having sole or joint custody of the children, or when the children were under the guardianship of a relative. Other outcomes considered not to be positive involved termination of the mother’s parental rights and the child being placed with a relative or in foster care.
The small number of mothers in this pilot study limited the chances of statistically significant findings, so the focus instead was on whether the differences between outcomes from the Engaging Moms Program and case management were large enough that with a bigger sample they might have proved statistically significant.
Main findings
Of the 31 Engaging Moms mothers, 24 had retained their parental rights compared to 17 of the 31 case management mothers, an advantage for Engaging Moms which narrowly missed the conventional criterion for statistical significance. These figures included 16 Engaging Moms mothers who had sole custody of their child compared to 12 allocated to case management. Over twice as many case management mothers had their children removed to foster care – 9 versus 4. Two-thirds of Engaging Moms mothers satisfactorily completed the drug court programme compared to about half the case management mothers.
Over the first three months both sets of mothers significantly improved in terms of their substance use, mental and physical health, family functioning, risk posed to child, and employment, improvements maintained or augmented through the remainder of the 18-month follow-up. In no case were these improvements significantly greater among Engaging Moms mothers, but several outcomes substantially favoured these mothers. They were more likely to further reduce their drinking, experience greater improvements in mental and physical health and family functioning, and more steeply decreased their risk of child abuse. At the three-month follow-up, on all three relationship dimensions they also reported significantly stronger therapeutic relationships with their counsellors.
The authors’ conclusions
The Engaging Moms Program delivered in the context of a family drug court increased the likelihood of positive outcomes for mothers (retention of parental rights and improved welfare and functioning) in comparison to intensive case management. In all domains of functioning, families assigned to Engaging Moms showed improvement that was equal to or better than families assigned to case management. Arguably the primary mechanisms leading to better results were a stronger therapeutic alliance with the counsellor and more extensive family involvement.
Although the results of this pilot study are encouraging, there are important limitations. The primary one is that a small sample size limits the scope for testing differences between outcomes in the two sets of mothers and weakens the reliability of the results; different results might be obtained with larger samples.
COMMENTARY Commending the Engaging Moms Program is its apparent non-punitive humanity and the plausibility of its strategy of repairing what may have been a damaging social network and engaging it in supporting the mother, promising not just the short-term gains which the study was able to document, but a more stable, long-term future for mother and child. Particularly encouraging is the non-diminution of the gains and sometimes their augmentation over the period after the interventions ended. As well as benefiting the families involved, long-term reduction in social costs can be expected. With family drug and alcohol courts spreading in the UK, the Engaging Moms model might be adapted to further improve their outcomes for parent and child.
However, convincingly demonstrating the advantages of the approach for maternal and child welfare is a difficult task when so much else is going on in the mothers’ lives, when the basic family drug court programme is the same for both intervention and comparison mothers, and when the comparator is itself seemingly a humane and well structured approach. Details below.
As the authors observed, if replicated with a larger sample, the difference in the retention of parental rights, and probably too in resort to foster care, would have been statistically significant, but also a larger sample may show these to have been unreliable findings. On the other measures of maternal welfare and family functioning and safety, though there were substantial extra improvements among the Engaging Moms group, in some cases this mainly reflected a drop from an initially higher level of severity. By the end of the study the differences in absolute terms between the two sets of mothers were generally very small. Several of the researchers were involved in developing the programme they evaluated, raising the possibility of their somehow favouring the programme, a risk endemic in substance use research. Also it has to be acknowledged that termination of a mother’s parental rights and placement of the child elsewhere is not necessarily a negative outcome from the point of view of the child’s long-term welfare. On this issue we can only rely on the professionalism and child-centredness of the Engaging Moms counsellors, and on the presumption that if there had been over-enthusiastic advocacy, the court would not have been unduly swayed.
UK research and practice
The first family drug and alcohol court in Britain was piloted at an inner London family court initially for three years to the end of 2010. Researchers concluded that more parents seen by these specialist courts than by comparison courts had controlled their substance misuse by the end of proceedings and been reunited with their children. They were also engaged in more substance misuse services over a longer period. Evidence of cost savings were noted in relation to court hearings, out-of-home placements, and fewer contested proceedings. Parents and staff felt this was a better approach than ordinary care proceedings. A later report from the same study with a longer follow-up of more families reinforced the earlier findings. More family drug and alcohol court parents had stopped misusing substances and dealt with other problems, and more mothers had been reunited with their children, but this 36% v 24% gap was not statistically significant.
The main weakness of this UK study is that in some known respects and perhaps in others not known, the comparison families differed from the family drug court families in ways which might have affected child welfare outcomes, regardless of the type of court proceedings. Also, through a preceding feasibility study the researchers had been involved in developing the programme they evaluated. As with the featured study, this raises the possibility of their somehow favouring the new intervention they helped to create.
Three NHS professionals who helped develop the first court in London have explained that it differs from normal family courts in its multi-disciplinary assessment and intervention team made up of both child workers (child protection social workers and a child and adolescent psychiatrist) and adult workers (substance misuse workers and an adult psychiatrist), plus volunteers with personal experience of overcoming substance misuse, some of whom are court ‘graduates’. Court proceedings form an integral part of the treatment process. The family works with the same judge throughout and compared to normal courts, the court takes a less adversarial approach to care proceedings, the parent speaking directly to the judge in the absence of lawyers.
Similar courts have now opened in Gloucestershire and Milton Keynes and as reported in 2015, more were due to open in 2015/16 in areas including East Sussex, Kent and Medway, Plymouth, Torbay and Exeter, and West Yorkshire, funded by the Department for Education. Despite this significant expansion, as in London, these courts will sit once a week and hear relatively few cases.
Large-scale US evaluation
From the USA the first large-scale outcome study of a family drug court compared the progress (as revealed by court and administrative records) of mothers and children processed through three such courts with those processed through normal channels either in the same areas or in similar areas without a family drug court. An attempt was made to statistically even out relevant differences between the two sets of families. Findings favoured the family drug courts. Mothers processed through these courts were more likely to be unified with their children, who spent less time in out-of-home placements. More drug court mothers entered substance use treatment and they did so more rapidly, stayed longer and were more likely to complete the programme. However, the relative benefits arising from the family drug courts were at best a minor influence on child custody outcomes, and the study could not be sure that all relevant differences between the two sets of families had been accounted for.
An Effectiveness Bank hot topic has explored the issues involved in protecting children and offers one-click access to all Findings analyses relevant to child protection.
Source: A randomized pilot study of the Engaging Moms Program for family drug court http://findings.org.uk/PHP/dl.php?file=Dakof_GA_2.txt Last revised 28 May 2015. First uploaded 20 May 2015
A recent example of the logical abandon of today’s backers of legal marijuana is the plan to defund the Drug Enforcement Administration’s program to eradicate illegal marijuana (DEA/CESP), an $18 million program that eliminates millions of plants a year and arrests thousands of criminals, many of whom were brought here to labor for Mexican drug cartels controlling the marijuana black market.
Yet Congressman Ted Lieu (D-CA) wants to end the effort as a “ridiculous waste” of federal resources, when multiple states “have already legalized marijuana,” use of which should “no longer be a federal crime.” Clearly, the congressman has not thought this through. He is, in fact, arguing against his own legal marijuana case.
A central tenet of the legalization movement is that criminal marijuana was to be supplanted by “safe, regulated and taxed” marijuana under careful control. It is a contradiction of that principle to foster, by cutting the DEA program, the proliferation of unregulated, untaxed and “unsafe” marijuana plants controlled by violent criminals, thereby corrupting the entire point of a “legalized” marijuana market.
While a “regulated and taxed market” was the position sold to legislators, the real objective seems to be a dope-growing paradise, unregulated and unopposed. Congressman Lieu doesn’t even try to explain how this is supposed to advance America’s well-being.
For years now, Americans have been subjected to efforts by advocates for legalized marijuana to make their case. Today, the arguments often come from legalization lobbyists, often with legal or political training, seeking to legitimize what they hope will become a billion-dollar business in addictive toxins – repeat customers guaranteed.
Or consider the argument that marijuana is “safer to use” than alcohol. That alcohol is dangerous all acknowledge, costing the health of thousands. But the proper argument is that each intoxicant presents its own unique threats. It is not productive medically to “rank” them. But what is the logical implication of the alcohol talking point?
The regulation of alcohol is precisely the idealized model that lobbyists put forth for legal drugs. Hence, every time they insist that alcohol is the more damaging substance, what they are actually showing is that the model of legal, regulated sales of addictive substances produces widespread harm to adults and adolescents.
A major dimension of alcohol damage is the sheer prevalence of use, some six times greater than the prohibited marijuana, driving up the “disease burden.” Were regulated marijuana to reach the proportions of use of alcohol, the public health impact would be staggering.
One cannot argue simultaneously that marijuana should be treated like alcohol in order to reduce societal harm, and then reveal this model fails as policy, as witnessed by the ensuing alcohol damage (to be compounded by vastly expanded cannabis use). Once again, one suspects that the regulated alcohol model is but a stalking horse, useful to advance the cause, but not to be taken as serious policy.
Further, advocates claim that a legalized regime will better keep marijuana out of the hands of children. Yet a recent pediatric journal reported on the nearly 147 percent rise in emergency episodes for children from marijuana “edibles” nationwide.
Marijuana lobbyists counter that poisoning happens “in all states,” and therefore legalization in some states can’t be blamed. But in states with medical marijuana dispensaries, the rate increase was four times greater (610 percent) than in states without.
Repeatedly, when such facts are presented, they are ignored by the marijuana lobbyists.
In like fashion you hear “marijuana is medicine” (case not made by medical standards); that the criminal element will be eliminated (the black market cartels are thriving in Colorado); that legalization will not promote nationwide smuggling of high-potency dope (it’s rampant, even leading to interstate lawsuits); or that legal drugs will do more good than harm to America (What family is stronger or safer or healthier with drug use?).
If marijuana legalization were a good idea, the facts would support it, and the arguments of advocates wouldn’t be so lame.
Murray and Walters direct the Hudson Institute’s Center for Substance Abuse Policy Research. They both served in the Office of National Drug Control Policy during the George W. Bush administration.
Source: By David W. Murray & John P. Walters San Diego UT July 30, 2015

A currently hip cause is to rail against sentencing pot smokers to jail time. It sounds good considering alcohol is legal, smoking pot is not considered harmful to others, and our jails are already overcrowded, straining taxpayers’ wallets. The only problem is there isn’t a shred of truth to it.
Sadly, many on the right have fallen into this trap. Attend a Republicans for Liberty meeting and some young, charismatic leader will give an impassioned speech ranting and raving about how terrible it is that we lock up people for simply smoking pot. To a cheering audience, they declare it’s all about liberty and stopping big government from its unsuccessful war on drugs.
I was a prosecutor for several years, and the facts are quite different. Smoking pot has actually been “de facto” legalized across the U.S. The police look the other way, even if a neighbor rats on someone. There aren’t enough police officers to enforce marijuana possession laws. In fact, when states began legalizing pot for medicinal and recreational use, most pot smokers didn’t bother leaving their illegal dealers, because there is so little risk.
As a county prosecutor, I came across thousands of criminal cases (I frequently covered multiple hearings in different cases on a daily basis for other prosecutors assigned to those cases). I never saw a single defendant who was really sentenced to jail for marijuana possession. Former Los Angeles District Attorney Steve Cooley once said, “No first-time offender arrested in California solely for drug possession goes to prison — ever.”
Here is why there is confusion: the only time someone is sentenced to jail for smoking pot is if there is a more serious crime they are clearly guilty of, and the prosecutor or judge wants to give them a lighter sentence. Theft or burglary were the most common crimes I came across. Instead of being required to sentence a defendant to a year imprisonment for stealing, a defendant could plead guilty to marijuana possession instead and get a much lesser sentence. So on paper, it looks like they are serving time for drug possession, but in reality, they were let off the hook for a serious crime.
Police arrest individuals for other crimes and discover marijuana in the process — which can then, ironically, be used to the defendant’s advantage to get a lighter sentence! Additionally, no judge wants to go on record sentencing someone to jail for merely marijuana possession unless the defendant has a serious crime accompanying it.
This is only the tip of the iceberg. The vast majority of the defendants I came across had long rap sheets; pages and pages of criminal history. Much of it was not permitted to be disclosed to the judge, it was considered inadmissible; things like arrests with no conviction, dismissals, juvenile crimes, convictions older than the statute of limitations, etc. Many defendants had been arrested 10 to 20 times and it was clear they had a pattern of theft or other crimes — and generally caught with drugs every time — but the outcome was always the same, they were allowed to plead guilty to some lesser crime and often escape any jail time. It was eye-opening to see how many crimes a defendant had clearly committed based on their rap sheet, yet they would only end up getting sentenced for one of them.
Additionally, it has been found that the average criminal is only caught once for about every 12 crimes committed. FBI crime data from 2013 reveals that only 13.1 percent of burglary offenses are ever solved. Add that to the crimes criminals do get caught committing, but escape consequences due to a good defense attorney, technical error by the prosecution, or other factor, and it becomes pretty clear that these folks are actually getting pretty lucky pleading guilty to marijuana possession.
Harder drugs and pot dealers don’t fare quite as well. But as long as they stay away from other criminal activity, they too are frequently left alone by the law. When caught, prosecutors also let them plea down to a lesser crime.
The problem is no one has the guts to stand up to this myth, afraid of being called a big government, authoritarian conservative. It’s much easier to look hip and make vague statements like “The war on drugs is not working.” There is no longer a war on drugs. There is the occasional ad campaign to warn teenagers against using drugs — and usually just hard drugs — but even those are directed at youth, not your average adult pot smoker. No one cares and no one enforces the law, it is treated like illegal immigration with law enforcement and the legal system looking the other way.
Obama is calling to end mandatory minimum sentencing, claiming there are too many nonviolent offenders behind bars. Several prominent Republicans are jumping on the bandwagon with him. Last month, Obama commuted the sentences of 46 “nonviolent drug offenders.” Does anyone actually believe even one of them was really serving time for drug possession, much less marijuana possession? Only the prosecutor and defense attorney will ever see their entire rap sheet, and are prohibited by law from disclosing it, so Obama gets away with this ruse.
Conservatives and libertarians shouldn’t buy into this typical rhetoric from the left, which is to stand for something because it sounds good on the surface, when in reality the truth is much different. Regardless of one’s position on drug legalization, stop saying that people are serving time behind bars for marijuana possession. You just look silly.
Source: http://townhall.com/columnists/rachelalexander/2015/08/03/no-one-serves-jail-time-for-smoking-pot- August 3rd 2015

Let us provide a rational answer to a nonsensical question. It is a nonsensical question because blood is never impaired by THC. Never. Alcohol doesn’t impair blood either. These drugs only impair the brain, not the blood.
We can only test for drug content in the brain by means of an autopsy, something most drivers would reasonably object to.
We test blood as a surrogate for what’s in the brain. For alcohol, blood is a very good surrogate. Alcohol is a tiny, water-soluble molecule that rapidly crosses the blood-brain barrier and quickly establishes and maintains an equilibrium concentration between what’s in the blood and what’s in the brain.
Blood is a terrible surrogate for learning the amount of THC in the brain. It’s used because we blindly follow the precedence set by alcohol, perhaps even believing the pot lobby’s mantra that marijuana should be regulated like alcohol. It’s also used because we haven’t proven anything else that’s any better. Oral fluid likely is somewhat better, but that may only be because it can be collected more quickly at the roadside.
Blood is a terrible surrogate because unlike alcohol, THC is a very large fat-soluble molecule. This results in three major differences in behavior compared to alcohol:
Perhaps this explains why researchers agree that marijuana impairs driving, but none claim there is a good correlation between blood levels of THC and impairment.
The fact is that there is no level of THC above which, everyone is impaired, and below which, no one is impaired.
The same is true of alcohol. In spite of common belief, the .08 BAC limit wasn’t determined by science. It can’t be, due to the reality of biological variability. The .08 BAC limit was determined by politicians, using scientific input as well as societal input. That explains why the alcohol per se limit varies from .02 to .08 gm/dl in various developed countries of the world, and those countries based their decision all on the same science! It’s other societal inputs such as risk tolerance and desire for freedom that come into play to make that decision.
None of this proves it’s safe to drive after smoking pot. It’s not. It simply explains why a defined per se limit of THC in blood that proves someone is impaired can never be supported by science.
This also may explain why the preferred means to deal with drug impaired driving is not to establish per se limits, but rather to establish a zero tolerance policy for mind altering drugs in a driver that has been shown to be impaired.
Source: http://www.duidvictimvoices.org/ April 2015
New drunken-driving laws in British Columbia have led to a dramatic decrease (roughly 50%). Officials ramped up penalties on drivers who tested at a lower blood alcohol level (.05, as opposed to the current .08 legal standard) and authorized police to immediately impound cars.
TRANSCRIPT
WILLIAM BRANGHAM: Six years ago, a terrible family tragedy occurred here in rural British Columbia. But over time, it became much more than that. This tragedy set in motion dramatic changes to the laws governing drinking and driving — changes that supporters say have already saved dozens of lives. That tragedy involved a four year old girl. Her name was Alexa Middelaer
LAUREL MIDDELAER: Well, it was a beautiful May long weekend and my daughter, Alexa, loved this one particular horse and she really wanted to show her grandparents that horse. I remember saying good bye to her, and then very shortly after that we heard all kinds of sirens. And at that moment I just– I just knew. I said, “It– it’s Alexa. Something happened to Alexa.”
WILLIAM BRANGHAM: A 56 year-old woman doing nearly twice the speed limit, lost control of her car and smashed into the exact spot where Alexa stood feeding the horse on the side of the road. The woman – – who was later convicted and sent to prison — admitted to police she’d had three glasses of wine before getting into her car.
LAUREL MIDDELAER: When we knew, roadside, that our daughter was dead, I remember my husband just — in the ambulance — we both held each other and he said, “This will not break us. This will define us. There will be some good in this.”
WILLIAM BRANGHAM: After the accident, Alexa’s parents – Michael and Laurel – launched a campaign to try and change the culture around drinking and driving … and to deter people from doing it…. Their events became a regular feature on local news
LAUREL MIDDELAER (from local news) We will honor our daughter and we will make the necessary changes that, number one…
WILLIAM BRANGHAM: But they soon realized it would take more than that – they realized they’d have to change the drunk driving laws, which, like in the U.S., sets the legal blood alcohol limit at .08 percent. After lobbying the government for nearly a year — alongside groups like Mothers Against Drunk Driving – their efforts paid off. In 2010, the Provincial Government not only stiffened penalties against driving at.08, but more importantly, it targeted drivers who fall below that level — to .05 — drivers who are not legally drunk. The rationale? Even a few drinks – as few as two for a woman, and three for a man — can impair your driving ability
The big change was that if you were now caught driving with a .05 blood alcohol level, the police were authorized – on the spot — to fine you, suspend your drivers license, and immediately impound your car for at least three days. They’d get you out of the vehicle, and a tow truck would haul it away.
In late 2010, police began enforcing the new laws, and police impound lots across British Columbia began filling up. The changes sparked an uproar. Civil libertarians argued it gave the police too much power – and restaurant owners like Mark Roberts said the new laws damaged the economy… he says his business dropped between 10 and 20 percent.
MARK ROBERTS: When the change of drinking-driving laws came out, we knew that was going to have a strong impact on our business.
WILLIAM BRANGHAM: What did you think? That customers would suddenly be afraid and that they wouldn’t come to your door?
MARK ROBERTS: We thought that there was a lot of unknowns about what that meant. How many drinks could people have? There was very little information about how that was going to be enforced, how it was going to impact what people could drink. We were creating non-alcoholic drinks to make up for the lost sales. It was a lot of fear, a lot of unknowns, and some real changes in people’s behavior.
WILLIAM BRANGHAM: And the impact was immediate. During the first year the new law was in effect, the number of drunk driving deaths in British Columbia plunged. Critics argued that first year was just a fluke. But the second year? The number declined again. A 55% reduction in deaths in just two years.
The message, it seemed, had started getting through to drivers
TIM STOCKWELL: So it was quite well-publicized. And for deterrence to work it’s as much about knowing and expecting there being a consequence than it actually be likely. People’s perception that they were likely to be caught was probably way higher than it actually was.
WILLIAM BRANGHAM: And that’s key?
TIM STOCKWELL: That is key. It’s very important….
WILLIAM BRANGHAM: Tim Stockwell is an expert on alcohol policy at the University of Victoria. He told us he can’t think of a single reform that’s had this big an impact, this quickly. He and his colleagues recently published a peer-reviewed study of the effectiveness of the new laws.
TIM STOCKWELL: These laws epitomize a perfect deterrence theory in action. And it is very important to understand that you don’t need draconian, severe penalties. They have to be severe enough. It’s more important that they are certain, and that they are swift. So on the spot, losing your car for three days, a week, that’s severe enough.
WILLIAM BRANGHAM: The new laws have faced some setbacks: the police had problems with some of their breathalyzers, the government had to ammend the laws when courts ruled that drivers deserved a better appeals process. And last fall a judge ruled in favor of a driver who appealed his 2012 driving suspension. Critics say that ruling that could force a rewriting of the laws. For now, the heart of the new laws though remain intact.
WILLIAM BRANGHAM: What about the argument that there have been so many lives saved by these new rules that yes, it may have taken a hit out of your business, but that to save a bunch of people’s lives that that’s an OK price to pay?
MARK ROBERTS: Yeah. Well, it’s hard to argue that. I’m certainly not going to sit here and say well, we should allow people to drink whatever, and whatever the consequences are, that’s the way it is going to be. I certainly wouldn’t advocate that.
WILLIAM BRANGHAM: Why do you think this has been so effective?
LAUREL MIDDELAER: I think because the consequence is firm. I think that people respond when there’s a harsher consequence. And I think, too, because it’s aligned to a larger goal. Just like secondhand smoke, we have no tolerance for that anymore, just like when seatbelts came in, there was that fundamental shift. My goal has always been that there will be a fundamental shift that it’s not OK to drink and drive. Drinking is fine. Absolutely — drink whatever you like and enjoy and partake, but just don’t mix it with driving.
Source: http://www.pbs.org/newshour Jan.2014
Definition of a Nightmare: Trying to Enforce Colorado’s Conflicting Marijuana Regulatory Laws
The Police Foundation and the Colorado Association of Chiefs of Police released the above report this week to guide law enforcement about marijuana in other states. The report points to the Byzantine layers of regulations that evolved from constitutional amendments voters passed to legalize medical marijuana in 2000 (Amendment 20) and recreational marijuana in 2012 (Amendment 64).
From June 1, 2001 to December 21, 2008, Colorado issued medical marijuana cards to 4,819 patients. Each cardholder could designate a caregiver to grow marijuana for up to five patients. In 2009, a court decision overturned the limit of five patients per caregiver. That year, with virtually no limits on the number of patients caregivers could supply, 41,039 citizens obtained medical marijuana cards, an increase of 762 percent.
The legislature responded by passing bills in 2010 and 2011 to create the Colorado Medical Marijuana Code. Among other things, the Code legalized commercial medical marijuana centers to grow and sell medical marijuana, reinstated the five-patient limit for caregivers, set up a business-licensing regimen, and allowed for marijuana-infused products to be sold to patients. In 2012, citizens passed Amendment 64, legalizing recreational marijuana, and new sets or regulations were created for both home growers and commercial growers, processors, and retail sales outlets. This resulted in four models of regulation.
Caregiver/Patient
Caregivers can grow medical marijuana for up to five patients and themselves.
Patients licensed by the Department of Public Health and Environment
Regulatory authorities: Department of Public Health and Environment & local law enforcement
Medical Commercial
Businesses, owners, and employees licensed
Regulatory authority: Department of Revenue, Marijuana Enforcement Division
Recreational Commercial
Businesses, owners, and employees licensed
Regulatory authority: Department of Revenue, Marijuana Enforcement Division
Recreational Home Grows
Anyone age 21 or older can grow up to six plants
Law enforcement seeing “co-op cultivations” where many home growers are growing at one location
No license required
Regulatory authority: local law enforcement
Caregivers must register the location of their cultivation sites, but no punishment is specified for those who do not, and many don’t. Because of privacy laws, patient information cannot be accessed to check for whom caregivers are growing. Caregivers have no cards and no sanctions if they fail to register. Attempting to establish probable cause under conflicting regulatory mechanisms makes it difficult to prosecute those who ignore the regulations.
Data kept by the Denver Police Department and the Department of Revenue show the number of marijuana facilities in Denver and statewide:
Medical Centers–Denver 198, Statewide 501
Infused Medical Product Factories–Denver 78, Statewide 158
Medical Cultivations–Denver 376, Statewide 739
Recreational Stores–Denver 126, Statewide 306
Infused Recreational Factories–Denver 44, Statewide 92
Recreational Cultivations–Denver 190, Statewide 375
Labs Checking Recreational for THC–Denver 9, Statewide 15
Total Marijuana Facilities–Denver 1,021, statewide 2,186
The result of trying to enforce conflicting regulatory laws can be seen in another recently released Colorado report. It estimated that demand for marijuana in Colorado in 2014 was 130 metric tons but legal supplies could only account for 77 metric tons. The rest, according to press reports, came from criminals in the black market or legal cultivators selling under the table in the “grey” market.
“Colorado law enforcement officials . . . are convinced that the black and the grey markets are thriving in Colorado primarily through unregulated grows, large quantities of marijuana stashed in homes, and by undercutting the price of legitimate marijuana sales. In fact, police have stated that legalized marijuana may have increased the illegal drug trade.”
Source: www.The Marijuana Report.Org February 2015
Law enforcement officials would love to have a clear way to tell when a driver is too drugged to drive. But the decades of experience the country has in setting limits for alcohol have turned out to be rather useless so far because the mind-altering compound in cannabis, THC, dissolves in fat, whereas alcohol dissolves in water.
And that changes everything. “It’s really difficult to document drugged driving in a relevant way,” says Margaret Haney, a neurobiologist at Columbia University, “[because of] the simple fact that THC is fat soluble. That makes it absorbed in a very different way and much more difficult to relate behavior to, say, [blood] levels of THC or develop a breathalyzer.”
When you drink, alcohol spreads through your saliva and breath. It evenly saturates your lungs and blood. Measuring the volume of alcohol in one part of your body can predictably tell you how much is in any other part of your body — like how much is affecting your brain at any given time.
That made it possible to do the science on alcohol and crash risk back in the mid-20th century. Eventually, decades of study helped formulate the 0.08 blood alcohol limit as too drunk to drive safely. “The 0.08 standard in alcohol is from decades of careful epidemiological research,” says Andrea Roth, a professor of law at the University of California, Berkeley.
But marijuana isn’t like that. The height of your intoxication isn’t at the moment when blood THC levels peak, and the high doesn’t rise and fall uniformly based on how much THC leaves and enters your bodily fluids, says Marilyn Huestis, who headed the chemistry and drug metabolism section at the National Institute on Drug Abuse.
Because THC is fat soluble, it moves readily from water environments, like blood, to fatty environments. Fatty tissues act like sponges for the THC, Huestis says. “And the brain is a very fatty tissue. It’s been proven you can still measure THC in the brain even if it’s no longer measurable in the blood.”
From her research, Huestis found that THC rapidly clears out of the blood in occasional users within a couple of hours. While they’re still high, a trickle of THC leaches out of their brains and other fatty tissues back into the blood until it’s all gone.
That means a lab test would only find a trace amount of THC in the blood of occasional smokers after a few hours. “You could have smoked a good amount, just waited two hours, still be pretty intoxicated and yet pass the drug test [for driving],” says Haney.
And if you eat the weed instead of smoking it, Haney says, your blood never carries that much THC. “With oral THC, it takes several hours for [blood THC] to peak, but it remains very low compared to the smoked route, even though they’re very high. It’s a hundredfold difference,” she says.
But daily users are different. Huestis says that heavy smokers build up so much THC in their body fat that it could continue leaching out for weeks after they last smoked. These chronic, frequent users will also experience a rapid loss of THC from their blood after smoking, but they will also have a constant, moderate level of blood THC even when they’re not high, Huestis says.
It gets trickier when you try to factor in the chronic effect of smoking weed, Huestis says. “We found [chronic, frequent smokers’] brains had changed and reduced the density of cannabinoid receptors,” she says. They were cognitively impaired for up to 28 days after their last use, and their driving might also still be impaired for that long. “It’s pretty scary,” she says.
The attitude difference between stoned drivers and alcohol drivers seems clear, Huestis
says. Pot smokers, she says, “tend to be more aware they’re impaired than alcohol users.” Drunk drivers are more aggressive, and high drivers are slower. But in her studies, she found that being blazed enough, as when a smoker’s blood THC level peaks at 13 nanograms per milliliter, could be just as a dangerous as driving drunk. The marijuana advocacy group NORML emphasizes that driving high can be dangerous, and advises people to drive sober.
This all translates into a colossal headache for researchers and lawmakers alike. While scientists continue to bang their heads over how to draw up a biological measurement for marijuana intoxication, legislators want a way to quickly identify and penalize people who are too high to drive.
The instinct, Huestis says, is to come up with a law that parallels the 0.08 BAC standard for alcohol. “Everyone is looking for one number,” she says. “And it’s almost impossible to come up with one number. Occasional users can be very impaired at one microgram per liter, and chronic, frequent smokers will be over one microgram per liter maybe for weeks.”
The shaky science around relating blood THC to driving impairment is unfair for people living in marijuana-legal states that have absolute blood THC limits for driving, says Andrea Roth, a professor of law at the University of California, Berkeley.
In states like Washington, if a driver is found to have over 5 nanograms of THC per milliliter in their blood, they automatically get a DUI-cannabis. “If we are going to criminalize DUI marijuana, we need to take information from scientific studies and use it to decide if that risk is sufficiently high to be so morally blameworthy that we call it a crime. But we don’t, so picking 5 nanograms per milliliter is arbitrary,” Roth says.
The complicated biology of THC makes current DUI cases very tricky.
“Blood isn’t taken in the U.S. until 1.5 to four hours after the [traffic] incident,” Huestis says. By then, THC levels would have fallen significantly, and these people might have been impaired but passed the test. At the same time, a heavy user living in a state like Washington would get a DUI even if she or he hadn’t smoked in weeks.
As a result, it gets difficult to even understand how risky blazed driving is. Traffic studies that rely on blood THC measures could also be inaccurate if blood is drawn too late and THC has already left the system. And some state traffic databases, including Colorado’s, according to state traffic officials, link accidents to 11-nor-9-carboxy-THC, a byproduct of marijuana metabolism that marks only recent exposure and not intoxication. That might result in an overestimation of marijuana-related accidents.
In the meantime, Haney says, the challenge shouldn’t deter people from trying to find a marijuana DUI solution. People are working on breath tests, saliva, other blood markers and behavioral tests, just nothing that so far has stuck, she says. “We need something, because it’s an important public health issue. But how we’re going to get there? I just don’t know.”
Source: http://www.npr.org/sections/health-shots/2016/02/09/466147956 Feb.2016
Seeking a safe haven in Colorado’s legal marijuana marketplace, illegal drug traffickers are growing weed among the state’s sanctioned pot warehouses and farms, then covertly shipping it elsewhere and pocketing millions of dollars from the sale, according to law enforcement officials and court records consulted by The Associated Press.
In one case, the owner of a skydiving business crammed hundreds of pounds of Colorado pot into his planes and flew the weed to Minnesota, where associates allegedly sold it for millions of dollars in cash. In another, a Denver man was charged with sending more than 100 pot-filled FedEx packages to Buffalo, New York, where drug dealers divvied up the shipment. Twenty other drug traffickers, many from Cuba, were accused of relocating to Colorado to grow marijuana that they sent to Florida, where it can fetch more than double the price in a legal Colorado shop.
These cases and others confirm a longstanding fear of marijuana opponents that the state’s much-watched experiment in legal pot would invite more illegal trafficking to other states where the drug is still strictly forbidden.
One source is Colorado residents or tourists who buy retail pot and take it out of state. But more concerning to authorities are larger-scale traffickers who move here specifically to grow the drug and ship to more lucrative markets.
The trend also bolsters the argument of neighboring Nebraska and Oklahoma, which filed a lawsuit in late 2014 seeking to declare Colorado’s pot legalization unconstitutional, arguing that the move sent a tide of illicit weed across their borders. The Obama administration last month urged the Supreme Court to reject the suit, saying that the leakage was not Colorado’s fault.
No one knows exactly how much pot leaves Colorado. When illegal shipments are seized, it’s often impossible to prove where the marijuana was grown. But court documents and interviews with law enforcement officials indicate well-organized traffickers are seeking refuge in Colorado’s flourishing pot industry.
“There’s no question there’s a lot more of this activity than there was two years ago,” said Colorado’s U.S. attorney, John Walsh.
Some in the legal industry say police have exaggerated the problem and put unfair scrutiny on people who legally grow pot on behalf of patients. Lawmakers last year limited unregulated pot growers to no more than 99 plants in an effort to crack down on those selling untaxed pot.
The federal government allowed Colorado’s experiment on the condition that state officials act to keep marijuana from migrating to places where it is still outlawed and out of the hands of criminal cartels. Federal authorities acknowledge that both things are happening but say that, because the state is trying to keep its industry tightly regulated, there’s no reason to end the legal pot trade.
(MY NOTE: This is an insane position to take. The feds are allowing large-scale manufacturing and distribution to take place in Colorado and elsewhere. All of it is in violation of numerous federal laws that bring mandatory minimum sentences to traffickers. This administration’s absolute failure to enforce federal law is catamount to aiding and abetting drug traffickers on a scale seldom seen in the drug trafficking world prior to legalization. DOJ’s initial claim was that federal resources would not be used to prosecute “patients”
who are in compliance with state “medi-pot” laws. In order words, it was supposed to be about leaving users alone. Nothing about the current situation is about “patients.” It is about commercialization and trafficking, with legalized states producing high-grade pot for the rest of the country.
The feds could immediately stop 90% of this nonsense for the cost of postage stamps — sending letters written on DOJ letterhead that provide notice of impending forfeiture of all property used in furtherance of large-scale trafficking and money laundering. This would include all drug proceeds (and arguably would include the seizure of drug proceeds disguised as “tax revenue.” I spent more than 20 years doing these cases in federal court, so I know what I am talking about. Back to the article. Monte Stiles)
The pot industry also acknowledges the criminal activity and insists it is doing all it can to keep legally grown weed from crossing state lines. Among other safeguards, Colorado law requires growers to get a license and use a “seed-to-sale” tracking system that monitors marijuana plants at every stage.
Many of the illicit growers come from elsewhere, never obtain a growing license and “don’t even attempt to adhere to the law,” said Barbra M. Roach, special agent in charge of the Drug Enforcement Administration’s Denver field division.
“It’s like hiding in plain sight,” she said. (EXACTLY WHAT WE HAVE BEEN SAYING ALL ALONG)
Authorities in Washington state, which also allows recreational marijuana, have noticed more marijuana leaving the state. But more reports are coming from Colorado, which has the nation’s most robust commercial market and an international reputation for producing premium, high-potency pot.
“It’s a brand name now,” Roach said.
Jason Warf, head of the Southern Colorado Cannabis Council, said people are “coming from out-of-state, buying products from licensed stores and being arrested on their way home.”
That “is really hard to curb,” he said. “We can’t essentially babysit adults and their behavior.”
The Colorado Department of Revenue’s marijuana-enforcement division cites shops if pot is unaccounted for but “after it’s sold, we have very little control what happens to the marijuana,” Director Lewis Koski said.
Police agencies seized nearly 2 tons of Colorado weed from drivers who had intended to take it to 36 other states in 2014, the year legal pot shops opened, according to the Rocky Mountain High Intensity Drug Trafficking Area, a federally funded drug task force. By comparison, they seized less than a ton in 2009.
U.S. postal inspectors seized about 470 pounds of Colorado pot from the mail in 2014, up from 57 pounds in 2010, according to the task force, whose findings are based on on voluntary submissions from law enforcement agencies and are largely anecdotal.
Some cases have comic overtones, like when a Wyoming patrolman discovered 7 ounces of high-grade weed in trick-or-treat bags the day after Halloween, or when police in northern Colorado seized stuffed animals full of marijuana destined for Florida.
Other operations are more sophisticated, like the one in which authorities say 32 people used skydiving planes and posed as licensed medical marijuana caregivers and small business owners to export tens of thousands of pounds of pot grown in Denver warehouses, usually to Minnesota. The organization made more than $12 million over four years, according to a state indictment.
When they busted illegal pot farms in southern Colorado in September, state and federal agents found 28 guns, more than 1,000 plants and $25,000 in cash.
A local UPS facility intercepts about 50 pounds of pot headed out of state each week, said Todd Reeves of the Colorado Drug Investigators Association. “We don’t have the resources,” he said, “to be able to go after every single one of these cases.”
Source: SADIE GURMAN, ASSOCIATED PRESS DENVER — Jan 28, 2016, 2:11 AM ET http://abcnews.go.com/US/wireStory/drug-traffickers-seek-safe-haven-amid-legal-marijuana-36564435
After the Police Chief of Gloucester, Massachusetts announced the town will connect people with treatment when they come to the police station with illegal drugs and paraphernalia, instead of arresting them, 56 police departments in 17 states have started similar programs.
An additional 110 police departments are preparing to start programs that emphasize treatment over incarceration, The New York Timesreports. Two hundred treatment centers nationwide have agreed to be partners in these programs. In May 2015, Gloucester Police Chief Leonard Campanello posted on Facebook, “We will walk them through the system toward detox and recovery. We will assign them an ‘angel’ who will be their guide through the process. Not in hours or days, but on the spot.” Since then, Gloucester has developed a national network of centers that are willing to provide treatment beds and take referrals by police, whether or not a person has insurance.
Several local pharmacies have agreed to make the opioid overdose antidote naloxone available at a discount.
Most of the program’s costs are covered by the Police Assisted Addiction and Recovery Initiative, which Chief Campanello founded with Gloucester businessman John E. Rosenthal. The initiative has raised hundreds of thousands of dollars. It has also received millions of dollars in in-kind contributions, including placement in treatment centers.
The program has 55 volunteers in recovery or who are familiar with addiction, who listen and offer moral support. Local taxi companies provide free rides to treatment facilities or the airport, if the treatment facility is far away.
Since the program started, 391 people have turned themselves in at Gloucester’s police station. About 40 percent are from the local area. All have been placed in treatment, the article notes.
Source: http://www.drugfree.org/join-together 26th Jan. 2016
By Mark H. Moore; Mark H. Moore is professor of criminal justice at Harvard’s Kennedy School of Government.
CAMBRIDGE, Mass.— History has valuable lessons to teach policy makers but it reveals its lessons only grudgingly.
Close analyses of the facts and their relevance is required lest policy makers fall victim to the persuasive power of false analogies and are misled into imprudent judgments. Just such a danger is posed by those who casually invoke the ”lessons of Prohibition” to argue for the legalization of drugs.
What everyone ”knows” about Prohibition is that it was a failure. It did not eliminate drinking; it did create a black market. That in turn spawned criminal syndicates and random violence. Corruption and widespread disrespect for law were incubated and, most tellingly, Prohibition was repealed only 14 years after it was enshrined in the Constitution.
The lesson drawn by commentators is that it is fruitless to allow moralists to use criminal law to control intoxicating substances. Many now say it is equally unwise to rely on the law to solve the nation’s drug problem.
But the conventional view of Prohibition is not supported by the facts.
First, the regime created in 1919 by the 18th Amendment and the Volstead Act, which charged the Treasury Department with enforcement of the new restrictions, was far from all-embracing. The amendment prohibited the commercial manufacture and distribution of alcoholic beverages; it did not prohibit use, nor production for one’s own consumption. Moreover, the provisions did not take effect until a year after passage -plenty of time for people to stockpile supplies.
Second, alcohol consumption declined dramatically during Prohibition. Cirrhosis death rates for men were 29.5 per 100,000 in 1911 and 10.7 in 1929. Admissions to state mental hospitals for alcoholic psychosis declined from 10.1 per 100,000 in 1919 to 4.7 in 1928.
Arrests for public drunkenness and disorderly conduct declined 50 percent between 1916 and 1922. For the population as a whole, the best estimates are that consumption of alcohol declined by 30 percent to 50 percent.
Third, violent crime did not increase dramatically during Prohibition. Homicide rates rose dramatically from 1900 to 1910 but remained roughly constant during Prohibition’s 14 year rule. Organized crime may have become more visible and lurid during Prohibition, but it existed before and after.
Fourth, following the repeal of Prohibition, alcohol consumption increased. Today, alcohol is estimated to be the cause of more than 23,000 motor vehicle deaths and is implicated in more than half of the nation’s 20,000 homicides. In contrast, drugs have not yet been persuasively linked to highway fatalities and are believed to account for 10 percent to 20 percent of homicides.
Prohibition did not end alcohol use. What is remarkable, however, is that a relatively narrow political movement, relying on a relatively weak set of statutes, succeeded in reducing, by one-third, the consumption of a drug that had wide historical and popular sanction.
This is not to say that society was wrong to repeal Prohibition. A democratic society may decide that recreational drinking is worth the price in traffic fatalities and other consequences. But the common claim that laws backed by morally motivated political movements cannot reduce drug use is wrong.
Not only are the facts of Prohibition misunderstood, but the lessons are misapplied to the current situation.
The U.S. is in the early to middle stages of a potentially widespread cocaine epidemic. (in 2001) If the line is held now, we can prevent new users and increasing casualties. So this is exactly not the time to be considering a liberalization of our laws on cocaine. We need a firm stand by society against cocaine use to extend and reinforce the messages that are being learned through painful personal experience and testimony.
The real lesson of Prohibition is that the society can, indeed, make a dent in the consumption of drugs through laws. There is a price to be paid for such restrictions, of course. But for drugs such as heroin and cocaine, which are dangerous but currently largely unpopular, that price is small relative to the benefits.
Source: http://nyti.ms/U1QHdN Published October 16 1989
1. Prohibited the commercial manufacture, and distribution of alcoholic beverages
It DID NOT prohibit use, or production for one’s own consumption
2. Alcohol consumption declined dramatically during prohibition.
Cirrhosis death rates for men were 29.5 per 100,000 in 1911 and 10.7 inn 1929
Mental hospital admission for alcoholic psychosis declined from 10.1 per 100,000 in 1919 to 4.7 in 1928.
Arrests for public drunkenness and disorderly conducted declined 50% between 1916 and 1922
Consumption of alcohol declined by 30 to 50%
3. Violent crimes DID NOT increase dramatically during prohibition. Homicide rates rose dramatically from 1900 to 1910 but remained roughly constant during prohibition’s 14-year rule. Organized crime did become more visible during prohibition but it existed before and after.
4. Following the repeal of prohibition, alcohol consumption increased. Today alcohol is estimated to be the cause of 50% of traffic deaths and is implicated in more than half of the nation’s homicides.
Source: J.McDougal 2001 – re-printed Drug Watch International e-mails.
Few topics have been more distorted by politicians and media than claims about the criminal justice system in its various forms. When the offense involves illicit drugs (use, possession, or trafficking), the distortion becomes pronounced.
In large measure, a complicated set of data have been made even more difficult to grasp because of tendentious (and often false) assertions forwarded by drug legalization advocates, who seek to advance their own “reforms” by first misrepresenting the criminal justice facts. Moreover, though drug use overall is subject to confusion, distortion is even greater when marijuana is the drug in question. An example of agendas distorting understanding is the effort to blamedrug laws for the growth in incarceration. That effort seeks to convince a public otherwise disinclined to accept more drugs that current drug laws have created the supposed injustice of “mass incarceration.” This is demonstrably untrue.
To answer with the facts, we will address several distinct dimensions of legal institutions concerning illicit drugs: prison sentences, recidivism of released prisoners, and the relationship of drug use to the commission of criminal acts. (We addressed the parallel issue of drug arrests in a previous study, showing that they are far fewer in proportion to drug use than drug reform advocates claim.)
We start with prison inmates, found in both state and federal prisons, and contrast the cumulative numbers of those imprisoned with those entering in a single year. In all cases, we will find that the proportion of drug offenses to the overall number of prisoners has been much overstated. Cumulatively, all drug offenders in both systems constitute20 percent of inmates (303,800 out of 1,508,636 sentenced inmates).
THE FEDERAL PRISON SYSTEM:
The federal system holds 13 percent of all prisoners, but contains the larger proportion of drug offenders. This happens because many trafficking offenses, be they interstate or international, are specifically federal in nature. But even as the total number of prisoners has grown, the drug-offender percentage has declined steadily.
There were 52,568 federal prisoners in 1989 (those “under jurisdiction”), and by 2014, there were 191,374 (those “sentenced” – the categories shifted slightly over time, yielding slight variation in respective calculations). Yet the percentage of drug offenders in the total peaked in 1996, when it stood at 59.6 percent. A 2014 publication from the White House showing the cumulative total of federal prisoners broken down to show drug offenses as the most serious charge, reveals that the proportion of drug offenders had dropped to 44 percent of all offenders in 2011. By 2014, the most recent data on sentenced drug offenders in the federal prison system shifted back to 50 percent of all federal inmates, an increase from the previous ratio due largely to recent inmate releases.
When we turn to inmates entering federal prison in a single year, data are more current, but show the same trajectory. In 1998, the proportion of drug offenders incarcerated for that year was 41 percent (vs. 57.8 percent of the 1998 cumulative “jurisdiction” figure). By 2014, according to the United States Sentencing Commission (USSC), drug offenders (of all types) had fallen to only 32 percent (of 75,836 entering federal inmates, 22,193 were drug offenders). Importantly, 96.6 percent of entering inmates who were drug offenders were convicted of trafficking offenses, while only 0.9 percent were convicted of simple possession.
We can further break these data down by drug type, and by nature of the drug offense. Methamphetamine resulted in the largest subset of drug types with more than 6,304 incarcerations, while heroin produced 2,431.
Though recent legislative reforms have altered the mandatory sentencing guidelines regarding powder cocaine offenses (based on weight) compared to crack offenses (a former ratio of 100 to 1 has been amended to 18 to 1), there were only 4,959 powder cocaine convictions in 2014, compared to 2,439 crack convictions. Moreover, the number of crack cocaine inmates sentenced for simple possession was 0.3 percent, or no more than 7 people.
Finally, marijuana federal incarcerations totaled only 3,971. Marijuana offenses are overwhelmingly (97.6 percent) for trafficking, with a “simple possession offense” representing only 75 individuals (or 1.9 percent), with that conviction often resulting from downward plea-bargaining from more serious offenses. To show the emphasis on traffickers, when asked in Congressionaltestimony how many drug possession offenders the Drug Enforcement Administration (DEA) refers for federal prosecution, Acting Deputy Administrator Jack Riley stated, “virtually none.”
What, then, is currently driving the changing distribution of the federal inmate population? To a large extent it is a rising number of immigration offenses, according to a study by the Congressional Research Service. This fact is echoed for single-year entry for prisoners as well: in 2014 the USSC shows 29 percent were immigration offenders, while 32 percent were drug offenders.
THE STATE PRISON SYSTEM: The state prison system is larger, holding 1,317,262 sentenced prisoners cumulatively in 2014. The state prison inmate population has also grown over time, and the absolute number of drug offenders within that total has nearly doubled since 1989 from 120,100 to 208,000 (sentenced) in 2014.
Yet just as with the federal system, the percentage of drug offenders has declined since the peak year 1990 when it stood at at 22 percent. For 2014, those whose most serious offense involved drugs were only 16 percent of sentenced state prison inmates (drug possession offenses are only 3.6 percent of all state inmates).
While there has been a marked increase in the state prison population over the past few decades as America has gotten more serious about combatting crime, the data do not support the idea that drug offenses are the primary driver of those increases. Further, with regard to the current push to decriminalize or legalize drug use, there is no support for the assertion that convictions for drug use/possession are responsible for the sharp increases in either state or federal prison inmates.
SENTENCING REFORM AND RECIDIVISM:
And what of sentencing reforms leading to the release of large numbers of federal drug offenders? A substantial problem is recidivism, or re-offending within a relatively short period of time, as we have elsewhere recently argued. Yet the press persists in misrepresentation. According to the Economist, advocating for prisoner release, “Given how high America’s incarceration rate is, it is fair to say reducing it won’t precipitate a crime wave. Many convicts serving long sentences were never generally dangerous, or have mellowed with age, and no longer pose a threat to the public.” But the data show otherwise. According to a Bureau of Justice Statisticsstudy of prisoners released in 2005 and tracked for five years, 32 percent were drug offenders.
Of these, fully 77 percent of those released re-offended within that five- year-period (57 percent of all offenders re-offended at only one year).
It is worth noting two features of a further breakdown of the 404,638 released prisoners in the study. First, the outcome is the same regardless of the type of drug offense (trafficking or possession); that is, either type of offense has comparable re-offense rates. Drug possession offenders had 78 percent recidivism, drug trafficking offenders, 75 percent.
Second, the percent of re-offenses where the subsequent crime specifically involved drugs reached 51 percent. More compelling, violent crimes were fully 25 percent of drug inmates’ recidivating offenses.
These data clearly show if drug offenders are released through sentencing reform, both drug and violent crime will follow; to the extent that they are released early, the effect is to compress their criminal impact into a shorter period.
Further, inmates’ prior arrest history matters. In this study, for all offenders, the mean number of prior arrests per released prisoner was nearly 11.
For those who had ten or more prior arrests, 86 percent re-offended within 5 years. (Even for those aged 40 and over, the recidivism for drug offenders was 71 percent.)
DRUG USE AND THE COMMISSION OF CRIMES:
Finally, there is the role of drugs in the commission of crime. According to another Bureau of Justice Statistics study, one third of state inmates and one quarter of federal inmates committed their offenses under the influence of illicit drugs. That holds for all crimes, not just drug offenses.
For state prisoners, 69 percent used drugs “regularly,” and for 59 percent, that drug was marijuana (with 30 percent using cocaine/crack).
For federal prisoners, 64 percent used drugs “regularly,” with 53 percent using marijuana (and 28 percent using cocaine/crack). Even for federal trafficking offenders, 34 percent were using drugs at the time of the offense.
The same pattern holds for violent offenders. Of them, 49 percent of both federal and state offenders used drugs in the month prior to the offense. The number using drugs at the time of the violent offense reached 28 percent of state and 24 percent of federal prisoners. Homicide-specific rates of drug use in the month prior to the offense were 49 percent and 45 percent, respectively for state and federal prison inmates, with a respective 27 percent and 17 percent using at the time of the homicide.
POLICY CONCLUSIONS:
By these data, we may conclude the following:
1. Sentencing reforms that result in the early release of prison inmates will increase the number of future crimes, and crime victims, through recidivism, while the effect will be concentrated in time, thereby stressing law enforcement and rehabilitation services.
2. Drug intoxication (including the most prevalent drug, marijuana), is deeply implicated in crime commission, including violent crime. It follows that enabling greater drug use
will magnify the criminal impact, with the corollary that efforts to reduce drug use prevalence should help lower the incidence of crime.
3. In particular, decriminalizing or legalizing marijuana will have virtually no impact on prison overcrowding, but the attendant increase in drug-use prevalence nationwide will likely lead to increased commission of crimes, including non-drug offenses and violent offense
Source: http://www.hudson.org/research Nov. 2015
David W. Murray and John P. Walters
At a Manhattan fundraiser yesterday (as noted by The Hill), potential presidential candidate Hillary Clinton spoke of the rioting in Baltimore by invoking a theme of the Obama administration: the need for reform of the criminal justice system. According to this critique, the current crisis in our cities, in particular focused on violence involving the police and African Americans, has its roots in America’s policies of criminal justice.Former Secretary of State Clinton insisted that we must “reform our criminal justice system” and, according to The Hill, “made a reference to ending ‘mass incarceration,’ but the specifics were drowned out by applause.”
The charge of “mass incarceration” is often attached to changes in criminal justice sentencing that were put in place in the mid-1990s, and led by political figures such as Vice President Joe Biden, a strong supporter of so-called “three strikes” laws and author (as a senator) of the Violence Against Women Act of 1994.
It should be remembered that such measures were politically popular during that decade, driven by the striking damage done to our cities (as well as to vulnerable women), by rising crime rates, in particular, crimes of violence. The circumstance has changed for the better so dramatically that current politicians can perhaps be forgiven for losing sight of the problems that such measures were crafted to address.
Reform of unjust laws is a constant duty, but we should not forget the genuine suffering of criminal victims that led to efforts at protecting those at risk. The reality is that the tough laws were put in place for a reason, to shelter those being devastated by crime and drugs and predatory behavior.
Few doubt that a result of the application of those laws, beyond unintended injustices, was that a great deal of predatory behavior was stopped, though as a consequence, incarceration numbers grew accordingly. The intended effect was produced, as the rate of crime fell dramatically and continues downward to this day.
A graph of forcible rapes reported to the police as found in the FBI Uniform Crime Reports can represent the nature of the overall criminal threat, and the impact of sentencing “reform” (as it was called then) has been surely one of the social factors driving this steep decline in crime. As can be seen, the incidence of “forcible rape” was climbing steeply until the time (1993-1995) that the reforms were implemented.
These laws were strong measures, but surely the sense at the time was that they were necessary, given the dangers to which they were the answer. It would be ironic, indeed, if we now, the very beneficiaries of the decline of violent crime were to reverse such conditions, in the hope of applause. An implication of falling crime is that America is unlikely to see a continuation of the rate of incarceration from those years, simply because the number of committed crimes has dropped so greatly. When crime falls, incarceration should level off, and then decline as a result. That is, in some respects, we could be on the verge of harvesting the benefits from those laws, and even entering a period where the number of incarcerations will decline. Further, because the impact of violent crime has fallen so steeply, we might even see that necessary and long-sought “structural reforms” of our inner cities (jobs, better schools, strengthened family formation), might begin to gain traction.
Yet because the political pressure behind the imposition of those laws has declined first, we could be on the verge of making a tragic mistake, by carelessly reversing the very steps that made vulnerable neighborhoods safer. Whatever new “reforms” we undertake
now, we must take heed lest we re-start the original conditions of crisis, simply to serve political opportunism, often from the very people who called for the initial intervention.
To sum up, it is possible to argue that faced with a threat, we made an intervention, and to a large degree that intervention worked, albeit at considerable social cost. Now is not the time to abandon those efforts. If proto-candidate Clinton and her allies succeed in an effort to abandon effective law enforcement in our cities, very soon, no one will be applauding.
Walters and Murray direct Hudson Institute’s Center for Substance Abuse Policy Research. They both served in the Office of National Drug Control Policy during the George W. Bush administration.
Source: http://www.weeklystandard.com) 29th April 2015
– and “It’s Time to Regulate E-Cigarettes,” by David A. Kessler and Matthew L. Myers (Op-Ed, April 23):
We applaud your editorial and Op-Ed essay for highlighting the rise in electronic cigarette use among high school students and for condemning the tobacco industry for aggressively targeting kids.
Unfortunately, the noxious tactics of Big Tobacco — flavored products, colorful packaging, kid-friendly advertising — are not limited to the marketing of e-cigarettes. They also characterize the commercialization of marijuana in states like Colorado, where pot has been legalized. Attempts to ban edible marijuana products that target youth, such as “Pot Tarts” or “Pot Lollipops,” have been met with fierce opposition from a burgeoning marijuana industry eager to hook kids early, and ensure a steady stream of future profits.
As we condemn the harms of e-cigarettes and their marketing to youth, we should also acknowledge that the legalization and mass commercialization of marijuana means yet another industry that thrives on addiction and recklessly targets the most vulnerable in society. We can reform our drug laws and address the currents pitfalls of prohibition without giving rise to the next Big Tobacco.
PATRICK J. KENNEDY
KEVIN A. SABET
Princeton, N.J.
The writers, a former congressman and a former White House drug policy adviser, respectively, are leaders of Smart Approaches to Marijuana.
Source: Letters to Editor nytimes.com 5th MY 2015
With the medical marijuana law cutting profits for street dealers, police believe that drug-trafficking organizations are turning to far more dangerous drugs, flooding the streets with cocaine, heroin and methamphetamine. Tempe Police, the DEA and the Arizona Attorney General’s Office attacked that trend in Operation Terminus, a 30-month investigation that resulted in the dismantling of what investigators described as an extensive drug trafficking network that stretched from Sinoloa, Mexico, to Phoenix, Los Angeles and Indianapolis. Tempe Police Chief Tom Ryff pointed out that the one missing item in this case is marijuana. During the investigation, there were 77 indictments, with authorities seizing $7.5 million cash, 485 pounds of methamphetamine, 50 Kilograms of cocaine, 4.5 pounds of heroin and 37 firearms. “Here, in Arizona alone, you can go to a strip mall and purchase marijuana,” Ryff said. “Drug cartels are sophisticated, they are a criminal enterprise. If the money is not there, they are going to change their tactics.” Ryff praised the Cronkite School at ASU for their work in evaluating the impact of drugs in Arizona as seen in their recent semester long project: Hooked, Tracking Heroin’s hold on Arizona. “They are plowing marijuana fields and planting opiates. It’s killing our youths. It’s an epidemic,” said Lt. Mike Pooley, a Tempe police spokesman. Police believe that drug addiction is the root cause of many property crimes, including burglary and shoplifting. Mesa police arrested a suspect last week who told them he used an air gun resembling a pistol to rob a bank in order to pay his heroin dealer. Operation Terminus started in 2012 with the arrest of an individual named Jesus who was picked up from a different criminal investigation,Tempe police Commander Kim Hale said. The drug-trafficking organizations are based in the Sinoloa state in Mexico, but the drugs are distributed by local syndicates throughout the Valley and as far away as Los Angeles and Indianapolis, he said. “Arizona is ground zero for for drugs and our border states have been impacted just as is the borders in California, Texas and News Mexico,” Hale said. Tempe police released a list of 70 defendants who were charged with a variety of drug trafficking crimes as the result of Operation Terminus.
Source: www.azcentral.com 6th March 2015
Though many young people seem to perceive marijuana as harmless, its use may pose serious risk for adverse behaviors and health consequences.
An extensive research review published June 5 in the New England Journal of Medicineconcluded that marijuana use is linked to multiple adverse effects—particularly in youth.
“Despite some contentious discussions regarding the addictiveness of marijuana, the evidence clearly indicates that long-term marijuana use can lead to addiction,” said lead author Nora Volkow, M.D., director of the National Institute on Drug Abuse (NIDA), and three of NIDA’s top officials.

Stanimir G.Stoev/Shutterstock
According to the 2012 National Survey on Drug Use and Health, marijuana is the most commonly used “illicit” drug in the United States, with an estimated 12 percent of people aged 12 or older reporting its use in the prior year. The 2013 Monitoring the Future Survey—supported by NIDA—found that 6.5 percent of 12th graders report daily or near-daily marijuana use, with 60 percent perceiving regular use of marijuana not to be harmful (Psychiatric News, February 6). Volkow and colleagues suggested that as more states move toward policies that legalize cannabis for medical or recreational purposes, rates for marijuana use among teenagers and young adults will increase, as will the negative health consequences associated with its use.
“The regular use of marijuana during adolescence is of particular concern, since use by this age group is associated with an increased likelihood of deleterious consequences,” Volkow and colleagues cautioned.
The review, “Adverse Health Effects of Marijuana Use,” provided science-based reasoning to explain the onset of marijuana addiction and gave an overview of the adverse health consequences associated with marijuana use from data of 77 studies and literature reviews.
From animal studies, the authors concluded that exposure to tetrahydrocannabinol (THC)—the primary psychoactive chemical in cannabis—in early life can recalibrate the dopaminergic system, the reward system of the brain, to become more sensitive to stimulation with drugs. The authors speculated that the findings may help to explain the increased vulnerability to abuse of marijuana and other substances in later life, which have been reported by adults who initiated cannabis use during adolescence.
The review also highlighted studies showing an association between marijuana use and impaired regions of the human brain, including the precuneas, a key node that is involved in alertness and self-conscious awareness, and the hippocampus, which is important in learning and memory. Other adverse consequences of cannabis use included impaired driving, lowered IQ scores into adulthood, and a potential risk to exacerbate psychotic symptoms in those with mental disorders. The review suggested that risks for adverse effects increase when the drug is used along with alcohol.
“Some physicians continue to prescribe marijuana for medicinal purposes despite limited evidence of a benefit,” noted Volkow and colleagues. “Because older studies are based on the effects of marijuana containing lower levels of THC, stronger adverse health effects may occur with the use of today’s more-potent marijuana.”
The authors emphasized that more research must be done on the potential health consequences of second hand marijuana smoke, the long-term impact of prenatal cannabis exposure, and the effects of marijuana legalization policies on public health.
“It is important to alert the public that using marijuana in the teen years brings health, social, and academic risk,” said Volkow. “Physicians in particular can play a role in conveying to families that early marijuana use can interfere with crucial social and developmental milestones and can impair cognitive development.”
Source: http://psychnews.psychiatryonline.org/ June 26, 2014
This article, based upon the research of professor Troy Payne from the University of Alaska, documents facts that dispel these claims. I think you will find it extremely informative. Similar information should be available in every state fighting legalization. Monte Stiles, DrugWatch International.
It’s complicated: Marijuana law enforcement numbers in Anchorage
There are numerous criminal justice statistics cited in support of and in opposition to Ballot Measure 2 (An Act to Tax and Regulate the Production, Sale, and Use of Marijuana). Recently, arrest numbers, prosecution outcomes, criminal sentencing practices, and incarceration rates, have all been referenced in ads, op-eds, and at debates.
Each of these statistics provides valuable information, but each represents only one aspect of the effect of marijuana on criminal justice in Alaska. The criminal justice system itself is comprised of multiple agencies (law enforcement, courts, corrections, each at local, state, tribal, and federal levels) which, while often working together, ultimately focus on separate tasks, then record, track, and monitor their progress differently and independently.
Focusing on arrests as the sole measure of the criminal justice impact of marijuana can be misleading. Often, marijuana crimes are accompanied by other criminal activity, so it is difficult to parse out what someone was actually “arrested for.” Many data sources will only report the most serious offense. Focusing on the number of prosecutions, convictions or incarceration rates does not provide an accurate overview either, because that number misses the people who had marijuana seized, but who were not prosecuted for marijuana offenses. Additionally, prosecutorial records, and any statistics drawn from them, may not be reliable indicators because as Dean Guaneli, former chief assistant attorney general for Alaska, pointed out in an Oct. 17 op-ed, to get the full view, “you have to look at the background facts in each case.”
As previous commentators have noted, no one in Alaska has completed a detailed analysis of marijuana-case processing from start to finish. Unfortunately, I do not currently have data for that either. But each piece of information is useful in light of the upcoming election. My goal is to bring another small amount of data to the public regarding this issue — a piece of data that illustrates one aspect of the effect of marijuana on criminal justice in Alaska: interaction with the Anchorage Police Department.
I looked at the beginning of the process — from the point police seized marijuana. Most other data sources (arrests, prosecution outcomes, sentencing, incarceration) deal with much later parts of the criminal justice system. None of these alone can provide a complete picture of marijuana-case processing in Alaska. Doing so is surprisingly complicated. (Readers are welcome to register for a few justice and legal studies classes at UAA to find out exactly why, but I will explain a few reasons here.)
I requested information on every incident in which APD seized any amount of marijuana from January 2010 through the latest date available, the end of June 2013. This allows me to describe all incidents in which marijuana was seized, regardless of whether an arrest was made or charges were ultimately filed — capturing all instances where individuals encountered law enforcement because of marijuana.
An “incident” can start with a citizen call to police or through proactive policing such as a traffic stop. “Incident” is the basic unit of police work. Marijuana is seized in less than one-half of 1 percent of all police incidents in Anchorage. Marijuana was seized in about 3,400 out of nearly 900,000 police incidents from January 2010 through midyear 2013, the latest data made available by APD. While that is a small percentage of overall police incidents, APD seizes marijuana between two and three times a day, on average.
The typical marijuana seizure in Anchorage involves a small amount of marijuana — 78.6 percent of incidents where marijuana was seized involved less than 1 ounce of marijuana. Over a third of incidents, 36.3 percent, involved less than 1/8 of an ounce of marijuana.
About three-quarters of incidents (76 percent) where marijuana was seized resulted in charges being referred to the prosecutor against at least one person. I examined what APD records noted was the primary, or most serious charge. The most common primary charge in these situations was use or display of marijuana (violation of AS 11.71.060(a)(1)). Nearly a third (31.4 percent) of persons had this as their primary charge. The next most common primary charges resulting from an incident where marijuana was seized were driving with no license or with a suspended license (10.6 percent), and possession of drugs within 500 feet of a school (10.2 percent).
Despite use or display of marijuana being the most common primary charge, most primary charges were for something other than marijuana use or possession. Over half (58 percent) of incidents where marijuana was seized began with a police response to something else, such as a disturbance or a burglary. Together with the primary charge data, this suggests either 1) that marijuana is most often seized during the investigation of other crimes which vary greatly, or 2) that marijuana use or display provides probable cause for a citizen to come to the attention of police, which then leads to more serious crimes being uncovered. Either way, the available evidence suggests that APD is not focused on making arrests solely for marijuana use, display, or possession.
Demographic data was available for incidents where a person was charged. Of persons charged, 18 percent were under the age of 18 at the time of the incident. Another 23 percent of persons were between the ages of 18 and 21 years. Persons over the age of 21 but under 30 were the largest group by age, comprising 32 percent of persons charged, with people in their 30s making up 15 percent of persons charged. Those 40 years and older made up 12 percent of persons charged. The available data on race is consistent with general trends in criminal justice, with minorities over-represented relative to their percentage in the Anchorage population.
I hope this has provided voters with more information to consider before heading to the polls in November. As I stated at the outset, these data do not present a complete picture of marijuana-case processing — doing that requires collecting, reviewing, analyzing, and synthesizing data from police departments, the state Department of Public Safety, Department of Law, Department of Corrections and the Alaska Court System. We do not yet have a comprehensive criminal justice data platform that would allow such cases processing analyses to be completed quickly.
Troy C. Payne, Ph.D. is assistant professor of justice at the University of Alaska Anchorage. He teaches data analysis, criminology, and crime mapping. His research has examined the effectiveness of policing and crime prevention strategies.
Source: Troy Payne, University of Alaska 25th October 2014
The drugs sent 28,000 people nationwide to the emergency room in 2011.
Attorneys general are fighting the illegal sale of synthetic marijuana with their pens.
A letter signed by 43 attorneys general — including Roy Cooper from North Carolina — was sent to nine major oil companies last Tuesday, urging them to eliminate synthetic marijuana from their gas stations’ convenience stores and retail locations.
Use of the drugs is a national problem — sending 28,000 people to the emergency room in 2011.
“Given the significant danger synthetic drugs present to users, especially our young people, we are extremely troubled that these drugs have been readily available in well-known retail locations,” the attorneys’ letter said.
Synthetic marijuana is often marketed under names like “K2” and “Spice” and is not tested for safety, according to the American Association of Poison Control Centers, which received 3,679 calls due to exposure to the drug in 2014.
Kelly Alanis-Hirsch, a researcher who studies substance abuse disorders at UNC, said the synthetic drug is not comparable to the organic drug, and the lack of regulation poses a serious threat to users’ health.
“It is created by spraying various chemicals on herbs or other leafy material,” Alanis-Hirsch said. “The chemicals mimic the effect of THC that appears naturally in organic marijuana, but the synthetic marijuana compounds vary by manufacturer.”
Federal and state laws prohibit the manufacture, sale and consumption of synthetic marijuana. Synthetic marijuana was made illegal in the state in 2011 when the N.C. General Assembly classified it as a controlled substance.
In 2012, President Barack Obama signed the Synthetic Drug Abuse Prevention Act, which categorized 26 synthetic cannabinoids as Schedule 1 drugs under the Controlled Substances Act — outlawing the drugs at the federal level.
But Alanis-Hirsch said that drug companies have evaded the federal law by manufacturing substances similar, but not identical, to those prohibited by the federal government.
“Recipes are changed in response to governmental efforts to make the product illegal; thus, it’s marketed as a ‘legal high,’” she said.
Mary-Nel Saarloos, a medical doctor in Asheville, said she often treats patients who have overdosed, but the constantly changing chemical components make it difficult to diagnose. Blood and urine tests often can’t detect these components of the drug, she said.
The National Association of Attorneys General called for major oil companies to revoke franchises of gas stations that violate the federal controlled substances laws.
“Young people should not die or be seriously injured from using products bought at gas stations or convenience stores,” the letter says.
Source: www.dailytarheel.com17th February 2015
It is widely known that drug legalizers will not be content with the legalization of pot. Their ultimate goal is the legalization of all drugs.
In using a few of their favourite tactics, they now argue that:
LSD and other psychedelic drugs are “safer than alcohol”
LSD and other psychedelics have “positive psychological benefits” and the ability to “defeat addiction”
The prohibition of psychedelics is a violation of “human rights” (including the right to “belief and spiritual practice, full development of the personality, and free-time and play.”
In other words – safer than alcohol, with medical properties, and fun.
According to long-time legalization advocate David Nutt, speaking at a briefing in London:
“We’ve banned research on psychedelic drugs and other drugs like cannabis for 50 years. Truly, in terms of the amount of wasted opportunity, it’s way greater than the banning of the telescope. This is a truly appalling level of censorship.”
The movement to legalize drugs follows a predictable pattern that must be recognized.
1. Ignore existing laws
2. Decriminalize use
3. Open the door for medi-pot (CBDs)
4. Expand medical use to include everything under the sun
5. Full legalization of marijuana for recreational use
Despite overwhelming evidence of their intent, states seems to be following this pattern as if the pro-drug forces are interested in only the next step, when in fact their long game is “all drugs, by anyone, and all the time.”
This surrender to the drug culture, where we allow a very small minority of the population to dictate policy, laws, and even constitutions, is creating disastrous results and permanent damage to society.
Drug education works when we do enough of it. Surrender is not an option.
Source: Letter from Monte Stile to DrugWatch International 7th March 2015
FOR IMMEDIATE RELEASE
CONTACT: KEVIN@LEARNABOUTSAM.ORG
Today, Smart Approaches to Marijuana (SAM) President Kevin A. Sabet released a statement on the lawsuit brought law enforcement officials in Colorado, Oklahoma and Nebraska against Colorado’s Amendment 64:
“Big Marijuana must be feeling the heat, and I’m sure they are lawyering up. This is now the latest in a series of lawsuits against legalization, and we support this action because Colorado’s decisions regarding marijuana are not without consequences to neighboring states, and indeed all Americans. The legalization of marijuana is not implemented in a vacuum. The current policy of denial about federal law is untenable. Surrounding states have seen a surge in marijuana-related trafficking activity. Dealers and traffickers are openly bragging about how they have been able to smuggle state-sanctioned marijuana out of Colorado. The underground market has thrived under Amendment 64, and ever-potent gummy bears, candies, and concentrates have flooded the national marijuana market.
“We don’t think people should go to jail for smoking a joint, but we also don’t want to create Big Tobacco 2.0. Although states should be able to determine appropriate penalties, we need uniform federal drug laws regarding legalization.
“We hope Attorney General-nominee Loretta Lynch will seriously consider the ramifications of ignoring federal law, and will understand that creating a Big Marijuana industry serves no one except the profiteers who hope to follow in Big Tobacco’s footsteps.”
Source: KEVIN@LEARNABOUTSAM.ORG 5th March 2015
It is widely known that drug legalizers will not be content with the legalization of pot. Their ultimate goal is the legalization of all drugs.
In using a few of their favourite tactics, they now argue that:
LSD and other psychedelic drugs are “safer than alcohol”
LSD and other psychedelics have “positive psychological benefits” and the ability to “defeat addiction”
The prohibition of psychedelics is a violation of “human rights” (including the right to “belief and spiritual practice, full development of the personality, and free-time and play.”
In other words – safer than alcohol, with medical properties, and fun.
According to long-time legalization advocate David Nutt, speaking at a briefing in London:
“We’ve banned research on psychedelic drugs and other drugs like cannabis for 50 years. Truly, in terms of the amount of wasted opportunity, it’s way greater than the banning of the telescope. This is a truly appalling level of censorship.”
The movement to legalize drugs follows a predictable pattern that must be recognized.
1. Ignore existing laws
2. Decriminalize use
3. Open the door for medi-pot (CBDs)
4. Expand medical use to include everything under the sun
5. Full legalization of marijuana for recreational use
Despite overwhelming evidence of their intent, states seems to be following this pattern as if the pro-drug forces are interested in only the next step, when in fact their long game is “all drugs, by anyone, and all the time.”
This surrender to the drug culture, where we allow a very small minority of the population to dictate policy, laws, and even constitutions, is creating disastrous results and permanent damage to society.
Drug education works when we do enough of it. Surrender is not an option.
Source: Letter from Monte Stile to DrugWatch International 7th March 2015
Can you put two and two together? Have a try. The authorities, and most of the media, cannot.
Did you know that the Copenhagen killer, Omar El-Hussein, had twice been arrested (and twice let off) for cannabis possession? Probably not.
It was reported in Denmark but not prominently mentioned amid the usual swirling speculation about ‘links’ between El-Hussein and ‘Islamic State’, for which there is no evidence at all.
El-Hussein, a promising school student, mysteriously became so violent and ill- tempered that his own gang of petty criminals, The Brothers, actually expelled him. Something similar happened in the lives of Lee Rigby’s killers, who underwent violent personality changes in their teens after becoming cannabis users.
The recent Paris killers were also known users of cannabis. So were the chaotic drifters who killed soldiers in Canada last year. So is the chief suspect in the Boston Marathon bombings of April 2013.
I might add that though these are all Muslims, who for rather obvious reasons are to be found among the marginalised in Europe and North America, it is not confined to them.
Jared Loughner, who killed six people and severely injured Congresswoman Gabrielle Giffords in Arizona in 2011, was also a confirmed heavy cannabis user. When I searched newspaper archives for instances of violent crimes in this country in which culprits were said to be cannabis users, I found many.
One notable example was the pointless killing of Sheffield church organist Alan Greaves, randomly beaten to death by two laughing youths on Christmas Eve 2012. Both were cannabis smokers.
By itself, the link is interesting. I wonder how many other violent criminals would turn out to be heavy cannabis users, if only anyone ever asked. But put it together with The Mail on Sunday’s exclusive story last week, showing a strong link between cannabis use and episodes of mental illness.
And then combine it with the confessions of two prominent British Left-wing figures, the former Tory MP and BBC favourite Matthew Parris, and Channel 4 news presenter Jon Snow, who both tried ‘skunk’ cannabis (by far the most commonly available type in the Western world) for a TV documentary.
Mr Parris wrote: ‘The effect was stunning – and not (for me) in a good way. Short-term memory went walkabout. I would forget what I was talking about even while talking. I became shaky. Time went haywire.’
But immediate effects are one thing. What about long-term use? Mr Parris recounted that he had ‘too many friends’ for whom cannabis had seemed destructive. He quoted one as saying: ‘I think it changed me permanently as a person.’
He said his mainly socially liberal friends, including health workers, generally agreed that ‘heavy use of cannabis, particularly skunk, can be associated with big changes in behaviour’.
Jon Snow said simply: ‘By the time I was completely stoned, I felt utterly bereft. I felt as if my soul had been wrenched from my body.
‘There was no one in my world. I was frightened, paranoid, and felt physically and mentally wrapped in a dense blanket of fog. I’ve worked in war zones, but I’ve never been as overwhelmingly frightened as I was when I was in the MRI scanner after taking skunk. I would never do it again.’
This is not some mild ‘soft’ thing. It is a potent, frightening mindbender. If it does this to men in late middle age who are educated, prosperous, successful and self-disciplined, what do you think it is doing to all those 13-year-olds who – thanks to its virtual decriminalisation – can buy it at a school near you, while the police do nothing?
And yet it is still fashionable in our elite to believe that cannabis should be even easier to get than it already is.
It is hard to think of a social evil so urgently in need of action to curb it. Why is nothing done? Need you ask?
Source: http://hitchensblog.mailonsunday.co.uk/2015/02
The last time Derrick Bergman came to Amsterdam to buy cannabis, he did so behind a locked door with a long, thick curtain obscuring his activity from the canal-lined residential street outside, in the quiet Lastage neighborhood. The secretary of the Netherlands’s Union for the Abolition of Cannabis Prohibition, Bergman comes here to weekly gatherings of a two-month-old—and seriously clandestine—“cannabis social club” called the Tree of Life, because it’s the only place in town he can find one of his favorite strains: Super Silver Haze.
Since 1976, authorities across the Netherlands have chosen to openly ignore that cannabis use is illegal here, and they prosecute no one in possession of less than five grams of marijuana for personal use. The policy, called gedoogbeleid, is known as the “Dutch model,” and it’s why hundreds of “coffee shops” sprung up across Amsterdam and the Netherlands, luring marijuana connoisseurs from across the globe to one of the few places they could roll and smoke a joint without fear. But that’s no longer the case.
Cannabis with more than 15 percent of the THC that makes it intoxicating is now under consideration to be reclassified as one of the “hard drugs” that come with stiff penalties. The government has also forced coffee shops where marijuana is sold to choose between alcohol and pot, prompting many to choose the former. Amsterdam once played host to nearly 300 coffee shops, of more than 1,000 scattered across the country. There are now fewer than 200 in the city and only 617 nationwide. While it’s always been illegal to grow marijuana in the Netherlands, authorities passively allow coffee shops to sell weed, often pretending not to know where the shops’ cannabis comes from.
But no longer. New laws target even the smallest of marijuana growers in Holland. In the past, people could grow up to five plants without fear of retribution. In 2011, the government issued new police guidelines and declared anyone who grew with electric lights, prepared soil, “selected” seeds or ventilation would be considered “professional.” It’s a significant change, as professional growers risk major penalties, including eviction and blacklisting from the government-provided housing in which more than half of the country’s citizens reside.
The result: Coffee shops are increasingly buying buds from criminal organizations willing to absorb the risk of prosecution by growing large amounts of cannabis in shipping containers buried underground, with little regard for quality or mold abatement. “It’s amazing how bad the quality has become,” says Bergman. “And the price is up. It’s what we’ve all predicted.”
That’s why Bergman travelled from his native Eindhoven to Amsterdam on a recent Monday, both to convene with other activists and to pick up five grams (the legal limit) of Super Silver Haze. Because the club is not-for-profit, its members can focus their efforts on finding and buying the best product and providing it to their members at much better prices than the coffee shops.
Modelled after a proliferation of similar establishments in Spain, the social clubs offer a new way to subvert the harsher laws. As in Holland, cannabis is illegal in Spain, but the government doesn’t prosecute anyone for personal consumption and there’s no implicit limit on the number of plants a person can grow, meaning the government doesn’t care if you grow one plant or 15. In fact, signs point to the government not caring at all. Barcelona is developing a reputation as “the new Amsterdam,” meaning the old Amsterdam is losing out on a significant source of revenue: drug tourists.
Inside an Amsterdam coffee shop called The Rookies, 22-year-old John Bell rolls a spliff of tobacco and a strain called Dutch Kashmir, which Bell can’t find in his native Liverpool. Bell has been to Amsterdam 11 times in the past three years, not because it’s hard to find weed in the U.K., but because the quality here is better. He wouldn’t visit the city at all if not for these coffee shops and Amsterdam’s quasi-legal cannabis, adding: “It’s too expensive to drink here, for a proper night out.”
Such drug tourists represent a major element of the city’s economy. The union of coffee shops in Maastricht commissioned research in 2008 that found foreign visitors to the city’s coffee shops spent money in other businesses there as well: €140 million (approximately $170 million) annually. It’s a significant number and one of the reasons government officials in Amsterdam have fought to keep the coffee shops from going out of business.
About a third of all visitors to Amsterdam step into one of its coffee shops at some point; nationally, the number is one in five. Banning such visitors would hit tourism revenues hard, chasing off travellers who tend to be well-behaved. “If you’re really a deadbeat hippie punk, a no-money kind of guy, how are you going to afford a ticket to Amsterdam?” Bergman says.
Cities such as Maastricht, on the other hand, have banned foreigners from coffee shops since 2005. The result, insists Bergman and other critics, is a proliferation of street dealers. People still come from neighboring countries to score marijuana, but now they stock up and head back home in a day, instead of spending any time in local hotels and restaurants.
How did Holland get here? Some trace the backlash to 9/11. The world’s global panic about terrorism in the wake of the attacks on New York City and Washington led to a surge in the power of conservative political parties in places as far away as the Netherlands. Ever since Holland’s People’s Party for Liberty and Democracy began to consolidate influence here, its leaders have pushed for zero tolerance drug laws. “Our last prime minister [Jan Peter Balkenende] believed in his heart that weed comes from Satan,” says Mila Jansen, a legendary figure in Amsterdam, who once invented a way to make hash in a washing machine.
Other factors influencing the government crackdown are pressure from outside nations, especially France, which has pushed the International Narcotics Control board to sanction Holland for violating international treaties on drug laws with its permissive pot policy. Ironic, argues Bergman, because the rate of marijuana use is twice as high in France as it is in the Netherlands, and Holland has one of the lowest number of drug-related deaths in Europe.
“Hard drugs are still illegal in Holland, but we also see that there are still many people who want to try drugs on occasion,” said the city’s mayor, Eberhard van der Laan, in a statement provided to Newsweek. “This is a reality we cannot ignore. And this is one of the key principles to our country’s drug policies: Drug use is first and foremost an issue of public health. By not focusing on the criminal aspects of drug use, as is the case in many other countries, we can be more effective when it comes to informing the public, testing drugs and prevention.”
Unfortunately, van der Laan’s federal counterparts don’t agree. They also don’t see that prohibition amounts to little more than, as they say here, “mopping with the tap on.”
Now, activists like Bergman are trying to convince Holland to consider the American model—the legalization and regulation of all components of marijuana cultivation and sale. Citing Oregon’s law, which allows residents to grow as many as four plants, Bergman says: “I’m sort of jealous.”
That’s because America seems to be learning from Holland’s mistakes. Holland’s passive-aggressive policy doesn’t stop illicit activity or drug tourism or make anyone safer, say activists: It actually has the reverse effect. Quasi-legalization leaves too many entry points for criminals to line their own pockets from the drug trade. State by state, the U.S. is legalizing pot with initiatives that clearly spell out who is allowed to manufacture, distribute and consume it. That’s the key to a successful policy, and it’s one Dutch activists are now working to implement in their own country, before things swing too far the other way.
This article appears in the latest Newsweek Special Edition, “Weed Nation: Is America Ready For a Legalized Future?” by Executive Editor Jeff Ashworth of Topix Media Lab.
Source: http://www.newsweek.com/marijuana-and-old-amsterdam- 22nd Feb.2015
Risk of developing psychosis up to five times greater for those who smoke ‘skunk’ cannabis every day


One in four new cases of psychotic conditions such as schizophrenia could be the direct result of smoking extra-strong varieties of cannabis, a major new study concludes.
The finding suggests that about 60,000 people in Britain are currently living with conditions involving hallucinations and paranoid episodes brought on by abuse of high-potency cannabis, known as skunk, and more than 300,000 people who have smoked skunk will experience such problems in their lifetime.
The six-year study, the first of its kind in Britain, calculates that daily users of skunk are five times more likely to suffer psychosis than those who never touch it.
Psychiatrists said there is now an “urgent need” for a drive to educate the public about the risks involved with the substance. It is believed that even newer varieties, some of them more than twice as potent as those currently available on British streets, have already been developed in the Netherlands.
The findings reopen the debate about the classification of cannabis as an illegal drug, with some supporters of liberalisation now considering tougher restrictions on some varieties.
Chris Grayling, the Justice Secretary, said the findings underlined arguments against decriminalisation. Norman Baker, the Liberal Democrat former Home Office minister who has called for drug laws to be relaxed, said that there may be a case for giving skunk a new classification. The study, by researchers from the Institute of Psychiatry, Psychology & Neuroscience at King’s College London, is due to be published in the journal Lancet Psychiatry later this week.
They studied almost 800 working-age adults from one area of south London, half of whom had been recently treated for a psychotic episode for the first time. The incidence of schizophrenia in the area has doubled since the mid-Sixties, a trend widely thought to be linked to drug use. Cannabis use in the UK overall has fallen by about 40 per cent in the past decade but, for those using it, the typical potency has increased sharply in that time.
Levels of tetrahydrocannabinol (or THC), the main psychoactive compound, are arbout 15 per cent in skunk, compared with about four per cent in traditional “hash” cannabis.
The study concluded that the strength of cannabis and the frequency of use play a crucial role in determining the mental health risks.
“Compared with those who never used cannabis, individuals who mostly used skunk-like cannabis were nearly twice as likely to be diagnosed with a psychotic disorder if they used it less than once per week, almost three times as likely if they used it at weekends, and more than five times as likely if they were daily users,” the paper notes. It found that skunk use was the “strongest predictor” of psychotic illness in those studied and that 24 per cent of new cases in the area could be attributed to skunk.
It also noted that those who started smoking cannabis before the age of 15 had higher risk of developing psychotic disorders than others. “Our findings show the importance of raising public awareness of the risk associated with use of high-potency cannabis, especially when such varieties of cannabis are becoming more available,” the paper concludes.
“The worldwide trend of liberalisation of the legal constraints on the use of cannabis further emphasises the urgent need to develop public education to inform young people about the risks of high-potency cannabis.” Dr Marta Di Forti, the lead author, said the significance of how regularly people smoked cannabis has often been overlooked in day-to-day treatment. “When a GP or psychiatrist asks if a patient uses cannabis it’s not helpful – it’s like asking whether someone drinks,” she said. “As with alcohol, the relevant questions are how often and what type of cannabis.”
Prof Sir Robin Murray, professor of psychiatric research at King’s, said: “It is now well known that use of cannabis increases the risk of psychosis. However, sceptics still claim that this is not an important cause of schizophrenia-like psychosis. “This paper suggests that we could prevent almost one quarter of cases of psychosis if no-one smoked high potency cannabis.” He added: “Education is the important thing – people need to know the risks of regular use of high potency cannabis.
Mr Grayling said: “Far too many of those who end up in our criminal justice system have got drug and mental health problems. “It’s clear to me that drug addiction is at the root of a large proportion of crimes in the UK and that it causes mental health problems which are all too apparent in our prisons. “That’s why mental health will be our next big reform focus – but it’s also why decriminalisation is not the right option.”
Mark Winstanley, the chief executive of Rethink Mental Illness, said: “Essentially, smoking cannabis is like playing a very real game of Russian roulette with your mental health. Reclassifying cannabis isn’t the answer.” A Home Office spokesman said: “Our approach remains clear: we must prevent drug use in our communities and help dependent individuals through treatment and recovery, while ensuring law enforcement protects society by stopping supply and tackling the organised crime that is associated with the drugs trade.”
Edward Boyd, deputy policy director of the Centre for Social Justice, the think-tank founded by the Work and pensions Secretary Iain Duncan Smith, said: “This study provides yet more evidence that liberalising drugs laws is not the way to go. “It will only lead to more people suffering from the misery of drug addiction, which, as this study shows, could well include psychosis. “Instead, politicians should focus on improving the UK’s poor level of treatment for addicts by investing in residential rehabilitation.”
Marjorie Wallace, chief executive of the mental health charity SANE, said: “This is yet another study that should worry all those who deny any direct link between skunk, a potent cannabis derivative, and psychotic breakdown. “While the scientists and politicians debate, we face the daily heartbreak of young people whose minds and thoughts have been altered through continued use and whose families feel helpless.
“What we need is a strong, uncompromising message so that parents, teachers, the police and young people themselves know that a significant percentage who take skunk risk acute, and in some cases lasting, mental illness.”
Source: http://www.telegraph.co.uk/news/health/news/11414605 26th Feb. 2015
US News and World Report reported today that George Soros plans to invest an additional $50 million to fundamentally change the way drugs are dealt with in society. Along with the support of the ACLU and other pro-pot groups, the goal is to decriminalize all drug use – paving the way to release thousands of drug dealers from prison.
This follows California’s disastrous passage of Proposition 47. Now they want to replicate this in other states.We know how the country has fared in following California’s example on drug policy.
As the commercialization of pot expands exponentially, the pro-pot groups have grown in power and influence. The only way to stop this madness is for the federal government to enforce laws relating to the large-scale manufacturing and sale of drugs. It is the inaction of the US Department of Justice that has allowed states to join in a drug trafficking conspiracy that disguises drug proceeds as “taxes.” It is a national tragedy. Monte Stiles
Pot Legalization: Gateway to What?
Advocates look to further reduce drug-related arrests, incarceration.
Buying marijuana is now about as easy as shopping for liquor in Denver and Seattle. Soon, four states will regulate and tax sales of joints and pot brownies, and drug policy campaigners see deeper reforms on the horizon. Flush with new funding and optimistic that Americans have turned a page, the American Civil Liberties Union plans to lead the charge. “What the marijuana legalization votes tell us is the door is open to reconsidering all of our drug laws,” says Alison Holcomb, national director of the ACLU’s new nationwide campaign against “mass incarceration.”
A $50 million grant from billionaire George Soros’ Open Society Foundations will fund the effort.
Holcomb wrote Washington state’s pot legalization initiative, which voters approved in 2012 along with a Colorado ballot measure. Residents of Alaska, Oregon and the District of Columbia voted last week to follow.
“These votes are not about whether or not voters think marijuana is wonderful and that people should be using marijuana,” Holcomb says. “Instead they are really rejections of the laws that have existed for the last four decades.” Marijuana continues to be illegal under federal law, but the Obama administration has allowed broad leeway for states to allow recreational sales, despite President Barack Obama’s reluctance to administratively change the 1970 congressional classification of pot as among the most dangerous drugs.
The legalization votes, Holcomb says, “are a harbinger of a deeply felt desire on the part of the American voters to do something completely different.” The ACLU plans to stay on the sidelines of future pot legalization campaigns – already supported by well-organized groups plotting about a half-dozen ballot campaigns in 2016 – and to instead pour resources into less-advanced fights for criminal justice reform.
One model the group hopes to replicate is California’s Proposition 47, approved by 58 percent of state voters last week to lower penalties for drug possession and other nonviolent crimes. The proposition allows for retroactive reclassification of felony convictions as misdemeanors and sentencing reductions for current inmates.
Lenore Anderson, a co-author of Proposition 47 and executive director of Californians for Safety and Justice, says she’s aware that people from other states are seeking to replicate the successful amendment. “When it comes to criminal justice and drug policy, Americans are thinking differently about these issues,” she says. “The main message for policymakers is some of the old ways of thinking around prison-first policies and using the criminal justice system to deal with something like drug addiction is something the public doesn’t think is wise anymore.”
Holcomb says the ACLU plans to support measures similar to Proposition 47 in 2016, and – ideally – measures that would not only de-felonize but also decriminalize drug possession, meaning eliminating criminal penalties like jail time for drugs other than marijuana. She says, however, the group will not press to regulate the sale of all drugs like marijuana.
“We would love to be able to have ballot initiatives in a number of states that may look very similar to Proposition 47,” Holcomb says. “Hopefully we will be able to find states where we can go further and say, ‘Let’s decriminalize the possession of drugs and let’s talk about what we can do to address drug use and abuse.’”Most Americans behind bars are there for violating state laws, so that’s where the ACLU plans to focus.
Ethan Nadelmann, executive director of the Drug Policy Alliance, says his organization would support decriminalization ballot measures in any state where polling indicates majority support. But, he says, broad drug decriminalization probably lacks such support in any state-level jurisdiction aside from the District of Columbia. Nadelmann says the pot legalization wins are “creating a sense of momentum, but with the other drugs it’s really about reducing dependence on arrest and incarceration.” He doubts there will be majority support in the near future for legalizing drugs other than marijuana, with the possible exception of certain hallucinogens.
Nadelmann’s group, a major national leader on marijuana legalization alongside the Marijuana Policy Project, has smaller steps in mind for drug policy reform. It supported an initiative approved this month by New Jersey voters to reform the state’s bail system so that low-income residents arrested on nonviolent charges be released pending trial and plans to push for Good Samaritan laws to encourage the reporting of drug overdoses and, ultimately, the establishment of harm-reduction measures such as safe injection sites.
“Drug policy reform has evolved from being the black sheep of criminal justice reform to being the cutting edge of criminal justice reform,” he says. “Basically, a majority of Americans clearly believe there are too many people behind bars for nonviolent, low-level drug offenses.”
About one in every 200 Americans was arrested for an alleged drug-related offense in 2013, according to data released Monday by the FBI. About 46.2 percent of those 1,501,043 drug-related arrests were for marijuana. The U.S. famously has the largest prison population in the world. A September report from the Justice Department’s Bureau of Justice Statistics reports about 16 percent of the 1,314,900 inmates warehoused in state facilities in December 2012 were convicted of drug crimes. About 51 percent of the 193,775 federal prison inmates in September 2013 were jailed on drug charges.
State-level action isn’t the only front for drug policy reform. There’s federal-level sentencing and criminal justice reform efforts, too, and the ACLU hopes to help make the issue a presidential election year issue in 2016.
Localities are also creeping toward reform. New York City’s government announced Monday a discontinuation of using arrests to punish citizens caught with small amounts of pot – opting instead for court summons – following the July decision by Brooklyn’s district attorney to stop prosecuting most small-scale pot cases. District of Columbia voters’ decision to legalize weed will likely test the congressional waters for more permissive policies early in 2015.
In addition to pushing particular reforms, the ACLU campaign will seek to assemble better data. Some of the group’s campaign will focus on non-drug offenses. As leading drug reform campaigners seek to either take a sledgehammer or chisel to current U.S. drug laws, idealists foresee a not-too-distant future where a comprehensive tax-and-regulate structure is established for most currently illegal drugs, a scenario that seemed implausible for marijuana not long ago.
“Legalizing all drugs and establishing a controlled and regulated market is what would really, really put the cartels out of business,” says Sean Dunagan, a former Drug Enforcement Administration intelligence specialist. Dunagan worked five years on the front lines of the war on drugs in Guatemala and Mexico and came to the realization it’s impossible to smash the black market for illegal substances or permanently drive down drug consumption.
“You can get cocaine in just about any school, there are heroin arrests in small towns across the country,” he says. “There’s really no way to arrest and incarcerate our way out of the problems associated with illegal drugs. It doesn’t work and if it doesn’t work, common sense would dictate we look for alternatives.” Dunagan, now affiliated with the group Law Enforcement Against Prohibition, says the small user populations for drugs such as cocaine compared with marijuana makes it difficult to see how significant public pressure for legalization would mount in the near term, but he’s confident the day will come. “For the government to do something that is so ineffective, and so costly and so deadly, I can’t believe that that policy would continue to exist in perpetuity,” he says.
Source:; e-mail from Monte Stiles, DrugWatch International Nov.2014
By John P. Walters and David W. Murray
Mayor de Blasio seems to believe that law enforcement doesn’t so much protect minority communities as harm them. His administration’s latest effort will have the NYPD reduce enforcement of marijuana laws — a move toward legalization under the banner of social justice. The push for marijuana legalization begins with the claim that the drug is essentially benign or even beneficial.
It follows that arresting people for using marijuana is unjust, with possession arrests damaging lives, filling prisons and wasting police resources. Worse, the enforcement of marijuana laws causes the disproportionate arrest and incarceration of African-American males and represents an assault on civil rights, if not a “war” on communities of color.
The claims are wrong:
Actual risk of arrest while using marijuana is stunningly low. Roughly 5 percent of US arrests in a given year are for marijuana possession. We calculate about one arrest for marijuana possession for every 34,000 joints smoked.
Drug arrests simply aren’t a significant portion of law-enforcement activity, and possession arrests for marijuana certainly don’t fill our prisons. A 2008 study by the Bureau of Justice Statistics found that fewer than 0.3 percent of those incarcerated in state prison (which is where most US inmates are incarcerated) are there for simple marijuana-possession offenses — and many of those have just “pled down” from more serious offenses.
Are African-Americans targeted victims of the drug laws? No — race is not the driver of “disparate impact.”
First, African-American drug-use rates are likely higher than most studies assume: Researchers usually rely on surveys of drug use, but such surveys undercount dropouts, the homeless and the imprisoned — populations in which African-Americans are disproportionately represented and drug use is high.
Second, African-Americans are arrested for drug trafficking more often than whites — crimes that more commonly lead to prison time.
Third, African-American drug use often occurs in areas with intensive policing, such as urban street corners, which means that the risk of arrest for African-Americans is higher than for whites, whose use of drugs is typically less conspicuous.
Fourth, it’s not just drug-related crime where we see racial disproportions in arrests and incarcerations: The same is true for almost all crimes. Eliminating drug-law enforcement would change little.
In short, Vanita Gupta, the acting assistant attorney general for the Justice Department’s Civil Rights Division, is simply wrong to say that the “war on drugs has been a war on communities of color” — unless she’s willing to argue that virtually all efforts to combat crime are wars on communities of color.
That is, the disproportions of arrests, incarcerations and victimization that afflict many African-American communities are a direct consequence of the disproportionate crime (and devastating suffering from crime) that plagues those communities.
Responding to this reality in the 1980s, then-Sen. Joe Biden led the bipartisan effort to pass tough new laws against cocaine and crack. Lawmakers have since made efforts to ensure the laws are more fair, but we shouldn’t forget how bad the epidemic was, and how law enforcement worked to protect victimized communities.
The problem isn’t the presence of the laws against drugs. Rather, the problem is the presence and use of illegal drugs.
Drug use is strongly associated with failure to finish high school. It has crippling effects on securing employment or joining the military — critical pathways out of poverty.
Poor cognitive performance linked to drug use most affects those who already struggle to succeed because of family disruption, poverty, disabilities and discrimination.
Does any serious person believe young men and women of all races and backgrounds will be better off with more drug use? Where we find racial injustice or failed policies, we should correct them. But abandoning law enforcement through drug legalization presents a grave danger to all young Americans.
John P. Walters and David W. Murray direct Hudson Institute’s Center for Substance Abuse Policy Research. Both served in the Office of National Drug Control Policy.
Source: http://nypost.com/2014/12/16/drug-enforcement-is-not-racist/
A large observational study of more 2000 participants who were admitted to specialized Veterans Administration treatment programs for PTSD showed that those who never used marijuana had significantly lower symptom severity 4 months later than those who continued or started use after treatment. Veterans who were using marijuana at treatment admission but quit after discharge (“stoppers”) also had significantly lower levels of PTSD symptoms at follow-up.
On the other hand, the highest levels of violent behavior were found in the so-called “starters,” those who were not using the substance at admission but who started use after discharge.
At the American Academy of Addiction Psychiatry (AAAP) 25th Annual Meeting, lead author Samuel T. Wilkinson, MD, from the Yale University School of Medicine, in New Haven, Connecticut, told conference delegates that the findings suggest marijuana nullifies the benefits of intensive PTSD treatment.
“This wasn’t a randomized controlled trial. But at least in this study, we found that marijuana is not associated with improvement in PTSD and that initiating marijuana was associated with worsening outcomes in a number of measures,” said Dr Wilkinson.
Little Substantive Evidence
Despite the fact that a number of states have approved the use of medical marijuana for PTSD, there’s little evidence to support its use for treatment of the disorder.
“There have been a few longitudinal assessments, but no randomized controlled trials showing efficacy and safety,” added Dr Wilkinson.
The investigators evaluated data from the Northeast Program Evaluation Center for veterans who were admitted across the United States between 1991 and 2011 into specialized intensive PTSD treatment programs lasting a mean of 42.5 days.
A total of 2276 representative veterans were included in this analysis. They were split into four groups: in addition to the marijuana starters (n = 831), those with no use at treatment admission or after discharge were placed in the “never used” group (n = 850); those using at admission and after discharge were placed in the “continuing use” group (n = 296); and those who quit using after treatment were in the “stoppers” group (n = 299).
All were evaluated at admission and at a follow-up 4 months after discharge. Measures used included the short version of the Mississippi Scale (MISS) to assess PTSD symptom severity, the drug and alcohol subscales of the Addiction Severity Index (ASI), and reports of violent behavior.
Results showed that use of marijuana was significantly associated with higher PTSD symptom severity, as well as higher levels of violent behavior and alcohol and drug use.
Scores on the MISS showed that all groups except the starters had at least some improvement. However, the lowest levels of PTSD symptoms at the 4-month follow-up were in the marijuana stoppers, with a score decrease of 7.9% (P < .0001 vs the continuing users and the starters), and in the never users, with a score decrease of 5.5% (P < .0001 vs the starters).
Surprise Finding
Although there were changes in violence scores in all three groups, improvement was significantly less in the starters than in the other 3 groups (P < .0001 for all three comparisons). “This was a surprise because generally, marijuana is not thought to be associated with violence. There’s been a little bit of literature investigating this, but this was interesting,” said Dr Wilkinson.
The starters also had greater severity in scores on both the ASI drug use and alcohol use subscales vs the other three groups (P < .0001 for all).
On the other hand, the stoppers had significantly lower severity scores on the drug use subscale (P < .0001 vs the other 3 groups) and lower alcohol subscale scores (P < .0001 vs continuing users; P < .001 vs never users).
“This showed that those who started marijuana did turn to other drugs to cope with residual PTSD symptoms, which is to be expected,” Dr Wilkinson said. “However, there was no evidence that those who stop cannabis use turn to other drugs or alcohol.”
During the Q&A session after his presentation, an audience member pointed out that there was no implication that cannabis drove PTSD severity and asked whether it could just be that the patients with more severe symptoms use more cannabis.“There wasn’t a sense of that from these data,” replied Dr Wilkinson. However, he added that they found only an association and not causation, because the study was not prospective or randomized.
“When we looked at a different analysis, there was a dose response. Those who used more marijuana or who had greater change in marijuana use had worse PTSD symptoms,” he said.
When another attendee mentioned that she had seen violent behavior in some veterans who use marijuana and have traumatic brain injuries (TBIs), Dr Wilkinson noted that the investigators did not evaluate whether any of the study participants specifically had a TBI.
A Band-Aid Solution?
Session moderator Carla Marienfeld, MD, told Medscape Medical News that public perception has been that marijuana soothes those with PTSD.
“Addiction psychiatrists struggle a lot with how to communicate with our patients about this. People assume that there aren’t a lot of risks, but there are some papers starting to show that there really are,” she said.“Most people assume things based on their own experience. So when you talk to patients, they often say, ‘it’s the only thing that helps me sleep’ or ‘it’s the only thing that calms me down.’ But when you actually start looking into the symptoms of whether or not they get better with marijuana use, I don’t think studies, at least with these initial data, are going to bear that out.”
Although Dr Marienfeld, like Dr Wilkinson, is from the Yale University School of Medicine, she was not involved with this research. She noted that it could be that cannabis is acting as a Band-Aid instead of being a long-term solution.“Marijuana use may make patients feel better for the short term, and we need to look at that. Does it make things better for a few hours and then it gets worse the next day? That would be an important study to understand,” she said.
She added that because Dr Wilkinson presented an association study, “there’s not really a take-away for clinicians yet. But I think it’s important for them to bear this in mind and watch for this kind of data.”Dr Wilkinson reports having received a past grant from the American Psychiatric Foundation/Janssen through Yale University for a project involving electroconvulsive and cognitive-behavioral therapies.
American Academy of Addiction Psychiatry (AAAP) 25th Annual Meeting: Paper presentation 5, presented December 6, 2014.
Health minister seeks court ban amid fears new cannabis-laced electronic cigarettes could incite further use of drug

Cannabis-laced electronic cigarette
Recreational use of cannabis is illegal in France.
France has sought to stamp out a new electronic cigarette containing cannabis, launched on Tuesday with the claim that it provides all of the relaxation but none of the mind-altering effects of the drug.
The health minister, Marisol Touraine, said the product would incite the consumption of cannabis and she intended to approach the courts to ban it. “I am opposed to such a product being commercialised in France,” she told RTL radio.
The product was launched by a French-Czech company called Kanavape which said it hoped to offer millions of people a legal and flavourful way to consume cannabis.
Smoking e-cigarettes, or vaping, is fashionable in France, and while people have long since figured out how to doctor them to smoke marijuana – as evidenced by hundreds of YouTube tutorials on the subject – Kanavape claims its product is legal.
The company extracts Cannabidiol – a compound in cannabis that does not contain the mind-altering THC ingredient – from hemp, a variety of cannabis grown for fibre and seeds.
The hemp is grown on farms in France, Spain and the Czech Republic without chemicals or fertiliser, the company claims on its website. “Kanavape provides you with a unique experience. Cannabidiol is a non-psychotic component of hemp. It does not have euphoric effects but helps you feel more relaxed,” it says.
Recreational use of marijuana is illegal in France, but the country allows the drug’s active ingredients to be used for medical purposes.
Source: The Guardian, Tuesday 16 December 2014 13.02 GMT
Two dozen doctors in Arizona are responsible for making medical marijuana available to more than 34,000 patients according to a new report, with several writing recommendations at the rate of one an hour for every business hour of the day.
The study being released today by the Arizona Department of Health Services finds these 24 doctors, most of them naturopaths, wrote close to two-thirds of all the recommendations in the most recent fiscal year.
State Health Director Will Humble said his agency has reported 30 of these doctors to their state licensing boards. But Humble said these were doctors where there was clear evidence that they were not following laws which require them to check a website run by the Arizona Board of Pharmacy to see whether their patients had prescriptions for other drugs. He does not know whether the boards ever followed up.
“One physician, a naturopath, over that last fiscal year, did almost 3,000 certifications,’’ Humble said. `It does make you raise an eyebrow.”
Humble said he has no independent authority to investigate whether the doctors that are writing out the lion’s share of the recommendations are in fact complying with requirements that they adequately examine patients to ensure that marijuana is appropriate.
The new report also finds that the highest concentration of medical marijuana users is in Yavapai County, with close to 1.5 percent of the total population there having a state-issued card entitling them to obtain up to 2.5 ounces of marijuana every two weeks. Gila County was a close second. At the other extreme, 0.3 percent of Yuma County residents are medical marijuana users.
Source:http://www.eastvalleytribune.com/arizona/politics/article_9140c3c3-34b7-5ac7-a46f-969eb5569091.html 13th Nov.2014
Thanks to Derek in Washington who forwarded this important news story on a Washington sheriff who taped an ad for the pro-legalization campaign in neighbouring Oregon. The sheriff made what seemed to be grossly inaccurate or misleading claims about the state of legalization in Washington. King 5 News ran a fact check on the DUI portion of his statement.
Other claims made by the sheriff (along with the real facts).
1. “Month by month tax dollars are going to schools and police, not drug cartels.”
There is no money for schools (except 3/10 of 1% of second tier funding for the Building Bridges program at OSPI).
There is no funding for police, sheriffs, or state patrol. Enforcement funding exists for LCB enforcement officers–about 12 statewide.
2012 NW HIDTA report says cartels are staying in WA and modifying their business model accordingly. They are now positioned to compete in the only remaining marketplace where MJ is illegal–young people under age 21.
2.“Wasteful arrests are way down.”
Yes, marijuana is no longer illegal for adults over 21. Of note is that there was not, and is not, anyone in jail for simple possession. Of the 8 cases found in 2012 to be in jail for possession, all had plead down from more serious crimes.
Saying arrests are wasteful implies that enforcement is not appropriate. However the law is clear about it remaining illegal for youth and gifting MJ is a felony. Also, law enforcement is now burdened with the additional, unfunded responsibility to police a new addictive commodity industry including DUI’s, gun violence when grows are burgled, and smoking in public. Of note is that in many jurisdictions, public smoking, and underage use for that matter, is not being enforced and sending a dangerous message to youth.
2. “DUI’s are down.”
Total DUI’s may be down thanks to Target Zero Task Forces and enforcement efforts, but, according to data adapted from the State Patrol/State Toxicologist, total driving cases testing positive for delta-9 THC increased by 33% the year after legalization, after decreasing by 7% the year prior.
3. “Drug prevention programs are getting funding.”
There has been no funding from I-502 to DSHS’s Division of Behavioral Health and Recovery which is responsible for community-based prevention efforts under 502. Nor has the Department of Health received any direct support from 502 proceeds. Funding has yet to “roll in” from marijuana sales and the amount that will is unknown.
Source: http://www.king5.com/story/news/local/2014/10/23/fact-checking-urquhart-marijuana-ad/17807305/
Over at Ezra Klein’s new site, Vox.com, German Lopez has an article claiming to show that Colorado’s recent marijuana legalization experiment hasn’t increased crime rates in Denver. In contrast, when we actually look at the raw data Lopez uses, the message isn’t so clear. In fact, using Lopez’s own methods, we might conclude pot legalization has dramatically increased crime in Denver.
Lopez claims that “three months into its legalization experiment, Denver isn’t seeing a widespread rise in crime.” To reach this conclusion, Lopez uses Denver’s crime data (available here) for the months of January and February in 2013 and 2014. When I look at the data, I see some potentially different findings.
Over the first two months of 2014, “simple assaults” in Denver are up an astonishing 70% over the same timeframe in 2013. The crime of “intimidation” is up 86%, and all “crimes against persons” have increased 32% compared to 2013. But the real changes are evident in the “all other offenses” category. Here we see that “disorderly conduct/disturbing the peace” has increased 1,144% (from only 18 offenses in 2013 to 224 in 2014), “family offences/nonviolent” are up 97%, “liquor law/drunkeness” is up 1,150%, “violation of a restraining/court order” increased 87%, “criminal trespassing” is up 339%, and the “all other offenses” subcategory have increased 400%.
Of course there is also data available back to 2009 that illustrates the anomalously high incidence level for these offenses during the first two months of 2014 following marijuana legalization, as shown in the table below.

The number of offenses in each of these categories during January and February of 2014 are, by far, the highest over Denver’s available historical record, in some cases by more than an order of magnitude.
Source: Sierra Rayne www.AMERICAN THINKER 4th Sept. 2014
On March 10, a college student from Wyoming bought four marijuana cookies for herself and her three friends at the 16th Street Mall in Denver.
Late into the night, restless and exhibiting erratic behavior, 19-year-old Levy Thamba leapt over the fourth-floor railing of a Holiday Inn into the lobby. He was pronounced dead at 3:51 a.m. Thamba’s tragic death highlighted the deceptive nature of THC-infused foods: They affect the human body later in time after ingestion than smoked bud.
The case is not the only disturbing episode connected to marijuana edibles since Colorado opened up the market for legal recreational marijuana eight months ago. Some children have gotten their hands on edibles, and landed in the emergency room, while one man who allegedly killed his wife—and faces a first-degree murder charge—was said to have eaten pot candy beforehand. The incidents have prompted changes in marijuana policies that are intended to make edibles safer to consume, keep them away from minors, and educate Coloradans and visitors on the differences between marijuana food and pot that you smoke.
Eating an edible is not like taking a shot of whiskey or smoking marijuana, said Ron Kammerzell, senior director of enforcement with the Colorado Department of Revenue. “You need to give yourself enough time to make sure you are feeling the effects of marijuana before you consume additional edibles,” he said in a phone interview.
While the effects of smoked bud are rather immediate, edibles are deceptive because it can take hours to feel anything from the THC, the psychoactive ingredient in marijuana. Thamba, a native of Africa who was on spring break from Northwest College in Powell, Wyoming, may not have known that.
Bessie Gondwe, one of his college friends with whom he was staying at the Holiday Inn, told Denver police she had purchased the cookies and it was the first time she believed Thamba had ingested marijuana. During a search of the hotel room, police found wrappers with labels that identified the marijuana products as “Sweet Grass Kitchen, lemon poppy seed cookie.” Gondwe and another friend staying in the room with Thamba told authorities the college students had begun eating the cookies around midnight. Each of the four cookies contained 65 milligrams (mg) of THC, or the equivalent of 6.5 servings; an employee at the marijuana store advised the students that they should split the cookie into six pieces and eat one piece at a time, according to the police report.
But Thamba revealed he wasn’t feeling anything from the marijuana cookie so he ate the rest of the edible all at once, Gondwe told police. Later in the night, the police report detailed, Thamba exhibited strange behaviour—screaming, speaking in French, apologizing for criminal behaviour that he had not committed, smashing fixtures and finally jumping off the balcony.
Thamba’s autopsy report said the cause of death was the result of “multiple injuries due to a fall from a height” and listed “marijuana intoxication” as “a significant contributing factor.” The college friends weren’t aware that Thamba had consumed any alcohol or other drugs, and other than detecting THC in his system, the blood results revealed no other “positive findings of toxicological significance.”
Limiting THC in Each Edible
In the wake of his death, Colorado regulators have adopted rules that are designed to encourage marijuana edible companies to make pot treats that contain no more than 10 mg of THC. Under emergency rules that were adopted on August 1, if a marijuana edible is more than 10 mg and up to 100 mg, “you have to score it or demark it in such a way that it is intuitively obvious to the consumer how to break off a serving size of that edible,” said Kammerzell of the Colorado Department of Revenue.
State regulators also gave marijuana edible makers an incentive to make products containing no more than 10 mg. If they do so, their products will be tested for potency fewer times than other edibles. Even before the emergency rule was adopted, a number of manufacturers had moved toward individual serving sizes of 10 mg, Kammerzell said.
“There is no lethal dose for marijuana other than maybe a 500-pound brick of it falling on your head, but we don’t want people to have a bad experience or get to the point where they are not functional,” said Andy Williams, president of Medicine Man, a marijuana dispensary in Denver.
As part of a responsible vendor training program modeled after one administered by the state’s liquor enforcement division, it is expected that marijuana establishments will educate consumers on the differences between eating an edible and smoking marijuana.
Williams and the owner of a recreational marijuana dispensary north of Boulder said their employees, or budtenders as they are affectionately known, already warn customers about edibles – “We take the extra step at the counter to really educate people on how to use them safely, how to get familiar with the effect of edibles,” said Dylan Donaldson of Karing Kind, who estimated edibles constitute 30 to 40 percent of sales on an average day. “It is quite different. It’s a whole other beast.”
Protecting Kids from Inadvertent Consumption
That beast has sickened some kids in Colorado. Since recreational marijuana was legalized on Jan. 1, “Children’s [Hospital] Colorado has treated 13 children, six of whom became critically ill from edible marijuana,” said Natalie Goldstein, a spokeswoman with the hospital, in an email last month.
In a May interview with the Denver Post, Michael DiStefano, the medical director of the hospital’s emergency department, said a number of children who accidentally ingested marijuana had been admitted for sedation or agitation and one child suffered breathing problems that required a respirator.
Earlier this year, a 10-year-old boy in Greeley, Colorado admitted to selling marijuana to other students on the playground while another child came to school with a THC-infused candy bar, according to CBS4. The kids reportedly obtained the pot from home where it was purchased by their grandparents.
Edibles today hardly are limited to the marijuana brownies of the 1990s. Other than the THC, the treats are the same ones kids savor at home and school: cookies, gummy bears, Lollipops.
“In Colorado, there is almost no limit to what marijuana can be put into whether that is infused or baked or sprayed,” said Rachel O’Bryan of Smart Colorado, an organization that is dedicating to protecting Colorado youth and advocates for policies that limit early marijuana consumption. Said state Rep. Frank McNulty: “Many of these marijuana edibles look just like kids’ snacks.”
The Colorado Marijuana Enforcement Division requires that a seal be placed on packaging of marijuana products, but “that doesn’t mean anything to most kids or parents,” said McNulty, a Republican who represents Highlands Ranch, a suburb south of Denver.
Colorado lawmakers have moved to solve the problem. House Bill 1366, signed in May by Gov. John Hickenlooper, required that Colorado’s state licensing authority convene a stakeholder group to discuss recommendations on how to make edibles clearly identifiable.
Members of the working group include a wide range of interests from law enforcement representatives and a school resource officer to a marijuana baker and testing facility owner. An initial meeting was held on Aug. 1, and a second meeting is scheduled for Sept. 11 in Denver. Rules will be adopted no later than January 2016.
“It’s going to be a challenging topic for sure,” Kammerzell said. But the edibles rule, once implemented, could save Colorado kids from unnecessary trips to the ER.
Source: www.naturalproductsinsider.com 5th Sept. 2014
Top 20 Anti-Marijuana Crusaders Fighting Against Pot Legalization

NEW YORK (MainStreet) — Even as a marijuana legalization gains traction around the U.S. and the world, the anti-pot contingent soldiers on to promote its own agenda. These advocates are on a mission to keep marijuana illegal where it is, make it illegal where it is not and to inform the public of the dangers of marijuana legalization as they see it.
So who are these anti-marijuana legalization crusaders?
They come from different backgrounds. Some come from the business world. Two are former White House cabinet members. Another is an academic. Two are former ambassadors. One is the scion of a famous political family. Many are psychiatrists or psychologists. Others are former addicts. Still others are in the field of communications. Oh – one is a Pope.
They have different motivations. Some act because of the people they met who suffered from drug abuse. Others are staunch in their positions for moral reasons and concern for the nation’s future; still others for medical and scientific reasons.
Here is a list of the most significant:
1. Calvina Fay

Calvina Fay
Drug Free America Foundation, Inc. and Save Our Society From Drugs (SOS). She is also the founder and director of the International Scientific and Medical Forum on Drug Abuse.
She was a drug policy advisor to President George W. Bush and former Tennessee Governor Lamar Alexander. She has been a U.S. delegate and lecturer at international conferences.
President Bush acknowledged her efforts in drug prevention in 2008, and in 2009 she received the President’s Award from the National Narcotics Officers Associations Coalition.
She related during an interview that she became involved in the world of countering drug abuse as a businessperson. She started a company that wrote drug policy for employers, educated employees on the dangers of drugs and trained supervisors on how to recognize drug abuse. It was from this that she became aware of the gravity of the issue.
“People used to come to me to tell me they had a nephew or niece who had a drug problem,” Fay said. “This was when I realized how broad a problem this is. It became personally relevant at one point.”
President Bush acknowledged her efforts in drug prevention in 2008, and in 2009 she received the President’s Award from the National Narcotics Officers Associations Coalition.
I realized how broad a problem this is. It became personally relevant at one point.”
After she sold her company, she was approached by the DEA and the Houston Chamber of Commerce to improve the way substance abuse in the workplace was addressed. After a while she built a coalition of about 3,000 employers.
During this time she kept meeting more and more people who were addicted or had loved ones who were. So it became important to her to be involved in drug abuse prevention and treatment. She then became aware of the movement to legalize drugs.
“I knew that we had to push back against legalization, because if we did not prevention and treatment would not matter,” Fay asserted.
2. Kevin Sabet

Kevin Sabet
Sabet is the director of the Drug Policy Institute at the University of Florida, where he is an assistant professor in the psychiatry department at the College of Medicine.
He is a co-founder of Project SAM (Smart Approaches to Marijuana) and has been called the quarterback of the anti-drug movement.
Sabet served in the Obama Administration as a senior advisor for the White House Office of National Drug Control Policy (ONDCP) from 2009-2011. He previously worked on research, policy and speech writing at ONDCP in 2000 and from 2003-2004 in the Clinton and Bush Administrations, respectively. This gives him the distinction of being the only staff member at ONDCP to hold a political appointment in both the Bush and Obama Administrations.
He was one of three main writers of President Obama’s first National Drug Control Strategy, and his tasks included leading the office’s efforts on marijuana policy, legalization issues, international demand reduction,drugged driving and synthetic drug (e.g. “Spice” and “Bath Salts”) policy. Sabet represented ONDCP in numerous meetings and conferences, and played a key role in the Administration’s international drug legislative and diplomatic efforts at the United Nations.
He is also a policy consultant to numerous domestic and international organizations through his company, the Policy Solutions Lab. His current clients include the United Nations, where he holds a senior advisor position at the Italy-based United Nations Interregional Crime and Justice Research Institute (UNICRI) and other governmental and non-governmental organizations.
Sabet is published widely in peer-reviewed journals and books on the topics of legalization, marijuana decriminalization, medical marijuana, addiction treatment, drug prevention, crime and law enforcement.
He is a Marshall Scholar. He received his Ph.D. and M.S. in Social Policy at Oxford University and a B.A. in Political Science from the University of California, Berkeley.
3. Bill Bennett

Bill Bennett
Bennett was a former “drug czar” (i.e. director of the Office of National Drug Control Policy) during the administration of President George H.W. Bush. Prior to that he was the Secretary of Education in the Reagan administration. Bennett is a prolific author – including two New York Times Number- One bestsellers; he is the host of the number seven ranked nationally syndicated radio show Morning in America. He studied philosophy at Williams College (B.A.) and the University of Texas (Ph.D.) and earned a law degree from Harvard.
Bennett, along with former prosecutor Robert White, recently penned an op-ed piece for the Wall Street Journal calling marijuana a public health menace. The two are also finishing a book about marijuana legalization which is due out in February 2015.
Bennett frequently features on his radio show guests warning of the dangers of marijuana legalization. He is concerned that while the science shows that legalizing marijuana is not beneficial, public opinion is going in the other direction.
Why is he involved in this? Simply put, he thinks marijuana legalization is bad for America. The author of the acclaimed series of books about American history called America: The Last Best Hope thinks marijuana legalization will have deleterious effect on Americans, especially the youth of America.
“Because as Jim Wilson said, drugs destroy your mind and enslave your soul,” he told MainStreet.
“Medical science now proves it,” he added.
4. Patrick Kennedy

Patrick Kennedy
The other co-founder of Project SAM is former Rhode Island Democrat congressman Patrick Kennedy, son of Ted Kennedy. When he started SAM in Denver in 2013, Kennedy, who has admitted past drug use, was quoted as saying, “I believe that drug use, which is to alter the mind, is injurious to the mind … It’s nothing that society should sanction.”
His organization seeks a third way to address the drug problem, one that “neither legalizes or demonizes marijuana.” Kennedy does not think incarceration is the answer. He wants to make small amounts a civil offense. He emphasizes his belief that public health officials need to be heeded on this issue and they are not. He predicts that, if legalized, marijuana will become another tobacco industry.
“The thought that we will have a new legalized drug does not make sense to me,” Kennedy said during a 2013 MSNBC interview.
.
5. Joseph Califano

Joseph Califano
This former Carter administration U.S. Secretary of Health, Education, and Welfare founded, in 1992, the Center on Addiction and Substance Abuse at Columbia University (since 2013, it has been called CASAColumbia). He is currently the chairman emeritus. The center has been a powerful voice for research, fundraising and outreach on the dangers of addiction. It shines the light, especially on the perils of marijuana for adolescents.
Recently Califano released an updated edition of his book How to Raise a Drug-Free Kid: The Straight Dope for Parents. He believes an update was needed because of the advances in science regarding youth and substance abuse that have occurred during the past five years.
He zeroes in on marijuana in the book, which he says is more potent today than it was 30 or 40 years ago. He points out – during an interview about the book published on the CASAColumbia website – the hazards of “synthetic marijuana” also known as Spice or K2. He says this is available in convenient stores and gas stations but is so lethal it was banned in New Hampshire.
Califano stresses that parents are the bulwark against substance abuse and addiction. He cited data during the interview that “70% of college students say their parents’ concerns or expectations influence whether or how much they drink, smoke or use drugs. Parental disapproval of such conduct is key to kids getting through the college years drug free. This is the time for you to use social media to keep in touch with your kids.”
He makes the analogy that “sending your children to college without coaching them about how to deal with drugs and alcohol is like giving them the keys to the car without teaching them how to drive.”
6. Stuart Gitlow

Stuart Gitlow
Gitlow is the President of the American Society of Addiction Medicine (ASAM), a professional organization representing over 3,000 addiction specialist physicians.
In 2005, he also started the Annenberg Physician Training Program in Addictive Disease at the Mount Sinai School of Medicine in New York, NY. He is currently executive director. He is on the faculty of both the University of Florida and Mount Sinai School of Medicine.
About ASAM’s attitudes toward marijuana, he said:
“Our positions and policies with respect to marijuana have been developed over many decades and have been updated based upon the latest scientific evidence. We are firmly opposed to legalization of marijuana and reject the notion that the plant marijuana has any medical application.”
That said, he believes anecdotal evidence supports that more research should be conducted to deduce which parts of the marijuana plan can havemedical value.
Why did he get involved in this?
“I didn’t get involved in this as a “crusader” or because of a specific interest, but rather because I serve as the spokesperson for ASAM,” he told MainStreet.com. “In fact, though, given that there is so much industry-sourced money financing the marijuana proponents, and that the science-based opposition has little funding at all, I recognize the need for the public to actually hear what the facts are, particularly given the media bias and conflict of interest in terms of being motivated by potential ad revenue.”
7. David Murray

David Murray
A senior fellow at the Hudson Institute, Washington D.C., Murray co-directs the Center for Substance Abuse Policy Research. While serving previous posts as chief scientist and associate deputy director for supply reduction in the federal government’s Office of National Drug Control Policy. Before entering government, Murray, who holds an M.A. and Ph.D. in social anthropology from the University of Chicago, was executive director of the Statistical Assessment Service and held academic appointments at Connecticut College, Brown, Brandeis and Georgetown Universities.
What motivated him to get involved in a campaign to oppose marijuana legalization?
“It results from a steady regress from encountering a host of social pathologies (homelessness, failed school performance, domestic violence, child neglect, poverty, early crime, despair and suicide) and then time and again stumbling over a common denominator that either was a trigger or an accelerator of that pathology – substance abuse,” Murray told MainStreet. “Yet one finds as a dispassionate social analyst that the matter is either discounted, or overlooked, or not given sufficient weight, in the efforts to remediate the other surface manifestation pathologies,” he continued. “Moreover, one keeps encountering a sense that there is a closet with a door that is shut and it holds behind the door a host of explanations or guides to understanding of our woes, yet few are willing to open that door and address what lies behind it.”
He notes that even those who acknowledge the impact of substance abuse across so many maladies seem to not approach the problem with an open and searching mind. He said often one finds a ready-made narrative that serves to explain away the impact. The more that narrative is refuted “with counter argument or robust data indicating otherwise” the more social analysts resist or are in denial about the inadequacy of the standard narrative.
Subsequently, people who do criticize this encounter pressure from peers essentially telling to accept the narrative or shut up.
He mentions a good specific example can be found by encountering the reaction to the “gateway hypothesis” regarding early marijuana exposure. The literature in support of the gateway is quite strong he says.
“Yet everywhere the dominant response is to evade the implications,” he points out. “Our analysts pose alternative and unlikely accountings that seem practically Ptolemaic in their complicated denial of the obviously more simple and more real mechanism: exposure to the drug does, in fact, increase the likelihood of developing dependency on other, ‘harder’ drugs in a measurable way.“
8. John Walters

John Walters
He was, from December 2001 to January 2009, the director of the White House Office of National Drug Control Policy (ONDCP) and a cabinet member during the Bush Administration. During this time he helped implement policies which decreased teen drug use 25% and increased substance abuse treatment and screening in the healthcare system.
He is a frequent media commentator and has written many articles opposing the legalization of marijuana. He points out many of the fallacies of the pro-legalization movement. His editorials, essays, and media appearances have refuted the claims of the New York Times, pro-legalization libertarians and others.
For example, during a July 2014 appearance on Fox News Walters responded to the editorial boards condoning legalizing pot. Walters said when the science is increasingly revealing the risks of marijuana the “New York Times wants to act like it time to be ruled by Cheech and Chong.”
Walters has taught political science at Michigan State University’s James Madison College and at Boston College. He holds a BA from Michigan State University and an MA from the University of Toronto.
9. Robert DuPont

Robert DuPont
DuPont was the founding director of National Institute on Drug Abuse. He has written more than three hundred professional articles and fifteen books including Getting Tough on Gateway Drugs: A Guide for the Family, A Bridge to Recovery: An Introduction to Twelve-Step Programs and The Selfish Brain: Learning from Addiction. Hazelden, the nation’s leading publisher of books on addiction and recovery, published, in 2005, three books on drug testing by DuPont: Drug Testing in Drug Abuse Treatment, Drug Testing in Schools and Drug Testing in the Criminal Justice System.
DuPont is active in the American Society of Addiction Medicine. He continues to practice psychiatry with an emphasis on addiction and anxiety disorders. He has been Clinical Professor of Psychiatry at the Georgetown University School of Medicine since 1980. He is also the vice president of a consulting firm he co-founded in 1982 with former DEA director Peter Bensinger – Bensinger, DuPont and Associates. DuPont also founded, in 1978, the Institute for Behavior and Health a drug abuse prevention organization.
10. Bertha Madras

Bertha Madras
A professor of psychobiology for the Department of Psychiatry of Harvard Medical School. She is in a new position at McLean Hospital, a Harvard Medical School hospital affiliate. She was a former deputy director for the White House Office of National Drug Control Policy (ONDCP).
She has done numerous studies about the nature of marijuana. She is the co-editor of The Cell Biology of Addiction, as well as the co-editor of the 2014 books Effects of Drug Abuse in the Human Nervous System andImaging of the Human Brain in Health and Disease.
She rejects the claims of pot proponents. For example, she states that the marijuana chemical content is not known or controlled. She also notes that the “effects of marijuana can vary considerably between plants” and that “no federal agency oversees marijuana, so dose or purity of the plant and the contaminants are not known.”
11. Carla Lowe

Carla Lowe
A mother of five grown children, grandmother of nine, graduate of UC Berkeley and former high-school teacher, Lowe got started as a volunteer anti-drug activist in 1977 when her PTA Survey to Parents identified “drugs/alcohol” as their priority concern. She organized one of the nation’s first “Parent/Community” groups in her hometown of Sacramento and co-founded Californians for Drug-Free Youth. She also chaired the Nancy Reagan Speakers’ Bureau of the National Federation of Parents for Drug-Free Youth, co-founded Californians for Drug-Free Schools, and in 2010 founded an all-volunteer Political Action Committee, Citizens Against Legalizing Marijuana (CALM)
She has travelled throughout the U.S. and the world speaking to the issue of illicit drug use, primarily marijuana, and its impact on our young people. As a volunteer consultant for the U.S. State Department and Department of Education, she has addressed parents, students, community groups and heads of state in Brazil, Malaysia, Singapore, Thailand, Pakistan, Germany, Italy, Ireland, and Australia.
CALM, is currently working with parents, law enforcement, and local community elected officials to stop the proliferation of marijuana by banning “medical” marijuana dispensaries and defeating the proposed 2016 ballot measure in California that will legalize recreational use of marijuana.
She wants to go national and is part of an effort to start Citizens Against Legalization of Marijuana-U.S.A. that will also function as a Political Action Committee dedicated to defeating legalization efforts throughout the country.
Lowe is a strong proponent of non-punitive random student drug testing. She believes this is the single most effective tool for preventing illicit drug use by our youth, and will result in billions of dollars in savings to our budget and downstream savings from the wreckage to our society in law enforcement, health and welfare, and education.
12. Christian Thurstone

Christian Thurstone
He is one of a few dozen mental health professionals in America who are board certified in general, child and adolescent, and addictions psychiatry. He is the medical director of one of Colorado’s largest youth substance-abuse treatment clinics and an associate professor of psychiatry at the University of Colorado Denver, where he conducts research on youth substance use and addiction.
According to a May 2013 interview posted on the University of Colorado website, Thurstone was named an Advocate for Action by the White House Office of National Drug Control Policy in October 2012 for his “outstanding leadership in promoting an evidence-based approach to youth substance use and addiction.”
Colorado Gov. John Hickenlooper named Thurstone to a state task force convened to make recommendations about how to implement Amendment 64, a constitutional amendment approved by Colorado voters in November 2012 to legalize the personal use and regulation of marijuana for adults 21 and older.
He became involved in the marijuana issue in 2009 “when a whole confluence of events occurred that led to the commercialization of marijuana….What matters is not so much the decriminalization; it’s the commercialization that affects people, especially kids. …95% of the treatment referrals to Denver Health are for marijuana. Nationwide, it’s two-thirds of the treatment referrals according to the Substance Abuse and Mental Health Services Administration (SAMHSA).”
13. Peter Bensinger

Peter Bensinger
Bensinger was a former DEA chief during the Ford, Carter and Reagan administrations. He was in the vanguard opposing medical marijuana in Illinois. He acknowledges medical marijuana as a value but he notes that it is available as a pill or spray, so the idea of legalizing smoked marijuana for medicinal purposes is merely a ploy.
14. David Evans

David Evans
The executive director of the Drug Free Schools Coalition before becoming a lawyer he was a research scientist, in the Division of Alcoholism and Drug Abuse, New Jersey Department of Health. He was also the manager of the New Jersey intoxicated driving program. He has written numerous articles warning of the dangers of marijuana legalization.
15. Pope Francis

Pope Francis
The new pontiff, while being hailed by many as being a liberal influence in the Catholic Church has taken an intransigent line against marijuana legalization. This past June the new international pop culture icon told the 31st International Drug Enforcement Conference in Rome, “No a ogni tipo di droga (No to every type of drug).”
He was an active opponent of marijuana while a bishop in his native Argentina. He says now that attempts to legalize drugs do not produce the desired results.
He deplores the international drug trade as a scourge on humanity. Pope Francis has said it is a fallacy to say that more drug legalization will lead to less drug use.
16. Dennis Prager

Dennis Prager
A nationally syndicated radio talk show host in Los Angeles, Prager has used his microphone to condemn marijuana legalization. He has asked rhetorically, “Would you rather your pilot smoke cigarettes or pot? and “ How would Britain have fared in World War II if Winston Churchill had smoked pot instead of cigars?
17. Mel and Betty Sembler

Mel and Betty Sembler
The Semblers are longtime soldiers in the war on drugs. They co-founded, in 1976, a nonprofit drug treatment program called Straight, Inc. that successfully treated more than 12,000 young people with drug addiction in eight cities nationally from Dallas to Boston. They also help fund other organizations dedicated to opposing legalizing drugs including marijuana. Betty Sembler is the founder and Board Chair of Save Our Society From Drugs (S.O.S.) and the Drug Free America Foundation, Inc. Both organizations work to educate people about attempts to legalize as “medicine” unsafe, ineffective and unapproved drugs such as marijuana,heroin, PCP and crack as well as to reduce illegal drug use, drug addiction and drug-related illnesses and death.
18. Seth Leibsohn

Seth Leibsohn
Leibsohn is a radio host, writer, editor, policy, political and communications expert. He is a former member of the board of directors of the Partnership for a Drug Free America-Arizona Affiliate.
He told MainStreet that he got involved in the campaign against marijuana after seeing the effects of pot smoking on a college friend.
“One thing I noticed and never left my mind was a friend I had in college who so very clearly, freshman year, was one of the most gifted and intelligent thinkers and writers I had ever met,” he said. ” I predicted to myself and others, he’d be the next big American author, published in The New Yorker, books of short stories galore. But then he picked up a really habitual marijuana smoking practice. He smoked, probably, daily. This was the mid to late ’80s. And to this day, I believe he is still a smoker….and he is a waste-case. Lazy, never had a serious job, never published a serious piece of writing, totally ended up opposite what I had predicted. That story never left my mind.”
Leibsohn also noticed this was happening more and more. But the problem really was driven home while he was the producer and co-host for the Bill Bennett radio show, Morning in America.
“We noticed something very interesting: whenever we dealt with the issues of drug abuse, and particularly marijuana, the phone lines lit up like no other issue,” he said. “We had doctors, we had nurses, we had truckers, we had small businessmen, we had housewives, we had moms, we had brothers, we had teachers, we had sisters, we had aunts, we had uncles telling us story after story of the damage marijuana and other drugs had done to their and their loved ones lives. It amazed me how widespread the issue is. I concluded, to myself, this issue of substance abuse may very well be the most important and damaging health issue in America.”
He also noticed that “there just weren’t that many who seemed to give a serious damn about it.” He said Joe Califano and Bill Bennett were about the only ones he knew with a large microphone or following who would address the issue. The silence in other precincts and from others was astounding to him.
“I still am amazed not more people are taking this as seriously as it should be taken,” he said. “But I know, too, that any family that has been through the substance abuse roller coaster, needs to know they are not alone, and they are the real experts–their stories tell the tale I wish more children and pro-legalizers could hear. Today, I still talk, write, and research on the issue and have joined the board of a non-profit dedicated to helping on it as well,” he explained.
19. Alexandra Datig

Alexandra Datig
A political advisor and consultant who has experience of more than 13 years on issues of drug policy she was instrumental in the defeat of California Proposition 19, The Regulate Control & Tax Cannabis Act. Datig serves on the Advisory Board for the Coalition for a Drug Free California, the largest drug prevention coalition in California.
She became involved in the anti-marijuana legalization movement because of her own experiences. She was working in politics at the local and state level for over eight years by 2009, but she also reached ten years in sobriety from a 13-year drug addiction that nearly cost her her life. When California Proposition 19 came along, she decided “to jump in and form my own independent campaign committee “Nip It In The Bud.”
“I began reaching out to several other committees, drug prevention groups and law enforcement and together we built a powerful statewide coalition for which I became one of its leading advisors and strategists,” she told MainStreet
“Today, I consider myself a miracle, because I was able to turn my life around,” she told MainStreet. “This is not something I could have done had I not gotten sober. Having rebuilt my life in recovery, I believed that my experience could convince voters that legalizing a drug like marijuana for recreational use would make our roads more dangerous and, much like cigarettes, was targeted at our youth. That legalization would cause harm to first time users, people who suffer from depression and mental disorders and especially people vulnerable to addiction or relapse.”
20. Monte Stiles

Monte Stiles
A former state and federal prosecutor, Stiles supervised the Organized Crime/Drug Enforcement Task Force – a group of agents and prosecutors who investigate and prosecute high-level drug trafficking organizations, including Los Angeles street gangs, Mexican cartels and international drug smuggling and money laundering operations.
One of his proudest personal and career achievements was the organization and implementation of the statewide “Enough is Enough” anti-drug campaign which produced community coalitions in every area of Idaho. In addition to the prosecution of drug traffickers, Monte has been a passionate drug educator and motivational speaker for schools, businesses, churches, law enforcement agencies, and other youth and parent organizations. He left government service in April 2011 to devote all of his time to drug education, other motivational speaking and nature photography.
The pro-drug brigade vilified me for saying cannabis wrecks lives. Now their lies have finally been exposed
With a mix of sneering condescension and intolerant certainty, pro- drugs campaigners are fond of saying cannabis is essentially harmless. Indeed, this claim has become one of the central planks of their propaganda in favour of the decriminalisation of the drug. But now their argument, so eagerly repeated by a host of self-appointed experts, liberal politicians and cheer-leading celebrities, has been blown apart by an authoritative report from a drugs adviser to the World Health Organisation.
Users can find themselves in a downward spiral. They drop out of school, fail to find employment, grow alienated from family and friends and become fully dependent on not just drugs but also welfare benefits . Based on in-depth research conducted over 20 years, the study by Professor Wayne Hall comprehensively refutes the fashionable pretence that cannabis is safe.
Through his wide-ranging analysis, he shows that the drug triggers psychotic disorders such as schizophrenia, traps its users in a spiral of dependency and inhibits brain development in young people.
Habitual users also suffer an increased risk of cancer and heart problems, he warns.
As a GP long concerned about the health problems caused by drug abuse, I could not be more pleased that this devastating study has been published.
In my work in a deprived area of Manchester, I have regularly seen how cannabis not only wrecks the lives of some of my patients, but can also cause social damage by fuelling family breakdown, crime and unemployment.
Yet for far too long, the decriminalisation lobby has been allowed to peddle the dangerous idea that this drug should not be too much of a worry to us. At last, thanks to Professor Hall, they are facing a challenge based on hard, long-term evidence. While I welcome this report as a powerful weapon against pro-drugs propagandists, I also see it as a personal vindication. For years, I have taken an uncompromising public stand against the decriminalisation of cannabis — and been vilified for it.
My interest in this field led to my appointment by the Home Office in early 2011 to an unpaid, voluntary position on the Advisory Council on the Misuse of Drugs (the official government body that makes recommendations on the control of dangerous or otherwise harmful drugs). I had planned to give up at least a day a week to help. But I had not reckoned on the insidious influence of the decriminalisation brigade.
The moment my appointment was announced, a campaign against me started. Appalled at my robust, anti-drug views, my opponents launched a hysterical vendetta. If their attacks had been confined to my supposedly ‘outdated’ opinions about cannabis, that would have been one thing. But they also resorted to character assassination. An attempt was made to paint me as an old-fashioned, backwards-looking reactionary because of my Christian faith.
And during this cynical orchestrated campaign, the ridiculous charge of homophobia was added to the charge sheet. Dredged up were my previously expressed reservations about gay marriage — though not civil partnerships. This view was based on my Christian belief (shared by many of faith and those with no faith) that marriage should be between a man and a woman.
They also highlighted a parliamentary briefing paper I and a number of other doctors had written in Canada that briefly mentioned studies that linked homosexuality and paedophilia. Though I can understand why this might have caused concern, and I would distance myself from such views today, no one who knows me could possibly describe me as anti-gay.
Yet I was called ‘a bigot’ and ‘scum’. One campaigner wrote that I was ‘no good with evidence’; another said appointing me to the Advisory Council on the Misuse of Drugs would be ‘a waste of a place’.
In this hysterical atmosphere, the Home Office proved spineless. Within less than a fortnight, my invitation to join the council was withdrawn. I never got to attend a single meeting.
What was so disturbing was the aggressive intolerance of my opponents. My presence on the council was deemed unacceptable simply because I did not abide by the progressive orthodoxy.
Yet in the wake of Professor Hall’s reports, it is the decriminalisation campaigners and their celebrity backers who look misguided. Their case has been weakened irrevocably.
To them, the harmlessness of cannabis has been an article of faith. Now it can be seen as a superstitious myth.
In every respect, my experience in general medical practice matches the findings of Professor Hall’s study.
Many cannabis users start taking the drug in their early teens while their brains are still developing. The brain does not stop its development until the early 20s, so cannabis could cause irreversible damage.
Some studies have shown those who start cannabis use in their adolescence and continue until adulthood can lose up to eight points of their IQ: a drastic decline that affects academic performance and motivation.
Users can find themselves in a downward spiral. They drop out of school, fail to find employment, grow alienated from family and friends and become fully dependent on not just drugs but also welfare benefits.
Crucially, as Professor Hall points out, the risk of developing addiction to cannabis can be compared with the risk of developing addiction to heroin or cocaine. The use of the drug itself also leads to depression and other serious mental illnesses such as schizophrenia.
A study of 18-year-old conscripts to the Swedish army showed those who smoked a cannabis joint once a week were far more at risk of psychosis than those who did not. Cannabis can bring other problems — such as increased suicide risk, criminality and danger on the roads since users are twice as likely to have car accidents as non-users. And as I have seen, many who try to give up cannabis suffer serious withdrawal symptoms, including restlessness, sleeplessness, mood changes, anxiety and even severe depression.
Yet none of this seems to matter to the campaigners and their celebrity supporters. Typical is the Liberal Democrat party, which loves to parade its metropolitan ‘sophistication’ by pushing for decriminalisation of cannabis. Like their fellow ideologues, such people think that by doing so they appear cool and ultra modern. But in reality they are pathetic, timid defeatists.
Have we learned nothing from the problems caused by alcohol and tobacco? Legalisation of cannabis would be another public health disaster.
They justify their approach by claiming the war on drugs has been ‘lost’. But it has never been properly fought. For the authorities, from police to politicians, have been reluctant to adopt a realistic drug prevention strategy that would involve not only enforcement of the law, but also effective rehabilitation programmes for addicts.
Yet other countries have shown there is no need to give up and that the war on drugs can be won.
Over the past few decades, Sweden and Japan have seen dramatic falls in drug use with an approach that combines vigour with rehabilitation. Sweden has shown it is possible to create a society where drug use is only a marginal phenomenon, thanks to the wide-ranging consensus on the need to create a drug-free society.
Above all, there is a remarkable paradox in the way progressive campaigners are only too keen to banish tobacco from society — through measures such as the ban on smoking in public or the insistence on plain packaging — yet the same toughness about drugs appears to be anathema to them. While they are happy to create ‘nicotine-free’ zones, they don’t want ‘drug-free’ ones. This contradiction only serves to illustrate the incoherence of their cause. The fact is that if you legalise cannabis, you would normalise its use.
Have we learned nothing from the problems caused by alcohol and tobacco? Legalisation of cannabis would be another public health disaster.
Instead, we should be fighting fiercely and passionately to reduce the use of this dangerous substance that causes such terrible, lasting damage.
DR HANS CHRISTIAN RAABE a GP in Manchester.
The following very pertinent comment re illegal growing of marijuana in California was sent by Monte Stiles of Drugwatch International.
Despite extremely liberal laws and policies in California regarding marijuana, the black market continues to thrive. Those who naively argue that drug dealers will go away when pot is taxed and regulated know little about how the black market operates, and why.
The underground drug business operates to avoid the law. In the case of legalization, the black market operates to avoid taxes and regulation. The same holds true for other legal commodities such as tobacco and prescription drugs. Does anyone really think that strict regulation has stopped the illegal sale of prescription drugs, or the sale of untaxed cigarettes in New York City?
The bottom line is demand. Until we impact the demand side in a big way, through prevention and eduction, the drug dealers (or the state) will continue to exact payment for their dangerous products. Education works when we do enough of it. Surrender to the drug culture is not a valid option. Monte
RIVERSIDE COUNTY: Authorities battle booming marijuana grows
A boom in illegal backyard marijuana grows – rumoured to be driven by Mexican drug cartels – has sown fear among residents in the unincorporated areas of Riverside County.
In Mead Valley, near Perris, a marijuana garden was growing in plain sight less than 50 yards from a playground. High-powered weapons, such as AK-47s, have been found at some of the grows. And there was a marijuana grow at the scene of a fatal shooting in August.
Sheriff’s officials say they are well aware of the increase in illegal marijuana grows and are aggressively investigating them, but they have disclosed little about their progress or what is driving the trend.
Riverside County Supervisor Kevin Jeffries, who raised the alarm about illegal activity earlier this year after receiving complaints from constituents, said his staff counted more than 300 marijuana gardens in his district alone. “It’s frankly scaring the hell out of the neighbors,” Jeffries said.
Residents have seen armed men around the grows and fear violent crimes in their neighborhoods are linked to them, he said. They have told Jeffries’ staff that people have been approaching property owners offering thousands of dollars to rent their land to grow marijuana and that the grows are affiliated with two particular Mexican drug cartels.
Jeffries has proposed an ordinance to crack down on for-profit marijuana growing, but he has encountered resistance from medical marijuana advocates.
Although Mead Valley and neighboring Good Hope are hot spots for growing, Jeffries said the problem is widespread across the western portion of the county. Among the communities where sheriff’s officials have investigated marijuana grows this year are Norco, Woodcrest, De Luz, Romoland, Nuevo and Anza.
“The Sheriff’s Department is greatly concerned about it,” Chief Deputy Patricia Knudson said of the increase. Though the department has a grant-funded marijuana eradication team that targets illegal marijuana growing, she said, it is dealing with a large number of grows and the investigation process is labor-intensive. Sorting out whether a grow is for-profit or for legitimate medicinal purposes can be particularly time-consuming, she said.
Sheriff’s officials said they received 300 reports of outdoor marijuana grows across the county this year. As of early October, the sheriff’s Special Investigations Bureau, which handles drug cases, had eradicated a total of 63 outdoor marijuana grows – some on public land – and made 66 arrests for illegal marijuana growing, sheriff’s officials said. That figure doesn’t include any grows eradicated by the local sheriff’s stations.
Sheriff’s officials declined to disclose details about their investigations, though they did say investigators have found no direct link to Mexican drug cartels. “We have rumours and innuendo,” Knudson said, adding that if members of the public have information, they should report it.
Source:http://www.pe.com/articles/marijuana-752347-grows-sheriff.html Oct.19th 2014
So who supports decriminalizing cocaine, heroin, LSD, methamphetamine, ecstasy and all dangerous drugs, including marijuana?
No, it’s not your teenage nephew. It’s President Obama’s new acting head of the Justice Department’s Civil Rights Division, Vanita Gupta. In 2012, Gupta wrote that “states should decriminalize simple possession of all drugs, particularly marijuana, and for small amounts of other drugs.” (Emphasis mine).
Last week, President Obama appointed Vanita Gupta to the position of acting head. According to the Washington Post, the administration plans to nominate her in the next few months to become the permanent assistant attorney general for the Civil Rights Division. Her views on sentencing reform–a bi-partisan effort in recent years–have earned her qualified kudos from some conservatives.
But her radical views on drug policy–including her opinion that states should decriminalize possession of all drugs (cocaine, heroin, LSD, ecstasy, marijuana etc.) should damper that support of those conservatives, and raise serious concerns on Capitol Hill.
As the deputy legal director of the American Civil Liberties Union and the director of its Center for Justice, Gupta’s legal and policy positions are well documented in her long paper trail, which, no doubt, will be closely scrutinized if and when she is nominated and gets a hearing before the Senate Judiciary Committee.
To begin, she believes that the misnamed war on drugs “is an atrocity and that it must be stopped.” She has written that the war on drugs has been a “war on communities of color” and that the “racial disparities are staggering.” As the reliably-liberal Huffington Post proclaimed, she would be one of the most liberal nominees in the Obama administration.
Throughout her career, 39-year old Gupta has focused mainly on two things related to the criminal justice system: first, what she terms draconian “mass incarceration,” which has resulted in a “bloated prison population, and second, the war on drugs and what she believes are its perceived failures.
She is particularly open about her support for marijuana legalization, arguing in a recent CNN.com op-ed that the “solution is clear: …states could follow Colorado and Washington by taxing and regulating marijuana and investing saved enforcement dollars in education, substance abuse treatment, and prevention and other health care.”
Yet just last week the current Democratic Governor of Colorado, John Hickenlooper, said that legalizing recreational use of marijuana was a “reckless.” And there is a growing body of evidence to prove his point: (1) pot-positive auto fatalities have gone up 100 percent in 2012, the year the state legalized pot; (2) the majority of DUI drug arrests involve marijuana and 25 to 40 percent were pot alone; (3) from 2011 through 2013 there was a 57 percent increase in marijuana-related emergency room visits–and there are many other indications of failure. New research, from a 20-year study, proves the dangers of marijuana.
But Gupta does not stop with marijuana. In calling for all drugs to be decriminalized–essentially legalizing all dangerous drugs–Gupta displays a gross lack of understanding of the intrinsic dangers of these drugs when consumed in any quantity.
Heroin, LSD, ecstasy, and methanqualone are Schedule I drugs, which are defined as “the most dangerous drugs of all the drug schedules with potentially severe psychological or physical dependence.” Cocaine, methamphetamine, Demerol and other drugs are Schedule II drugs, defined as “drugs with a high potential for abuse…with use potentially leading to severe psychological or physical dependence.”
Sound public policy must be based on facts, not radical unsafe, and dangerous theories.
Charles “Cully” D. Stimson is a leading expert in criminal law, military law, military commissions and detention policy at The Heritage Foundation’s Center for Legal and Judicial Studies. Read his research.
Source: www.dailysignal.com
ALASKA Association of Chiefs of Police, Inc.
1. Legalization will place a significant financial burden on local law enforcement agencies due to the need for special training that will be necessary to identify marijuana users who are driving impaired and to create or enhance youth education programs.
It is estimated that Alaskan police departments will have combined costs of nearly $6,000,000 to respond to immediate needs which will arise from legalization of marijuana. These costs include necessary training of police officers to establish drug impairment based on symptomology because there are no roadside tools like breathalyzers for testing marijuana usage, and for increasing the number of School Resource Officers (SROs) in communities to educate teens about the dangers of drug use. These are expenditures that have been tallied by mostly municipal police departments, therefore the bulk of these costs will likely need to be borne by taxpayers in the impacted communities. Additional costs may exist for the Department of Public Safety.
After medicinal marijuana became easy to get in Colorado, seizures of smuggled marijuana quadrupled in roughly 4 years as “legal” marijuana was diverted to other markets . No comparable studies have been found addressing this problem in Alaska, but if legalization in this state results in a similar increase in diversion trafficking, more than 75% of Alaskan police feel they will not have sufficient local resources to combat the potential impact in their community.
In 2011, the national average for youth aged 12 to 17 years old and considered “current” marijuana users was 7.64 percent which was the highest average since 1981. The most recent figures found for Alaska teens dates from 2009 and puts the number of students claiming to have used marijuana within the last 30 days at 22.7% and the number who have used the drug during their lifetime at 44.5% . Only 16 Alaskan chiefs report currently having SROs in their communities. If legalization occurs in Alaska, 64% of police chiefs felt it would be necessary to increase the number of school resource and DARE officers doing youth outreach in their communities to protect against an increase in local teen drug usage.
In 2006, Colorado drivers testing positive for marijuana were involved in 28 percent of fatal vehicle crashes involving drugs. By 2011 that number had increased to 56 percent. These statistics clearly indicate the importance of traffic enforcement, but identification of impairment due to marijuana requires special skills. No figures seem to exist which can illuminate the degree of the problem in Alaska but the consistency of data from other states would support the assumption that the Alaskan experience would be comparable. Ninety seven percent of Alaskan chiefs responding to the AACOP survey felt their officers needed additional Advanced Roadside Impaired Driving Enforcement (ARIDE) or Drug Recognition Expert (DRE) training to help them properly identify drivers impaired by marijuana. Of more than 950 police officers in the state, less than 100 are estimated to have ARIDE training, and less than 20 now have DRE training.
Less than 6% of the AACOP survey respondents felt their local taxpayers would support a sufficient increase in their police budget to meet the anticipated financial implications of marijuana legalization.
Seventy five percent of respondents felt their agency would require financial assistance to meet training needs that will be created by legalization. Providing this training for all police officers will not only be costly to local taxpayers and also logistically difficult.
·Unlike alcohol, for which impairment can be reasonably measured using a breathalyzer (and confirmed with a blood alcohol content measurement), valid detection for cannabis is time-consuming, and blood tests cannot definitively determine an approximate degree of impairment. The lack of suitable roadside tests and agreed-upon intoxication levels will make enforcement of impaired driving more difficult.
The necessity of drawing blood for toxicology testing creates another potential problem for police as it will necessitate training officers as phlebotomists, contracting with an independent phlebotomist to be on call, or taking all drivers suspected of impaired driving due to drugs (DUID) to the nearest hospital or clinic to have blood drawn.. In this “post-CSI” era, juries are likely to expect effective prosecution of drug impairment will require a toxicology evaluation combined with the testimony of a trained Drug Recognition Expert.
2. Stoned driving and other dangers would be increased, while the difficulty of proving impairment from marijuana may impact prosecutions, and could make civil settlements more difficult in the case of personal injury lawsuits.
Drugged driving impairs one’s motor skills, reaction time, and judgment and is a public health concern because it puts not only the driver at risk, but also passengers and others who share the road.
In other states where there has been an enormous increase in “medical” marijuana cardholders, DUI arrests involving marijuana have skyrocketed, as have traffic fatalities where marijuana was found in the system of one of the drivers. Because toxicology results are not universally reported for Alaskan crashes no definitive data exists which would demonstrate a different result here.
In 2011 there were 9.4 million persons aged 12 and older who reported driving under the influence of illicit drugs during the past year. The rate was highest among young adults aged 18 to 25.
Drugs that may affect driving were detected in one of every seven weekend night time drivers in California during the summer of 2012. In the first California state wide roadside survey of alcohol and drug use by drivers, 14 percent of drivers tested positive for drugs, 7.4 percent of drivers tested positive for alcohol, and just as many as tested positive for marijuana as alcohol.
In a study of seriously injured drivers admitted to a Maryland Level-1 shock-trauma center, 65.7 percent were found to have positive toxicology results for alcohol and/or drugs. Almost 51 percent of the total tested positive for illegal drugs. A total of 26.9 percent of the drivers tested positive for marijuana.
The National Organization for the Reform of Marijuana Laws (NORML) has called for a science-based educational campaign targeting drugged driving behavior. In a January 2008 report titled, Cannabis and Driving, it is noted that motorists should be discouraged from driving if they have recently smoked cannabis and should never operate a motor vehicle after having consumed both marijuana and alcohol. The report also calls for the development of roadside, cannabis-sensitive technology to better assist law enforcement in identifying drivers who may be under the influence of pot.
In a 2007 National Roadside Survey of alcohol and drug use by drivers, a random sample of weekend nighttime drivers across the United States found that 16.3 percent of the drivers tested positive for drugs, compared to 2.2 percent of drivers with blood alcohol concentrations at or above the legal limit. Drugs were present more than 7 times as frequently as alcohol.
Low doses of THC moderately impairs cognitive and psychomotor tasks associated with driving, while severe driving impairment is observed with high doses, chronic use and in combination with low doses of alcohol. The more difficult and unpredictable the task, the more likely marijuana will impair performance.
3. Persons under the influence of marijuana will present a risk on job-sites. If marijuana is legalized, aggressive drug screening and periodic testing of medical personnel, industrial workers, transportation workers. and others will be necessary to insure safety of the public and other workers.
According to the American Council for Drug Education in New York, employees who abuse drugs are 10 times more likely to miss work, 3.6 times more likely to be involved in on-the-job incidents (and 5 times more likely to injure themselves or another worker in the process) and 5 times more likely to file a workers’ compensation claim. They also are said to be 33 percent less productive and responsible for potentially tripling health care costs.
The risk that your surgeon, pilot, bus driver, or coworker has used marijuana will increase if the drug is decriminalized.
A Rand study suggests drug use leads to about a 25-percent increase in men’s risk of having a workplace injury.
In addition to the acute effects of alcohol and other drug use on judgment and psychomotor skills, substance use that occurs hours before a worker begins his or her shift can cause spillover effects, such as fatigue and hangovers, that may independently increase injury risk. Studies have shown that hangovers affect cognitive skills, including tasks related to driving or piloting aircraft, which may therefore influence the risk of injury in a manner similar to the influences of acute alcohol intoxication.
Persons more likely to misuse alcohol and other substances may be more likely to be engaged in other behaviors that increase the risk of injury, a concept termed deviance proneness
4. Marijuana legalization will usher in Drug Commercialization increasing the chances of the drug falling into the hands of kids.
Already, private holding groups and financiers have raised millions of start-up dollars to promote businesses that will sell marijuana and marijuana-related merchandise.
Cannabis food and candy is being marketed to children and are already responsible for a growing number of marijuana-related ER visits. Edibles with names such as “Ring Pots” and “Pot Tarts” are inspired by common children’s candy and dessert products such as “Ring Pops” and “Pop Tarts.”
Several, profitable vending machines containing products such as marijuana brownies are emerging throughout the country.
The former head of Strategy for Microsoft has said that he wants to “mint more millionaires than Microsoft” with marijuana and that he wants to create the “Starbucks of marijuana.”
5. Marijuana use will increase under legalization
Because they are accessible and available, our legal drugs are used far more than our illegal ones. According to recent surveys, alcohol is used by 52% of Americans and tobacco is used by 27% of Americans. Marijuana is used by 8% of Americans.
When RAND researchers analyzed California’s 2010 effort to legalize marijuana, they concluded that the price of the drug could plummet and therefore marijuana consumption could increase.
The 2011 Monitoring the Future Survey noted that daily or near daily marijuana use, defined as use on 20 or more occasions in the past 30 days rose significantly in the 8th, 10th and 12th grades in 2010 and rose slightly higher again in 2011. This translates to one in every 15 high school seniors smoking pot on a daily or near daily basis, the highest rates that has been seen in thirty years – since 1981.
6. Marijuana is especially harmful to kids and adolescents.
Marijuana use that begins in adolescence increases the risk they will become addicted to the drug. The risk of addiction goes from about 1 in 11 overall to 1 in 6 for those who start using in their teens, and even higher among daily smokers.
Marijuana contributes to psychosis and schizophrenia , addiction for 1 in 6 kids who ever use it once , and it reduces IQ among those who started smoking before age 18.
Regular or daily use of marijuana may be robbing many young people of their potential to achieve and excel. THC, a key ingredient in marijuana, alters the ability of the brain’s hippocampus to communicate effectively with other brain regions. In addition, recent research has shown that marijuana use that begins during adolescence can lower IQ and impair other measures of mental function in adulthood.
7. Today’s marijuana is NOT your Woodstock weed.
In the 1960s and ‘70s, THC levels of the marijuana smoked by baby boomers averaged around 1%, increasing to just under 4% in 1983, and almost tripling in the subsequent 30 years to around 11% in 2011.
8. Marijuana legalization will increase public costs.
For every $1 in alcohol and tobacco tax revenues, society loses $10 in social costs, from accidents to health damage .
In addition to the costs to law enforcement for training and prevention, the anticipated increase in impaired driving arrests would result in additional court costs including prosecution and public defenders. Even in places where these costs are not borne directly by taxpayers, they will divert funds which might otherwise be used to support other civic needs.
9. People are not in prison for small time marijuana use.
Few people are currently in prison for marijuana possession (in fact, only 0.1% of prisoners with no prior offenses ) and current alcohol arrest rates are over three times higher than marijuana arrest rates.
Statistics on state-level prisoners around the United States reveal that just 0.3% of all state inmates were behind bars for marijuana possession only (with many of those pleading down from more serious crimes).
99.8% of federal prisoners sentenced for drug offenses were incarcerated for drug trafficking.
The risk of arrest for each joint smoked is estimated at 1 in 12,000.
On the most recent prison census date only 4 people were incarcerated in Alaska prisons due to conviction on 6th degree Misconduct Involving Controlled Substance (MICS) which would include possession of less than 1 oz. of marijuana (the amount legalized by the proposed legislation). It is undetermined if these MICS-6 offenders had concurrent convictions for other offenses as well, but it is possible that at least some do.
10. Drug cartels and the black market will continue to function under legalization.
A recent RAND report showed that Mexican drug trafficking groups only received a minority of their revenue (15-25%) from marijuana. For them, the big money is found in illegal trade such as human trafficking, kidnapping, extortion, piracy, and other illicit drugs.
We know from past experience with other businesses that illegal actors have a lot to do with so called legal industries. These cartels will only be helped with legalization and more addiction, not hurt.
Dealers aren’t likely to give up their lucrative income. Legalization of marijuana will lead entrepreneur dealers and cartels to focus their energies on selling harder drugs.
11. The foreign experience is not promising. Neither Portugal nor Holland provides any successful example of legalization.
Offenses related to drug use or possession for use continued to comprise the majority of drug law offenses in 2010; between 2005 and 2010, there was an estimated 19 percent increase in the number of offenses related to drug use in Europe.
Independent research reveals that in the Netherlands, where marijuana was commercialized and sold openly at “coffee shops,” marijuana use among young adults increased almost 300%. Now, the Dutch are retreated from their loose policies. About 70 percent of Dutch towns have a zero-tolerance policy toward cannabis cafes.
There are signs that tolerance for marijuana in the Netherlands is receding. They have recently closed hundreds of coffee shops, and today Dutch citizens have a higher likelihood of being admitted to treatment than nearly all other countries in Europe.
In Portugal, use levels are mixed, and despite reports to the contrary, they have notlegalized drugs. In 2001, Portugal started to refer drug users to three person “panels of social workers” that recommend treatment or another course of action. As the European Monitoring Center’s findings concluded: “the country does not show specific developments in its drug situation that would clearly distinguish it from other European countries that have a different policy.”
12. Marijuana is believed by some to have medicinal properties, but we shouldn’t smoke the plant in order to derive those benefits, just like we do not smoke opium to get the benefits of morphine. More widespread use would increase the dangers of secondhand smoke damage to nonsmokers and children in the homes of users.
A 1999 The Institute of Medicine (IOM) study explained that “smoked marijuana . . . is a crude THC delivery system that also delivers harmful substances.” In addition, “plants contain a variable mixture of biologically active compounds and cannot be expected to provide a precisely defined drug effect.” Therefore, the study concluded that “there is little future in smoked marijuana as a medically approved medication.”
The principal IOM investigators explicitly stated that using smoked marijuana in clinical trials “should not be designed to develop it as a licensed drug, but should be a stepping stone to the development of new, safe delivery systems of cannabinoids.”
In states with medical marijuana laws, the average user is a male in his 30s with no terminal illness and a history of drug abuse.
Less than 2% of users have cancer or AIDS.
Residents of states with medical marijuana laws generally have abuse and dependence rates almost twice as high as states with no such laws.
·Research should be conducted to produce pharmacy-attainable, non-smoked medications based on marijuana.
13. The Alaska Initiative is premature. The experience of Colorado and Washington is not promising. It is better to wait to see if predictions of both sides are borne out by hard data rather than rely on speculation and the promise that benefit will outweigh harm.
Two independent reports released in August 2013 document how Colorado’s supposedly regulated system is not well regulated at all.
Teen use has increased in the past five years. Currently, the marijuana use rate among Colorado teens is 50% above the national average.
Drug-related referrals for high school students testing positive for marijuana has increased.
Medical marijuana is easily diverted to youth.
While the total number of car crashes in Colorado declined from 2007 to 2011, the number of fatal car crashes with drivers testing positive for marijuana rose sharply.
14. Marijuana is often used as a stepping-stone drug, leading to heroin, cocaine, or other harder drugs.
Teens who experiment with marijuana may be making themselves more vulnerable to heroin addiction later in life, if the findings from experiments with rats are any indication. Cannabis has very long-term, enduring effects on the brain..
Marijuana is a frequent precursor to the use of more dangerous drugs and signals a significantly enhanced likelihood of drug problems in adult life. The Journal of the American Medical Association reported, based on a study of 300 sets of twins, “that marijuana-using twins were four times more likely than their siblings to use cocaine and crack cocaine, and five times more likely to use hallucinogens such as LSD.”
Long-term studies on patterns of drug usage among young people show that very few of them use other drugs without first starting with marijuana. For example, one study found that among adults (age 26 and older) who had used cocaine, 62 percent had initiated marijuana use before age 15. By contrast, less than one percent of adults who never tried marijuana went on to use cocaine.
Columbia University’s National Center on Addiction and Substance Abuse (CASA) reports that teens who used marijuana at least once in the last month are 13 times likelier than other teens to use another drug like cocaine, heroin, or methamphetamine and almost 26 times likelier than those teens who have never used marijuana to use another drug.
An estimated 3.1 million persons aged 12 or older – an average of approximately 8,400 per day – used a drug other than alcohol for the first time in the past year according to the 2011 National Survey on Drug Use and Health. More than two-thirds (68 percent) of these new users reported that marijuana was the first drug they tried.
Nearly one in ten high school students (9 percent) report using marijuana 20 times or more in the past month according to the findings of the 2011 Partnership Attitude Tracking Survey.
Teens past month heavy marijuana users are significantly more likely than teens that have not used marijuana in the past to: use cocaine/crack (30 times more likely); use Ecstasy (20 times more likely); abuse prescription pain relievers (15 times more likely): and abuse over the counter medications (14 times more likely). This clearly denotes that teens that use marijuana regularly are using other substances at a much higher rate than teens who do not smoke marijuana, or smoke less often.
ENDNOTES
AACOP survey of Alaskan police chiefs conducted April 28-May 5, 2014
The Legalization of Marijuana in Colorado: The Impact Vol. 1/August 2013
AACOP survey of Alaskan police chiefs conducted April 28-May 5, 2014
MARIJUANA USE BY YOUNG PEOPLE: The Impact of State Medical Marijuana Laws By Karen O’Keefe, Esq, .Director of State Policies, Marijuana Policy Project and Mitch Earleywine, Ph.D., Professor of Psychology University at Albany, State University of New York, Updated: June 2011
AACOP survey of Alaskan police chiefs conducted April 28-May 5, 2014
The Legalization of Marijuana in Colorado: The Impact Vol. 1/August 2013
AACOP survey of Alaskan police chiefs conducted April 28-May 5, 2014
AACOP survey of Alaskan police chiefs conducted April 28-May 5, 2014
AACOP survey of Alaskan police chiefs conducted April 28-May 5, 2014
http://en.wikipedia.org/wiki/Cannabis_drug_testing
Interview with AK Crime lab director O. Dym, May 27,2014
NIDA Info Facts: Drugged Driving, September 10, 2009, page 1. http://drugabuse.gov/Infofacts/driving.html
Volz, Matt. “Drug overdose: Medical marijuana facing a backlash.” http://www.msnbc.msn.com/id/37282436
Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Office of
Applied Studies. Results from the 2011 National Survey on Drug Use and Health: Summary of National Findings.
September 2012. P.2
“California Roadside Survey Finds Twice as Many Weekend Nighttime Drivers Test Positive for Other Drugs as for Alcohol: Marijuana as Likely as Alcohol.” CESARFAX, Col. 21, Issue 48, December 3, 2012.
www.cesar.umd.edu/cesar/vol21/21-48.pdf .
DuPont, Robert. “National Survey Confirms that Drugged Driving is Significantly More Widespread than Drunk
Driving.” Commentary, Institute for Behavior and Health, July 17, 2009. page 1. http://www..ibhinc.org.
“Cannabis and Driving: A Scientific and Rational Review.” Armentano, Paul. NORML/NORML Foundation. January 10, 2008.http://normal.org/index.cfm?Group_ID=7475 for article and http://normal.org/index.cfm?Group_ID=7459 for the full report.
DuPont, Robert. “National Survey Confirms that Drugged Driving is Significantly More Widespread than Drunk
Driving.” Commentary, Institute for Behavior and Health, July 17, 2009. page 1. http://www.ibhinc.org
http://www.nhtsa.gov/people/injury/research/job185drugs/cannabis.htm.
http://www.safetyandhealthmagazine.com/articles/6044
http://www.rand.org/content/dam/rand/pubs/occasional_papers/2009/RAND_OP247.pdf
Dawson, 1994; Lehman et al., 1995; Newcomb, 1994; Spicer, Miller, and Smith, 2003.
Alface, I. (2013, May 27). Children Poisoned by Candy-looking Marijuana Products. Nature World News. Retrieved
from https://owl.english.purdue.edu/owl/resource/560/10 ; Jaslow, R. (2013, 28 May). Laxer marijuana laws linked to
increase in kids’ accidental poisonings CBS News. Retrieved from http://www.cbsnews.com/8301-204_162-
57586408/laxer-marijuana-laws-linked-to-increase-in-kids-accidental-poisonings
Gruley, B. (2013, May 9). Medbox: Dawn of the Marijuana Vending Machine. Bloomberg Businessweek. Retrieved
from http://www.businessweek.com/articles/2013-05-09/medbox-dawn-of-the-marijuana-vending-machine
Ex-Microsoft exec plans ‘Starbucks’ of marijuana. (2013, May 31). United Press International. Retrieved from
NSDUH, Summary of National Findings, 2012. Retrieved from
http://www.samhsa.gov/data/NSDUH/2012SummNatFindDetTables/NationalFindings/NSDUHresults2012.pdf
Kilmer, B., Caulkins, J.P., Pacula, R.L., MacCoun, R.J., & Reuter, P.H. Altered State? Assessing How Marijuana
Legalization in California Could Influence Marijuana Consumption and Public Budgets. Santa Monica, CA: RAND
Corporation, 2010. http://www.rand.org/pubs/occasional_papers/OP315
“Marijuana use continues to rise among U.S. teens, while alcohol use hits historic lows.” University of Michigan
Press Release, December 14, 2011. 2-3.
“Regular marijuana use by teens continues to be a concern.” National Institute of Drug Abuse, Press Release, December 19, 2012. P.2
Andréasson S, et al. (1987). Cannabis and Schizophrenia: A longitudinal study of Swedish conscripts. Lancet,
2(8574).
Anthony, J.C., Warner, L.A., & Kessler, R.C. (1994). Comparative epidemiology of dependence on tobacco, alcohol,
controlled substances, and inhalants: Basic findings from the National Comorbidity Survey. Experiential and Clinical
Psychopharmacology, 2.
Meier, M.H. (2012). Persistent cannabis users show neuropsychological decline from childhood to midlife. Proceedings of the National Academy of Sciences.
“Regular marijuana use by teens continues to be a concern.” National Institute of Drug Abuse, Press Release, December 19, 2012. P.2
Mehmedic, Z., et al. (2010). Potency Trends of D9-THC and Other Cannabinoids in Confiscated Cannabis Preparations from 1993 to 2008. The Journal of Forensic Sciences, 55(5).
Updating estimates of the economic costs of alcohol abuse in the United States: Estimates, update methods, and data.
Report prepared for the National Institute on Alcohol Abuse and Alcoholism. Retrieved from
http://pubs.niaaa.nih.gov/publications/economic-2000; Urban Institute and Brookings Institution (2012, October 15).
State and local alcoholic beverage tax revenue, selected years 1977-2010. Tax Policy Center. Retrieved from
http://www.taxpolicycenter.org/taxfacts/displayafact.cfm?Docid=399; Saul, S. (2008, August 30). Government gets
hooked on tobacco tax billions. The New York Times. Retrieved from
http://www.nytimes.com/2008/08/31/weekinreview/31saul.html?em&_r=0; for Federal estimates, see Urban Institute
and Brookings Institution (2012, October 15). State and local tobacco tax revenue, selected years 1977-2010. Tax
Policy Center. Retrieved from http://www.taxpolicycenter.org/taxfacts/displayafact.cfm?Docid=403; Campaign for
Tobacco-Free Kids (n.d.). Toll of tobacco in the United States of America. Retrieved from
http://www.tobaccofreekids.org/research/factsh
Bureau of Justice Statistics. (2004). Data collection: Survey of inmates in state correctional facilities (SISCF). Retrieved from http://www.bjs.gov/index.cfm?ty=dcdetail&iid=275
Federal Bureau of Investigation. (2011). Persons arrested. Retrieved from http://www.fbi.gov/aboutus/cjis/ucr/crime-in-the-u.s/2011/crime-in-the-u.s.-2011/persons-arrested
Bureau of Justice Statistics. (2004). Data collection: Survey of inmates in state correctional facilities (SISCF). Retrieved from http://www.bjs.gov/index.cfm?ty=dcdetail&iid=275
Bureau of Justice Statistics. (2004). Data collection: Survey of inmates in state correctional facilities (SISCF). Retrieved from http://www.bjs.gov/index.cfm?ty=dcdetail&iid=275
Kilmer, B., et al. “Altered State? Assessing How Marijuana Legalization in California Could Influence Marijuana Consumption and Public Budgets”. Santa Monica, CA: RAND Corporation, 2010.http://www.rand.org/pubs/occasional_papers/OP315
Alaska Department of Corrections prison population census data 2013
Kilmer, B, Caulkins, J.P, Bond, B.M. & Reuter, P.H. “Reducing Drug Trafficking Revenues and Violence in Mexico: Would Legalizing Marijuana in California Help?” Santa Monica, CA: RAND Corporation, 2010.
http://www.rand.org/pubs/occasional_papers/OP325 ___“Annual Report 2012: The State of the Drugs Problem in Europe.” European Monitoring Centre for Drugs and Drug Addiction. Lisbon. November 2012. P. 35.
Annual Report 2012: The State of the Drugs Problem in Europe.” European Monitoring Centre for Drugs and Drug Addiction. Lisbon. November 2012. P. 35.
MacCoun, R. & Reuter, P. (2001). Evaluating Alternate Cannabis Regimes. The British Journal of Psychiatry, 178.
INTRAVAL Bureau for Research & Consultancy. “Coffeeshops in the Netherlands 2004.” Dutch Ministry of Justice. June 2005.http://www.intraval.nl/en/b/b45.html.
MacCoun, R. (2010). What can we learn from the Dutch Cannabis Coffeeshop experience? RAND Drug Policy Research Center.Retrieved from http://www.rand.org/content/dam/rand/pubs/working_papers/2010/RAND_WR768.pdf
European Monitoring Center for Drugs and Drug and Addiction. (2011). Drug Policy Profiles-Portugal. Retrieved fromhttp://www.emcdda.europa.eu/publications/drug––policyprofiles/portugal
Institute of Medicine. “Marijuana and Medicine: Assessing the Science Base.” (1999). Summary http://www.nap.edu/html/marimed (January 11, 2006).
Benson, John A., Jr. and Watson, Stanley J., Jr. “Strike a Balance in the Marijuana Debate.” The Standard-Times. 13 April 1999.
O’Connell, T.J. & Bou-Matar, C.B. (2007). Long term marijuana users seeking medical cannabis in California
(2001–2007): demographics, social characteristics, patterns of cannabis and other drug use of 4117 applicants. Harm
Reduction Journal, 4(16)
Colorado Department of Public Health and Environment. (2011)
Cerda, M., et al. (2012). Medical marijuana laws in 50 states: Investigating the relationship between state legalization of medical marijuana and marijuana use, abuse and dependence. Drug & Alcohol Dependence, 120(1-3).
Colorado Office of the State Auditor. (2013). & City of Denver Office of the Auditor. (2013).
NSDUH, Summary of National Findings, 2012. Retrieved from
http://www.samhsa.gov/data/NSDUH/2012SummNatFindDetTables/NationalFindings/NSDUHresults2012.pdf
Rocky Mountain HIDTA. (2013). Legalization of Marijuana in Colorado: The Impact. Retrieved from
http://www.rmhidta.org/html/FINAL%20Legalization%20of%20MJ%20in%20Colorado%20The%20Impact.pdf
Salomonsen-Sautel, S., et al. (2012). Medical marijuana use among adolescents in substance abuse treatment. Journal of American Academic Child & Adolescent Psychiatry, 51(7).
Rocky Mountain HIDTA. (2013). Legalization of Marijuana in Colorado: The Impact. Retrieved from
http://www.rmhidta.org/html/FINAL%20Legalization%20of%20MJ%20in%20Colorado%20The%20Impact.pdf
Harding, Anne. “Pot May Indeed Lead to Heroin Use, Rat Study Shows” Reuters. July 12, 2006. See also: “Why Teenagers Should Steer Clear of Cannabis” Vine, Gaia. www.NewScientist.com
“What Americans Need to Know about Marijuana.” Office of National Drug Control Policy. October 2003.
Gfroerer, Joseph C., et al. “Initiation of Marijuana Use: Trends, Patterns and Implications.” Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Office of Applied Studies. July 2002. Page 71.
“Non-Medical Marijuana II: Rite of Passage or Russian Roulette?” CASA Reports. April 2004. Chapter V, Page 15.
“More Than Two-Thirds of U.S. Residents Who First Started Using Drugs in the Past Year began with Marijuana: 22% Started with Nonmedical Use of Prescriptions.” CESARFAX. Vol. 21. Issue 42. October 22, 2012
“Nearly One in Ten U.S High School Students Report Heavy Marijuana Use in the Past Month: One Third or More of Heavy Users Also Used Cocaine, Ecstasy, or Other Drugs.” CESARFAX, Vol 21. Issue 21. May 29, 2012
The Partnership Attitude Tracking Study: 2011 Parents and Teens Full Report.” MetLife and the Partnership At Drugfree.org. May 2, 2012. P7.
Source:
Alaska Association of Chiefs of Police, Inc. – 14 Reasons Against Marijuana Legalization Sept.2014
D.A.R.E. America joins every major public health association, including the American Medical Association, the American Psychiatric Association, the American Society of Addiction Medicine, and other groups in opposing the legalization of marijuana. Simply put, legalization would drastically increase marijuana use and use disorder rates, as well as hamper public safety and health at a cost of billions to society in lost productivity, impaired driving, health care, and other costs.
Of particular concern to D.A.R.E. is the relaxed attitude regarding the use of marijuana, which will lead to increased accessibility and reduced perception of harm. This will undoubtedly contribute to greater youth use and abuse of the drug.
Legalized marijuana means ushering in the next “Big Tobacco.” Already, private holding groups and financiers have raised millions of start-up dollars to promote businesses that will sell marijuana and marijuana-related merchandise. The former head of Strategy for Microsoft has even said he wants to “mint more millionaires than Microsoft” with marijuana and that he wants to create the “Starbucks of marijuana.” A massive industry has exploded in the legal marijuana states of Washington and Colorado.
Colorado’s experience is already going poorly. Colorado is the first jurisdiction to fully legalize marijuana and sell marijuana in state-licensed stores. And already in its first year, the experience is a disaster. Calls to poison centers have skyrocketed, incidents involving kids coming to school with marijuana candy and vaporizers have soared, and explosions involving butane hash oil extraction have increased. Employers are reporting more workplace incidents involving marijuana use, and deaths have been attributed to ingesting marijuana “edibles.” Open Colorado newspapers and magazines on your web browser (or look at the real thing) on any given day and you will find pages of marijuana advertisements, coupons, and cartoons. Remember Joe Camel and candy cigarettes? The marijuana industry offers a myriad of marijuana-related products such as candies, sodas, ice cream, and cartoon-themed paraphernalia and vaporizers, which are undoubtedly attractive to children and teens.i As Al Bronstein, medical director of the Rocky Mountain Poison and Drug Center recently told the Denver Post, “We’re seeing hallucinations, they become sick to their stomachs, they throw up, they become dizzy and very anxious.” Bronstein reported that in 2013 there were 126 calls concerning adverse reactions to marijuana. From January to April 2014 alone the center receive 65 calls.ii Dr. Lavonas, also from the Rocky Mountain Poison and Drug Center, said in 2014 that emergency rooms have seen a spike in psychotic reactions from people not accustomed to high potency marijuana sold legally, severe vomiting that some users experience, and children and adults having problems with edibles. iii
No advocate for marijuana legalization will openly promote making marijuana available to minors. However, it would be unwise to believe that relaxed attitudes about the drug, reduced perceptions of harm and increased availability will not result in increased youth use and abuse of marijuana. Children are the marijuana marketer’s future customers. Just as alcohol and tobacco companies have been charged with promoting their goods to children, so has the Colorado marijuana industry. In March 2014, the Colorado legislature was forced to enact legislation to prohibit edible marijuana products from being package to appeal to children. “Keeping marijuana out of the hands of kids should be a priority for all of us,” said Governor Hickenlooper, before signing the bill.iv But that was not enough.
As discussed above, Dr. George Sam Wan of the Rocky Mountain Poison and Drug Center and his colleagues compared the proportion of marijuana ingestions by young children who were brought to an emergency room before and after October 2009, when Colorado drug enforcement laws regarding medical marijuana use were relaxed. The researchers found no record of children brought into the ER in a large Colorado children’s hospital for marijuana-related poisonings between January 2005 and September 30, 2009 — a span of 57 months. It is a different story following legalization.v Dr. Bronstein reported twenty-six people have reported poisonings from marijuana edibles this year, when the center started tracking such exposures. Six were children who swallowed innocent-looking edibles, most of which were in plain sight. Five of those kids were sent to emergency rooms, and two to hospitals for intensive care.vi
The scientific verdict is in: marijuana can be addictive and dangerous. Despite denials by legalization advocates, marijuana’s addictiveness is not debatable: 1 in 6 kids who ever try marijuana, according to the National Institutes of Health, will become addicted to the drug. Today’s marijuana is not your “Woodstock weed” – it can be 5-10 times stronger than marijuana of the past.vii More than 400,000 incidents of emergency room admissions related to marijuana occur every year, and heavy marijuana use in adolescence is connected to an 8-point reduction of IQ later in life, irrespective of alcohol use.
Marijuana legalization would cost society in real dollars, and further inequality in America. Alcohol and tobacco today give us $1 for every $10 that we as society have to pay in lost social costs, from accidents to health damage.viii The Lottery and other forms of gambling have not solved our budget problems, either. We also know these industries target the poor and disenchantedix – and we can expect the marijuana industry to do the same in order to increase profits.
|
IF THEY SAY… |
YOU SAY… |
|
Marijuana is not addictive. |
Science has proven – and all major scientific and medical organizations agree – that marijuana is both addictive and harmful to the human brain, especially when used as an adolescent. One in every six 16 year-olds (and one in every eleven adults) who try marijuana will become addicted to it.x |
|
Marijuana MIGHT be psychologically addictive, but its addiction doesn’t produce physical symptoms. |
Just as with alcohol and tobacco, most chronic marijuana users who attempt to stop “cold turkey” will experience an array of withdrawal symptoms such as irritability, restlessness, anxiety, depression, insomnia, and/or cravings.xi |
|
Lots of smart, successful people have smoked marijuana. It doesn’t make you dumb. |
Just because some smart people have done some dumb things, it doesn’t mean that everyone gets away with it. In fact, research shows that adolescents who smoke marijuana once a week over a two-year period are almost six times more likely than nonsmokers to drop out of school and over three times less likely to enter college.xii In a study of over 1,000 people in 2012, scientists found that using marijuana regularly before the age of 18 resulted in an average IQ of six to eight fewer points at age 38 versus to those who did not use the drug before 18.xiii These results still held for those who used regularly as teens, but stopped after 18. Researchers controlled for alcohol and other drug use as well in this study. So yes, some people may get away with using it, but not everyone. |
|
No one goes to treatment for marijuana addiction. |
More young people are in treatment for marijuana abuse or dependence than for the use of alcohol and all other drugs.xiv |
|
Marijuana can’t hurt you. |
Emergency room mentions for marijuana use now exceed those for heroin and are continuing to rise.xv |
|
IF THEY SAY… |
YOU SAY… |
|
I smoked marijuana and I am fine, why should I worry about today’s kids using it? |
Today’s marijuana is not your Woodstock Weed. The psychoactive ingredient in marijuana—THC—has increased almost six-fold in average potency during the past thirty years.xvi |
|
Marijuana doesn’t cause lung cancer. |
The evidence on lung cancer and marijuana is mixed – just like it was 100 years ago for smoking – but marijuana contains 50% more carcinogens than tobacco smokexvii and marijuana smokers report serious symptoms of chronic bronchitis and other respiratory illnesses.xviii |
|
Marijuana is not a “gateway” drug. |
We know that most people who use pot WON’T go onto other drugs; but 99% of people who are addicted to other drugs STARTED with alcohol and marijuana. So, indeed, marijuana use makes addiction to other drugs more likely.xix |
|
Marijuana does not cause mental illness. |
Actually, beginning in the 1980s, scientists have uncovered a direct link between marijuana use and mental illness. According to a study published in the British Medical Journal, daily use among adolescent girls is associated with a fivefold increase in the risk of depression and anxiety.xx Youth who begin smoking marijuana at an earlier age are more likely to have an impaired ability to experience normal emotional responses.xxi
The link between marijuana use and mental health extends beyond anxiety and depression. Marijuana users have a six times higher risk of schizophreniaxxii, are significantly more likely to development other psychotic illnesses. |
|
Marijuana makes you a better driver, especially when compared to alcohol. |
Just because you may go 35 MPH in a 65 MPH zone versus 85 MPH if you are drunk, it does not mean you are driving safely! In fact, marijuana intoxication doubles your risk of a car crash according to the most exhaustive research reviews ever conducted on the subject.xxiii |
|
IF THEY SAY… |
YOU SAY… |
|
Marijuana does not affect the workplace. |
Marijuana use impairs the ability to function effectively and safely on the job and increases work-related absences, tardiness, accidents, compensation claims, and job turnover.xxiv |
|
Marijuana simply makes you happier over the long term. |
Regular marijuana use is associated with lower satisfaction with intimate romantic relationships, work, family, friends, leisure pursuits, and life in general.xxv |
|
Marijuana users are clogging our prisons. |
A survey by the Bureau of Justice Statistics showed that 0.7% of all state inmates were behind bars for marijuana possession only (with many of them pleading down from more serious crimes). In total, one tenth of one percent (0.1 percent) of all state prisoners was marijuana-possession offenders with no prior sentences. Other independent research has shown that the risk of arrest for each “joint,” or marijuana cigarette, smoked is about 1 arrest for every 12,000 joints.xxvi |
|
Marijuana is medicine.
|
Marijuana may contain medical components, like opium does. But we don’t smoke opium to get the effects of Morphine. Similarly we don’t need to smoke marijuana to get its potential medical benefit.xxvii |
|
The sick and dying need medical marijuana programs to stay alive.
|
Research shows that very few of those seeking a recommendation for medical marijuana have cancer, HIV/AIDS, glaucoma, or multiple sclerosis;xxviii and im most states that permits the use of medical marijuana, less than 2-3% of users report having cancer, HIV/AIDS, glaucoma, MS, or other life-threatening diseases.xxix |
|
Marijuana should be rescheduled to facilitate its medical and legitimate use.
|
Rescheduling is a source of major confusion. Marijuana meets the technical definition of Schedule I because it is not an individual product with a defined dose. You can’t dose anything that is smoked or used in a crude form. However, components of marijuana can be scheduled for medical use, and that research is fully legitimate. That is very different than saying a joint is medicine and should be rescheduled.xxx |
|
IF THEY SAY… |
YOU SAY… |
|
Smoking or vaporizing is the only way to get the medical benefits of marijuana.
|
No modern medicine is smoked. And we already have a pill on the market available to people with the active ingredient of marijuana (THC) in it – Marinol. That is available at pharmacies today. Other drugs are also in development, including Sativex (for MS and cancer pain) and Epidiolex (for epilepsy). Both of these drugs are available today through research programs.xxxi |
|
Medical marijuana has not increased marijuana use in the general population. |
Studies are mixed on this, but it appears that if a state has medical “dispensaries” (stores) and home cultivation, then the potency of marijuana and the use and problems among youth are higher than in states without such programs. This confirms research in 2012 from five epidemiological researchers at Columbia University. Using results from several large national surveys, they concluded, “residents of states with medical marijuana laws had higher odds of marijuana use and marijuana abuse/dependence than residents of states without such laws.xxxii |
|
Legalization is inevitable – the vast majority of the country wants it, and states keep legalizing in succession. |
The increase in support for legalization reflects the tens of millions of dollars poured into the legalization movement over the past 30 years. Legalization is not inevitable and there is evidence to show that support has stalled since 2013. |
|
Alcohol is legal, why shouldn’t marijuana also be legal? |
Our currently legal drugs – alcohol and tobacco – provide a good example, since both youth and adults use them far more frequently than illegal drugs. According to recent surveys, alcohol use is used by 52% of Americans and tobacco is used by 27% of Americans, but marijuana is used by only 8% of Americans.xxxiii |
|
IF THEY SAY… |
YOU SAY… |
|
Colorado has been a good experiment in legalization.
|
Colorado has already seen problems with this policy. For example, according to the Associated Press: “Two Denver Deaths Linked to Recreational Marijuana Use”. One includes the under-aged college student who jumped to his death after ingesting marijuana cookie.
The number of parents calling the poison-control hotline to report their kids had consumed marijuana has risen significantly in Colorado. Marijuana edibles and marijuana vaporizers have been found in middle and high schools.xxxiv |
|
We can get tax revenue if we legalize marijuana. |
With increased use, public health costs will also rise, likely outweighing any tax revenues from legal marijuana. For every dollar gained in alcohol and tobacco taxes, ten dollars are lost in legal, health, social, and regulatory costs.xxxv And so far in Colorado, tax revenue has fallen short of expectations. |
|
I just want to get high. The government shouldn’t be able to tell me that I can’t.
|
Legalization is not about just “getting high.” By legalizing marijuana, the United States would be ushering in a new, for-profit industry – not different from Big Tobacco. Already, private holding groups and financiers have raised millions of start-up dollars to promote businesses that will sell marijuana and marijuana-related merchandise. Cannabis food and candy is being marketed to children and are already responsible for a growing number of marijuana-related ER visits.xxxvi
Edibles with names such as “Ring Pots” and “Pot Tarts” are inspired by common children candy and dessert products such as “Ring Pops” and “Pop Tarts.” Moreover, a large vaporization industry is now emerging and targeting youth, allowing young people and minors to use marijuana more easily in public places without being detected.xxxvii |
|
IF THEY SAY… |
YOU SAY… |
|
Legalization would remove the black market and stop enriching gangs. |
Criminal enterprises do not receive the majority of their funding from marijuana. Furthermore, with legal marijuana taxed and only available to adults, a black market will continue to thrive. The black market and illegal drug dealers will continue to function – and even flourishxxxviii – under legalization, as people seek cheaper, untaxed marijuana. |
The following two articles come from Australia. The co-author of the first, Alex Wodak is a world renowned activist in the movement to legalise drugs – in particular cannabis. The carefully referenced response in the second article was written by Professor Dr. Stuart Reece.
Some frequently asked Q’s and A’s about medicinal cannabis
Prepared by Laurie Mather, PhD, FANZCA, FRCA, Emeritus Professor of Anaesthesia, The University of Sydney (lmather@med.usyd.edu.au) and Alex Wodak, AM, FRACP, FAChAM, FAFPHM Emeritus Consultant, Alcohol and Drug Service, St Vincent’s Hospital, Sydney, NSW, Australia (alex.wodak@gmail.com), 18 June, 2014
A History:
Q: What is cannabis?
A: Some people call it by its American name, marijuana. The name ‘cannabis’ describes its botanical origins and comes from the Latin word for hemp. The name ‘marijuana’ (or sometimes ‘marihuana’) is a contrived name given to associate it with African and Hispanic Americans who used it as a recreational drug in the United States during the 1930s.
Q: What has the cannabis plant been used for?
A: Cannabis is an ancient herb-like plant that has been used for thousands of years for fibre-making for products such as clothing and rope, for dietary ingredients, as an element of folk medicine, and as an agent to promote spiritual transcendence, particularly in the religions of South Asia. ‘Recreational’ cannabis use was uncommon in the West before the 1960s. A League of Nations meeting in Geneva in 1925 decided to ban cannabis internationally. Cannabis first started to come to the attention of law makers and enforcers in the USA in the 1930s. The Congressional Record from that time includes comments about perceived depravity attributed to cannabis use along with racial slurs. Progressively it became an illegal substance in many countries, including Australia.
Q: When did cannabis come into Western civilisations?
A: European venturers over many centuries, as judged by their writings, certainly encountered cannabis in their travels to exotic Eastern and Far Eastern lands. By the mid 19th century, cannabis, in one form or another, had become part of the medical-societal-experimental experience of many European societies.
Q: When did cannabis come into Western-style medicine?
A: Cannabis was adopted into British medicine from India in the mid-19th century having been observed there to relieve pain, muscle spasm, convulsions of tetanus, rabies, rheumatism and epilepsy.
B Cannabis as a medicine:
Q: How does cannabis work?
A: As a plant preparation, cannabis ordinarily contains many hundreds of chemical substances commonly found in plants (‘phytochemicals’), and a hundred or so unique substances commonly referred to as ‘phytocannabinoids’. A small number of phytocannabinoids are believed to cause the main pharmacological effects of cannabis in humans. Cannabis attaches to special receptors in the brain and some other organs in the body. This releases a special chemical that the body produces. The chemical acts as a transmitter.
Q: What is ‘medicinal cannabis’? Some people also refer to this as ‘medical marijuana’.
A: The ‘medicinal’ tag recognizes that cannabis, among many other uses, has the properties of a medicine.
C Benefits of medicinal cannabis:
Q: Why do some argue that medicinal cannabis be legalised?
A: It helps some people with distressing symptoms from serious medical conditions when they have not been sufficiently helped by the standard medicines. Cannabis is considered a ‘second line’ drug to be used when the first line drugs have been tried and have either not worked or had unacceptable side effects.
Q: What kind of evidence is there that cannabis can help some people?
A: The evidence is basically of three kinds. First, there is anecdotal evidence, usually provided by people who have experienced in themselves or observed in others some effect. Most information like this is hard to assess because it lacks corroborative documentation – and this is the kind of evidence that tends to appear in the lay press and on internet blog sites. This is not to say that the evidence is invalid – but only to say that the much of the vital information underpinning the claims is not available in a way that permits scientific scrutiny. The second type of evidence is papers published in reputable medical and scientific journals after peer-review. A third type of evidence is careful reviews of papers reporting the results of cannabis research.
Q: How good is the evidence that cannabis can help some people?
A: Randomised controlled trials (RCTs) are usually regarded as the best way of telling whether a medication is effective. In one recent review, for example, 82 RCTs showed that medicinal cannabis is effective in relieving distressing symptoms in about half a dozen conditions. 9 RCTs found that medicinal cannabis was not effective. This is quite an impressive result. There are at least half a dozen favourable reviews by prestigious organisations.
Q: What are the main medical conditions that might be helped by medicinal cannabis?
A: Severe nausea and vomiting after cancer chemotherapy, especially if no standard treatment has worked; severe chronic non cancer pain, especially if the pain is due to nerve damage; severe wasting in cancer or AIDS (though this is less common these days); stiffness due to multiple sclerosis. There are also some other conditions.
Q: Is cannabis a cure for any conditions or diseases?
A: Not as far as we know so far from scientifically assessed evidence.
Q: Can cannabis help young children with severe epilepsy resistant to all known treatments?
A: A number of people have claimed this. But this possible benefit has not yet been tested in scientifically assessable research.
D Potential risks:
Q: Are there any bad side effects from medicinal cannabis? People talk a lot about psychosis and marijuana: should we be worried about using a medicine that could cause schizophrenia?
A: Most of the assessment of side effects has been based on what is known from studying recreational cannabis. That’s like studying the safety of bootleg alcohol to estimate the safety of regulated alcohol. Used medically, cannabis can cause some mental disorientation, sleepiness, and dry mouth but these are typically less severe and troublesome than many of the medications that might be used to treat the same conditions. Besides, the effects of not treating the conditions also has to be considered. It has also been said that some of these side effects counteract the worse side effects of the other medications such as chemotherapy agents that cause serious side effects themselves. People distressed by severe symptoms unrelieved by conventional medications are unlikely to be concerned by the small risk of serious mental illness in a couple of decades time.
Q: Is there a risk that legal medicinal cannabis would increase the use of recreational cannabis.
A: Recreational cannabis use in those US states which allow medicinal cannabis is not greater than those states where medicinal cannabis is not permitted.
Q: Can’t people taking cannabis become addicted to it?
A: Dependence is a small risk with cannabis in the sense that it is not as severe as the dependence that occurs with tobacco, heroin or cocaine. What matters is not just the risks of cannabis but also its possible benefits and the benefits and risks of using other medicines or no medicines.
Q: Aren’t there more modern and more effective drugs than cannabis?
A: Yes there are. But these don’t work in every case and sometimes they too can produce nasty side effects. Many of the more modern drugs are also much more expensive and some require the patient to be kept in hospital while they are being administered.
E Taking medicinal cannabis:
Q: Are there alternatives to taking cannabis by smoking it? How else can medicinal cannabis be taken?
A: Cannabis can also be vaporised and the vapour inhaled. Devices are now available to make inhalation of cannabis vapour convenient and inexpensive. Oral forms of cannabis (dronabinol and nabilone, developed some 30 years ago) used to be available in Australia but are not available any more because they were expensive and not especially reliable, and they have been made obsolete. There is little scientific information available about other forms of medicinal cannabis given by mouth (such as tincture). Cannabis taken by mouth, although perhaps well-enough absorbed, is broken down in the liver before it gets into the main blood stream, making it hard to get the right dose in many people. Also, when cannabis is taken by mouth there seems to be an increased risk of anxiety attacks because there is no way to ‘stop giving it’ once it has been swallowed. Sativex (aka nabiximols) is a form of medicinal cannabis manufactured by a small pharmaceutical company. It is sprayed on the inside of the mouth. There are many attractive aspects of Sativex®, particularly convenience, but it is not readily available in Australia, and is only permitted in cases of stiffness (spasticity) from multiple sclerosis. Tincture of cannabis used to be legally available some 20 years ago. It has been made available by some individuals in Australia but its supply, these days, is not legal. If medicinal cannabis is allowed in Australia, some people with only a short time left to live and others who have been smoking cannabis for a long time are likely to continue to smoke the drug
Q: Aren’t Sativex and dronabinol available on the Pharmaceutical Benefits Scheme?
A: Neither Sativex (nabiximols) nor dronabinol are available on the Pharmaceutical Benefits Scheme.
Q: Is cannabis available medically in any other countries?
A: Medicinal cannabis is now available in about twenty countries including the USA (23 states), Canada, Switzerland, the Netherlands, and Israel.
Q: How is medicinal cannabis controlled in other countries?
A: In some countries medicinal cannabis controlled quite carefully with prescriptions by doctors and pharmacy dispensing. In some other countries, controls are much more relaxed and cannabis can be bought over the counter.
F Political and community factors:
Q: What’s stopping the government from legalising medicinal cannabis in Australia?
A: The main reason cannabis in not available in Australia is because of political impediments. Some Commonwealth and state/territory laws would have to be changed slightly. States make their decisions independently. Medicinal cannabis is allowed, in principle, under Australia’s international treaty obligations.
Q: How can we allow cannabis to be used medicinally while stopping it being used recreationally?
A: Easy. Australia allows morphine, cocaine, amphetamine and ketamine to be used medically while the recreational use of these drugs is prohibited.
Q: Is Australia doing enough research on medicinal cannabis?
A: Very little research on medicinal cannabis is carried out in Australia.
Q: What about people who might take medicinal cannabis and then try to drive a car?
A: There is an increased risk of a car crash if a driver has taken cannabis recently. This risk is much less than with alcohol but the risk if even greater after a combination of alcohol plus cannabis has been taken. A number of medicines which are prescribed today in Australia also increase the risk of a car crash.
Q: What is public opinion in Australia about medicinal cannabis?
A: In a community survey commissioned by the Commonwealth Department of Health in 2010, 69% of Australians supported medicinal cannabis with 75% supporting more research.
Q: Do many Australians take cannabis for medicinal purposes now?
A: Yes, but we don’t know how many.
Q: Will medicinal cannabis be allowed in Australia?
A: Possibly. But it’s very hard to predict this.
* * * * * * * * * * * * *
Response to Comments by Wodak and Mather
1. One notes that Dr Alex Wodak is one of the key authors of this paper. As the undisputed champion of drug decriminalisation in Australia for the last 30 years one must necessarily wonder what impact his personal views have on the advice he has provided to the parliament on this occasion.
2. The title of the paper uses the phrase “Medical cannabis”. It is a matter of record that “medical cannabis” has been deliberately used as the “Trojan horse” or thin edge of the wedge which is strategically used to introduce cannabis decriminalization. This has been true in many instances overseas, and the US states where it is now decriminalized. Moreover this tactic was made explicit in NSW last year during the unsuccessful attempt to introduce what was popularly thought to be a medical cannabis bill, but it turned out was only for homosexual patients who liked to smoke cannabis. In the GPSC2 report which was tabled before the parliament at that time, it was acknowledged that only patients who liked to smoke cannabis – and their friends and carers – would be likely to avail themselves of the alleged benefits of the then proposed legislation. In other words the very use of the term “medical cannabis” is the standard misnomer for cannabis decriminalization 1 which it has been found to be the most successful way to introduce it in virtually every jurisdiction around the world, and has been repeatedly used in NSW.
3. As was noted recently by Dr Nora Volkow the Director of the NIH Institute concerned with drug addiction 2, cannabis has a well recognized withdrawal syndrome associated with it, which can be experienced by up to 50% of people who are exposed to it on a daily basis, particularly when that exposure occurs in adolescence 1. In the fourth answer on page 1, the authors list a series of symptoms including pain, muscle spasm, agitation, fits, convulsions and rheumatics all of which are recognized presentations of cannabis withdrawal 3. Since the pro-pot group acknowledged that only pot-smokers will want to smoke pot if it is legalized, what they are really saying is that they will be able to treat their cannabis dependence syndrome more easily if it is made more readily available. Even the cannabis advocates acknowledge that more efficacious and safer treatments exist for every purported indication for which they suggest its use.
4. The first answer on page 2 is completely incorrect. In this response Wodak et. al. appear to claim that smoked cannabis is a medicine. As noted by Dr Volkow raw cannabis contains hundreds of chemicals and is an impure substance. After burning as in smoking the products of full and partial oxidation form thousands of chemicals many of them highly toxic and frankly carcinogenic including similar tars, polycyclic hydrocarbons and aromatic amines as those found in tobacco smoke. No regulatory authority in the world (e.g. FDA 4 in USA or TGA 5 in Australia) acknowledges any smoked preparation as a valid form of dosing of any medicine. The term “medical cannabis” is therefore in strictly medical terms a misnomer which has been
strategically designed to confuse and mislead people as part of the clever public relations marketing campaign of the big cannabis industrial developers (by analogy with big tobacco interests), as have now developed in California, Colorado, Oregon, Washington state and elsewhere.
——————
1 Lonsberry B “Medical marijuana is a fraud.” News Radio WHAM 1180. http://www.wham1180.com/onair/bob-lonsberry-3440/medical-marijuana-is-a-fraud-12428431 Viewed 13th July 2014. 2 The Institute she directs is called the National Institute of Drug Abuse. 3 See Epilepsy Action Australia – http://www.epilepsy.org.au/living-with-epilepsy/lifestyle-issues/alcohol-and-drugs 4 Food and Drug Administration 5 Therapeutic Goods Administration
——————-
5. The answer to the second question on page 2 is also incorrect. Wodak et. al. claim that cannabis is a second line drug for various – unspecified – medical conditions. This is erroneous. As clearly stated on the Epilepsy Action Australia webpage cited 6 it is not indicated at all by reputable authorities in this country as it is not even legal! The other point is that to achieve the so-called therapeutic effects one frequently has to achieve concentrations into the toxic range. There are numerous other treatments for glaucoma, asthma, epilepsy, pain and nausea. Were it legal and therefore ethical to list cannabis for these disorders, cannabis would be about 10th line, 20th line, 60th line, 80th line and 10th line respectively. This is another way of – politely – saying that there are no valid clinical indications for cannabis at this time. As Wodak and colleague correctly observe the indication for AIDS wasting has now become obsolete because of the great improvements in the treatments for AIDS.
6. Moreover in addressing this all important issue – the motivation for medical cannabis – Wodak and Mather appear to overlook the role of the pro-cannabis lobby in this campaign. Indeed one wonders if there would be any campaign to legalize cannabis if those who do not like to use it themselves were excluded from advocacy roles. One can only surmise at the relationship of the present advocates of the pro-pot position to the pro-pot practice.
7. Wodak and colleague’s answer to Question 3 on page 2 is also erroneous. Anecdotal evidence is not considered evidence which is even evaluable by reputable medical authorities. Wodak’s remarks do not state this clearly. One notes – paradoxically – that Wodak is keen to discount such evidence in the case of implant naltrexone – even in anecdotal cases where implant naltrexone has been obviously enormously successful (such as five years heroin free). At this point Wodak appears to be applying a double standard. The third type of evidence cited by Wodak and colleague is vague and unclear. The authors refer to “careful reviews of papers”. This is not a medical term. Modern Science considers “systematic reviews” and “meta-analyses”. Wodak and Mather do not even use these terms. So their meaning is unclear. In the context one must be concerned that this obfuscation of meaning may be deliberate.
8. Similar concerns apply to the fourth answer on page 2. Wodak and Mather refer to “one recent review”. The source is not even referenced! There are many reviews in medicine and one needs to consider the whole of the literature. Apparently this was not a systematic review or a formal meta-analysis as otherwise one would expect the authors of the present work to have cited this. Moreover the results of meta-analyses are typically reported in very complex form – not the very simplistic format which seems to be indicated by Wodak and Mather. The question is not “What were the findings of one particular review?”. The question in principle is “What does the totality of the literature say?”, or more formally “What were the findings of the largest, most comprehensive and most recent meta-analyses of the topic”. Moreover one again notes that Wodak and Mather have reported only a fraction of the information required to form an evaluation. How many of the patients involved in these un-sourced trials had to discontinue their trial medication because of toxicity? How many were lost to follow up? And particularly in how many patients who had not been previously exposed to smoked cannabis and who had been provided with access to all the usually recommended treatment options – was cannabis found to be the best therapy? Wodak and Mather’s un-referenced material does not even consider these pivotal questions, much less provide the parliament with the sorely needed information to address them.
————-
6 http://www.epilepsy.org.au/living-with-epilepsy/lifestyle-issues/alcohol-and-drugs
————–
9. The fifth answer on page 2 realting to the alleged medical indications for cannabis is also highly suspect. Let us review these conditions individually.
1) Nausea and vomiting with cancer chemotherapy can generally be controlled adequately with current methods. The drugs most commonly used and often effective are prochlorperazine and metaclopramide. Chief amongst the newer agents is the 5HT3 7 antagonists such as ondansetron, tropisetron and dolasetron, some of which can also be given as a sub-lingual wafer or by subcutaneous, intramuscular, or intravenous injection if needed so that vomiting itself does not preclude their administration. Similarly prochlorperazine can be given by suppository. These medications can all be given by many routes of administration. Other medications can also be used including steroids where required.
2) Pain clinics have numerous ingenious ways to control pain. Pain can also be induced by cannabis withdrawal, and cannabis use itself has been shown to be linked with chronic back pain, so beware the pain presenting in the cannabis addicted patient / advocate. Nevertheless Wodak and Mather are correct that many patients are left in difficult situations by their chronic non-cancer pain. This is an active area of research internationally, and one to which Australian researchers, particularly at the University of Adelaide, are making major contributions. The recent demonstration that inflammatory activity in the brain and nerves is associated with pain generation and pain perceptual mechanisms has opened major investigative pathways for the development of several exciting new agents. This is a project upon which some of the top medicinal chemists in the world are actively engaged, some of whom work intramurally at the NIH and NIDA 8 itself. One notes in passing that Wodak and Mather have neglected to observe that D-naltrexone and D-naloxone show special promise for this application.
3) AIDS wasting – As noted by Wodak and Mather this indication is disappearing due to the efficacy of the newer treatments for AIDS.
4) There are other treatments for MS stiffness. In particular recent advances in immunology have meant that the treatment of MS itself has dramatically improved in recent times with several newer options including teriflunomide, dimethyl fumarate, fingolomod and dalfampridine. Benzodiazepines, Lioresal, several anticonvulsants and local Botox can all find application when spasm is a problem.
10. The sixth answer on page 2 is also erroneous. Wodak and Mather claim that cannabis is not a cure for any described medical condition. Cannabis dependence and withdrawal is a well described medical condition acknowledged both in DSM-IV and DSM-V 9 of the APA 10. Administration of cannabis to patients in such states will produce a short term relief of symptoms, albeit with an exacerbation of its many long term toxic effects, oncogenicity, and gateway effects in other drug use, and likely damage to adolescent brain development 1-2. There is no intention in making this point to be humorous. This is very important because it is clear that many of the patients who are brought along to parliamentary enquiries, and who offer public testimony of the wonderful effects of cannabis are actually speaking from a background of pre-existing cannabis dependency and addiction. Lawmakers need to keep this key issue always in the forefront of their minds. As correctly identified by Dr Volkow, cannabis can cause many illnesses so the claim that cannabis relives a pain in whose aetiology cannabis was implicated, must be viewed with substantial circumspection by those charged with responsible decision making in our community. Lawmakers should note that these disorders include chronic back pain 2.
—————
7 5HT is the standard medical abbreviation for serotonin. This refers to the 5HT-3 ligand – receptor pair. 8 National Institute of Drug Abuse 9 Diagnostic and Statistical Manual IV and V respectively. 10 American Psychiatric Association
—————-
11. The purported answer of Wodak and Mather to the issue of cannabis related toxicity given as answer 1 on page 3 is not only erroneous but dangerous. It is misleading and confusing. Of course one can form an impression of the possible early toxicity of high level cannabis exposure by studying low level recreational exposure.
12. In addressing the subject of cannabis toxicity their answer actually acknowledges none of the key salient points made by Dr Nora Volkow in her leading article in the New England Journal of Medicine on June 4th 2014. The interested reader is referred there for more information, and to Hon. Rev. Fred Nile’s speech introducing the subject to the Legislative Council of NSW. In particular, compared with the eminent work of Volkow and colleagues, Wodak and Mather overlook:
1) Known psychiatric toxicity – schizophrenia, anxiety, depression, bipolar disorder;
2) Effects as a gateway agent to other and hard drug use;
3) Damage to brain development particularly when exposure occurs in key developmental stages such as pregnancy, childhood and adolescence
4) Damage to attention, intellect, cognition, memory
5) Damage to long term lifetime trajectories including ability to form stable relationships and to gain useful employment;
6) Respiratory toxicity including chronic bronchitis and emphysema-like changes;
7) Driving related toxicity including fatal car crash, both alone and in combination with alcohol;
8) Cardiovascular diseases including stroke, and heart attack and transient ischaemic attacks;
9) Immunosuppressive actions particularly when given to AIDS patients, and especially when taken by the smoked route;
10) Real concern in many studies about the connections of cannabis to cancer.
13. Moreover as Dr Volkow astutely observes many of these old cannabis studies were done when the THC concentration of cannabis was 3%. So the studies which found no ill effects in the 1970’s – 1990’s are likely out of date at this time. Dr Volkow has noted that THC concentrations of cannabis are now reported in the USA commonly at 12%. Indeed one cannabis shop is said to be opening in Colorado reporting a choice for patrons from 17% – 20% THC in its product!
14. Wodak’s answer in relation to side effects also reverses the true state of affairs. Clinical reports of cannabis use cite a very high rate of unacceptable side effects, which frequently precludes is clinical application. Such very elevated rates of discontinuation (often around 30-50%) of cannabis based treatments are rare with other treatments in the conditions under discussion.
15. The risks of mental side effects from cannabis are not distant and remote as Wodak and Mather claim. Cannabis intoxication, dependence and tolerance in patients exposed to high levels of it – albeit for therapeutic purposes – are common, and
entail anxiety, paranoia, forgetfulness and depression, and at times psychotic disturbances and hallucinations as being not unusual.
16. The second answer on page 3 is misleading. There is extreme concern in the US now, and numerous on the ground reports that cannabis use in states permitting cannabis use has increased dramatically. California tabled its first cannabis BILLIONAIRE in 2013. Does anybody seriously believe that that is because nobody is buying his products??
17. It was estimated recently by official sources that Colorado will consume 130 tonnes of cannabis annually 11. Selling at $220 per ounce 12 and with 35,274 ounces per tonne, this translates to $7,760,280 / tonne or $1,008,836,400 for the whole crop in that state alone. Unfortunately, whilst tax revenues were cited as a major reason for legalization in Colorado, the simple expedient of not buying it from one of the state’s three registered recreational cannabis dispensaries which were more expensive than the medical pot shops, allowed taxation to be circumvented 13. It is important to note that 67% of all the cannabis sold was used by the 22% of heaviest users, further confirming the addictive nature of the legally available weed 14.
18. The trade was also encouraging cannabis tourists to flow into the state, just as had happened in the Netherlands 15. Indeed one court has ruled that the Dutch coffee shops be compensated for the reduction in their trade consequent upon a tightening of the laws which have now been put in place to restrict such cannabis tourism 16.
19. The US reviews cannabis consumption in numerous states. The CDC have just published national figures however the data from two key states was not available. The sample from Colorado was unusable, and Washington state did not participate in the survey at all 17. In other words if official figures fail to show increased use in the states legalizing cannabis that is likely a direct product of the “Don’t’ ask, Don’t tell” policy applied to addiction epidemiology by CDC.
20. The third answer on page 3 is also incorrect as judged by Dr Volkow’s article. Even the baseline risk of cannabis addiction is high at 9%, particularly given that up to 40% of the community have been exposed to cannabis. As Dr Volkow points out the addiction rate can rise up to as high as 50% in many groups. If as is widely suggested cannabis is legalized, then heavily cannabis addicted patients will become much more commonplace.
——————
11 Silva R “Colorado marijuana market consumes estimated 130 tonnes of the drug annually.” HNGN 12th July 2014. http://www.hngn.com/articles/35958/20140711/colorado-marijuana-market-consumes-estimated-130-tonnes-of-the-drug-annually.htm Viewed 13th July 2014. 12 Wyatt C., “Colorado Completed First Legal Pot Study.” Associated Press. http://hosted.ap.org/dynamic/stories/U/US_RETHINKING_POT_DEMAND?SITE=AP&SECTION=HOME&TEMPLATE=DEFAULT Viewed 13th July 2014. 13 Wyatt C., “Colorado Completed First Legal Pot Study.” Associated Press. http://hosted.ap.org/dynamic/stories/U/US_RETHINKING_POT_DEMAND?SITE=AP&SECTION=HOME&TEMPLATE=DEFAULT Viewed 13th July 2014. 14 Light M.L., Orens A.;, Lewandowski B., Pickton T. “Market size and demand for marijuana in Colorado.” Prepared for Colorado Dept of Revenue. http://www.colorado.gov/cs/Satellite?blobcol=urldata&blobheadername1=Content-Disposition&blobheadername2=Content-Type&blobheadervalue1=inline;+filename%3D”Market+Size+and+Demand+Study,+July+9,+2014.pdf”&blobheadervalue2=application/pdf&blobkey=id&blobtable=MungoBlobs&blobwhere=1252008574534&ssbinary=true Viewed 13th July 2014. 15 Rodriguez C., “Marijuana for tourists, discord for the Netherlands.” Forbes magazine 24th September 2013. http://www.forbes.com/sites/ceciliarodriguez/2013/09/24/weed-ghettos-for-tourists-anger-netherlands-neighbors/ Viewed 13th July 2014. 16 Kooren M, “Dutch Cannabis coffee shops to be compensated over tourist laws.” Reuters. http://rt.com/business/shops-dutch-coffee-cannabis-303/ Viewed 13th July 2014. 17 CDC MMWR – Youth Risk Behaviour Surveillance – United States , 2013. http://www.cdc.gov/mmwr/pdf/ss/ss6304.pdf Viewed 13th July 2014.
———————
21. The fourth answer on page 3 is also misleading. If one speaks with unbiased and independent respiratory physicians who treat asthma, ophthalmologists who treat glaucoma, neurologists who treat epilepsy, and pain physicians who treat pain, one hears the same refrain repeated over and over again that cannabis is not required as a treatment. The treatments of today are in general more than sufficient for the clinical requirements.
22. The fifth answer on page 3 is strangely at variance with every drug regulatory agency in the world. Oddly, Wodak and Mather seem to recommend the smoked route in direct contrast to every other medicinal chemist and regulatory agency the world over. One can only wonder if this does not reveal their personal bias.
23. Australia is a signatory to the international narcotic conventions particularly the Single convention 1961. Legalization would entail a major change in Australian society and Australian Law to allow legal cannabis. We would be in breach of our international treaty obligations. Amongst other things, these treaties allow us to participate in international policing operations to help to break up global drug running gangs, and to cooperate with law enforcement across national boundaries on many issues.
24. There is no question that Australia’s use of its presently legal drugs, tobacco and alcohol is responsible for an enormous public health burden. Adding cannabis to this situation, when – paradoxically – Wodak has been one of the loudest voices opposing alcohol- and tobacco- related harms – would clearly compound this situation. Moreover because of the well established gateway effect of cannabis, allowing cannabis would increase the use of the other illegal drugs. Hence this change would signal Australia’s degeneration into an increasingly drug taking-culture. We would become less employed and less employable; that is our welfare bill will inevitably rise. The rate of congenital abnormalities would rise so children would be borne with lifelong disabilities including mental retardation. The rate of chronic disease in the community, including chronic back pain, would rise. In other words legalizing cannabis will increase our physical and mental health bill and our long term welfare dependency bill, at the same time as reducing our taxation base and national income generating capacity. This is an impossible cost squeeze and social dysfunction squeeze for any Government.
25. The fifth answer on page 3 relating to restricted use of cannabis is invalid. Wodak and Mather claim that one could nevertheless restrict cannabis use if it was allowed medicinally by analogy with morphine, cocaine, amphetamine and ketamine. 40% of our population has not been exposed to these agents. Moreover this is not the pattern which has been seen recently as medicinal cannabis is the all too obvious leading edge of cannabis decriminalization around the world. One notes the very reverse of this in the Dutch experience alluded to above.
26. The sixth answer on Page 3 is also suspect. Wodak and Mather have neglected to mention that cannabis is the drug most frequently implicated in car crashes after alcohol, and the most frequently implicated of all the illicit drugs in motor vehicle crashes. Legalizing it and increasing its use would obviously exacerbate this by an amount at least proportional to the amount of its increased use.
27. Moreover as the authors correctly observe alcohol is already legal, so that legalizing cannabis effectively legalizes the highly dangerous cannabis–alcohol cocktail. This
has been shown to be very dangerous in many studies, as is acknowledged by the present authors.
28. Wodak claims that many Australians take cannabis medicinally at present. He has not stated how many of these were previously habituated to cannabis. He does not say how many of these are taking it for cannabis-induced diseases. He does not give data on the overall physical or mental health of cannabis smokers, prior to the commencement of their supposed serious illness.
29. The other chestnut which Dr Wodak frequently mentions, although it is absent from the present paper, is that alcohol and tobacco are related to far more ill-health in the Australian community than cannabis. In a simple quantitative sense it may or may not be correct. In either event it is an appalling argument in that it fails to correct for the very different exposure patterns of the different agents. The more frequent use of tobacco and alcohol in our community is directly related to their differing legal status. Both the numbers consuming tobacco and alcohol and the relative amounts consumed, are greater for the legal drugs than any of the illegal drugs, precisely because of their legal status. So whilst Wodak and colleagues frequently use this argument to ridicule genuine medical concerns in relation to the illicit drugs, in fact it is a potent argument in favour of retention of the present status quo, and the illicit status of the presently proscribed agents including cannabis. Given what has now been established by medical researchers in relation to cannabis-induced toxicity it presumes far too much to suppose that cannabis is any less toxic than our presently legal intoxicants. No reputable scientist who is unbiased and familiar with the published research in this area would support this liberalist position.
30. In fact detailed examination of communities where cannabis consumption is normative, such as the northern rivers district of NSW including the Nimbin-Mullumbimby area, show that the area is shockingly affected by unduly elevated rates of depression, suicide, murder, unemployment, family breakdown rates, poverty and general unhappiness 18, despite its being situated in some of the most fertile and productive rural landscapes in the country. Given what is now known of the medical effects of cannabis, much of this social disadvantage and community repression which is reflected on every metric, can likely be related directly or indirectly to the known high cannabis consumption rate in the area, and the apparently legally protected status of the region’s not insignificant cannabis crop.
General Remarks
31. Overall one is left with the impression that the work that has been produced by Wodak and Mather is a thoroughly activist piece. This document distorts and mishandles the truth at most points. In short it is a document such as might be expected from Australia’s leading drug advocate. In that sense it is highly predictable.
32. That it purports to be a reputable and scientifically reliable source of information for lawmakers is appalling. It is neither scientific nor reliable. In a scientific sense it is nothing less than a national scandal. It is not so much a scurrilous abuse of scientific process and current evidence in regard to both the basic science of pathophysiology and applied clinical therapeutics, as a mockery, a debasement, and a frank abuse of science and medical data.
33. Given that Dr Alex Wodak appears to position himself as one of Australia’s leading national figures advising the nation on addictive drugs, the conclusion becomes inescapable that Australia has been ill-advised on illicit drug policy by this self-confessed drugs legalization activist, and that our policies in this area are therefore likely misinformed, ill-conceived and / or ill-constructed.
34. Given that the activist position adopted by Dr Wodak, speaking in the name of Science, is clearly at major variance with the contemporaneous pronouncement of acknowledged world leaders, sufficient evidence exists for a formal motion of censure against Dr. Wodak from this house for attempting to mislead the Legislative Council of NSW.
References
1. Volkow ND, Baler RD, Compton WM, Weiss SR. Adverse health effects of marijuana use. N Engl J Med 2014;370(23):2219-27.
2. Reece AS. Chronic toxicology of cannabis. Clin Toxicol (Phila) 2009;47(6):517-24.
President Obama visited Denver this week, was offered marijuana, and laughed. His administration made possible the open marketing and use of marijuana in Colorado and Washington state by directing that federal law not be enforced. The president is joined by Hillary Clinton and Rand Paul in supporting marijuana legalization. As Clinton recently told CNN, “On recreational marijuana, states are the laboratories of democracy. We (are) experimenting with that right now. I want to wait and see what the evidence is.”
There is no indication that Obama is really paying attention to what he has done in Colorado. During our recent visit to the state we found no one is measuring this “experiment” at all. Even more troubling, if this were truly an experiment, the impact of this “laboratory” is on human subjects, many of whom—Colorado adolescents, communities in neighboring states—were hardly approached for “informed consent.” Nor did citizens we talked to vote for what they see happening to them now.
To get the ballot amendment passed, promises were made to the residents of Colorado. The marijuana market would be tightly monitored, and strictly regulated, “from seed to sale.” There were assurances of no underage youth involvement, no blatant advertising to kids, no interstate trafficking, or black-market criminal cartels running operations. All transactions would be regulated, controlled, and assessed.
But none of that “assessing” is actually happening. And as we learned from a first-hand visit to Colorado this month, there is ample, clear, and disturbing evidence that each of those promised conditions is being violated, with impunity.
We learned that legalization has encouraged soaring levels of potency as new forms of the drug have appeared in edible candies, butane-extracted cannabis oils, in vaporizers used at school desks, undetected. The impact on society? Nobody knows, as nobody is measuring.
Are the underage getting the drug in greater numbers? One public school administrator told us that he is attending increasing numbers of private, disciplinary hearings for twelve-year olds who are daily marijuana users. Denver is awash with marijuana that is advertised as having a potency of three times or more the national average—which is already almost three times stronger today than it was in days of Woodstock. Potent, cheap THC gummy bears with hallucinogenic effects are advertised in newspapers, featuring cartoon characters such as Fred Flintstone.
On our visit we met with community leaders, educators, law enforcement personnel, and researchers at the University of Colorado medical center. They are the ones assembling the evidence from the front lines, from schools, hospitals, burn centers, and treatment facilities. A portrait is emerging of considerable, and rising, damage. And yet no comprehensive study is
being undertaken. No surveillance, evaluation, or even plotting a trajectory against a prior baseline.
Governor Hickenlooper’s office intends to conduct a “gap analysis,” trying to determine what information is missing in order to conduct a proper study, and whether there are data sufficient to learn anything. But aren’t these steps one takes before you plunge? As one parent put it, “you don’t want to have the only experiment be your own son.” People said that the state was “hurtling forward, with no one driving.” Meanwhile, legalization advocates are already proclaiming that all is well.
The black market thrives. According to the director of the Rocky Mountain trafficking center, “By legalizing marijuana in Colorado, we have become the black market for about 40 other states that we can document. So instead of eliminating it, we have become it. We are also the black market for those under twenty-one.”
Is any of this really unexpected? Dr. Francis Collins, head of the National Institutes of Health, was recently asked about legalization by USA Today. He warned, “We don’t know a lot about the things we wish we did.” Risks of IQ loss? “Perhaps it would be better if, before we plunged into (legalization) there was a little bit more recognition of that particular consequence.” Increased cancer risk? “We don’t know. Nobody’s done that study.”
Advocates rushed right over these gaping holes in our knowledge. Profits beckoned, and surely tax revenue. Well, actually, tax revenues are well below those promised, but the profits—and the costs—are real.
What we saw in Colorado has the markings—the steeply rising curve—of a drug use epidemic. Epidemics subside, but after the outbreak, the populace often settles into a new normal, at higher levels of the disease. The damage is difficult to reverse, and of those caught in the outbreak, not all return. Are other states going to follow this leap?
If the president believes that there is some important medical and societal “experiment” going on with legal marijuana, he is simply not paying attention. The evidence to date is stunning. It is time to stop pretending otherwise.
Source: http://www.weeklystandard.com July 10, 2014
Steroid use in Britain’s gyms is growing so fast, dirty needles are being disposed of in fitness centre sharps bins. The explosion in the popularity of potentially lethal muscle-building drugs has led to hundreds of thousands taking jabs. Their numbers now outstrip drug addicts who inject themselves with heroin in the UK, a Sunday Mirror investigation reveals. Our findings today confirm rising fears among drug charities and health experts that use of anabolic steroids – which mimic the effects of male hormone testosterone – is spiralling out of control. We discovered HIV infection among steroid injectors has risen to the same level found in heroin users – 1.5 per cent.
At one needle exchange in Warrington staff told us 90 PER CENT of the syringes they see have been used for steroids compared to only 10 per cent for heroin. Another exchange said children as young as 15 were using the drugs.
Anabolics can become addictive and lead to heart attacks, strokes and a higher chance of liver and prostate cancer as well as psychological problems. Killer Raoul Moat was on them when he shot three people in two days in 2010.
They are all too easily available online. But it is the tolerance of the growing problem by gyms around the country that is most worrying.
A shocked fitness fan who spotted one of the “sharps” bins containing used needles at a Virgin Active health club in London told us: “I couldn’t believe my eyes. “It’s one of the poshest gyms I’ve been in, £100 a month, and the bins were sitting right there in the toilets. It’s the first time I’ve seen that. I had a look and there were loads of needles and swabs.”
Easygym say they have the bins in their clubs for “safety reasons” and there are plans in place to introduce them in Dragon’s Den star Duncan Bannatyne’s 61 health clubs. Anytime Fitness is considering whether to introduce them. The clubs are following recommendations from health watchdog NICE – but nowhere near far enough.
NICE is concerned that gym users will share needles and spread HIV and Hepatitis B and C. It asked gyms not just to provide sharps bins but also sterile syringes for its members. None of the gyms we spoke to said they did this.
But the watchdog’s policy of accepting steroid use and the gyms’ adherence to that was yesterday blasted by tragic mum Tina Dear, whose Royal Marine son Matthew, 17, died just weeks after he started using steroids to bulk up. He is throught to have had a severe reaction sending his body into shock.
Tina, of Southend, Essex, said: “Needles bins in gyms normalise steroid use. People will go into changing rooms, see the gym has provided a bin and naturally presume steroids are safe.
“They’ll think it’s OK. But it’s not. It’s Russian Roulette. People don’t know what they’re taking. Gyms should be practising zero tolerance, especially when it comes to youngsters who look up to the older guys. They need positive role models.”
Jim McVeigh is acting director at the Centre for Public Health at Liverpool John Moores University and Britain’s leading expert in the misuse of anabolic steroids. He said the official figure of 70,000 steroid users in the UK was wrong. He warned: “It’s safe to say there are hundreds of thousands of steroid users in this country, more than heroin injectors.”
Needle exchanges – first set up in the wake of the AIDS crisis – confirm what he believes. One in Yorkshire, run by drug and alcohol charity Crime Reduction Initiatives (CRI), deals with 70 per cent steroid users compared to 30 per cent heroin.
And the problem is affecting younger and younger people. David Rourke from CRI’s Sheffield needle and syringe programme said he’s heard of children as young as 15 using steroids. He said: “We deal with guys over 18, but elsewhere I know of much younger kids.”
He believes the bins are a good idea. He said: “I have heard of gyms where used needles are shoved up into ceiling tiles. A safe alternative can’t be a bad thing.” Steroids are legal for personal use, but Jim McVeigh warned that is no indication they are safe. He said: “The fact is, users are taking a big risk. Often they don’t have a clue what they’re taking.
“These are people who wouldn’t buy a hotdog off the street, but they’ll take drugs off a stranger on the internet and inject themselves. There have been no long-term clinical tests on these substances, and most users take a cocktail of anything up to 12. They are playing with fire. We have no idea what long term health effects will be.”
Researchers from Public Health England and Liverpool John Moores University last year surveyed 395 men who used steroids and other performance enhancing drugs. As well as the one in 65 found to have HIV, the study also found one in 18 had been exposed to Hepatitis C and one in 11 had been to Hepatitis B.
While dealing steroids person to person is illegal, buying them online is easy. A simple Google search presents dozens of outlets offering the drugs. Gyms who have installed the bins yesterday defended their use.
Virgin Active said: “Sharp boxes are installed for practical and safety purposes for those with medical conditions, or needing to dispose of razors. Their presence in no way condones the use of steroids in our clubs.” Any illegal steroid activity is reported to the police, the spokesman added.
Easygym said: “Steroid use is not something we encourage or promote. For Health and Safety reasons only we provide a sharps bins for needles and razor blades. Bannatyne Health Clubs said: “The 61 health clubs will all have sharps boxes shortly.”
Anytime Fitness added: “We are currently looking at a sharps policy.” Professor Mike Kelly, Director of the NICE Centre for Public Health said: “Research shows people who inject these drugs are at an increased risk of blood-borne viruses including hepatitis.
“Needle and syringe programmes aim to stop people sharing potentially contaminated injecting equipment. Delivering these programmes in gyms is an important way to protect people.” But mum Tina, still grieving her lost son, said: “Gyms should be pushing education as their first priority instead of putting bins in their toilets.” * For more advice visit cri.org.uk and matthewdearfoundation.co.uk
Drug is a fuel for violent crime
Men on steroids are twice as likely to be involved in violence and carry weapons, say US studies. Scientists have linked steroid use to mood swings, paranoid jealousy, extreme irritabililty and impaired judgement. Anabolics addict Raoul Moat shot his ex-girlfriend Samantha Stobbart, her new partner Chris Brown and blinded PC David Rathband after blasting him in the face in 2010. In a letter to police, Moat, 37, described his anger saying: “It’s like the Hulk. It takes over and it’s more than anger and it happens when I’m hurt.”
Ex-US Marine David Bieber, who shot dead PC Ian Broadhurst in Leeds in 2003, was also pumped up on steroids. His father blamed the drugs for his 48-year-old son’s descent into a life of violence and crime. And 35-year-old Norwegian mass murderer Anders Breivik, who killed 77 people in a bombing and shooting rampage in July 2011, was a heavy steroid user too.
Serious health risks for users Anabolic steroid users take enormous risks to boost the size of their muscles. But it’s not only serious medical conditions – from high blood pressure to liver, kidney and prostate cancer – they could trigger.
Taking the drugs can also can lead to a reduced sperm count, infertility, shrunken testicles and baldness in men. It can also cause severe acne. In women, steroid use can increase facial and bodily hair growth, deepen the voice and cause problems with periods. And some of the darker side effects are psychological, such as aggressive behaviour, mood swings, manic behaviour and even hallucinations.
Source: http://www.mirror.co.uk/news/uk-news/sunday-mirror-investigation-reveals-shocking-3816366#ixzz36tr76b7s
Overall crime in the City and County of Denver has increased nearly 7 percent in the first six months of 2014 compared to the same period last year, according to new analyses of Colorado crime data.
The numbers, released by the Rocky Mountain High Intensity Drug Trafficking Area (HIDTA), differ markedly from widely published reports claiming crime in the Mile High City has dropped since the state opened its first recreational marijuana shops Jan. 1. (This April 7 report in the Washington Post is a great example of how journalists have jumped the gun — so to speak — on declarations that “crime is down across the board.”)
Before unpacking the numbers, HIDTA officials said they do “not infer causality” between the increased crime rates they found and the opening of Colorado’s recreational pot shops, most of which are concentrated in Denver. Similarly, marijuana proponents should not claim the drug’s legalization has caused crime to drop.
OK, so why such sharp discrepancy between the numbers reported by marijuana-interest groups, marijuana-cheerleading reporters and the HIDTA analyses, which are based on data collected by the National Incident Based Reporting System (NIBRS) and prepared to Denver Department of Safety Public Information Standards?
Rocky Mountain HIDTA Director Tom Gorman explains:
“The marijuana advocates’ claims boil down to old-fashioned cherry picking. What they are not telling everybody is that they are not looking at all reported crime categories in Denver, or even at all the crimes that fall under those categories. They are taking the numbers that favor their position — and in their case, those numbers are some of the crimes included in the FBI Uniform Crime Report, Part I.
“If you want a true and complete picture of all crime in Denver, you have to look at the Denver report that uses the National Incident Based Reporting System (NIRBS) because the FBI Uniform Crime Report (UCR) captures only about 50 percent of all crimes reported — and tracked — in Denver.”
To illustrate how much more thoroughly NIRBS data are tracked than the UCR data, Mr. Gorman’s office provided this quick chart listing only two categories of crime. The numbers in parenthesis refer to the number of subcategories of crime tracked under that larger category. (Note: For example, the FBI report looks at four subcategories of “violent crime,” while the Denver Police Department tracks those four subcategories and three others under the heading “crimes against persons.”)
The NIRBS data show overall crime in Denver is up 6.7% when comparing the first six months of 2014 to the first six months of 2013.
We encourage you to review all of the numbers for yourself, but here are some highlights:
Crimes against people in Denver County increased more than 18 percent. Under this category:
There were 21 murders in the first six months of 2013 and 13 in the same period of this year. That’s a drop of 38 percent.
Aggravated assault was up 2.2 percent, from 1,167 reports to 1,193.
Simple assault increased 35 percent, from 1,634 reports to 2,207.
Reports of intimidation jumped 45 percent, from 370 reports to 537.
Forcible sex offenses dropped from 419 reports to 340 reports, or 18.9 percent.
Non-forcible sex offenses declined from 12 to 7, or 41.7 percent.
Reports falling under the category of crimes against property fell 8 percent. However, subcategories of crime often involving marijuana were on the rise, Mr. Gorman noted. Among them were reports of stolen property, which increased 16.4 percent.
Criminal offences reported under the category of crimes against society increased 22.8 percent. Under this category:
Drug/Narcotics Violations increased 20.6 percent, from 1,069 reports to 1,289 reports.
Weapon law violations jumped 43 percent from 209 reports to 299 reports.
Criminal offences falling under the category titled “all other offenses,” nearly doubled with an increase of 96.2 percent. Under this category:
Reports of disorderly conduct and disturbing the peace skyrocketed 214 percent from 234 reports in the first six months of 2013 to 735 reports in the same period of this year.
Family offences considered nonviolent jumped 30 percent from 174 to 227 reports.
Criminal trespassing also rocketed up 162.4 percent from from 274 reports to 719.
Liquor law and drunkenness violations were up 237 percent from 27 reported offenses to 64.
Like the Rocky Mountain HIDTA, the National Association of Drug Court Professionals has examined the NIRBS data. Researchers affiliated with that organization compared the first six months of each of the last five years and found that reports of simple assault and domestic violence have risen steadily.
“We are not inferring causality between these increases … just like legalization proponents should not infer causality regarding the downward trend observable when isolating just the UCR’s Part One Crime Index,” NADCP Chief Executive Officer West Huddleston recently wrote. “However, we are promoting the position that the question remains open, and at best we can say there is contradictory evidence when trying to draw conclusions about the effect marijuana legalization has had on crime.”
It’s past time for news organizations to report this more accurate picture of crime in Denver — and not just the numbers handed to them by marijuana proponents or the numbers they select to build their preferred narratives.
Source:drthurstone.com 23rd July 2014
The latest statistics provide no surprises. Almost all of the top marijuana-using states have already legalized pot in some form or have a legalization bill on the ballot for 2014. This is especially true for youth use rates. Proof that where marijuana is legalised youth use escalates – and there is much research evidence that shows that marijuana is especially harmful for adolescents. The evidence also shows that the younger a person is when they begin to use drugs they are statistically much more likely to become dependent and problem users.
It is critical that we understand that only 7.3% of the population are current marijuana users, and yet the legalization of pot consumes the headlines and public debate around the country. Should massive changes in public policy, laws (and even state constitutions) be made in order to cater to the wishes of 7.3% of the population? This only makes sense if greed is the primary motive for doing so.
We need to help the general public understand that smoking pot is not the norm, that a relative few consume all of the pot being smuggled into and grown in the United States, and that there are serious consequences for surrendering to the drug culture.
Where Americans smoke marijuana the most
Forget Colorado or Washington — tiny Rhode Island is the marijuana capital of the United States, at least as measured by the percent of state residents who regularly use marijuana.
Marijuana use by state
State-level statistics from the latest National Survey on Drug Use and Health show that just over 1 in 8 Rhode Island residents over age 12 smoke marijuana monthly. This is more than three times the rate in Kansas, where only 4 percent of residents regularly indulge.
Nationally about 7 percent of Americans over age 12 have used marijuana in the past month. Western states tend to have the highest rate of usage, at 9 percent, followed by the Northeast. The South has the lowest overall rate at 5.83 percent.
In what will surely not be a surprise to anyone who has ever been young, 18- to 25-year-olds use marijuana the most. Nearly 19 percent of that group has used marijuana in the past month, according to the NSDUH. But again, the state-to-state variation in those numbers are considerable. More than one third of Vermonters in that age bracket regularly use marijuana, compared to less than 10 percent of Utah’s 18- to 25-year-olds.
But usage rates drop off considerably for people age 26 and older: Only 5 percent of Americans in that age group smoke marijuana regularly. Alaska’s 26-and-over crowd is the most likely to regularly use marijuana, at 11.18 percent. To put it another way, Alaska’s adults are more likely to use marijuana than Utah’s college-age crowd.
Both Oregon and Alaska have marijuana legalization measures on their ballots this fall. Not coincidentally, these are the two states with the highest rates of 26-and-over marijuana use.
Source: Comment from Monte Stiles to Drugwatch International August 2014
Marijuana use in the past month (%), by age group and state
|
State |
Total 12+ |
12 to 17 |
18 to 25 |
25+ |
|
|
||||
|
Total U.S. |
7.13 |
7.55 |
18.89 |
5.05 |
|
Alabama |
5.07 |
5.62 |
14.34 |
3.38 |
|
Alaska |
12.97 |
10.01 |
24.77 |
11.18 |
|
Arizona |
7.22 |
8.37 |
17.20 |
5.33 |
|
Arkansas |
5.30 |
6.01 |
14.71 |
3.61 |
|
California |
9.08 |
8.83 |
21.74 |
6.74 |
|
Colorado |
10.41 |
10.47 |
26.81 |
7.63 |
|
Connecticut |
8.44 |
8.72 |
23.66 |
6.01 |
|
Delaware |
7.49 |
9.58 |
20.95 |
4.95 |
|
District of Columbia |
10.45 |
9.35 |
24.49 |
7.24 |
|
Florida |
6.65 |
7.03 |
19.02 |
4.73 |
|
Georgia |
5.96 |
7.20 |
16.65 |
3.88 |
|
Hawaii |
7.57 |
9.69 |
18.15 |
5.69 |
|
Idaho |
5.29 |
6.21 |
13.09 |
3.77 |
|
Illinois |
7.03 |
6.94 |
20.27 |
4.79 |
|
Indiana |
6.20 |
6.25 |
16.78 |
4.31 |
|
Iowa |
6.10 |
6.65 |
16.84 |
4.13 |
|
Kansas |
4.06 |
5.47 |
11.34 |
2.55 |
|
Kentucky |
5.63 |
6.06 |
17.35 |
3.65 |
|
Louisiana |
4.62 |
5.01 |
13.00 |
3.02 |
|
Maine |
8.38 |
8.94 |
22.66 |
6.29 |
|
Maryland |
5.81 |
7.54 |
17.53 |
3.66 |
|
Massachusetts |
9.37 |
10.58 |
25.77 |
6.34 |
|
Michigan |
8.89 |
8.89 |
22.13 |
6.61 |
|
Minnesota |
6.30 |
7.27 |
17.58 |
4.33 |
|
Mississippi |
5.80 |
6.32 |
15.86 |
3.88 |
|
Missouri |
5.94 |
7.28 |
17.41 |
3.83 |
|
Montana |
10.45 |
9.56 |
26.51 |
7.94 |
|
Nebraska |
5.51 |
6.53 |
14.83 |
3.74 |
|
Nevada |
8.36 |
8.77 |
20.01 |
6.44 |
|
New Hampshire |
8.37 |
9.61 |
26.37 |
5.41 |
|
New Jersey |
6.05 |
6.85 |
19.26 |
3.96 |
|
New Mexico |
9.14 |
9.82 |
21.35 |
6.94 |
|
New York |
8.24 |
7.86 |
21.35 |
5.98 |
|
North Carolina |
6.49 |
7.69 |
19.28 |
4.24 |
|
North Dakota |
5.15 |
6.02 |
14.44 |
3.07 |
|
Ohio |
7.37 |
7.53 |
19.22 |
5.39 |
|
Oklahoma |
6.04 |
6.37 |
14.14 |
4.55 |
|
Oregon |
12.16 |
9.86 |
25.81 |
10.25 |
|
Pennsylvania |
6.18 |
6.87 |
17.54 |
4.20 |
|
Rhode Island |
13.00 |
12.44 |
30.16 |
9.74 |
|
South Carolina |
7.20 |
7.24 |
19.24 |
5.15 |
|
South Dakota |
5.79 |
6.44 |
13.95 |
4.28 |
|
Tennessee |
5.41 |
5.92 |
14.70 |
3.81 |
|
Texas |
5.11 |
6.32 |
13.76 |
3.30 |
|
Utah |
4.41 |
5.12 |
9.83 |
3.04 |
|
Vermont |
12.86 |
13.36 |
33.18 |
9.34 |
|
Virginia |
5.54 |
6.61 |
17.06 |
3.44 |
|
Washington |
10.21 |
9.45 |
23.44 |
8.11 |
|
West Virginia |
5.27 |
6.63 |
17.55 |
3.29 |
|
Wisconsin |
6.69 |
7.78 |
18.18 |
4.65 |
|
Wyoming |
5.68 |
6.00 |
13.06 |
4.36 |
Christopher Ingraham is a data journalist focusing primarily on issues of politics, policy and economics. He previously worked at the Brookings Institution and the Pew Research Center.
Source: Comment from Monte Stiles to Drugwatch International August 2014
Public opinion is moving in favor of marijuana, even as medical research raises fresh alarms.
The great irony, or misfortune, of the national debate over marijuana is that while almost all the science and research is going in one direction—pointing out the dangers of marijuana use—public opinion seems to be going in favor of broad legalization.
For example, last week a new study in the journal Current Addiction Reports found that regular pot use (defined as once a week) among teenagers and young adults led to cognitive decline, poor attention and memory, and decreased IQ. On Aug. 9, the American Psychological Association reported that at its annual convention the ramifications of marijuana legalization was much discussed, with Krista Lisdahl, director of the imaging and neuropsychology lab at the University of Wisconsin-Milwaukee, saying: “It needs to be emphasized that regular cannabis use, which we consider once a week, is not safe and may result in addiction and neurocognitive damage, especially in youth.”
Since few marijuana users limit themselves to use once a week, the actual harm is much worse for developing brains. The APA noted that young people who become addicted to marijuana lose an average of six IQ points by adulthood. A long line of studies have found similar results—in 2012, a decades-long study of more than 1,000 New Zealanders who frequently smoked pot in adolescence pegged the IQ loss at eight points.
Yet in recent weeks and months, much media coverage of the marijuana issue has either tacitly or explicitly supported legalization. A CCN/ORC International survey in January found that a record 55% of Americans support marijuana legalization.
The disconnect between science and public opinion is so great that in a March WSJ/NBC News poll, Americans ranked sugar as more harmful than marijuana. The misinformation campaign appears to be succeeding.
Here’s the truth. The marijuana of today is simply not the same drug it was in the 1960s, ’70s, or ’80s, much less the 1930s. It is often at least five times stronger, with the levels of the psychoactive ingredient tetrahydrocannabinol, or THC, averaging about 15% in the marijuana at dispensaries found in the states that have legalized pot for “medicinal” or, in the case of Colorado, recreational use. Often the THC level is 20% or higher.
With increased THC levels come increased health risks. Since Colorado legalized recreational use earlier this year, two deaths in the state have already been linked to marijuana. In both cases it was consumed in edible form, which can result in the user taking in even more THC than when smoking pot. “One man jumped to his death after consuming a large amount of marijuana contained in a cookie,” the Associated Press reported in April, “and in the other case, a man allegedly shot and killed his wife after eating marijuana candy.” Reports are coming out of Colorado in what amounts to a parade of horribles from more intoxicated driving to more emergency hospital admissions due to marijuana exposure and overdose.
Over the past 10 years, study after study has shown the damaging effect of marijuana on the teenage brain. Northwestern School of Medicine researchers reported in the Schizophrenia Bulletin in December that teens who smoked marijuana daily for about three years showed abnormal brain-structure changes. Marijuana use has clearly been linked to teen psychosis as well as decreases in IQ and permanent brain damage.
The response of those who support legalization: Teenagers can be kept away from marijuana. Yet given the dismal record regarding age-restricted use of tobacco and alcohol, success with barring teens from using legalized marijuana would be a first.
The reason such a large number of teens use alcohol and tobacco is precisely because those are legal products. The reason more are now using marijuana is because of its changing legal status—from something that was dangerous and forbidden to a product that is now considered “medicinal,” and in the states of Colorado and Washington recreational. Until recently, the illegality of marijuana, and the stigma of lawbreaking, had kept its use below that of tobacco and alcohol.
Legality is the mother of availability, and availability, as former Health, Education and Welfare Secretary Joseph A. Califano Jr. put it in his 2008 book on substance abuse, “High Society,” is the mother of use. According to the Substance Abuse and Mental Health Services Administration, currently 2.7 million Americans age 12 and older meet the clinical criteria for marijuana dependence, or addiction.
Mark A.R. Kleiman, a professor of public policy at the University of California, Los Angeles, has estimated that legalization can be expected to increase marijuana consumption by four to six times. Today’s 2.7 million marijuana dependents (addicts) would thus expand to as many as 16.2 million with nationwide legalization. That should alarm any parent, teacher or policy maker.
There are two conversations about marijuana taking place in this country: One, we fear, is based on an obsolete perception of marijuana as a relatively harmless, low-THC product. The other takes seriously the science of the new marijuana and its effect on teens, whose adulthood will be marred by the irreversible damage to their brains when young.
Supporters of marijuana legalization insist that times are changing and policy should too. But they are the ones stuck in the past—and charting a dangerous future for too many Americans.
Mr. Bennett is a former secretary of education (1985-88) and was the first director of the National Drug Control Policy (1989-90). Mr. White is an attorney in Princeton, N.J.
Source: William J. Bennett/ Robert A. White Aug. 13, 2014 WALL STREET JOURNAL http://online.wsj.com/articles/william-bennett-and-robert-white-legal-pot-is-a-public-health-menace-1407970966?mod=hp_opinion#
Lawmakers have expressed concern over a new form of alcohol that could hit the market as early as the fall. In early April, the Alcohol and Tobacco Tax and Trade Bureau (TTB) approved labels for seven varieties of Palcohol, a brand of dehydrated alcohol, ranging from straight vodka to a powdered margarita. Derided as “the Kool-Aid of teen binge drinking,” lawmakers and other concerned parties say Palcohol poses a particular risk for youth who may be attracted to this easily portable, easily hidden form of alcohol.
The modified FAQ section on snorting now reads: “Can I snort it? We have seen comments about goofballs wanting to snort it. Don’t do it! You wouldn’t want to anyway. It would take you approximately 60 minutes of painful snorting to get the equivalent of one shot of vodka up your nose. Why would you do that when drinking a shot of liquid vodka takes about two seconds?”
While Phillips has modified his marketing approach and resubmitted Palcohol for TTB review, concerned lawmakers, such as Senator Chuck Schumer (D-N.Y.) are calling for the product to be banned before it enters the market.
“It’s absurd. It’s scary,” Schumer told WCBS Radio and other news outlets recently. “I’m calling on the Food and Drug Administration to immediately step in, investigate Palcohol based on its obvious health risks and prohibit this ludicrous product from going to market.”
Schumer was a driving force behind the ban of Four Loko and other dangerous caffeinated alcohol products, the last alcoholic fad abused by teens and young adults.
CADCA agrees with Sen. Schumer.
“Palcohol is a ridiculous product and really just an attempt to appeal to young people. CADCA believes that there’s nothing good that can come out of powdered alcohol and we support efforts to restrict it. It’s important to remain vigilant about new and emerging novelty products like these and that’s why it’s critical that we have community coalitions across the country that are alerting us to these products and trends before they wreak havoc on our communities,” said Gen. Arthur T. Dean, CADCA Chairman and CEO.
While Palcohol is being resubmitted to the TTB for further review, some states are working to ban the product before it enters the national market. While Mark Phillips notes that Palcohol would federally be processed and sold in the same venues as traditional alcohol, in Vermont, state Senator Kevin Mullin is concerned that current state laws only address liquid alcohol, making the powdered form difficult to regulate, and more accessible to youth.
“You can’t buy a bottle of gin at the liquor store if you’re 16. But there’s nothing that I can see in Vermont statute that would prohibit you from buying powdered alcohol, if it was available,” he told Vermont’s NPR affiliate.
In Minnesota, state Representative Joe Atkins has introduced a bill to enact a statewide ban as quickly as possible, noting “with how quickly this is moving, we shouldn’t wait until next session to deal with this issue. We need to move quickly to protect public health.”
Alcohol Justice, an alcohol industry watchdog group, agrees that immediate action is necessary to prevent powered alcohol from ever reaching the market. The group has asked concerned parties to write letters to federal officials through their online tool, calling for the ban of powdered alcohol before it ever is available to teens or young adults.
Source: CADCA May 07, 2014
It may well be that health care providers in Springfield are mum on medical marijuana because of the potential liability associated with it. Just last week a Florida jury awarded Cynthia Robinson, whose husband died of lung cancer, $23.6 billion in punitive damages from R.J. Reynolds.
Paving the way for the verdict was the state’s Supreme Court’s ruling making it easier to prove that Big Tobacco knowingly sold dangerous products and hid the hazards of cigarette smoking. The Court said that smokers and their families needed only to prove addiction and illnesses or death.
The dangers of marijuana are well documented. Based upon years of research the Food and Drug Administration has concluded that “marijuana has a high potential for abuse, has no accepted medical use in the United States, and lacks an acceptable level of safety for use even under medical supervision.”
Physicians who are considering recommending marijuana should be checking their medical malpractice insurance. They may find that recommending the use of a non-FDA approved medication is excluded from coverage.
Source: State Journal-Register (IL) Copyright: 2014 The State Journal-Register
Source: Judy Kreamer Educating Voices, Inc. Naperville August 2014
This morning the letter below was sent to the editor of the Denver Post and their marijuana publication The Cannabist . The letter was expressing alarm at their promotion of numerous marijuana strains to treat serious mental health issues without any medical protocols. We did receive a response and a news release will follow tomorrow. This letter will be sent to individuals and organizations in our state and nationally working on public health (including mental health and substance abuse) , public policy and enforcement.
Feel free to forward this information to anyone you feel appropriate.
Here is the letter sent this morning:
Greg Moore, Editor, Denver Post
Ricardo Baca, EditorThe Cannabist
Dear Mr. Moore and Mr. Baca,
We are writing to express serious concerns regarding The Denver Post’s The Cannabist website’s recommendations of various marijuana strains to “treat” mental illnesses, including attention-deficit/hyperactivity disorder (ADHD), bipolar disorder, depression and post-traumatic stress disorder (PTSD). We are writing as concerned professionals with extensive experience in mental health treatment, medicine, and/or public health.
The Denver Post’s web site provides information from Leafly.com listing 92 Colorado specific strains of marijuana with 88 claimed to treat depression, 25 to treat PTSD, 23 for bipolar, and 40 for ADHD (see attached document assembled by Bob Doyle, Chair, Colorado SAM (Smart Approaches to Marijuana) Coalition). And a few strains are noted to treat cancer. The improper treatment or delay in effective treatment of mental health issues and major psychiatric illnesses can exacerbate the problem and could lead to additional harm to the patient and/or those around them.
In light of the serious potential impact of your recommendations, including possible delay in medical treatment for serious and potentially life threatening mental illnesses, and the potential for worsening of those illnesses by the marijuana you recommend, we request that you release the data upon which these recommendations for dispensing the specific marijuana strains as a treatment for bipolar disorder, PTSD, ADHD, and depression are based. We are sending a copy of this letter to medical authorities with knowledge of science and regulatory policies and procedures.
The absence of critical information on the web site for those accepting your advice to use the various marijuana strains is alarming and demonstrates a failure to appreciate the potential implications of your protocol. For each of the strains, we request to know the recommended dosage, duration, the THC and CBD content, whether you’re recommending they be used with or without FDA approved medication or behavioral treatment for the condition, what contraindications are known, and whether other physical or mental health issues should preclude certain people from using the strain.
We look forward to your prompt reply given the seriousness of the claims on your web site and their potential negative impact on serious psychiatric conditions your web site claims will be “treated” by particular strains of marijuana.
Sincerely,
Bob Doyle, Chair, Colorado SAM (Smart Approaches to Marijuana) Coalition Christian Thurstone, MD General, child and addiction psychiatrist
A. Eden Evins, MD, MPH, Associate Professor of Psychiatry, Harvard Med School Director, Center for Addiction Medicine, Mass.Gen.Hospital
The United States is divided over the legalization of marijuana. Arguments in favor include protection of individual rights, elimination of criminal sentencing for minor offenses, collection of tax revenue, and elimination of the black market. Counterarguments include the possible escalation of use, adverse mental and physical health effects, and potential medical and social costs.
Some steps have already been taken to reduce harsh and racially biased sentencing. There is growing support in Congress to eliminate federal mandatory minimums for drug offenses, and 19 states have either decriminalized or eliminated jail time for possession of small amounts of marijuana. Furthermore, 21 states and the District of Columbia have legalized the medical use of marijuana.
Washington State and Colorado went further, authorizing the retail sale of marijuana and opening the door to a legal marijuana industry. Given the lessons learned from the 20th-century rise of another legal addictive substance, tobacco, we believe that such an industry could transform marijuana and its effects on public health. Like tobacco, marijuana harms health and is addictive; unlike alcohol, both tobacco and marijuana came of age after the Industrial Revolution. And although the United States has, since tobacco’s rise, adopted regulatory structures designed to protect consumers, they do not apply to marijuana, in part because marijuana use and sales remain illegal under federal law. Colorado and Washington are developing regulatory infrastructures to fill this gap, but the goals and potential effectiveness of their proposed regulations are unclear. No evidence exists regarding which regulations might minimize population harm from marijuana. The marijuana industry’s trajectory could therefore repeat tobacco’s.
In its current form, smoked marijuana is less deadly than tobacco. Although case–control studies have found increased mortality associated with heavy marijuana use — attributable to vehicle crashes from driving while high, suicide, respiratory cancers, and brain cancers the nonfatal adverse effects of marijuana use are much more prevalent. These include respiratory damage, cardiovascular disease, impaired cognitive development, and mental illness. These harms are very real, though they pale in comparison with those of tobacco, which causes almost 500,000 U.S. deaths annually. Marijuana is also less addictive than tobacco. About 9% of cannabis users meet the criteria for dependence (according to the Diagnostic and Statistical Manual of Mental Disorders) at some time in their lives, as compared with 32% of tobacco users.
But tobacco was not always as lethal or addictive as it is today. In the 1880s, few people used tobacco products, only 1% of tobacco was consumed in the form of manufactured cigarettes,3 and few deaths were attributed to tobacco use. By the 1950s, nearly half the population used tobacco, and 80% of tobacco use entailed cigarette smoking; several decades later, lung cancer became the top cause of cancer-related deaths. This transformation was achieved through tobacco-industry innovations in product development, marketing, and lobbying.
The deadliness of modern-day tobacco stems from product developments of the early 1900s. Milder tobacco blends and new curing processes enabled smokers to inhale more deeply, facilitated absorption by lung epithelia, and boosted delivery of nicotine to the brain. Synergistically, these changes enhanced tobacco’s addictive potential and increased intake of toxins. In addition, the industry added other ingredients, including toxic substances that enhanced taste and sped absorption — without regard for safety. When tobacco was a cottage industry, cigarettes were either “roll-your-own” or expensive hand-rolled products with limited market reach; after industrialization, machines rolled as many as 120,000 low-cost, perfectly packaged cylinders daily.
The burgeoning marijuana industry is already following the same successful business strategy by increasing potency and creating new delivery devices. The concentration of tetrahydrocannabinol (THC), marijuana’s principal psychoactive constituent, has more than doubled over the past 40 years. Producers are manufacturing strains that they claim are less addictive or less harmful to mental health, but no supporting scientific evidence has been published. New vaporizer delivery systems developed by some manufacturers may reduce lung irritation from smoking but may also allow users to consume more THC (the component most closely associated with euphoria, addictive potential, and mental health side effects) by enabling them to inhale more often and more deeply. The business community recognizes these innovations’ economic potential: a recent joint venture between a medical-marijuana provider and an electronic-cigarette maker sent stock prices soaring.
Marketing strategies go hand in hand with product innovation. The market for marijuana is currently small, amounting to 7% of Americans 12 years of age or older, just as the tobacco market was small in the early 20th century. Once machines began mass-producing cigarettes, marketing campaigns targeted women, children, and vulnerable groups by associating smoking with images of freedom, sex appeal, cartoon characters, and — in the early days — health benefits.
There is reasonable evidence that marijuana reduces nausea and vomiting during cancer treatment, reverses AIDS-related wasting, and holds promise as an antispasmodic and analgesic agent. However, marijuana manufacturers and advocates are attributing numerous other health benefits to marijuana use — for example, effectiveness against anxiety — with no supporting evidence.
Furthermore, the marijuana industry will have unprecedented opportunities for marketing on the Internet, where regulation is minimal and third-party tracking and direct-to-consumer marketing have become extremely lucrative. When applied to a harmful, addictive commodity, these marketing innovations could be disastrous. This strategy poses a particular threat to young people. Adolescents are more likely than adults to seek novelty and try new products. The developing adolescent brain is particularly vulnerable to the development of addiction. According to the Substance Abuse and Mental Health Services Administration (SAMHSA), children who use marijuana are up to four times as likely as adults to become chronic, heavy users — the type that would generate consistent sales for the marijuana industry.
Today, nearly one in five U.S. adults still smokes, despite extensive public health campaigns focused on reducing uptake and increasing cessation. The tobacco industry has provided a detailed road map for marijuana: deny addiction potential, downplay known adverse health effects, create as large a market as possible as quickly as possible, and protect that market through lobbying, campaign contributions, and other advocacy efforts.
The tobacco industry, bolstered by enormous profits, successfully lobbied to be exempted from every major piece of consumer-protection legislation even after the deadly consequences of tobacco were established. With nothing to sell or profit from, health advocates had difficulty fighting a battle that was clearly in the best interest of the public. The marijuana industry has already formed its own advocacy organization — the National Cannabis Industry Association — to protect and advance its corporate interests.
It took the medical and public health communities 50 years, millions of lives, and billions of dollars to identify the wake of illness and death left by legal, industrialized cigarettes. The free-market approach to tobacco clearly failed to protect the public’s welfare and the common good: in spite of recent federal regulation, tobacco use remains the leading cause of death in the United States.
Addictive substances with known harms may merit completely new policy approaches. For example, the government of Uruguay’s marijuana program will restrict sales to government-produced strains, limit prices in order to undercut illicit markets, and closely monitor individual consumption. The effects and side effects of this approach, however, remain to be seen. At present, we should accelerate collaboration among the Food and Drug Administration, the National Institutes of Health, SAMHSA, the National Highway Traffic Safety Administration, and other agencies to fully understand current harms and forecast the effects of industrialization.
In theory, any revenues from sales of marijuana products should pay for all regulation and harms so that society will not have to pick up the tab for damage done by the product. However, we know from the history of tobacco that this is hard to implement in practice.
History and current evidence suggest that simply legalizing marijuana, and giving free rein to the resulting industry, is not the answer. To do so would be to once again entrust private industry with safeguarding the health of the public — a role that it is not designed to handle.
Source: N Engl J Med 2014; 371:399-401 July 31, 2014
How goes Colorado’s experience with legal marijuana? Spend some time on social media or on numerous blogs and you’ll read headlines like “Revenue Up, Crime Down!” or “Youth Use Declining After Legalisation.”
Lately legalization advocates have been cheering numbers that show a decline in crime. There are literally hundreds of articles that have been written with this narrative. But an honest look at the statistics shows an increase — not decrease — in Denver crime rates.
Crime is tracked through two reporting mechanisms: the National Incident Based Reporting System (NIBRS), which examines about 35 types of crime, and the FBI Uniform Crime Reports (UCR). The FBI UCR only captures about 50 percent of all crimes in Denver, so the NIBRS is generally regarded as more credible. The Denver Police Department (DPD) uses NIBRS categories to examine an array of crime statistics, since it is the more detailed and comprehensive source of numbers.
The Denver Police statistics show that summing across all crime types — about 35 in all — the crime rate is up almost 7 percent compared with the same period last year. Interestingly, crimes such as public drunkenness are up 237 percent, and drug violations are up 20 percent.
So why are advocates claiming a crime drop? Easy: They blended part of the FBI data with part of the DPD/NIBRS data to cook up numbers they wished to see. When one picks the Part I data from UCR and uses DPD/NIBRS property-crime numbers only while studiously avoiding the DPD/NIBRS data on all other crimes, one can indeed manufacture the appearance of a decline. As one can see here, even when using the FBI UCR numbers — in their entirety — crime has risen.
A report commissioned by the National Association of Drug Court Professionals puts it nicely: When a closer look at the data is undertaken, a different picture — something other than “crime is down” — appears to emerge. …
Legalization proponents should not infer causality regarding the downward trend observable when isolating just the UCR’s Part I crime index.
When I asked the president of the Colorado Drug Investigators Association, Ernie Martinez, about these statistics, he urged me to look at the crimes that have been happening in connection to marijuana — even after legalization:
Across the Front Range, we are experiencing more and more butane explosions due to hash extraction methods, calls for service on strong smells, and calls to ER’s on adverse effects after either ingestion or smoked use. Black-market continues to exist unabated, availability of black market marijuana is ever present and cheaper than legalized MJ. Medical marijuana registrants continue to rise due to many factors such as more quantity allowed and more plants allowed, all due to Physician recommendations.
So if crime is up, can we blame legal pot? We do not know whether legalization has anything to do with it. But we do know that reputable news organizations should stop relying on the Big Marijuana lobby for statistics. They wouldn’t blindly trust coal-industry statistics on the environmental effects of strip mining, and they should bring similar scepticism to propaganda claims disseminated by this new industry.
Source: www.conservativewoman.co.uk 13th August 2014
Two new drugs are detected each week across Europe with researchers trying to alert the public to the dangers of new chemicals. Young people have died “horrific deaths” from taking multiple drugs, a senior member of the Forensic Science service in Northern Ireland has said. Twenty people have died in the last year from drugs known as “speckled cherries”. Many more have died from taking a cocktail of other substances.
Forensic expert Peter Barker said it was time for an anti-drugs campaign along the lines of road safety adverts. “We’ve seen some really horrific deaths where people have killed themselves after taking multiple drugs,” he said. “I think we need to be much more stark in the message we send to the public – adverts similar to those we’ve seen in road safety campaigns.” The forensic labs are based in Carrickfergus and they use state of the art equipment to carry out toxicology reports after someone has died.
‘Bucket chemistry’
Mr Barker said so-called legal highs are presenting significant challenges. “We call it bucket chemistry – these drugs are developed in back alley garages,” he added. “They haven’t had clinical trials and no one knows what is in them. They are not safe for people to take, even if they have taken a similar compound before.”
About two new drugs are detected each week across Europe and that means researchers are always trying to stay ahead of the game to alert the public to the dangers of new chemicals. They have the same machines used by the Olympics dope-testers – cutting edge technology that can detect tiny amounts of different substances.
At a recent inquest, Coroner John Leckey described the recent drugs deaths as being similar to having a serial killer on the loose. Mr Barker said the deaths were extremely unpleasant: “They can cause convulsions, palpitations and heart attacks.
“Children do need to be educated about the dangers.”
Source: http://www.bbc.co.uk/news/uk-northern-ireland 21st August 2014
A Liverpool coroner has warned drug users that a batch of tablets containing the ecstasy-like drug PMA (paramethoxyamphetamine) may be circulating in the area. Douglas Fraser issued the warning after recording a verdict of death due to non-dependent use of drugs at the inquest of a 29-yearold Toxteth man, Lee Monaghan, who was found dead at his home on June 8. The investigating pathologist, Dr Jonathan Medcalf, said that Mr Monaghan had a fatal concentration of PMA in his system when he died, as well as traces of alcohol and cocaine. Paramethoxyamphetamine has been used as a recreational drug since the 1970s and has had short periods of popularity in Australia, Canada and Scandinavia.
The substance is a Class A drug under the Misuse of Drugs Act. The drug may be sold as ecstasy or it may be referred to by street names such as ‘cloverleaf’ or ‘Positive Mental Attitude (PMA)’. The drug is chemically similar to MDMA and effects include an increase in energy, visual distortions, a general feeling of changes to consciousness and hallucinations. Reactions after ingestion can include pupil dilation, erratic eye movements, muscle spasms, sharp increases in body temperature, nausea and vomiting. In some cases the drug can lead to convulsions, coma and death.
Anecdotal reports suggest that people who may be used to taking MDMA may find that PMA does not act as quickly as they would normally expect. Users should be warned not to redoes too quickly as increasing the concentration of PMA in the body increases the risk of adverse effects, including fatalities. According to the US Drug Enforcement Agency, doses of less than 50 milligrams (usually one pill) cause symptoms like MDMA, while dosages over 60-80 mg (lower than those used regularly for MDMA) are considered potentially lethal. DrugScope has ascertained that press reports suggesting that Mr Monaghan’s death was the first in the UK to be attributed to the drug are inaccurate. The National Programme on Substance Abuse Deaths confirmed that PMA toxicity was implicated in the death of a 21-year-old Cornish man who died in August 2001.
Source: Drugscope Sept.2011
The Obama administration, driven by the notion that America’s prisons are unjustly filled with first-time marijuana offenders, has condoned marijuana use through an artful blend of inaction and avoidance towards legalization initiatives. Not only has the administration declined to challenge legalization ballot initiatives (or even speak against them during the state campaigns), they have turned a blind eye to recreational marijuana usage by ranking such activities as beneath their “prosecutorial priorities.”
In reality, less than one out of every 200 inmates in a state prison system is incarcerated due to first-time marijuana use or possession. And many of those who are incarcerated have pled down from more serious charges. The fact is most inmates are incarcerated for multiple, non-marijuana drug offenses, often involving trafficking or violence.
Of greater concern, however, is how this prosecutorial neglect will harm the administration’s own efforts to treat substance abuse through the Affordable Care Act.
While the administration’s new policy of neglect won’t substantially reduce drug-related incarceration, it will inflict harm on effective programs in drug prevention and treatment. Though the administration’s rhetoric has stressed a public health approach to curb drug use, their policies will produce short-term harm from increasing marijuana use and long-term damage to the administration’s stated prevention and treatment objectives.
Legal marijuana undermines social norms against drugs, diminishes perceptions of risk, handcuffs the courts as an instrument in treatment, and makes it less likely that the largest category of dependent drug users in need of treatment will pursue a path to their recovery.
Consider the impact on the Affordable Care Act. Initially hailed as a ‘breakthrough’ for substance abuse treatment, the Act mandates expanded insurance coverage for drug treatment with “parity” requirements (comparable to coverage of other medical conditions) that ACA supporters hope will revolutionize health care for the addicted.
Concerns now beset this provision, especially concerning marijuana, which is the largest cause driving treatment need. While the heaviest drug using age cohort (18-25 year olds) should now be covered until age 26 under their parents’ plan, if the ACA falters in its funding assumptions or in some other manner, federal funding for treatment under the old system would be wholly inadequate to cover expanded treatment need spurred by legal, recreational marijuana.
Legal marijuana also has a perverse impact on getting people needed treatment.
The National Survey on Drug Use and Health discloses the problem. Among the 7.3 million Americans in 2012 who met the criteria for needing treatment (4.3 million of whom were dependent on marijuana), high cost or lack of insurance were offered by some as the reasons that they didn’t actually get the treatment they sought. But these problems were cited by fewer than half of those who didn’t get, for any reason, the treatment they wanted. In fact, the entire category of those who sought treatment but failed to get it represents only 1.7 percent of those who needed it.
In fact, a remarkable 95 percent of those who needed treatment for a drug abuse disorder were not seeking it – that is, they are in denial. No provision of an expanded ACA can help those who do not seek their own recovery. Public policy should be designed to motivate those in need to seek help. Regretfully, widely accessible, socially acceptable marijuana provides no incentive for the dependent to enter recovery; rather, such a permissive environment makes it easier for a person to persist in denial and continue the self-destruction of addiction.
Moreover, the legalization mantra has taken its toll on the views of our youth. Perceptions of risk and norms of disapproval are consequential matters, especially for the young. School surveys show that the perceived risk in smoking marijuana regularly has declined among high school seniors from 80 percent in 1991, to only 39 percent in 2013. Norms of social disapproval have a similarly trended downward, from 80 percent disapproval among 10th graders to only 59 percent over the same time period.
Significantly, there is an inverse relationship between these two measures of youth attitudes and their actual rates of marijuana use. In 1992, when use was at an historic low, perceived risk of even “occasional” marijuana use stood at 40 percent, and past-year use by senior high school students was only 20 percent. But by 2013, those figures had reversed: perceived risk had fallen to only 19 percent, while past year use had soared to 39 percent. As researchers know, when perceived risk and disapproval fall, higher rates of youth use will shortly follow. Legal, socially acceptable marijuana will only accelerate this trend.
There is similar jeopardy for drug courts, which serve as an alternative to incarceration for non-violent drug offenders. There are now more than 2,700 such courts, where offenders are directed to treatment, completion of which can lead to clearing their record, with no resort to prison. They are a huge success; in fact, the criminal justice system today is the largest single source of referral for treatment for drugs like marijuana. But the success of these courts in driving treatment will likely suffer as a consequence of legalization, which weakens the criminal justice system as an adjunct to treatment and recovery.
In the end, the administration is undermining effective responses to real problems by peddling a false narrative regarding incarceration and implementing public health policies at odds with its own objectives.
Source: http://thehill.com/blogs/congress-blog/healthcare/208687 June 10, 2014
(New Zealand Health Minister Tony Ryall has welcomed Parliament’s support for the Psychoactive Substances Amendment Act, passed today under urgency by New Zealand parliament. The Act, expected to receive Royal assent on Wednesday and become law on Thursday 8 May 2014, removes all remaining psychoactive products on the New Zealand market. It also bans the use of animal testing data in support of product approvals. “When the Psychoactive Substances Act was passed last year, some products were allowed to stay on the market,” says Ryall. “The amendment means all interim retail and wholesale licences will be cancelled and all psychoactive products given interim approval will be removed from sale. It will also become illegal to possess and supply the products. “While animal testing remains a necessary and important component of the process for developing a number of important products, such as medicines, the government does not believe that such testing was justifiable for the recreational drug market. “The intent of the original Psychoactive Substances Act remains with approved low risk products able to come to market in the future when regulations are made,” Ryall said. All psychoactive products will become unapproved from Thursday and it will be an offence to possess, supply or sell them. Those in possession of products are advised to return them to the retailer they purchased them from. (national.org.nz) *A psychoactive drug is a chemical substance that crosses the blood–brain barrier and acts primarily upon the central nervous system where it affects brain function, resulting in alterations in perception, mood, consciousness, cognition, and behavior.
Source: www.nation.lk www.national.org.nz 6th May 2014
When it comes to tobacco and marijuana, public policies appear headed in contradictory directions. For years, candy cigarettes have been criticized as providing children a gateway to tobacco smoking. In similar fashion, the federal government banned candy and fruit-flavored cigarettes in 2009 as part of an effort to reduce youth smoking.
Yet in Colorado, the legalization of marijuana has produced a rash of candy products infused with tetrahydrocannabinol (THC), the main psychoactive ingredient in pot. THC products include everything from gummy bears to caramels. In some cases, a single piece of candy is the recommended dose, yet packages contain numerous pieces. Once opened, those products can easily be mistaken for traditional candies that are eaten in far larger quantities.
It doesn’t take a genius to see what comes next.
Marshall Allen, writing for ProPublica, recently noted that some children in Colorado are being exposed to THC products. Dr. Andrew Monte, a medical toxicologist at the University of Colorado Medical School and Rocky Mountain Poison and Drug Center, told Allen a poison control call occurs every few days involving a child accidentally eating marijuana products. Similar anecdotal reports are coming from emergency room doctors. In some cases, those children undergo CT scans and spinal taps before the patient’s problem is identified.
“What kid doesn’t want a brownie or a gummy bear?” Monte said.
Cigarette vending machines were once common in the United States, but are rare today because of concerns about youth access. Yet in Colorado, a company has unveiled the first-ever marijuana vending machine. It supposedly has safeguards to prevent youth access, but it’s hard to believe they will prove effective.
These developments are worth noting because some in Oklahoma wish to enact similar pro-marijuana policies here. In the governor’s race, two candidates are running on pro-marijuana platforms: Oklahoma City attorney Chad Moody is challenging incumbent Gov. Mary Fallin in the Republican primary, while 34-year-old motorcyclist Joe Sills is challenging Fallin as an independent candidate. Moody bills himself as “the drug lawyer.” Among other things, his website advises citizens to “never answer police questions” and “never open your door to a stranger, including police.”
In the state’s open U.S. Senate race, state Sen. Connie Johnson of Oklahoma City is seeking the Democratic nomination. She is a longtime proponent of marijuana legalization. At the same time, an initiative petition has been filed with the Oklahoma Secretary of State’s Office seeking a statewide vote to legalize “medical” marijuana. That group has 90 days to gather 155,216 valid voter signatures to place the measure on the ballot.
In evaluating those candidacies and causes, citizens shouldn’t ignore the early lessons of Colorado, nor the ripple effects in neighboring states. In Oklahoma, law enforcement officials report an increase in drug trafficking that originates in Colorado. And the social impacts of marijuana legalization have not been limited to children’s accidental THC exposure.
“The state of Colorado and the state of Washington are seeing significant, both social and enforcement, issues,” Ricky Adams, chief of the Oklahoma Highway Patrol, recently told The Oklahoman’s editorial board. “It’s not all money and tax dollars.”
Practices that have long been discouraged when associated with tobacco are now being nonchalantly embraced in support of marijuana, even as the crackdown on tobacco use (and users) continues.
Perhaps history really does repeat itself — as farce.
Source: www.gopusa.com The Oklahoman April 22, 2014
GEORGIA — Gov. Nathan Deal today plotted a path forward for the safe and legal use of cannabis oil by Georgia children suffering from epileptic disorders. The governor also announced that he and the Department of Human Services will launch pilot projects for public-private partnerships in the state’s foster care system. Deal has consulted with the federal Food and Drug Administration on how the state can begin legal clinical trials with cannabis oil products at Georgia Regents University Augusta. “So far we have identified two tracks worthy of pursuit,” Deal said. “Our most promising solution involves pairing GRU with a private pharmaceutical company that has developed a purified liquid cannabinoid currently in the FDA testing phase. The product contains no THC, which is the component in marijuana that intoxicates a user. The university would create a well-designed trial for children with epileptic disorders, and in order to serve as many children as we can, we would like to pursue a statewide investigational new drug program through a multicenter study that would allow GRU to partner with other research facilities across the state. We have talked with the pharmaceutical company to gauge interest, and the company is willing to continue those initial talks. “Georgia will also possibly pursue a second clinical trial at GRU that would use cannabidiol oil obtained from cannabis product grown by the National Institute on Drug Abuse at its farm located at the University of Mississippi. This road would perhaps take more time because it would require GRU to work through an approval process with NIDA and the FDA. “We do not see these options as mutually exclusive, and we’re looking to move forward on both options at this time. “The General Assembly this year gave serious consideration to legislation that would pave the way for patients in need of cannabis to receive it safely and legally. An issue that could have triggered controversy instead yielded teamwork and a commitment to see this through, as legislators – and I as well – learned the stories of these brave families who are desperately seeking relief for their children’s debilitating conditions. The legislation earned significant levels of support in both houses and in both parties but didn’t make into any bills that reached my desk. “Even if the legislation had passed, we still would need to take these steps, so we haven’t lost any time. As we progress, we’ll determine if the General Assembly needs to take additional action next year.” Georgia Regents University expressed its excitement about the clinical trials. “As the state’s academic health center encompassing a 154-bed children’s hospital, we have a responsibility to address the needs of families whose children are suffering,” said Georgia Regents University President Ricardo Azziz. “We are appreciative of Gov. Nathan Deal for this vote of confidence and look forward to working with the state to establish clinical trials to research the benefits of treating epilepsy and other neurological conditions with cannabidiol oil.”
Source: www.valdostadailytimes.com 10th April 2014
Billionaire philanthropist George Soros hopes the U.S. goes to pot, and he is using his money to drive it there. With a cadre of like-minded, wealthy donors, Mr. Soros is dominating the pro-legalization side of the marijuana debate by funding grass-roots initiatives that begin in New York City and end up affecting local politics elsewhere. Through a network of nonprofit groups, Mr. Soros has spent at least $80 million on the legalization effort since 1994, when he diverted a portion of his foundation’s funds to organizations exploring alternative drug policies, according to tax filings. His spending has been supplemented by Peter B. Lewis, the late chairman of Progressive Insurance Co. and an unabashed pot smoker who channeled more than $40 million to influence local debates, according to the National Organization for the Reform of Marijuana Laws. The two billionaires’ funding has been unmatched by anyone on the other side of the debate. Mr. Soros makes his donations through the Drug Policy Alliance, a nonprofit he funds with roughly $4 million in annual contributions from his Foundation to Promote an Open Society. Mr. Soros also donates annually to the American Civil Liberties Union, which in turn funds marijuana legalization efforts, and he has given periodically to the Marijuana Policy Project, which funds state ballot measures. Lewis, who died in November, donated to legalization efforts in his name and through the ACLU and the Marijuana Policy Project, on which he served as the chairman of the board. Lewis‘ estate declined to comment for this article.
“The pro-legalization movement hasn’t come from a groundswell of the people. A great deal of its funding and fraud has been perpetrated by George Soros and then promoted by celebrities,” said John Walters, director of the White House Office of National Drug Control Policy under George W. Bush. “The truth is under attack, and it’s an absolutely dangerous direction for this country to be going in.” Mr. Soros‘ Open Society Foundations have annual assets of more than $3.5 billion, a pool from which he can dole out grants to pet projects, according to 2011 tax returns, the most recent on file for his charitable organizations. David and Charles Koch, the billionaire brothers who often are cited for their conservative influence, had $308 million tied up in their foundation and institute in 2011. Mr. Soros did not respond to a request to be interviewed.
‘A question of when’ In his book “Soros on Soros: Staying Ahead of the Curve,” he said the U.S. policy of criminalizing drug use rather than treating it as a medical problem is so ill-conceived that “the remedy is often worse than the disease.” Although Mr. Soros didn’t outline an alternative in his book, he wrote that he could imagine legalizing some of the less-harmful drugs and directing the money saved from the criminal justice system to treatment.
“Like many parents and grandparents, I am worried about young people getting into trouble with marijuana and other drugs. The best solution, however, is honest and effective drug education,” Mr. Soros said in a 2010 op-ed in The Wall Street Journal.
“Legalizing marijuana may make it easier for adults to buy marijuana, but it can hardly make it any more accessible to young people. I’d much rather invest in effective education than ineffective arrest and incarceration.” The Drug Policy Alliance stands firmly behind Mr. Soros‘ position.
“Drug use, the use of any substance, is a health issue and we shouldn’t be throwing people in jail for health issues,” said Bill Piper, the alliance’s director of national affairs in Washington. “The No. 1 reason why people with substance abuse disorders don’t seek help is because they’re afraid of getting arrested. From a constitutional and legal perspective, states can legalize marijuana if they want, and there’s nothing the federal government can do,” he said. “State after state decided to end the prohibition of alcohol and forced the federal government to change federal law.
“What we’re going to see over next decade is states repel marijuana prohibition and then the federal government following suit. It’s not a question of whether it’s going to happen; it’s a question of when.” Drug Policy Alliance Executive Director Ethan Nadelmann said in an email that funding levels from Mr. Soros “have bounced around a bit over the years but it’s roughly $4 million per year (i.e., 1/3) of DPA’s general operating budget.”
“Other funding comes from other wealthy individuals (including quite a number who agree with Soros on little apart from drug policy), foundations and about 25,000 people making smaller contributions through the mail and Internet,” Mr. Nadelmann said in the email. Mr. Soros and Lewis, with help from the Drug Policy Alliance and Marijuana Policy Project, helped 2012 ballot initiatives that legalized the recreational use of marijuana in Washington state and Colorado. Federal law still outlaws possession, use, sale and distribution of the drug. Mr. Soros, Lewis and their various nonprofits provided 68 percent of the funding that went to New Approach to Washington, the group that mobilized signatures to get the initiative on the state ballot and then promoted it. The Campaign to Regulate Marijuana Like Alcohol, a grass-roots group that supported pot legalization in Colorado, was established by the Marijuana Policy Project and was 67 percent funded by nonprofits associated with the two billionaires. The campaign then bankrolled Moms and Dads for Marijuana Regulation, a seemingly unassociated group of pro-legalization parents that in reality consisted of only a billboard and a press release, according to state election records.
“The other side has so much money, it’s incredible, and the bulk of it is coming from a handful of people who want to change public policy,” said Calvina Fay, executive director of Save Our Society From Drugs, whose organization was the largest donor to Smart Colorado, the initiative opposed to legalization.
“When we look at what we’ve been able to raise in other states, they raise millions. We’re lucky if we can raise $100,000. It’s been a process of basically brainwashing the public. They run ads, put up billboards, get high-profile celebrity support and glowing media coverage. If you can repeat a lie often enough, the people believe,” Ms. Fay said.
Other states line up Mason Tvert, co-director and spokesman for the Marijuana Policy Project’s Colorado campaign, disagrees. “There simply is no grass-roots support for maintaining marijuana
prohibition,” he said. “Anyone who suggests otherwise is just not paying attention. They’re railing against a public policy that most Americans support.” Mr. Tvert said the Marijuana Policy Project collected no money from Mr. Soros or Lewis for the 2012 initiative. “Not that we would turn away Mr. Soros‘ money in the future,” he said. “There are countless people that want to make marijuana legal, but only so many people who can afford to make it possible.”
Those people are turning out to make the 2014 election cycle look much like the 2012 cycle in Colorado and Washington, state election records show. • In Alaska, the grass-roots Campaign to Regulate Marijuana Like Alcohol has emerged with the help of funding from the Marijuana Policy Project, which gave the campaign its first big contribution of $210,000.
If history repeats itself, then a few months before the election in Alaska, the Drug Policy Action group, the political arm of Mr. Soros‘ Drug Policy Alliance, will start contributing hundreds of thousands of dollars to help fund a media blitz and drive voters to polls to help support the measure.
• In Oregon, New Approach Oregon has collected enough signatures to get a legalization initiative on the ballot and has cashed its first checks: $96,000 from Lewis before he died last year and $50,000 from Mr. Soros‘ Drug Policy Alliance, according to state election records. • In Florida, Mr. Soros has teamed up with multimillionaire and Democratic fundraiser John Morgan to donate more than 80 percent of the money to get medical marijuana legalization on the ballot through its initiative “United for Care, People United for Medical Marijuana.”
Calls to Tim Morgan, John Morgan’s brother who is handling press inquiries, were not returned. The Marijuana Policy Project and Mr. Soros‘ Drug Policy Alliance aim to support full legalization measures in 2016 in Arizona and California — where they have funded and won ballot initiatives for medical marijuana use — and in Massachusetts, Maine, Montana and Nevada, Mr. Tvert said. The Marijuana Policy Project also is “focusing a lot of time and resources passing bills” in Delaware, Hawaii, Maryland, New Hampshire, Rhode Island and Vermont, where it considers legalized marijuana to be a realistic prospect in the next few years, he said.
‘Phony propaganda’ Mr. Soros also is putting money into studies that show economic benefits from marijuana legalization. In Colorado, the Drug Policy Alliance helped bankroll the Colorado Center on Law and Policy’s study that found marijuana legalization could generate as much as $100 million in state revenue after five years. That research was widely considered to have influenced the election. The ACLU also has penned studies supporting legalization, and the Marijuana Policy Project commonly cites these and Drug Policy Alliance research to argue its case for legal marijuana. Calls and emails to ACLU headquarters in New York were not returned, but its website says that “removing criminal penalties for marijuana offenses will reduce the U.S. prison population and more effectively protect the public and promote public health.” Last year, Mr. Soros, via donations from his Open Society Foundation and the Drug Policy Alliance, helped fund Uruguay’s effort to become the first country to legalize the commercialization of pot. He also offered to pay for a study to evaluate the ramifications of the experimental legislation, which he has said will reduce overall drug use and help fight illegal drug trade, according to news reports. “There are addictive, harmful effects of smoking marijuana,” said Mr. Walters, citing studies by the federal government and organizations such as the American Medical Association. “The silliness of pop culture is pretending this isn’t a serious problem. Their entire message is built on phony propaganda that has been far too successful in the mainstream media.” The Drug Enforcement Administration agrees, despite President Obama’s proclamations that marijuana is no worse than alcohol. In the official “DEA Position on Marijuana” paper last April, the agency said marijuana has a “high potential for abuse, [and] has no accepted medicinal value in treatment in the U.S.” It also cited that “a few wealthy businessmen — not broad grassroots support — started and sustain the ‘medical’ marijuana and drug legalization movements in the U.S. Without their money and influence, the drug legalization movement would shrivel.”
Even Mr. Obama’s drug czar said the legalization of marijuana is dangerous.
“Young people are getting the wrong message from the medical marijuana legalization campaign,” drug czar Gil Kerlikowske said in December. “If it’s continued to be talked about as a benign substance that has no ill effects, we’re doing a great disservice to young people by giving them that message.” But the message is being propagated by Mr. Soros and groups of his supporters who have created their own nonprofits and political action committees. Although these organizations appear on the surface to have no affiliation, closer examination shows all are linked through their personnel and cross-promotion. Drug Policy Alliance President Ira Glasser is a former executive director of the ACLU. Marijuana Policy Project co-founders Rob Kampia, Chuck Thomas and Mike Kirshner originally worked at the National Organization for the Reform of Marijuana Laws, which hosts industry conferences attended and promoted by Drug Policy Alliance staff, and has a political action committee that donates to marijuana advocacy candidates. The Marijuana Policy Project’s co-founders also frequently speak at events sponsored by the Drug Policy Alliance. The National Cannabis Industry Association — known as the chamber of commerce for marijuana — was co-founded by Aaron Smith, who previously worked at Safe Access Now, another Soros-backed nonprofit that promotes the legalization of pot. After 20 years trying to influence policy, Mr. Soros‘ army is winning the marijuana debate. Last year, for the first time in four decades of polling, the Pew Research Center found that more than half of Americans support legalizing marijuana, compared with 30 percent in 2000. Lawmakers are following suit, with an unprecedented number of legalization bills brought to the floors of state legislatures.
“It’s only a matter of time before marijuana is legalized under federal law,” said Tom Angell, founder and chairman of the Marijuana Majority, an advocacy group based in Washington, D.C. “We now have 20 states plus the District of Columbia considering legalization efforts, two states have already legalized it for all adults over the age of 21 — politicians will have to follow the will of the people on this.” Or follow Mr. Soros‘ money. Mr. Angell’s group is funded, in part, by a grant from the Drug Policy Alliance.
Kelly Riddell covers national security for The Washington Times.
Source: www.washingtontimes.com 2nd April 2014
If we care about our children’s futures the pro drug lobby’s campaign to dismantle the international drug control system must be resisted
Last week in Vienna the United Nations hosted the 2014 Commission on Narcotic Drugs. This annual review of the world’s drug problem may not sound like the ‘must attend’ event of the year, but that is to underestimate its importance in drug policy politics.
Two years from now at a General Assembly Special Session On The World Drug Problem, the United Nations will carry out a review of global drug policy. There is no doubt that international legal framework that has kept drug use under control will be under threat. For there are powerful lobby groups like the Global Commission on Drug Policy supported by Richard Branson, the international financier George Soros, and the International Drug Policy Consortium all of whom want to dismantle the current legal framework.
They say the ‘war on drugs’ has been lost. The truth is that international drug policy has been a significant success story. The mutually and freely agreed international treaties and drug conventions have kept drug use low – far lower than it was globally at the turn of the 19th and 20th centuries. They have kept it a marginal, as opposed to a mainstream, activity.
The pro-drug lobbies also argue that drug policy should be treated as a health issue. But it is already. Criminal justice systems in the USA and Europe routinely divert drug users and addicts into treatment. Interventions from needle exchanges to methadone have been made freely available by individual nations’ state health systems since the 1980s. But, however successful in reducing immediate harm such interventions are, they come after the horse has bolted the stable door. On their own they do not prevent or control the drug use problem or its collateral damage.
The fact is that drug use (legal or illegal) is a risk factor for a wide range of negative outcomes including mental and other illnesses, school dropout and academic failure, road accidents, unemployment, low life-satisfaction and relationship difficulties. Drug use is intertwined with many social and health issues. It exacerbates all other problems.
It does not just affect the user; it has serious consequences for society as a whole and our demand for drugs in the West negatively affects all regions of the world.
Marihuana is particularly harmful to young people – typically started in adolescence it can adversely impact on the developing brain. It is a ‘gateway’ drug and the scientific evidence of its harms mounts daily.
The legalization and normalization of marijuana in the USA – where its use and its diversion to young people are rising – creates grave concerns for drug policy.
It is in face of the danger of dramatically increased drug use posed by the legalising lobbyists, that Drug Policy Futures, was launched last week. This new alliance represents over 35 organizations from 21 countries and five continents and includes the Drug Free America Foundation.
It is a critically important initiative. I am delighted that so many like-minded groups have come together to promote drug-free environments and to support the associated social norms of responsibility and restraint. I am looking forward to collaborating with Drug Policy Futures to support the international drug treaties and importantly the
Convention of the Rights of the Child. Its purpose, ‘to protect children from the illicit use of narcotic drugs and psychotropic substances’ is critical. We need to be quite clear that any attempt to legalise drugs contravenes this most fundamental of international commitments. By Calvina Fay Executive Director of Drug Free America Foundation
Source: www.conservativewoman.co.uk 26th March 2014
The annual report by the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA), has shown that 11 per cent of Scottish adults used cannabis last year – second only to Italy – compared with an European average of 6.8 per cent, and a UK rate of 8.4 per cent.
The report also showed Scotland has the highest usage of cocaine (3.8 per cent), amphetamines (2.2 per cent) and LSD (0.6 per cent), while ecstasy use came in at 3.2 per cent, second to the Czech Republic, which has a rate of 3.5 per cent.
The figures follow controversy over cannabis classification following UK government drug adviser Professor David Nutt’s sacking last week.
He had spoken out against the decision to reclassify cannabis from a Class C drug to the more dangerous category B.
The EMCDDA’s figures, which are based on the most up-to-date regional cannabis-use statistics, revealed that the Dutch were among the lowest users, with just 5.4 per cent using the drug.
Scottish Drugs Forum director David Liddle said the figures pointed to wider issues about approaches to tackling drug use.
“They raise the question of what is the best route, through education and giving young people information about drug use, or through the legal route,” he said. “The bigger issue is the one of early use, which leads young people on to particular cultures and problematic use of illegal substances, but early drunkenness and smoking are also linked to this.”
A spokesman for the Scottish Government said: “This report highlights why Scotland’s drugs problem cannot be tackled overnight.
“We need long-term cultural change, which is why we launched ‘Road to Recovery’, Scotland’s national drugs strategy.”
Scottish Conservative justice spokesman Bill Aitken said the figures reflected the need for a rethink on drugs policy.
Mr Aitken said: “These are clearly very concerning figures, and the cannabis statistics in particular result from the lack of a firm message from the UK government on cannabis classification.”
Source: http://thescotsman.scotsman.com/scotland 7th Nov. 2009
The legalization of marijuana in Colorado and Washington and President Barack Obama’s recent remarks again headline the marijuana issue.
In spite of the widespread effort to normalize it, Montana knows firsthand the societal problems marijuana can cause. Colorado and Washington are headed for big problems.
Obama, a former pot smoker himself, recently stated that smoking marijuana was no worse than drinking and his soft approach to enforcing federal law all but endorses the use of it. There seems to be a new — if you like your joint, you can keep it — policy in America. In effect, he has undone years of “zero tolerance” and the “drug free” crusade in our schools and communities.
The legalizers agree that marijuana is dangerous for adolescents and argue that it will still be illegal for them. But it’s those under the age of 21 the industry targets. They are the primary users, consuming the majority of illegal drugs and suffering the most from its long-term consequences. As it becomes more socially accepted, usage increases. That was the case in Montana.
By 2011, Montana had the sixth-highest rate of youth marijuana use in the country and the fourth-highest rate of youth addiction.
After U.S. Attorney General Eric Holder announced that those in compliance with their state’s medical marijuana laws would not be prosecuted, the industry in Montana exploded and became a billion-dollar operation. Montana’s chief of the narcotics bureau, Mark Long, testified, “The current situation is a public health and safety disaster as well as a law enforcement nightmare … and an embarrassment to Montana on a national level.” He said Montana was growing so much marijuana it had become a “source country” for illegal export of the drug. Organized crime moved in and one of the world’s largest outlaw motorcycle gangs was involved in running drugs to their East Coast counterparts. Our surrounding states did not consider us good neighbors as can be anticipated by the neighbors of Colorado and Washington.
As a legislator I was inundated with complaints from cities, towns, communities, law enforcement officials, treatment centers and schools about disruption, safety, crime, dropout rates, students stoned and apathetic toward school and life in general. This new enterprise was making drugs so familiar and acceptable that it was changing Montana’s culture.
I heard of growers destroying neighborhoods, reducing the values of homes and of the language, harassment and stench of crowds at the dispensaries. Parents complained that kids could not play in their own yards. Multiple dispensaries set up near schools, targeting our youth.
Students wrote asking who was defending their rights to a safe, drug-free school. They wanted their friends back. Major industries in Montana reported the inability to find job applicants who didn’t test positive for drugs.
The 2011 Montana Legislature reined in the exploding marijuana industry. They passed the repeal of the medical marijuana initiative, which the governor vetoed in a showy display with a branding iron on the front steps of the capitol. Subsequent legislation took out the profit, curbing commercial growing. Those who had moved to Montana to capitalize on the cannabis industry moved on and those who railed against us for ruining cannabis tourism went elsewhere.
The arguments behind legalization are similar to those used to promote “medical marijuana.”
The illogical deluge of propaganda leaves one to wonder if we are not only losing the war on drugs, but the war on common sense as well.
Source: www.greatfallstribune.com 2nd March
————————————————————-
MONTANA SOAP BOX: MARIJUANA CAUSES BIG PROBLEMS
The legalization of marijuana in Colorado and Washington and President Barack Obama’s recent remarks again headline the marijuana issue.
In spite of the widespread effort to normalize it, Montana knows first hand the societal problems marijuana can cause. Colorado and Washington are headed for big problems.
Obama, a former pot smoker himself, recently stated that smoking marijuana was no worse than drinking and his soft approach to enforcing federal law all but endorses the use of it. There seems to be a new — if you like your joint, you can keep it — policy in America. In effect, he has undone years of “zero tolerance” and the “drug free” crusade in our schools and communities.
The legalizers agree that marijuana is dangerous for adolescents and argue that it will still be illegal for them. But it’s those under the age of 21 the industry targets. They are the primary users, consuming the majority of illegal drugs and suffering the most from its long-term consequences. As it becomes more socially accepted, usage increases. That was the case in Montana.
By 2011, Montana had the sixth-highest rate of youth marijuana use in the country and the fourth-highest rate of youth addiction.
After U.S. Attorney General Eric Holder announced that those in compliance with their state’s medical marijuana laws would not be prosecuted, the industry in Montana exploded and became a billion-dollar operation. Montana’s chief of the narcotics bureau, Mark Long, testified, “The current situation is a public health and safety disaster as well as a law enforcement nightmare … and an embarrassment to Montana on a national level.” He said Montana was growing so much marijuana it had become a “source country” for illegal export of the drug. Organized crime moved in and one of the world’s largest outlaw motorcycle gangs was involved in running drugs to their East Coast counterparts. Our surrounding states did not consider us good neighbors as can be anticipated by the neighbors of Colorado and Washington.
Source: www.greatfallstribune 3rd March 2014
Marijuana legalization may be the same-sex marriage of 2014 — a trend that reveals itself in the course of the year as obvious and inexorable. At the risk of exposing myself as the fuddy-duddy I seem to have become, I hope not. This is, I confess, not entirely logical and a tad hypocritical. At the risk of exposing myself as not the total fuddy-duddy of my children’s dismissive imaginings, I have done my share of inhaling, though back in the age of bell-bottoms and polyester.
Next time I’m in Colorado, I expect, I’ll check out some Bubba Kush. Why not? They used to warn about pot being a gateway drug, but the only gateway I’m apt to be heading through at this stage is the one to Lipitor.
Still, widespread legalization is a bad idea, if an inevitable development. Washington state will be the next to light up, in a few months. A measure is heading to the ballot in Alaska this year, along with measures in Oregon and California. As with gambling — also a bad idea, by the way — more states are certain to feel the peer pressure for tax dollars and tourist revenue. I’m not arguing that marijuana is riskier than other, already legal substances, namely alcohol and tobacco. Indeed, pot is less addictive; an occasional joint strikes me as no worse than an occasional drink. If you had a choice of which of the three substances to ban, tobacco would have to top the list. Unlike pot and alcohol, tobacco has no socially redeeming value; used properly, it is a killer.
So the reason to single out marijuana is the simple fact of its current (semi-)illegality. On balance, society will not be better off with another legal mind-altering substance. In particular, our kids will not be better off with another legal mind-altering substance. As the American Medical Association concluded in recommending against legalization in November, “Cannabis is a dangerous drug and as such is a public health concern.” It added: “It is the most common illicit drug involved in drugged driving, particularly in drivers under the age of 21. Early cannabis use is related to later substance use disorders.” And this point, for me, is the most convincing: “Heavy cannabis use in adolescence causes persistent impairments in neurocognitive performance and IQ, and use is associated with increased rates of anxiety, mood, and psychotic thought disorders.” A 2012 study of more than 1,000 New Zealanders from birth to age 38 found that “persistent cannabis use was associated with neuropsychological decline broadly across
domains of functioning, even after controlling for years of education.” Long-term users saw an average decline of eight IQ points. Once again, teenage toking was the problem. The decrease in IQ was linked only to those with adolescent marijuana use, not those who started in adulthood.
“Impairment was concentrated among adolescent-onset cannabis users, with more persistent use associated with greater decline,” the study reported. For those who started as teens, stopping didn’t fully restore functioning. The results, the study concluded, “are suggestive of a neurotoxic effect of cannabis on the adolescent brain.” Please do not argue that Colorado’s law, like those proposed elsewhere, bans sales to those under 21. Ha! I have teenage children. The laws against underage drinking represent more challenge to overcome than barrier to access. And although alcohol seems to be the teen drug of choice among the adolescents I know, the more widely available marijuana becomes, the more minors will use it. If seniors in fraternities can legally buy pot, more freshmen and sophomores will be smoking more of it.
And it’s not as if the kids need encouragement. By the time they have graduated from high school, nearly half have tried smoking pot; 16.5 percent of eighth-graders have. More alarming, the number who perceive great risk from regular use has been plummeting, from 58 percent to 40 percent among 12th-graders, according to a study funded by the National Institute on Drug Abuse. And, that study says, for those who trumpet tight controls on sales to minors, a third of 12th-graders who live in states with medical marijuana and who have used the drug in the past year report that one source is another person’s prescription. Another 6 percent have their own Rx.
Throwing people in jail for smoking pot is dumb and wasteful. Given changing public attitudes — for the first time last year, a majority of Americans supported legalization — Colorado and Washington are apt to be the vanguard states, not the outliers.
If this doesn’t make you nervous, you are smoking something. Maybe even legally.
Source: www.washingtonpost.com 3rd Jan.2014
MERIDIAN — Idaho State Police say they’re seeing a lot more marijuana trafficked through the state than they used to. “Over the last five years, we’ve tripled the amount of drug seizures in regards to marijuana,” said Lt. Brad Doty.
In the last fiscal year, ISP seized 806 pounds of pot on Interstate 84, Interstate 86 and other Idaho highways. Doty says they are already on pace to soundly beat that number again. Just last weekend, state police in American Falls seized more than 100 pounds of marijuana in three separate busts.
Why the increase? Doty says it has nothing to do with anything that’s changed in Idaho, rather within the nearby states. “As those states that surround us lessen their marijuana laws our drug seizures have increased.”
Oregon, California, and Nevada have all decriminalized marijuana and legalized medical marijuana. Washington and Colorado have legalized medical and recreational use.
“So basically, the large grows in Idaho will get you a lot of jail time,” said Doty. “Large grows in those states where it’s not a crime to possess marijuana, won’t.”
Doty says traffickers often take marijuana from those legal grow sites in those other states and bring it into and through Idaho to the Midwest to sell it. Since it’s illegal here there’s higher demand and bigger profits, which is why Doty also believes this trafficking trend will only continue. “The seizures are getting larger and larger, some of the largest I’ve ever seen in my career.”
But, Doty says traffickers often aren’t just trafficking drugs, they’re committing other crimes too. “It can trickle into other aspects of law enforcement. So, whether that’s thefts or burglaries or other crimes that are all contributed to or surround drug interdiction or drug enforcement. So, the more marijuana that we can seize off the road, obviously leads to more convictions with other crimes, as well.”
Fourteen weapons were seized during drug trafficking busts last year.
Doty also stressed that not all users are traffickers, but reminded everyone that Idaho doesn’t issue or recognize medical marijuana cards.
In order to help battle this trafficking, ISP is adding three drug detection dogs next year.
Source: www.nwcn.com November 13, 2013
The legalization of drugs will have harmful effects on society, and a discussion that fails to acknowledge this is ridiculous
Since Del. Heather Mizeur, a candidate for governor, announced a plan to legalize marijuana in Maryland, there has been a great deal of discussion of the issue. The Baltimore Sun called for a more measured approach that avoided the risk of “rushing to embrace a sweeping but untested new policy that could create as many problems as it solves.” In an op-ed in The Sun, Walter Olson, a fellow at the Cato Institute, derided conservative opposition to Ms. Mizeur’s drug legalization proposal and regurgitated many of the arguments that have been made by legalization advocates for decades.
What has been missing from the discussion, however, has been an honest analysis of both the impacts of broad legalization and the true intent of its advocates. Such a discussion would, no doubt, quickly chill any public momentum toward marijuana legalization.
Delegate Mizeur’s proposal is the next step in a well established playbook that drug legalization advocates have been employing in states throughout the country.
First comes a focus on marijuana, a drug that legalization advocates claim is harmless, and a proposal to decriminalize it for only those with serious medical conditions. The second play is a call for the full legalization of “medical marijuana,” often with provisions wide open to fraud and abuse. And finally, as we have seen in Washington and Colorado, advocates seek full pot legalization, making wild claims of new revenue and greater resources for other police priorities, among other benefits and no acknowledgment of the downsides.
This creeping approach to legalization of marijuana is always bolstered by arguments that also support legalization of all drugs. It is pretty obvious where the drug legalization advocates next target is and what their ultimate goal will be: full legalization of all drugs. Of course, few advocates would dare say such a thing openly, but the direction of their logic is straightforward and undeniable.
Mr. Olson argued that the coming debate would include the question of “What business is it of the government what citizens do behind closed doors?”
The question Mr. Olson raises is the quintessential argument behind legalization of all drugs, not just marijuana. It embodies the excesses of the Libertarian philosophy, sacrificing all practical consideration for purity of ideology. A corollary of the “behind closed doors” rationale of drug legalization is the constant refrain of the “failed war on drugs.” While the prisons are allegedly full with those incarcerated for using and selling marijuana, they are also full of users and dealers of every manner of drug, as well as murders, rapists and thieves. Have we lost the War on Murder as well? If so, should we simply declare our surrender and legalize it? Why is that concept any less absurd than the legalization of drugs because drug use has not stopped?
We then come to the argument that does differentiate pot advocates from those favoring full drug legalization, the contention that marijuana is a harmless drug that many celebrities and captains of industry have indulged in. Only in the warped mind would a vice become a virtue when committed by the “successful.” Many legalization advocates point to the prosecution of young offenders, their lives ruined not by their conscious choice to engage in illegality but by the oppressive state seeking to stamp out a harmless vice. They lament their children’s bright futures threatened by what they insist is the inevitability of illicit drug use. Of course, this argument pushes the envelope of the free-condom, lack of personal responsibility, entitlement culture in which too many young people are raised. Drug legalization will not prevent the penchant for teen self-destruction, and its justification on such a basis speaks far more about a generation of parents than their children.
In 2005, the DEA issued a publication entitled “Marijuana: The Myths Are Killing Us.” One by one, the myths of marijuana’s harmlessness were deconstructed. Among the details documented in the report were: smoked marijuana is a health danger without any medicinal value; decriminalization and legalization efforts in other countries have led to increased usage among teens; and use of marijuana has a demonstrable harmful impact on nonusers.
The simple, undeniable reality is that the legalization of drugs will have harmful effects on society and a discussion that fails to acknowledge this is folly.
Source: Gregory Kline is a frequent contributor to Red Maryland, a conservative radio network and blog whose content appears regularly in The Baltimore Sun and on baltimoresun.com. His email is: gregorykline@aol.com.
When teams hailing from Denver and Seattle solidified spots at Sunday’s Super Bowl XLVII, it wasn’t just talk of two No. 1 seeds duking it out or even Richard Sherman’s antics, but the states’ recreational marijuana sales policies that got the online world buzzing about the “Marijuana Bowl.”
Even the U-T San Diego polled readers online positing: “Should California legalize pot to help the Chargers get to the Super Bowl?” Some even took to social media with memes depicting a football with green laces in the shape of a pot leaf. It’s getting such laughs that one might be quick to dismiss the documented harms of marijuana use, particularly among teens.
Smart Approaches to Marijuana, or SAM, a national alliance of organizations and individuals dedicated to a health-first approach to marijuana policy, recently presented on the outcomes of Colorado’s policy, starting with legalizing marijuana for medical use in 2001. The presentation focused on the years from 2006 to 2012, a span of time when the number of dispensaries grew to 532, thereby vastly increasing the access and availability of marijuana.
During that time, the use of marijuana among teens spiked, while the perception of harm plummeted significantly. In fact, marijuana use among Colorado teens is currently fifth in the nation — 10.7 percent compared with the national average of 7.6 percent, the report found. Drug-related referrals for high school students testing positive for marijuana increased 150 percent.
Diversion to young people was also commonplace. About 74 percent of Denver teens in drug treatment said they used someone else’s medical marijuana card an average of 50 times, according to SAM. Of serious public safety concern; Colorado traffic fatalities involving drivers testing positive for marijuana rose by 112 percent between 2006 and 2011.
Despite these public health and safety issues, as well as the Colorado State Auditor showing poor regulation or none at all, voters proceeded to legalize the drug for recreational use. But local governments in Colorado seem to understand they foot the bill for public safety — four of the 10 largest cities in Colorado have opted to prohibit the sale of recreational marijuana, and five others have moratoriums.
Today, nine more states, including California, could be facing recreational legalization initiatives on the ballot by 2016. Despite these steps toward legalization, San Diego County continues to succeed in pushing back against the pro-pot movement.
In 2012, voters across San Diego rejected ballot propositions in various cities to zone marijuana dispensaries where they are currently banned, and Californians defeated Proposition 19 to legalize the recreational use of marijuana.
On a local level, the North Coastal Prevention Coalition (NCPC) recently led an evaluation of its efforts to counter pro-marijuana influences between 2004 and 2012. Conducted in partnership with California State University San Marcos, and funded through the federal Substance Abuse and Mental Health Services Administration’s Service to Science Initiative, the evaluation compared student survey data from NCPC’s region and other areas of California.
The bad news — marijuana use in the past 30 days and over a lifetime increased in all regions studied from 2004 to 2010. The good news — the increase was significantly less in NCPC’s region, where the reported ease of access declined. Implementing a comprehensive set of strategies developed in collaboration with the HARM Initiative (Health Advocates Rejecting Marijuana) reduced the retail availability of drug paraphernalia and marijuana, as well as community and media messages that trivialized marijuana use.
One example of an effective strategy aimed at public events pushed a vendor policy prohibiting the sale of “tobacco, tobacco/drug paraphernalia, or any item that promotes the use of illicit drugs.” First adopted by Oceanside Harbor Days, the policy is now implemented at more than 20 events countywide, including the San Diego County Fair. These 20 North County events have an annual attendance of more than 2 million people.
Ultimately, we’re fighting for the health and public safety of San Diego County residents through comprehensive public policies, but it will take collective action to make it last. The voices of our community leaders make a world of difference in the lives of so many. While it might be amusing to some, the downplaying of illegal drug use influences young people to falsely believe its harmless.
It’s crucial now, more than ever, that we stand firm rather than punt on the well-being of adolescents in San Diego County and throughout California.
Pearson, a Carlsbad resident, is vice president of the North Coastal Prevention Coalition, www.northcoastalpreventioncoalition.org
Source: http://www.utsandiego.com/ 30th Jan. 2014
Good luck to the people of Colorado. They’ve made it easier for drug cartels to tap into their children’s latent desire to experiment with marijuana.
Adults 21 and older now can buy marijuana legally for recreational use in Colorado. As of Thursday, residents and visitors can go to a state-regulated pot center, ask for an ounce or less, and pay the over-the-counter price. Just like the Obamacare rollout, no one knows exactly what they’re getting; Colorado hasn’t established a price structure, leading one Denver shop to sell one-eighth of an ounce of “high-quality” marijuana for $70. That’s in sharp contrast to state-licensed pot centers filling medical prescriptions at $25 an ounce.
It also creates a new governmental bureaucracy of state-paid pot shop inspectors, and all the expenses that come with it. Anyone who thinks tax revenue from pot sales will pay for Colorado’s new schools and roads is seriously deluding themselves.
So while the adults turn to pot for recreational purposes, what are the kids to think? In this case, they might be just as confused as their pot-smoking parents.
No doubt, kids below the age of 21 will be out to experiment with marijuana, knowing the worst that can happen is a civil penalty and small fine.
And since they can’t buy it legally like their parents, they’ll get it from drug dealers who now have a better mass market than previously when pot was outlawed. Why’s that? First, drug dealers will set prices that undercut the Colorado-regulated market. Second, the drug dealers probably will be kids themselves, taking advantage of a loosey-goosey situation to make a few bucks. Third, there will be parents who, believing they are protecting the children, will insist that the kids smoke pot at home under adult supervision.
This is a Colorado crisis in waiting. Over time the legalized use of a drug that impairs judgment will lead to dangerous consequences and have a deleterious impact on society. It’s too bad the children are caught in the middle of the adults’ urge for getting high for fun.
Massachusetts must resist the temptation to follow Colorado’s delusion. We’ve already legalized medicinal marijuana and that should be the extent of it.
Source: www.sentinelandenterprise.com 5th Jan.2014
December 16, 2013
By Robert DuPont
White House “Drug Czar” (1973-1977)
Uruguay has become the world’s first country to legalize the growth, consumption, and trading of marijuana, highlighting the impatience that many have for the protracted Drug War. Former White House Drug Czar Robert DuPont argues that legalization of prohibited drugs will not lead to their disappearance on the black market.
According to the pro-drug lobby – and with a boost from the media – Uruguay is leading the world by legalizing marijuana. The pro-drug lobby claims that prohibition is a failure and that all drugs should be legalized. Marijuana, the most widely used illegal drug in the world, is just the leader of this campaign. The strategy takes its precedent from the legalization of the sale of alcohol, but the policy is disarmingly simplistic and presents a terrible threat to public health and safety.
Alcohol and tobacco are the leading preventable causes of illness and death in the United States and the rest of the developed world. This is not because they are more dangerous than drugs that are currently illegal, but because they are legal and commercially produced and distributed.
Legalizing marijuana would not stop the production, sale, or use of illegal marijuana.
Look at the numbers: In the United States, 52 percent of those aged 12 and older drank alcohol in the past month, and 27 percent used tobacco, but only nine percent used any illegal drug and only seven percent used marijuana. This indicates that prohibition is successfully deterring illegal drug use. While prohibition is not without real costs, and today’s drug policy can be improved, our balanced and restrictive drug policy is limiting the damage done by illegal drug use in the United States and around the world.
The promises of drug legalization are bogus. Legalizing marijuana would not stop the production, sale, or use of illegal marijuana. If marijuana were taxed and regulated, there would be plenty of marijuana grown and sold on the black market. Furthermore, normalizing marijuana use would increase demand in both the legal and illegal markets.
The tax bonanza promoted by legalization advocates is hard to take seriously. Legal marijuana sales would struggle to compete with black-market sales, which would continue to provide more potent products at lower, tax-free prices. To the extent that there would be tax revenues from legal marijuana, they would pale in comparison to the social costs. In the United States, the tax revenues from alcohol and tobacco are far less than their social costs. Is this an attractive precedent? I don’t think so.
The public has been led to believe that this politically potent movement is just about marijuana. It is not. Every argument made today in support of marijuana legalization is also being made – or will be made – for other illegal drugs.
The real drug-abuse challenge facing the world today is seldom recognized, let alone debated. It is rooted not in politics, but in biology. Drugs of abuse, including marijuana, target the brain’s reward system more intensely than natural pleasures such as food and sex. Drugs are addicting not because users experience withdrawal when they stop using them, but because they produce a brain reward that the once-addicted brain never forgets. That is why relapses to drug use are so common long after all withdrawal symptoms have passed.
Legalizing drugs, including marijuana, is absolutely not the new and better idea to reduce the toll of illegal drug use.
To combat the rising demand for illegal drugs around the world, we must fashion more effective strategies to limit the use of drugs of abuse outside legitimate and controlled medical situations – strategies that are affordable and compatible with contemporary laws and culture. This is an enormous task, but one that can be completed with international cooperation and leadership. Drug use can be reduced by, among other things, implementing strong prevention strategies, increasing access to treatment, improving quality of treatment, and leveraging the criminal justice system to reduce drug use while also reducing recidivism and incarceration. Legalizing drugs, including marijuana, is absolutely not the new and better idea to reduce the toll of illegal drug use.
As for Uruguay, President José Mujica and his legislature have produced a media sensation. It is difficult to imagine that legalizing marijuana as envisioned in Uruguay’s proposed law could result in the reduction of Uruguay’s role as a country used for drug transit for Paraguayan marijuana and Bolivian cocaine. Monitoring the outcomes of this policy change is enormously important. Sadly, there is little doubt that the new law will encourage the use and sale of marijuana and other drugs of abuse both in Uruguay and in the international marketplace.
Having spent four decades working to reduce drug use and lower the devastating public-health costs of drug abuse, I struggle to understand why so many otherwise sensible and responsible people accept the drug legalization hogwash.
Today CALM (Citizens Against Legalizing Marijuana) joins with the rest of the World community in mourning the passing of Nelson Mandela.
In a world beset by forces of enslavement and bondage, Nelson Mandela was a poetic and articulate voice – and often a lonely voice – on behalf of freedom from those evil forces. His leadership not only erased the toxins of Apartheid from his beloved homeland, but also resulted in the creation of a new nation, one based on freedom, justice and reconciliation.
Nelson Mandela had a keen understanding that enslavement comes in all forms, and recognized and fought against the bondage of drug use. His very words on this subject should give pause to the politicians bent on increasing the availability of enslaving drugs:
“We should never underestimate the dangers of the drug problem and the high price that it exacts from many countries, including our own. It is a serious threat not only to moral and intellectual integrity of our nation and other nations. It is a serious threat to the health and well being of our people.”
“Drug trafficking and corruption pose serious problems for South Africa and for most African countries. The problem is exacerbated by the fact that cultivation and manufacturing of drugs such as cannabis and mandrax are also being done in our sub-region.”
In recognition of the lasting imprint made by this great man, CALM today announces its intent, beginning in December 2014 and every year thereafter to confer the Nelson Mandela Freedom from Drug Enslavement Award on the person who has contributed singularly to freeing people from the enslavement of drug use. Of course, for 2013 and for all of the years preceding this year, our first award is conferred on Nelson Mandela.
Source: CALMca.org: 12/11/2013
In two years of work as an undercover officer with a drug task force, Mike Dillon encountered plenty of drugs. But nothing has surprised him as much as what he has seen in schools lately. Dillon, who is now a school resource officer with the Mesa County Sheriff’s Department, said he is seeing more and younger kids bringing marijuana to schools, in sometimes-surprising quantities. “When we have middle school kids show up with a half an ounce, that is shocking to me,” Dillon said. The same phenomenon is being reported around Colorado after the 2010 regulation of medical marijuana dispensaries and the 2012 vote to legalize recreational marijuana. There are no hard numbers yet because school disciplinary statistics do not isolate marijuana from general drug violations. But school resource officers, counselors, nurses, staff and officials with Colorado school safety and disciplinary programs are anecdotally reporting an increase in marijuana-related incidents in middle and high schools. “We have seen a sharp rise in drug-related disciplinary actions which, anecdotally, from credible sources, is being attributed to the changing social norms surrounding marijuana,” said Janelle Krueger. Krueger is the program manager for Expelled and At-Risk Student Services for the Colorado Department of Education and also a long time adviser to the Colorado Association of School Resource Officers. Krueger said school officials believe the jump is linked to the message that legalization (even though it is still prohibited for anyone under 21) is sending to kids: that marijuana is a medicine and a safe and accepted recreational activity. It is also believed to be more available. Marijuana that parents or other adults might have kept hidden in the past may now be left in the open, where it is easier for kids to dip into it to sell, use or, in some cases, simply to show off, said school officials and law enforcement. “They just want to be cool,” said Dillon of some of the younger students he has seen with pot at school. Krueger, who has been an adviser to resource officers across Colorado for 17 years, said she has heard many stories from officers about kids bringing pot to schools. One that an officer related at a meeting recently involved a student dropping a small baggie of marijuana from his pocket as he was walking down a school hallway. The school principal was walking past the student at the time and picked up the pot. He asked the student if it belonged to him. The student immediately admitted it was his and reached out to take it back from the principal. What struck Krueger and the officer about this incident was the fact that the student didn’t seem to realize that there was anything wrong with having the pot or that there would be any disciplinary consequence for it. The officer said the student acted like having marijuana was an ordinary thing and no big deal. Jeff Grady, a Grand Junction school resource officer who has spent 25 years working in schools, tells a story about sitting in his car at a park near Grand Junction High School one day watching groups of kids through binoculars because they come to the park to smoke on lunch breaks. “Kids are smoking before school and during lunch breaks. They come into school reeking of pot,” he said. “They are being much more brazen.” He said school officials call him and he talks to the kids, but it is a little more difficult now to cite them if they aren’t caught in the act. They can say that they were around an adult medical marijuana user and weren’t smoking themselves, Grady said.
The best quantifiable evidence the state has yet to indicate that marijuana is a significantly growing problem in schools comes from the 2012-13 report that documents why 720 students were expelled from public schools across Colorado. For the first time, marijuana was separated from other drugs when school officials were asked to identify the reason for students’ expulsions. Marijuana came in first. It was listed as being a reason for 32 percent of expulsions. National statistics also point to marijuana being more prevalent in schools. The National Institute of Drug Abuse found that marijuana use has climbed among 10th- and 12th-graders nationally, while the use of other drugs and alcohol has held steady or declined. Marijuana is the only drug showing steady increases, the ” Monitoring the Future” study showed. Christine Harms, director of the Colorado School Safety Resource Center, said the increase of marijuana in schools is not just a problem for school resource officers to grapple with. It was discussed when school psychologists met in Vail last week. “They are seeing more incidents of kids smoking and thinking it is a safe thing to do. More kids are saying they are getting it from their parents,” Harms said. She said counteracting the message legalization is sending to kids is especially difficult now because federal grants for drug abuse prevention have been cut. She and other officials urge parents to take the lead with help from the Speak Now Colorado program that guides parents in how to talk about substance abuse. “They need to know how destructive it is to the adolescent brain,” Harms said.
Source: www.denverpost.com 11.11.23
Largest medical group in the US explicitly rejects calls to become “neutral” on legalization; supports full funding of the Office of National Drug Control Policy; calls for proper study of Colorado and Washington policies. It joins the American Psychiatric Association, who issued a statement last week outlining the public health harms of marijuana.
NATIONAL HARBOR, MD-The delegates at the 2013 Interim Meeting of the American Medical Association (AMA) House of Delegates, in National Harbor, Maryland, today voted to pass a resolution on marijuana, “Council of Science & Public Health Report 2 in Reference Committee K,” explicitly opposing marijuana legalization – fending off a challenge to “neutralize” their position. The report changes H-95.998 AMA Policy Statement on Cannabis to read in part that: “Our AMA believes that (1) cannabis is a dangerous drug and as such is a public health concern; (2) sale of cannabis should not be legalized.”
“The AMA today reiterated the widely held scientific view that marijuana is dangerous and should not be legalized,” commented Dr. Stuart Gitlow, Chair-Elect of the AMA Council on Science and Health and SAM Board Member. “We can only hope that the public will listen to science – not ‘Big Marijuana’ interests who stand to gain millions of dollars from increased addiction rates.”
Additionally, the report called for several provisions consistent with Project SAM’s marijuana pillars, including efforts to “discourage cannabis use, especially by persons vulnerable to the drug’s effects and in high-risk situations…support the determination of the consequences of long-term cannabis use through concentrated research, especially among youth and adolescents… support the modification of state and federal laws to emphasize public health based strategies to address and reduce cannabis use.”
“The American Medical Association took a bold step today, and they should be commended,” commented former Congressman Patrick J. Kennedy, SAM’s co-founder. “By explicitly rejecting calls to neutralize their anti-legalization position, they are sending a loud and powerful message to state and local decision makers, the Federal government, and the general public that to be on the side of science is to oppose efforts to expand marijuana use and addiction.”
Furthermore, several other elements in the report are consistent with SAM’s pillars, including calls to support: “the availability of and reduction (of) the cost of treatment programs for substance use disorders…a coordinated approach to adolescent drug education…community-based prevention programs for youth at risk to fund the Office of National Drug Control Policy… greater protection against discrimination in the employment and provision of services to drug abusers.” The report sums up much of these policy initiatives as a public health approach to marijuana use, which SAM wholeheartedly supports.
The AMA report follows an American Psychiatric Association position paper released last week, which concluded: “There is no current scientific evidence that marijuana is in any way beneficial for the treatment of any psychiatric disorder. In contrast, current evidence supports, at minimum, a strong association of cannabis use with the onset of psychiatric disorders. Adolescents are particularly vulnerable to harm, given the effects of cannabis on neurological development.” Source: www.learnaboutsam.com 9th Dec.2013
A doctor who runs a drug treatment clinic for youth in Colorado says legalizing marijuana has led to many problems in his state and also carried over into Iowa. Dr. Christian Thurstone recently met with drug prevention groups in Iowa. “We’ve seen referrals to substance treatment, to adolescent substance treatment skyrocket — they’ve quadrupled in the last couple of years. We’ve seen used rates, prevalence of use among teenagers — go up significantly, pre-post,” Thurstone says.
He says there are other problems created by marijuana. “We’ve seen a doubling in traffic fatalities, with a driver who is positive for marijuana, double since 2006. We’ve seen school expulsions go up 40-percent pre-post 2010 when we had our defacto legalization of marijuana,” according to Thurstone.
Thurstone says three peer-reviewed medical articles have documented widespread abuse of medical marijuana. “We’ve documented that teenagers who use medical marijuana have more severe addiction than those who don’t use medical marijuana, just because of the potency of medical marijuana products that they’re using,” Thurstone says. He says the legalization has led to some ironic circumstances for the kids he sees in his Denver practice. “Sometimes people will be in treatment for marijuana addiction, yet they will also have a medical marijuana card,” Thurstone says.
He says Iowa has also been impacted. “In terms of the internet advertising of marijuana products, and the specific marijuana products which have tripled the number interdictions of marijuana coming from Colorado to Iowa the last few years. So, there are people who are really trying to change the current patterns of marijuana use in Iowa,” according the Thurstone.
Thurstone made a couple of appearances in Iowa last week. One was in his role as board member of the group “Smart Approaches to Marijuana” or SAM.
Source: www.radioiowa.com 18th Nov.2013
Transport Minister Gerry Brownlee says Cabinet has agreed to lower the legal blood alcohol limit from 80 to 50 milligrams of alcohol per 100 millilitres of blood for drivers aged over 20.
“Legislation to bring about this change will receive its first reading before the House rises for the Christmas break,” Mr Brownlee says.
“Alcohol impairment is a major cause of road accidents in New Zealand, with an average of 61 fatalities, 244 serious injuries, and 761 minor injuries every year caused by at-fault drivers who have been drinking.
“The social cost of these injuries and fatalities is $446 million – a huge sum in a country of our size.”
A two year review of the impact of lowering the legal blood alcohol limit by 30 milligrams suggests 3.4 lives will be saved a year and 64 injury causing crashes avoided – and save $200 million in social costs over 10 years.
“Data collected by Police over the past 22 months shows 53 drivers were involved in fatal and serious injury crashes with blood alcohol readings of between 51 and 80 milligrams per 100 millilitres of blood,” Mr Brownlee says.
It’s proposed the new regime will impose civil infringements on drivers with between 50 and 80 milligrams of alcohol per 100 millilitres of blood. Drivers testing positive for this lower limit will receive a $200 fine and gain 50 demerit points. “This is not a soft option,” Mr Brownlee says.
“Drink driving is a serious matter and I would note that accumulation of 100 demerit points for driving related offences in any two-year period can lead to three months’ suspension of a driver’s licence.” Testing positive to over 80 micrograms of alcohol per 100 millilitres of blood while in charge of a motor vehicle will remain a criminal offence.
“We know that drivers with a very high blood alcohol concentration, and recidivist drink drivers, are responsible for a much higher proportion of alcohol related road fatalities,” Mr Brownlee says. “That is why we believe this fine-based approach at the lower end is most appropriate.” Mr Brownlee says the Government has a strong record on road safety and today’s decision reinforces that.
Source: www.vixy.co.nz 4th Nov. 1213
This letter to the Editor followed a front page article in the New York Times which was judged to be from a pro-marijuana perspective.
—————-
Kennedy and Sabet address what wasn’t said in the NY Times’ front page article about medical marijuana in CA. Ill Effects of Marijuana To the Editor: By focusing on changes in California marijuana use since 1996, and then citing a controversial study called into question by some leading think tanks and experts in marijuana policy, “Few Problems With Cannabis for California” (front page, Oct. 27) does not reflect the growing reality of marijuana as a public health and safety threat in that state. First, the important year to look at in California isn’t when the medical marijuana initiative passed – 1996 – but rather when it was implemented in the form of “dispensaries,” around 2004. And since then there has been a rise in marijuana use and marketing. Second, the single academic study used to substantiate the article’s thesis can be called into question for many reasons, including its silence about research that does not conform to the authors’ pro-legalization perspective. That research finds that legally protecting dispensaries equals more marijuana use and more problems. Finally, absent from the article was any perspective from educators, prevention groups or treatment centers in California, who have reported that as marijuana has become more normalized and accepted, their work has become harder and, in the case of treatment centers, much more in demand. Also, there was little about the mental or physical health effects of marijuana. Those are not outcomes of marijuana use that should be brushed off, even if bringing them to light hurts the prospects for full legalization in 2016.
Source: New York Times Opinion Pages October 2013
This article shows a clear link between marijuana legalisation in the USA and use amongst teenagers.
————————
At a time when more states are legalizing marijuana for medical or recreational purposes, marijuana use among the nation’s youth is rising, a psychiatrist who specializes in addiction said at a conference Friday.
In a presentation entitled, “Not a Harmless Drug: Prevention and Treatment of Marijuana Addiction,” Kevin P. Hill, an addiction psychiatrist at McLeanHospital in Belmont, Mass., and an assistant professor of psychiatry at Harvard Medical School, described what he says is a clear correlation between marijuana legalization and its use among teenagers.
Unlike alcohol use, which society generally recognizes can be dangerous, Hill said, “Many [people] feel that marijuana is harmless, despite science that shows otherwise.”
About 16 percent of youths and 9 percent of adults who use marijuana become addicted, Hill said, “but for those people it becomes very addictive.”
In a brief phone interview after the presentation, Hill said his findings are supported by a 2012 national survey funded by the National Institute on Drug Abuse, a division of the National Institutes of Health, that showed “continued high use of marijuana” among 8th-, 10th- and 12th-graders, combined with a drop in perceptions about its potential harms. Marijuana use among teens has been rising since 2008, the study reported. Hill pointed to a chart with data from the federal government’s 2009-2010 National Survey of Drug Use and Health that showed states with medical marijuana laws tended to have higher-than-average rates of marijuana use among people ages 12 to 17 and 18 to 25.
The chart was prepared by Educating Voices Inc., a nonprofit “founded to proactively support education and communication of the dangers of marijuana and other drugs,” according to its website.
Though more is now known about how addiction hijacks the brain’s frontal lobe, which regulates impulses, Fiori said, long-term effects of drug abuse on adolescents is not as well researched.
Source: www.providencejournal.com 25th Oct. 2013

Scratch and sniff cards to help people detect cannabis farms have resulted in a 28% increase in reports of cultivation, Crimestoppers said.
More than 200,000 cards were issued by the charity to hotspots including London, Greater Manchester, Merseyside, South Yorkshire and Avon and Somerset . The cards release a scent that replicates the growing plant to help people identify the smell of cannabis.
The initiative was inspired by a pilot set up in Holland three years ago.The three-month campaign was launched by Crimestoppers in March. Since then the crime-fighting charity said it had received more than 3,500 pieces of information from the public on cannabis cultivation – a 28% increase on the same period last year.
‘Innovative ways’
Using the information generated, the Metropolitan Police seized more than £2.1m worth of the drug and closed down 34 cannabis factories.
Merseyside Police received a 56% increase in pieces of intelligence in the first month of the campaign and at least 25 cannabis farms were identified.
Whilst South Yorkshire Police seized £89,000 worth of cannabis plants and made 15 arrests.
Mark Hallas, the charity’s chief executive, said the organisation’s commitment to fighting crime had “never been stronger”. “We continue to be proactive and determined in exploring new and innovative ways to educate, empower and encourage the UK public to put their trust in Crimestoppers,” he said.
“Working with communities and government agencies, we believe Crimestoppers to be a truly effective crime-fighting charity that will continue to have a highly significant and successful impact on keeping communities safe.”
Source: BBC News 22nd Oct. 2013
A possible future legalization of cannabis (marijuana) would lead to wide commercial access of cannabis and an increase in the cannabis-using population, as found in other countries. As reported in many studies, increased cannabis use leads to a later increase in psychoses, especially schizophrenia. T.H. Moore and colleagues in the Lancet, 2007, concluded that there was “sufficient evidence to warn young people that using cannabis could increase their risk of developing a psychotic illness later in life”.
For example, cannabis use in the UK increased four-fold between 1970 and 2002, and increased 18-fold in the under-18s. They estimated that new cases of schizophrenia would increase by 29% in men between 1990 and 2010. In fact, it was later found that the annual new cases of schizophrenia and psychoses increased from 49 per 100,000 in 1996 up to 77 per 100,000 in 1999, an increase of 58% over three years.
In the canton of Zurich, Switzerland, cannabis use in 15-16-year old boys went up from 15% in 1990 to 50% in 2002. This was followed by a doubling in hospital first admissions for psychosis and schizophrenia in those aged 15 to 24. A major study by Zammit and colleagues in 2008 found that 1.1% of 1,648 Swedish men conscripts for military service who had ever used cannabis prior to 1970 subsequently developed schizophrenia, two-fold higher than those who never used cannabis. This went up to six-fold higher in those who ever used cannabis 50 times or more.
In general, studies found that psychosis occurs 2 to 8 years after a significant amount of cannabis use, and that the risk of psychosis is higher when cannabis use starts at an earlier age. An Australian study of 83 reports found that cannabis users had an age of onset of psychosis that was 2.7 years younger than non-users. Alcohol use was not associated with an earlier age of psychosis onset. In The Netherlands men cannabis users had a first psychotic episode 7 years younger than non-users.
Any future increases in cannabis-associated new cases of schizophrenia would add to the current high rate in Canada and the USA. M.-J. Dealberto at Queen’s University in Ontario found that the rate of new cases of schizophrenia in Canada is about 26 per 100,000 per year, considerably higher than the countries outside Canada which average about 12 new cases per 100,000 per year. (Quebec is even higher at 40.)
In addition, such an increase in new schizophrenia cases would need to be matched by significant increases in psychiatric hospital budgets and in community-based housing and welfare. For example, Ontario’s two major psychiatric centers (Ontario Shores Centre for Mental Health Sciences in Whitby, and the Centre for Addiction and Mental Health in Toronto) have a combined annual budget of about 400 million dollars, with
approximately half assigned for schizophrenia. Across Canada, such budgets would need major increases. Considering that Ontario, for example, receives about 1,100 million dollars each year for tobacco taxes, a cannabis tax might cover the increased needs of the psychiatric hospitals and the community housing.
While the majority of cannabis users would not develop schizophrenia, the wider use of cannabis would lead not only to more hospitalizations of the new cases of schizophrenia, but also to an increased confrontation of psychotically disturbed young men with police.
Although there are valid medical uses for cannabis in cases of resistant epilepsy, and various painful chronic illnesses, wider use of cannabis may also be associated with drowsy driving and car accidents.
Almost all aspects of cannabis use and the related laws are contentious. Whatever laws are adopted by government may have to be a compromise between medical need and a reduced burden to all citizens.
******************
The author discovered the human brain’s dopamine receptor for psychosis and all antipsychotic drugs. Philip.Seeman@utoronto.ca
Source: www.dontdecriminalise.org blog Oct. 17, 2013.
The article below was written in 2007 but has relevance to the issues in the USA now in 2013.
In Defense of the Drug War
Libertarians often attack the war on drugs as a waste of tax dollars and an infringement on personal liberties. That is misguided thinking that comes from trying to apply unworkable theoretical concepts in the real world.
For example, you often hear advocates of drug legalization say that we’re never going to win the war on drugs and that it would free up space in our prisons if we simply legalized drugs. While it’s true that we may not ever win the war against drugs — i.e. never entirely eradicate the use of illegal drugs — we’re not ever going to win the war against murder, robbery and rape either. But our moral code rejects each of them, so none — including drugs — can be legalized if we still adhere to that code.
If we legalized drugs, we’d be able to tax them and bring in more revenue for the state. But, how is that working out with alcohol and cigarettes? In 2004 and 2005, 39% of all traffic-related deaths was related to alcohol consumption and 36% of convicted offenders “had been drinking alcohol when they committed their conviction offense.” When it comes to cigarettes, adult smokers “die 14 years earlier than nonsmokers.” But, will we ever get rid of tobacco or alcohol? No, both products are too societally accepted for that and perhaps more importantly, the government makes enormous amounts of revenue from their sale. Do we really want to be sitting around 10 or 15 years from now saying, “Gee, we’d like to get rid of heroin, but how could we replace the revenue we make from taxing it at an exorbitant rate?”
Of course, the number of people using what are currently illegal drugs would skyrocket if they were legalized, so we’d see a new wave of drug-addled burglars if we “legalized it.” Now, maybe you think that’s not the case. Some people certainly argue that if illicit drugs were legalized, their usage would drop. However, the fact that drugs are illegal is certainly holding down their usage. Just look at what happened during prohibition. Per Ann Coulter in her book, “How to Talk to a Liberal (If You Must)“:
“Prohibition resulted in startling reductions in alcohol consumption (over 50 percent), cirrhosis of the liver (63 percent), admissions to mental health clinics for alcohol psychosis (60 percent), and arrests for drunk and disorderly conduct (50 percent).” — p.311
That’s what happened when alcohol was made illegal. However, on the other hand, if we make drugs legal, safer, easier to obtain, more societally accepted, and some people say even cheaper as well, there would almost have to be an enormous spike in usage.
Certainly that’s what happened in the Netherlands where “consumption of marijuana…nearly tripled from 15 to 44% among 18-20 year olds” after the drug was legalized.
But, some people may say, “so what if drug usage does explode? They’re not hurting anyone but themselves.” That might be true in a purely capitalistic society, but in the sort of welfare state that we have in this country, the rest of us would end up paying a significant share of the bills of people who don’t hold jobs or end up strung out in the
hospital without jobs — and that’s even if you forget about the thugs who’d end up robbing our houses to get things to pawn to buy more drugs. Even setting that aside, we make laws that prevent people from harming themselves all the time in our society. In many states there are helmet laws, laws that require us to wear seatbelts, laws against prostitution, and it’s even illegal to commit suicide. So banning harmful drugs is just par for the course.
And make no mistake about it, drugs do wreck a lot of lives. Of course, drugs aren’t the only things that wreck lives and not every person who does drugs ends up as a crackhead burglar or a dirty bum living in an alley. Heck, Barack Obama, a man some people would like to see as our next President has used cocaine — and doesn’t it seem like every few weeks we read about another celebrity who comes out of rehab and goes on to have a successful career?
Sure, that’s true. But, every person who plays Russian Roulette doesn’t end up with a bullet in his head either. Look at the flip side of the equation. How many homeless people are drug addicts? How many women have had crack babies? How many people are in jail today because they got high and committed a crime? How many lives have been wrecked in some form or fashion by drug use? There’s probably not a person reading this column who doesn’t know someone who has faced terrible consequences in his life because of drug use.
That’s why once, way back when William Bennett was the drug czar, he responded like so to a caller on the Larry King show who told him that he should “behead the damn drug dealers.”
“I mean what the caller suggests is morally plausible,” he said. “Legally, it’s difficult. But somebody selling drugs to a kid? Morally, I don’t have any problem with that at all.”
Bennett was right then, he’s right now, and my guess is that most parents, upon finding out that someone was peddling drugs to their kid, would agree with him. Since that’s the case, do we really want the federal government to take over the role of a pusher and get our kids hooked on drugs to make a profit? No, we don’t
Source: www.eaglepub.com Human Events 25.1.07
Legalising heroin would cost the NHS and damage the UK
The siren call for drug legalisation sounds again. This time it issues from Mike Barton, the Chief Constable of Durham. The NHS should be used to supply addicts, Class A drugs should be legalised and drugs “prohibition” must be ended, he advises. It is a solution loved by top police officers and is no doubt borne out of a sense of frustration at the apparent intractability of drug-infected gangland crime.
It seems so seductively simple. Except it is not. Mr Barton is at the coalface of a drugs policy regime that is paying a high price for its liberality. It is a confusing place to be: officers are expected to give clean needles to the addicts they should be arresting. Prohibitive it is not. The UK citizen is more likely to be convicted for defaulting on his TV licence than for possessing and using illegal drugs.
Muddled thinking follows muddled practice. Much as the Chief Constable would like it otherwise, an addict is no more likely to be transformed by being sent to the doctor for his daily fix than than a legal market would put his supplier out of business.
The system Mr Barton suggests is already in place. The NHS spends £1 billion a year supplying the Class A synthetic opiate methadone to 150,000 addicts. Replacing methadone with heroin would put it up by several more billion. Mr Barton might stomach this cost, but I doubt a British public waiting for hip, heart and cancer operations would.
Improved health and reduced crime outcomes are overestimated. The “safe” (heroin is anything but safe) injecting sites integral to this policy — at least one for every market town and city centre — would not even sanitise the problem, let alone solve it. That is the experience of countries that have tried it.
Vancouver’s InSite programme is far from living up to its promises to reduce the spread of HIV, get clients into treatment and off drugs, or cut deaths from overdosing. It’s a policing problem in itself. Here in this country addicts on expensive NHS-funded opiate-prescribing trials were given daily injections and intensive nurse supervision, but still stayed street-drug dependent and continued to commit crime. That is the nature of addiction: addicts always want more.
The legal supply of heroin would no more undercut illicit demand than sate addicts’ desire. It would encourage drug tourism, black-market dealing (by adding to the supply) and the gangland crime that Mr Barton want to escape .
Supply without sanction feeds demand, which in turn feeds rates of use and, inevitably, harm.
Kathy Gyngell is a research fellow at the Centre for Policy Studies
Source: The Times 28th September 2013
Huffington Post – Colorado Fails to Regulate Marijuana – and Colorado Springs Decides Not to Take Their Chances With Legalization At All – Dr. Kevin A. Sabet
Though voters in Colorado and Washington officially legalized marijuana in November, most of us have known for a while that marijuana has enjoyed de facto legalization status in a few places for a long while now (you know who you are). One of those places is Colorado, where anyone with a little back pain and some cash can get a legal recommendation for pot shielding them from any legal sanction. But unlike in California, some Colorado officials have taken it upon themselves to try and regulate this trade, hoping for tax revenue and some control over the very strange and wild world of medical marijuana.
Their hopes have been dashed.
Two reports published within days of each other last week are enough to be a real buzz-kill for anyone high on legalizing marijuana in Colorado. Both reports, which closely examined the medical marijuana regulation business in Colorado, reveal that Colorado has failed their citizens by, well, not regulating marijuana at all. It serves as a troublesome warning for officials earnestly trying to implement a law filled with loopholes and special interest (read: marijuana industry) concessions.
And to add insult to injury, major cities like Colorado Springs – Colorado’s second largest city – have decided to ban recreational marijuana stores altogether (thanks to 5 city officials who resisted heavy lobbying by marijuana interest groups). And there’s good reason to think they just saved themselves from a big headache.
In the first of two major audits released last week, the Colorado State Auditor concluded the following about the Department of Public Health’s oversight:
* “Public Health does not sufficiently oversee physicians who make medical marijuana recommendations. We found evidence suggesting that some physicians may be making inappropriate recommendations.”
* 12 physicians made recommendations for 50% of the 108,000 patients; with one physician making a whopping 8,400 recommendations.
* “Some physicians have recommended what appear to be higher than-reasonable amounts of medical marijuana. In one case, a physician recommended 501 plants for a patient.” 501 plants is enough pot for an entire city, let alone one patient.
* “Public Health has not established a process for caregivers to indicate the significant responsibilities they are assuming for managing the well-being of their patients or for documenting exceptional circumstances that require a caregiver to take on more than five patients.”
* “It is not clear whether Public Health was adhering to the Colorado Constitution when it allowed staff of contract firms and other state agencies to access the confidential Registry. ”
* “Legal restrictions on Registry access create barriers for law enforcement agencies to effectively and efficiently enforce the State’s medical marijuana laws. ”
* “The Medical Marijuana Cash Fund has been out of compliance.”
The second audit reviewed the city of Denver’s medical marijuana licensing practices by the Department of Excise and Licenses. In many ways it was even more damming than the previous report, concluding that the city of Denver “does not have a basic control framework in place for effective governance of the… medical marijuana program.” The auditors wrote how the medical marijuana records are “incomplete, inaccurate, inaccessible,” and that many medical marijuana businesses are operating without valid licenses. Moreover, the Department does not even know how many medical marijuana businesses are operating in Denver. In addition, the audit reported that the Department’s personnel lacked formal policies and procedures to govern the licensure process. Finally, the auditors concluded that the medical marijuana licensure fee was established arbitrarily and the Department does not know the extent to which the marijuana license fees cover the costs of administering the program.
Taken together, these reports show that the state gets an F for “regulating” marijuana as medicine in Colorado. And it is not just the auditors who are worried. Treatment centers in Colorado are reporting more and more problems with marijuana, and emergency room admissions for the drug are skyrocketing among kids. The journal JAMA Pediatrics reported that unintentional marijuana poisonings among kids have risen significantly since marijuana as medicine has been available. Other peer-reviewed papers are finding that medical marijuana is easily diverted to youth. The Journal of the American Academy of Child and Adolescent Psychiatry in 2012 surveyed 164 Denver-area teens in treatment, and 121 of them — or nearly 74 percent — said they had used someone else’s medical marijuana. The average number of times they had done so? 50 times. Researchers also found that after adjusting for gender and race/ethnicity, teenage patients who used medical marijuana had more symptoms of marijuana dependence and conduct disorders than those who did not use medical marijuana.
Additionally, according to the Department of Health, only 3% of users in Colorado reported cancer, and less than 1% reported HIV/AIDS as their reason for marijuana. The vast majority (94%) reported “severe pain.” New York Mayor Michael Bloomberg best summed up marijuana as medicine when he said that it is “one of the greatest hoaxes of all time.”
Add this to other law enforcement reports showing that more than 70 instances of the diversion of medical marijuana to criminal drug operations, and the picture is not good.
And a new, nationally representative survey released on July 16 confirms that parents who support legalization of marijuana expect strict regulation of the substance’s availability. While 40 percent of adults say they are in favor of legalizing marijuana for recreational purposes, a majority of them oppose any form of legal marijuana for use among kids and teens. Almost everyone surveyed expects no advertising or commercialization of the drug in a legal environment. Legalization advocates in Colorado, who stand to make millions off of this new industry, insist on sweeping aside any concerns by saying “we’ll learn from the past and do it better.” But, given the vast influence of Big Marijuana involved in the current process to draft marijuana regulations — we shouldn’t count on it.
Source: Colorado Fails to Regulate Marijuana
By Anthony Evans,
To what end?
When it comes to radical shifts in public policy, this is the single most important question that must be asked, because actions don’t take place in a vacuum. Instead, they take place in a society that consists of all of us, from the very young to the very old. We’re all inextricably linked in a gigantic causal chain, and as Americans our fates are interconnected.
So when contemplating radical shifts to American drug laws – specifically, the legalization of marijuana: To what end?
The unfortunate truth of the human condition is that most of the time, we can’t foresee all the consequences of our actions. Not everything can be anticipated. This lack of foreseeability is why people, businesses and yes, even governments often make decisions that aren’t in their own best interest. Businesses fail, governments collapse and societies disintegrate because hindsight alone is 20-20.
Sometimes, it’s the unintended consequences that carry the most weight.
What we do know is large, far-reaching decisions have more unknown variables than smaller ones. Large decisions are the most unpredictable.
It doesn’t get much larger than radicalizing our drug laws.
To be fair, a number of Americans would personally benefit if marijuana was legalized. First and foremost for drug users, it would allow them to continue to enjoy drugs without the threat of arrest. Clearly, this is a key incentive; in countless interviews, the pro-legalization demonstrators have been very candid about being motivated by personal self-interest. Various economic benefits have also been touted by marijuana proponents, although it should be noted that the annual state and federal tax revenue for alcohol is $15.3 billion – yet alcohol costs $237.8 billion in health care, treatments, lost productivity and criminal justice.
But what are the other consequences?
Nicotine and Alcohol: The two most heavily abused recreational drugs in America are nicotine and alcohol – and what nicotine and alcohol have in common is that they’re both legal. That’s probably not coincidental: Shortly after Los Angeles legalized marijuana under the guise of “medical marijuana,” there were suddenly more licensed marijuana dispensaries in the city than Starbucks! The Obama Administration has stated: “It is therefore fair to suggest that decriminalizing or legalizing marijuana might not reduce the drug’s burden to our justice and public health system with respect to arrests, but might increase these costs by making the drug more readily available, leading to increase use, and ultimately to more arrests for violations of laws controlling its manufacture, sale and use.”
Genetically-Strengthened THC:We know that marijuana plants have been genetically engineered to produce higher levels of THC, the plant’s inebriating agent. By some estimates, today’s marijuana has between 600 percent and 1,300 percent higher levels of THC than plants from the mid-1970s. What this ultimately means is unclear, but it
does suggest that Baby Boomers who are basing the legalization argument on their past experiences might be underestimating today’s societal impact.
Violent Crimes and Hospital Visits: Roughly 500,000 people are arrested for violent crimes each year in America – and 98,000 people are arrested for marijuana-related crimes not including simple, nonviolent possession. Furthermore, a study of shock-trauma patients reported 15 percent of those injured while driving a car or a motorcycle had been smoking marijuana; another 17 percent tested positive for both THC and alcohol in their blood. And if this wasn’t enough, 450,000 annual visits to the hospital emergency room involve marijuana. If marijuana is legalized and its availability increases, it seems reasonable to assume that these numbers will rise. – as will the respective costs to society
There is an undeniable statistical link between marijuana usage and violent crimes, although we don’t fully understand the causal relationship. But it’s worth noting that there was more gun violence at Denver’s recent “4/20” pro-marijuana rally than at any Tea Party rally – ever. In fact, there’s actually been more gun violence at pro-marijuana rallies than at pro-Second Amendment rallies!
So again we ask: To what end?
Source: www. sun-sentinel.com/2013-07-16
New Zealand have passed new legislation which will make the production and selling of ‘legal highs’ and synthetic cannabis much more difficult since suppliers will have to prove the substances for sale are low risk. Offences will result in a large fine or even prison.
Mike Sabin, MP for Northland says he is hoping to see ‘backyard chemists’ who manufacture psychoactive substances, commonly sold as legal highs and synthetic cannabis, put out of business following the passing of the Psychoactive Substances Bill this afternoon.
“Over the last 20 years, countries all over the world have been dealing with an acceleration in the development of new forms of synthetic so-called ‘legal highs’ with the psychoactive compounds being ones that fall outside of drug classifications. This creates a cat and mouse effect for legislators and authorities trying to respond to the impacts of these drugs, says Mr Sabin.
“This Bill is unprecedented in that it responds directly to the exploitation of this anomaly, thus reversing the burden of proof to the manufacturers and suppliers of substances, meaning they will have to demonstrate that what they want to supply is low risk – or it won’t be able to make it to market.
“Scores of products with unknown effects and unknown risk profiles have made their way through this gap in the regulatory net and ended up on dairy counters alongside lollies,” says Mr Sabin.
“This new legislation is not in any way legitimising drug taking. It is specific to the particular nature of synthetically manufactured drugs, by beating the chemists at their own game through putting the onus on them; something I hope will drive them out of business and turn Kiwis off these products.
The new legislation includes provisions for:
· A regulatory authority within the Health Ministry to
o consider and approve or decline psychoactive substances
o issue a manufacturing code of practice
o issue importation, manufacturing and sale licences
o conduct post-marketing monitoring, audit and recall functions
* Establish an expert advisory committee to provide the authority with technical advice
* Set offences and penalties under the Bill, including up to two years’ imprisonment for some offences, and fines of up to $500,000
· Restrict sales of approved products to those over 18, remove sales from dairies and other non-specialty shops and restrict advertising to point of sale only.
· Prescribe retail restrictions (including advertising, labelling, and packaging restrictions), health warnings, signage, display, and other requirements.
“We should all remember that the only safe drug use is no drug use. Far from being an example as to how to deal with other drugs, as some opposition Parties are suggesting, this law change is simply the best way to stop chemists from altering the chemical compounds to beat the legislation, says Mr Sabin.
“These drug manufacturers have made a lot of money and caused a lot of misery in New Zealand. I hope the new law will put them out of business, because society doesn’t need what they have to offer.”
Source: Media Statement by Mike Sabin National MP for Northland NZ July 2013
This letter was recently sent to US Attorney General Holder. It contains a great deal of good information about why the so-called ‘medical marijuana scam has resulted in increased use, and increased problems in the USA.
To: Hon. Eric Holder, US Attorney General and Michele M. Leonhart, Administrator of the Drug Enforcement Administration
From: David G. Evans, Executive Director of the Drug Free Schools Coalition
Dear Mr. Holder and Ms. Leonhart:
Parents across America are waiting for you to enforce the federal Controlled Substances Act in the states of Colorado and Washington, which have legalized recreational marijuana, as well as in the 19 states where “medical” marijuana is legal. These laws were passed as the result of a well-funded lobbying campaign by the marijuana industry. The public has been misled by this campaign to see marijuana as harmless, natural, and medicinal, just as we were misled years ago by the tobacco industry, which claimed that tobacco was not addictive and that smoking had no ill effects.
Anyone who is in the business of cultivating, selling, or distributing marijuana, including “medical” marijuana, is in violation of the federal Controlled Substances Act, which preempts state law. You must enforce federal law and begin prosecutions to stop the proliferation of “medical” marijuana stores and widespread recreational use of marijuana. I also urge you and President Obama to use the “bully pulpit” to make parents aware of the dangers of these pro-marijuana laws to our kids.
The damage of marijuana – and these laws – is clear. Legalization of marijuana for “medical” use and recreational use in those states has resulted in more marijuana use, particularly among young people, which can permanently impair brain development. Teens who use marijuana are more likely to engage in delinquent and dangerous behavior and experience increased risk of schizophrenia and depression. Despite arguments by the drug culture to the contrary, multiple studies show that marijuana is addictive. Marijuana is the number one drug causing young people to enter treatment and there has been a substantial increase in the people in treatment for marijuana dependence.
Marijuana use also damages the American economy. Employees who test positive for marijuana had 55 percent more industrial accidents and 85 percent more injuries, and they had absenteeism rates 75 percent higher than those who tested negative.
Medical marijuana
Science and experience say that passing “medical” marijuana legislation is bad medicine and poor policy. A past evaluation by several federal Department of Health and Human Services agencies, including the Food and Drug Administration, Substance Abuse and Mental Health Services Administration, and the National Institute for Drug Abuse, concluded that “no sound scientific studies supported medical use of marijuana for treatment in the United States, and no animal or human data supported the safety or efficacy of marijuana for general medical use.”
A major study, “Early Findings in Controlled Studies of Herbal Cannabis: A Review,” concluded that despite the widespread public interest in the therapeutic potential of herbal cannabis, “the data alone fails to make the case that crude, smoked cannabis should be made available to patients.” Numerous other studies have replicated those findings.
If marijuana is going to be considered a medicine, it should be treated as such and be subject to the Food and Drug Administration approval process that includes clinical trials to determine its efficacy as a medication.
Who is really using “medical” marijuana?
“Medical” marijuana is generally a ruse for recreational use of marijuana. Let’s look at two states with medical marijuana dispensaries – Colorado and California. Who is really getting “medical” marijuana in Colorado? As of December 31, 2012, there were 108,526 people getting “medical” marijuana. Of those, 94 percent are treating “pain,” and 16 percent are treating “muscle spasms.” These are very subjective determinations. Very few are getting it for serious conditions such as cancer (3 percent), glaucoma (1 percent), and HIV/AIDS (1 percent). The average age of cardholders is 41, and 68 percent are male; 37 “patients” are under the age of 18.
The Rocky Mountain High Intensity Drug Trafficking Area, which coordinates federal and state drug enforcement efforts in Colorado and nearby states, conducted a study to determine if Colorado’s “medical” marijuana is being diverted for unintended purposes. The report cites more than 70 public record examples of diversion by patients, caregivers, and dispensaries within Colorado and 23 different states. The assessment is just a sampling of what is suspected of being diverted. The Colorado program is not effective in stopping diversion.
A recent study examining California’s average “medical” marijuana patients found that the average “patient” was a 32-year-old white male with a history of drug and alcohol abuse and no history of a life-threatening disease.
Our children are being hurt
Mr. Holder, last month, during your testimony before the House Appropriations Committee, you were asked what factors would be weighed by the Department of Justice in deciding how to respond to the legalization of marijuana in Colorado and Washington. You stated that: “When it comes to these marijuana initiatives, I think among the kinds of things we will have to consider is the impact on children.”
It is time for you to act. Our kids are being hurt. A recent Colorado study surveyed kids from adolescent drug treatment programs in the Denver area and found that 73.8 percent of them reported using medical marijuana that had been recommended for someone else and was diverted to the kids.
A recent article from the Journal of the American Medical Association (JAMA) Pediatrics edition found that there is “a new appearance of unintentional marijuana ingestions by young children after modification of drug enforcement laws for marijuana possession in Colorado.”
A major study recently published by researchers at Columbia University in New York found that “medical” marijuana states have significantly higher rates of marijuana use and of marijuana abuse and dependence than states without such laws. In California, drugged driving is more prevalent than drunk driving nowadays.
“Medical” marijuana negatively affects public health especially in regard to our youth. Since the message that “marijuana is medicine” has been popularized, perceived harm from smoking marijuana among kids has steadily decreased.
America is violating international law
In addition to the harm being visited upon our children by recreational and medical” marijuana, your failure to adequately enforce federal law is also in violation of international law – the United Nations Single Convention on Narcotic Drugs of 1961, to which the United States is party. America has been warned by the International Narcotics Control Board about this violation. The UN can place sanctions on the US for violating the treaty. How could you let that happen?
To date, your enforcement has been spotty and only in a few states. Most of the marijuana states have seen no enforcement or even threats of enforcement by your office.
Please take action in Colorado and Washington and all the “medical” marijuana states. In many of the “medical” marijuana states, a simple letter from you that you were going to enforce federal law would have stopped “medical” marijuana laws from being passed or implemented.
Put our kids first and enforce the law.
Sincerely yours,
David G. Evans
Executive Director of the Drug Free Schools Coalition, Special advisor to the Drug Free America Foundation
Russian President Vladimir Putin has signed a law introducing tests for students that will determine if they use drugs or psychotropic substances.
The federal law On Changes to Specific Legislative Acts of the Russian Federation on Issues Relating to the Prevention of Illegal (Non-Medical) Consumption of Drugs and Psychotropic Substances was passed by the State Duma on May 15 and approved by the Federation Council on May 29, the Kremlin reported on its website.
The document amends the legislation by introducing a system for early detection of the use by students of secondary and vocational schools of narcotic substances and psychotropic substances without a doctor’s prescription.
The law also outlines the powers of the federal and local authorities in the prevention of illegal drug consumption, including the powers to establish procedures and administer socio-psychological tests and preventive evaluations of students for early detection of drug abuse.
According to earlier reports, the law provides that teenagers younger than 15 will be tested with the consent of their parents and teenagers who are older than 15 can give their own consent to such tests.
The purpose of drug tests on students is to located risk groups and provide timely medical and psychological assistance.
Russian Deputy Education and Science Minister Alexander Klimov, who represented the bill at the State Duma meeting, said the socio-psychological evaluations will be conducted in the form of conversations and tests.
“Doctors will conduct these tests using modern technologies,” he said, pointing out that the results of the tests will be confidential by law. “It will be strictly controlled,” he said.
Source: www.rbth.ru 8th June 2013
California voters passed the country’s first medical-marijuana law in 1996, but many are having second thoughts. Last year, five California cities voted on initiatives to allow marijuana dispensaries, and all five voted no. Oregon also voted down dispensaries. These liberal West Coast states have seen medical marijuana up close, and learned it’s barely medical at all.
That shouldn’t surprise anyone. The idea that smoking pot is medicine didn’t come from doctors or groups representing the seriously ill. Neither the American Cancer Society nor the National Multiple Sclerosis Society supports it, and the American Medical Association and American Academy of Pediatrics strongly oppose it.
The idea to call marijuana medicine came from the National Organization for the Reform of Marijuana Laws and the Marijuana Policy Project. These two organizations are part of a national marijuana lobby that represents drug users, growers and sellers. They’re behind every medical-marijuana law in the country.
They advertise these laws with an impassioned plea to allow suffering, terminally ill people access to medicine. However, once these laws pass, most medical-marijuana patients claim pain, not serious illness. In Arizona, 90 percent get their marijuana for pain. In Colorado and Oregon, it’s 94 percent. Pain is every drug addict’s favorite complaint; it’s easy to fake and impossible to disprove.
Good doctors try to screen out drug abusers, but medical-marijuana laws are designed to circumvent good medical care. Most marijuana patients get their prescriptions from a few unethical doctors who see patients one time only and hand out marijuana recommendations to anyone.
Pot-smokers know who these doctors are, and they line their waiting rooms. Before Montana tightened its law, eight doctors wrote three-fourths of all the recommendations. In Arizona, 24 doctors did the same.
That’s why there’s a backlash. People feel hoodwinked. They voted for compassionate care, not drug abuse.
I’m a partisan Democrat who supports most liberal causes, but I’m also an addiction psychiatrist. I work with drug abusers. They’re amazing con artists who will say anything to get their drugs. And the marijuana lobby is no different.
For example, based on scant evidence, advocates claimed for years that marijuana could treat glaucoma. Today, ophthalmologists believe marijuana can damage the optic nerve and make glaucoma worse. The Glaucoma Foundation now warns patients not to use the drug, yet no marijuana advocate has ever apologized for handing out bad medical advice.
The pot lobby paints the Drug Enforcement Agency and the Food and Drug Administration as blue meanies, depriving people of needed medicine. But science consistently proves these agencies right. For every illness possibly helped by marijuana, there are safer and more effective medications already available. There aren’t thousands of people suffering because they can’t use pot; that’s a fiction the marijuana lobby invented.
In Arizona, they actually called their campaign “Stop Arresting Patients.” They wanted us to picture grannies in prison, doing their knitting surrounded by tattooed gang-bangers. But in a live debate, the Marijuana Policy Project lobbyist could not name even one genuine medical patient who’d been arrested solely for possession. That’s because there aren’t any. Medical-marijuana laws protect drug dealers and drug users, not the seriously ill.
Even worse, these laws hurt innocent people. An analysis of several studies, published in the British Medical Journal, found that drivers under the influence of marijuana had nearly twice as many serious and fatal car wrecks as nonusers. California, Colorado and Montana all documented increased traffic fatalities caused by drivers with marijuana components in their bloodstreams, coinciding with increased use of medical marijuana.
The biggest damage, however, is done to our kids. The National Survey of Drug Use and Health shows that teenage marijuana use is 30 percent higher in medical-marijuana states. Teens who smoke pot do worse in school, do worse in their adult careers and have twice the school drop-out rate of nonsmokers. No parent wants that.
Last, these laws cost states money. The marijuana lobby promises that taxes on pot will fill state coffers, but it’s just another deception. States with these laws pay out of their general funds to regulate marijuana, and for the increased health care, substance-abuse treatment and law enforcement needed any time an addictive drug becomes more available.
So don’t be taken in; medical marijuana is a ruse. It’s bad medicine that helps hardly anyone and has serious social and economic side effects for all.
Dr. Ed Gogek is an addiction psychiatrist in Prescott, Ariz., and board member of Keep AZ Drug Free, a group that opposes legalization and medical-marijuana laws.
By Peter Wehner,
Peter Wehner is a senior fellow at the Ethics and Public Policy Center. He was director of the White House Office of Strategic Initiatives in the George W. Bush administration and special assistant to the director of the Office of National Drug Control Policy during the George H.W. Bush administration.
Some say that the Republican Party needs to find new issues to champion if it hopes to become Americas majority party. There is something to this. But being a conservative party, the GOP should also look to the past, where wisdom often resides.
In that spirit, Republicans once again should take a strong stand against drug use and legalization. Virtually no lawmaker in either party is doing so.
For his part, President Obama has said more about the NCAA mens basketball bracket than he has about the dangers posed by illegal drugs. Gil Kerlikowske, the presidents drug czar, said last month that The administration has not done a particularly good job of, one, talking about marijuana as a public health issue, and number two, talking about what can be done and where we should be headed on our drug policy.
This is a startling admission, and there is a cost to abdication.
The drug-legalization movement is well-funded and making inroads. Voters in Washington state and Colorado passed ballot initiatives in November legalizing marijuana for recreational use. A bill to legalize marijuana was introduced in the Maryland House of Delegates last month. And Democrats in Congress have introduced legislation to end federal prohibitions on marijuana use.
This is the perfect time for Republicans to offer counterarguments grounded in medical science, common sense and human experience.
For example: One of the main deterrents to drug use is because it is illegal. If drugs become legal, their price will go down and use will go up. And marijuana is far more potent than in the past. Studies have shown that adolescents and young adults who are heavy users of marijuana suffer from disrupted brain development and cognitive processing problems.
Drug legalization will lead to more cases of addiction, which shatters lives. The vast majority of people who are addicted to harder drugs started by using marijuana. John P. Walters, the drug czar in the George W. Bush administration, noted last year, Legalization has been tried in various forms, and every nation that has tried it has reversed course sooner or later.
Strong, integrated anti-drug policies have had impressive success in the United States. Both marijuana and cocaine use are down significantly from their peak use in the 1970s and 80s.
So the policy arguments against drug legalization are all there; they simply need to be deployed.
But there is another, deeper set of arguments to be made.
In his dialogues, Plato taught that no man is a citizen alone. Individuals and families need support in society and the public arena. Today, many parents rightly believe the culture is against them. Government policies should stand with responsible parents and under no circumstances actively undermine them.
Drug legalization would do exactly that. It would send an unmistakable signal to everyone, including the young: Drug use is not a big deal. Were giving up. Have at it.
In taking a strong stand against drug use and legalization, Republicans would align themselves with parents, schools and communities in the great, urgent task of any civilization: protecting children and raising them to become responsible adults. But the argument against drug legalization can go even further. As the late social scientist James Q. Wilson noted, many people cite the costs of and socioeconomic factors behind drug use; rarely do people say that drug use is wrong because it is morally problematic, because of what it can do to mind and soul. Indeed, in some liberal and libertarian circles, the language of morality is ridiculed. It is considered unenlightened, benighted and simplistic. The role of the state is to maximize individual liberty and be indifferent to human character.
This is an impossible stance to sustain. The law is a moral teacher, for well or ill, and self-government depends on certain dispositions and civic habits. The shaping of human character is preeminently overwhelmingly the task of parents, schools, religious institutions and civic groups. But government can play a role. Republicans should prefer that it be a constructive one, which is why they should speak out forcefully and intelligently against drug legalization.
Source: The Washington Post Published: April 2nd 2013
Responding to Joe Klein on Drug Legalization
Earlier this week I wrote an op-ed in the Washington Post opposing drug legalization. In response, TIME magazine’s Joe Klein, who favors it, has written a dissent, critical but serious, which you can read here. Some responses to Klein follow:
1. “Most of [Wehner’s] arguments against dope come from a different era. He assumes a bright line between alcohol and ‘drugs.’ He assumes that marijuana is the entry drug on an inevitable path toward addiction. (He also seems to infer that marijuana is addictive.) Most of these arguments seem ridiculous to anyone who has inhaled.”
What I actually argue is a bit more nuanced and up-to-date than Klein’s characterization, and my claims happen to be true. Marijuana is much more potent than in the past. (In the 1970s, marijuana was at most 2-3 percent tetrahydrocanabinol, or THC. Recent Drug Enforcement Agency seizures were 7-10 percent. In Colorado and California, the marijuana dispensaries go as high as 15-20 percent or more.) Heavy use of marijuana does adversely affect brain development in the young. And the vast majority of people who are addicted to harder drugs start by using marijuana.
2. Does this mean that everyone who uses marijuana will become addicted to drugs like heroin and cocaine? Of course not. But it does mean that most of those who are addicted to cocaine and heroin started out by using marijuana. This hardly seems coincidental. Nor is there any credible evidence that I’m aware of that supports Klein’s sweeping claim that “Those who move on to harder drugs—and the infinitesimal minority who get hooked on harder drugs—would do so if marijuana were legal or not.”
Think about it like this: Some appreciable percentage of the population has a susceptibility to addiction (genetic factors account for between 40 and 60 percent of a person’s vulnerability to addiction). Under legalization, the pool of those exposed to marijuana will certainly increase by a significant factor; and the result will be that the number of those at considerable risk of moving to addiction on heroin or cocaine likewise grows.
Government surveys found that of those age 12 and above, 22.5 million were current illicit drug users (18.1 million of whom used marijuana) and 133.4 million were current users of alcohol. More than 20 million of these people suffered from dependence or abuse: 14.1 million for alcohol alone, 3.9 million for drugs alone, and 2.6 million for drugs and alcohol.
What can we reasonably expect the drug problem to look like if we increase the number of illicit drug users to, say, 50-60 million? You will get significantly more addiction–and significantly more shattered lives.
3. We know from Monitoring the Future studies, conducted by the University of Michigan since 1975, that the rate of marijuana use in youths is inversely related to “perceived risk” and “perceived social disapproval.” Legalization would lead to decreased perceived risk and decreased perceived social disapproval; the result would almost certainly be greater drug use. (See Figure 1 from this article by Drs. Herb Kleber and Robert DuPont.) On the flip side, treating drugs as unlawful acts as a deterrent, which is one reason we criminalize behavior in the first place.
4. Many legalizers assume that past efforts to reduce drug use have been failures. But the assumption is flawed. For example, William Bennett was President George H.W. Bush’s director of the Office of National Drug Control Policy. Under his strong leadership, we saw substantial decreases in overall drug use, adolescent drug use, occasional and frequent cocaine use, and drug-related medical emergencies. Student attitudes toward drug use hardened. In fact, the two-year goals that were laid out in Bennett’s first ONDCP strategy were exceeded in every category.
John Walters, who was President George W. Bush’s “drug czar,” also experienced impressive success during his tenure. Anti-drug policies have shown far more success than, to take just one example, gun control laws. (Two different studies–this one by the Centers for Disease Control, which reviewed 51 published studies about the effectiveness of eight types of gun-control laws, and this one by the American Journal of Preventive Medicine–found that the evidence is insufficient to determine whether firearms laws are effective.)
5. Several times Klein compares marijuana to alcohol, arguing that “it is simply illogical for alcohol to be legal and pot not.” The rejoinder is fairly obvious, and it goes like this: Alcohol has deep roots in America in ways that marijuana and other illegal drugs do not. I readily conceded that alcohol abuse is problematic and destroys many lives (estimates are that there are 80,000 alcohol-related deaths each year). The question is whether we want to compound this damage by increasing marijuana use as well. And to throw the argument back at Klein: Would he favor legalizing cocaine and heroin based on the argument that alcohol kills many more people than those two drugs do? Alcohol kills many more people than automatic weapons would if they were legalized. Does Klein therefore, in the name of an allegiance to logic, believe we should legalize ownership of M-16s? I rather doubt it.
Governing involves making prudential judgments that take into account complexities, nuances, and even inconsistencies in a polity’s views and attitudes. Human actions cannot be reduced to mathematical formulations. Edmund Burke’s discussion of “prejudice” in the context of his concerns with the French Enlightenment and its devotion to Reason are apposite here.
Where Klein and I do agree is that, in his words:
legalization of marijuana would compound the cascade of society toward unlimited individual rights—a trend that can be catastrophic if there isn’t a countervailing social emphasis on personal and civic responsibility. It might well accelerate the trend toward the couchification of American life; it certainly would not be a step toward the social rigor we’re going to need to compete in a global economy… if, in the mad dash toward pleasure and passivity, we lose track of our citizenship and the rigorous demands of a true working democracy, we may lose the social webbing that makes the pursuit of happiness possible.
Having found common ground with Joe Klein, New Democrat, I will happily pitch my tent there.
Peter Wehner is a senior fellow at the Ethics and Public Policy Center.
Source: http://www.commentarymagazine.com/2013/04/04/responding-to-joe-klein-on-drug-legalization/
DALGARNO INSTITUTE
The real subtext of the decriminalisation push
Shane Varcoe
5/22/2012
Author: Mr. S.W.Varcoe May 2012 www.dalgarnoinstitute.org.au
There is a maxim that remains constant in our consumerist culture and that is ‘availability, accessibility and of course the key component permissibility all increase consumption’.
I was speaking with a close friend who spent years in the horse racing industry and he told me the story about the advent of TAB betting outlets and the reason why such measures were introduced. One of the key motivators was the desire to diminish, if not eradicate the underground ‘S.P (Starting Price) bookies’ who would ‘assist’ punters who couldn’t get to the race track to make a wager on the ponies!
The strategy was to set up government controlled facilities that would enable people to gamble on the horse races in a more ‘scrutinized’ and accountable manner. Sounds fair? So to introduce state sponsored gambling they most certainly had to have ‘safe-guards’ in place; the following are just some of the caveats that must be adhered to in the setting up of government licensed TAB’s
a) Must not be within 200 metres of a hotel
b) Must not be within 200 metres of a church
c) Automatic Teller Machines or other money distribution mechanisms not permitted at race tracks.
Sounds wise, reasonable, especially to ensure some modicum of ‘harm minimisation’ was in place. For those at all familiar with this race betting industry, you will have no doubt raised your eyebrows to the clear fact that all of these ‘harm minimising’ measures have long since fallen by the wayside. Consumer demand insisted on it, didn’t it? The thin end of the wedge went deep and went fast!
Now we see….
a) Rows of ATM’s at racetracks
b) Gambling facilities and hotels merged into an indistinguishable melting pot of ‘alcohol enhanced’ entertainment
c) Churches… sorry what about them?
Now in this scenario, permission to gamble already existed, but it was access and availability that changed to increase its incidence.
What of other ‘permission’ increasing exercises? Let’s look at the legalisation of brothels in the State of Victoria; from 1984, when Victoria first legalised brothels, to 2004, the number of licensed ‘sexual services providers’ increased from 40 to 184 (Business Licensing Authority 2004a, p.1). Significantly, these figures do not include the growth in illegal prostitution, estimated to be four to five times the size of the regulated sector. The legalization of a once illegal industry has only seen an increase, not only in the spread of this ‘service’, but an exponential increase in those workers operating ‘outside the law’, to avoid regulatory processes and accountability. I’ll state it again… “Operating outside the law to avoid regulatory processes and accountability” Now, we have two tiers to contend with and still with no more, and one could argue, even less management of this dehumanising ‘industry’.
So, will this increase in both use and uptake happen with decriminalizing drugs? Of course not! Is the pro-drug lobby cry, but why would this arena be any different to the above mentioned?
The emergence of a new drug genre, ‘Novel Psychoactive Substances’ (NPS) gives us a clear indicator as to whether decriminalizing current illicit drugs will promote usage; the colloquial ‘tag’ given to these ever morphing chemical cocktails is the giveaway –‘Legal Highs’. The idea that one may be able to get a ‘buzz’ without breaking the law is a ‘permission slip’ for, if nothing else, a ‘guilt free’ try. Social prohibitions that are informed by not merely health and safety, but economic/productivity values do influence decision making. However, once these are viewed by the egocentric and ‘care-less’ social isolationist, as arbitrary, and personal ‘taste, mood and urge’ become the informing agents of policy, then removing illegality gives a further ‘push’ toward use.
If you think this is mere social theory, then think again. A very recent (and first of its kind for Australia) survey/study conducted by Dr Monica Barratt from National Drug Research Institute (Curtin University in Melbourne) reveals some, albeit unintentional, findings. The research, published in Australasian Professional Society on Alcohol and other Drugs, ‘Drug and Alcohol Review’ revealed not only the impact of Synthetic Cannabinoids, but the reasons for uptake. Not surprisingly the top reason for trying this substance was ‘Curiosity’ which 50% of those surveyed admitted as the motivation for engagement with the substance. However, it is reason two and three that reinforce what we here at The Dalgarno Institute have always known, and that is – ‘permissibility, accessibility and availability, all increase consumption.’
The research revealed that 39% of these first time users did so because of its perceived ‘legality’ and 23% took it up because it was ‘available’.1
Let’s turn this axiomatic formula to the legal drug of tobacco. Certainly more than permission for use of this substance has existed for over a century. More than permission was a sociable ‘insist-ability’ to partake – it was high fashion. At one point some medical doctors were prescribing cigarette smoking as a stress management tool, as mind-boggling as that is to contemplate in today’s social climate.
The growing and relentless assault against tobacco via the QUIT campaign in Australia is something only ‘mushrooms’ would know little of. This vital and effective demand-reduction and education ‘crusade’ that is raging against tobacco has been clear from its inception, and has continued to burgeon, evermore aggressively to the veritable ‘war’ we now see today.
The message is at the very least unambiguous, at times, bombastic! There is no guessing what the outcome of this assault on this ‘legal’ drug is to be. The message and mandate, at least in Australia, is not ‘slow down’, it is not ‘moderate’ it is QUIT. The end game is the only game. Sure, there are no illusions about the time it may take for many to reach that goal, but that goal is the only target to aim at and as a consequence measures and outcomes are effective – more and more Australians are quitting!
In 1945 approximately 72% of Australian men smoked. The rate has been dropping ever since then. In 2007 only 18% of Australian males were daily smokers. In 1945 26% of Australian women smoked…In 2007 women were smoking at a lower rate than men with 15.2% still smoking daily. 2
• increases in getting help to quit smoking, especially use of the Quitline (2% to 4%) and nicotine replacement therapy (7% to 10%);
• increase in one year quit rate from 8% to 11% among smokers and recent quitters;
• a statistically significant reduction of about 1.5% in the estimated adult prevalence of smoking. 3
However, as successful as this message has been, the fight is not over yet, as the following excerpt so irrefutably affirms…
“ANTI-SMOKING campaigners have far from finished their battle with the tobacco industry, with some pushing for a ”license to smoke” and many predicting that cigarettes could be outlawed within a decade.” 4(emphasis added)
Well, so was the bold opening statement in recent article ‘Now butt out: new push seeks to outlaw cigarettes’ in The Age Newspaper.
Fascinating! Outlawing cigarettes, even though around 17% of Australians are still smoking – outrageous! The article went on to note that if such a ban were to take place the government would stand to lose around $6 billion dollars in tax revenue, but save an estimated $31 billion dollars currently spent per annum on smoking related health problems.
No doubt to everyone who is not a smoker this makes good health and fiscal sense – maybe even to some smokers too?
So how is that we have managed to convince a society that a ban could actually be possible on a legal drug – tobacco, that in its boom era (during the 40’s, 50’s and 60’s) was a key social accessory? A quick inventory of the processes engaged may give us some insight:
? A clear and uncompromising acknowledgement from health, government and fiscal sectors that cigarette smoking was damaging our community.
? The ensuing resolve that this must change for both fiscal, but more importantly, health reasons.
? The continuing single voice of disapproval of cigarettes from academics, politicians and health professionals. (Stopped the propaganda of the pro-smoking academics/doctors and started the recognition of the undeniable facts that ‘every cigarette is doing you damage’.)
? The sustained political will to create and implement policies to bring about change, including increased taxation, total advertising ‘blackouts’ and bans – that’s right, ‘prohibition’ on smoking in defined places.
? These have been followed by the creation and implementation of Demand Reduction strategies that only grow in number and intensity; including health warnings and plain packaging on cigarette packets; and the relentless public education campaign on the dangers of smoking.
Author: Mr. S.W.Varcoe May 2012 www.dalgarnoinstitute.org.au
It would appear from both anecdotal and empirical data that such resolute policies work, even with a once widely accepted and socially palatable ‘legal drug’ like tobacco.
But I’m confused! How can such a relentlessness, ‘war’ on this ‘legal’ drug – tobacco, of which some 17% of Australians still use, be not only waged, but affirmed; while at the same time an apparent ‘war’ on illicit drugs be waged, declared ‘lost’ by noisy protagonists and discounted as no longer a worthy strategy? Especially when statistically less than 6% of the world’s 16-65 y.o. olds have tried or may be using some illicit drug intermittently, why would one give up on changing that statistic?
Why is a ‘war’ being fought so assiduously against tobacco and given up on against illicit drugs and the human cost they incur? Wouldn’t a war to reduce the now less 6% statistic be worth fighting to do all it can to prevent it increasing? Yet instead we hear, from a very small, but noisy minority, a call to not only stop the all but non-existent war on drugs and instead let them off the leash through decriminalisation or legalisation.
You, the reader, must understand something here and make no mistake; this call is a key component to the greatest drug pushing measure to ever be foisted on a culture – the push of permission! And timing for such a push is everything.
If you are an architect of such a blatant drug ‘push’ exercise, you must…
a) Cultivate the message that drug use is ‘normal’, everybody is trying it!
b) Cultivate a notion that some drugs are harmless and drug use is manageable, no different to alcohol or cigarettes.
c) Set up the ‘couch of credibility’ for some drugs by declaring them ‘medicine’. For example push the following specious logic; Cannabis can be used for some medical purposes, therefore marijuana is medicine, therefore marijuana is healthy, therefore marijuana is ok to use!
d) Have ‘celebrities’ and ‘doctors’ come out with claims of functional drug use giving credibility to the ‘product’.
e) However, the real key, if these elements are going to get real traction, is you must have an easily to manipulate demographic. To do that you have to ‘set people up’, particularly the young who have never really been taught how to think in any anthropological context of sustainable ‘why’ on life, rather only being told that what they think they want to right and good or bad, right or wrong, no longer come into it.
In our current confused culture, the plumbline for right and wrong has been ostensibly removed. There is no one unified ‘moral code’ to keep other than ‘one’s own’. It is Generation Y and the emerging generation who are best set up for this manipulation. Add to that the attentive issues of a ‘fun focused’ pop-culture, ruled by and ever distracting technocracy and you have a demographic easy to ‘play’ in a well-pitched market scenario.
When ‘selfist’ relativism erodes all sense of the ‘common’ good and any version of collective morality banned. When anchorless, rudderless and directionless ‘ethics’ are wielded by the manipulative apologists of chaos, thinly cloaked in ‘progressive spin’, we are left with only one vehicle by which to somewhat order society and prevent descent into anarchy, that vehicle is the rule of law.
Author: Mr. S.W.Varcoe May 2012 www.dalgarnoinstitute.org.au
The prominent Statesman Edmund Burke made this clear…
“Human Beings are qualified for liberty in exact proportion to their disposition to put moral chains upon their own appetites… Society cannot exist, unless a controlling power upon will and appetite be placed somewhere; and the less of it there is within, the more there must be without. It is ordained in the eternal constitution of things, that men of intemperate minds cannot be free. Their passions forge their fetters.”
Of course then comes the next question; what law and who gets to make it? This now becomes the arena of debate.
I want to present a couple key scenarios in this brief treatise that leave us little ‘wiggle-room’ for the idea of abandoning criminal sanctions on drug use, let alone the unthinkable society wide and ultimate ‘drug pushing’ scenario of legalisation.
A basic principle of good democratic and functional communities is to do with foundational governance issues. When it comes to legislation, what principle/s should it be founded on, or at least informed by?
Gus Jaspert the Deputy Director of UK Home Office speaking at the 3rd World Forum Against Drugs, declared…
Governments should aim to…
a) Protect their citizens from harm.
b) Provide environments that enable its citizens to reach their full productive potential.
Any legislation must be filtered through these two foundational principles and the tough questions asked of any proposed introductions or amendments that may breach these principles.
So follow the questions…
a) Does illicit drug use cause harm to citizens?
b) Does illicit drug use impede/diminish the productive potential of a nation’s citizens?
Subsequent to these basic questions one then must also ask…
? Will widening illicit drug accessibility, permissibility and availability, improve the safety, amenity and wellbeing of any or all of a nations’ citizens?
? Will widening illicit drug accessibility, permissibility and availability, improve familial and community functionality, harmony and cohesiveness?
? Will widening illicit drug use improve or put greater burden on the physical, emotional and mental health of our community?
? And last, but by no means least, will widening illicit drug accessibility, permissibility and availability improve or diminish the well-being and safety of our nation’s children?
These last two of these questions are most important to answer, not only on their own merit, but also within the context of other social justice and social responsibility charters, being a) Good professional health care/management and b) nothing less than the United Nation’s Convention of the Rights of the Child.
A précised, but lucid look at professional health management strategies of functional societies reveals that all measures and means be taken to maximise community health for one primary reason (other than well-being of its citizens) and that is good fiscal policy. Healthy people not only save any society immense amounts of money, but contribute more productively to its growth and improvement.
In answering above questions a) and b) just the following pieces of data is evidence enough for governments to move against illicit drugs to protect its citizens against such harms:
‘‘Illicit drug use shaves approximately 13 million years off the world’s collective drug users lives.” 5
“Americans spend approximately $65 billion per year on illicit drugs,6 but the costs to society from drug consumption far exceed this amount. Illegal drugs cost the U.S. economy $98.5 billion in lost earnings, $12.9 billion in health care costs, and $32.1 billion in other costs, including social welfare costs and the cost of goods and services lost to crime.”7
“Principle 16 – Research-based prevention programs can be cost-effective. Similar to earlier research, recent research shows that for each dollar invested in prevention, a savings of up to $10 in treatment for alcohol or other substance abuse can be seen (Aos et al. 2001; Hawkins et al. 1999; Pentz 1998; Spoth et al. 2002a; Jones et al. 2008; Foster et al. 2007; Miller and Hendrie 2009).”8
“The success of demand reduction in the US is reflected in long-term decreases in rates of illegal drug use. The percentage of persons aged 12 and older in the US who used an illegal drug in the past 30 days has decreased 38% from its peak in 1979 (14.1%) to 2009 (8.7%). Equally impressive are statistics from the United Nations Office on Drugs and Crime (UNODC), which has documented a greater than 80% reduction in annual opioid use over the past century!”9,10,11
Yet, there is more to professional health management strategies than economic rationalism. Disease control is a primary goal of good health management policy/strategies. Eradication of any disease is the ultimate goal, but in the interim, management practices can be used with an attempt to alleviate symptoms and to improve health status, enabling best opportunities to work toward recovery and wellness. When there is any option for recovery/wholeness then that becomes the goal.
No good health professional will refuse or omit such options when they are available.
For instance, when it comes to the epidemiology of a disease, treating physicians look to a number of factors, including the agent of contagion. They look to manage, negate and prevent these agents from spreading.
Illicit drug use dependency has now been widely touted as a ‘disease’ and as such the term ‘disease’ has an ever morphing definition in various diagnostic manuals. Regardless of the definition, treatment principles still remain the same – the containment, cessation and future prevention of this disease. Two key factors must be addressed if any sort of positive health outcome is going to be achieved…
a) Susceptibility factors of the patient
b) Exposure factors to the patient
So in treating the disease of drug dependency/addiction one must address both of these factors to have best hope of the drug user becoming healthy again – The health that a) saves money b) keeps you from harm c) enables your full productive potential d) adds to your and the communities general well-being.
The question we now have to ask of any measure that will increase accessibility, permissibility and availability of illicit drugs is, will it exacerbate or alleviate a) susceptibility factors and b) exposure factors? If it does the former, then we have breached good, professional and fiscally responsible health care practice. Any action/method/process that enables the increase or worsening of these two factors is at best reprehensible and at worse culpable and worthy of malpractice suites and license revocation.
When it comes to the mental, physical and emotional health of society’s citizens and particularly its children, any measure that increases the exposure or susceptibility to a disease must be, if not eradicated, utterly contained. To do less is to collapse the very core of what good governance and good health care strategy is for a nation.
When the already available, well managed and effectively deployed ‘exposure’ preventing tool of criminality is employed, we are half way to achieving best potential for full recovery. Removing this proactively used mechanism will only see the opposite be true in a community.
In summary, when it comes to the notion of drug decriminalisation or legislation and the key issues that we have looked briefly at here, we need to ask….
a) Will decriminalisation/legalisation of currently illicit drugs increase the harms to citizens, the children and their productivity/potential?
b) Will decriminalisation/legalisation of currently illicit drugs make for better health care policy/practice and outcomes?
c) Can criminal sanctions be used effectively, not as a punitive sanction, but as a collaborative vehicle to enable both unwitting causalities or even recalcitrant purveyors of drug disease to not only diminish harms to the wider society and themselves, but more importantly to discover the potential and productivity that both functional society and good government endeavour to promote?
It is clear that when societal expectations and conventions of protection, safety, productivity, health and wellbeing are breached by its citizens, then sanctions are not only expected, but demanded. However, the caring use of these sanctions and prohibitions is not about what is ‘put down’, but much more about what can be ‘taken up’. Why remove a mechanism (criminality) that has the proven potential (when used proactively for care i.e. diversion/rehabilitation) to provide safety, promote recovery and more importantly promote wholeness?
I think it is time we stopped the ‘war’ on good drug policy and start to take up the fight for a better society for all our citizens and not just the one dimensional demands of disease promulgating and society damaging minority; the careless minority who seek to avoid, not only the consequences of their bad choices, but more callously, demand the rest of the community to pay for their ongoing bad choices.
I will conclude with a quote from one of the ‘fathers’ of modern libertine ideology, John Stuart Mills; A caveat even the most self-absorbed, ‘rights’ demanding drug user cannot easily dismiss…
No person is an entirely isolated being; it is impossible for a person to do anything seriously or permanently hurtful to himself without mischief reaching at least to his near connections, and often far beyond them…If he deteriorates his bodily or mental faculties, he not only brings evil upon all who depended upon him for any portion of their happiness, but disqualifies himself for rendering the services which he owes to his fellow creatures generally, perhaps becomes a burden on their affection or benevolence; and if such conduct were very frequent hardly any offense that is committed would detract more from the general sum of good.
Endnotes
1. Barratt,1 Monica J* Patterns of synthetic cannabinoid use in Australia, Drug and Alcohol Review: Volume 32, Issue 2, pages 141–146, March 2013
2 http://www.cancercouncil.com.au/editorial.asp?pageid=371
3 CHANGES ASSOCIATED WITH THE NATIONAL TOBACCO CAMPAIGN PRE AND POST CAMPAIGN SURVEYS COMPARED by Melanie Wakefield http://www.health.gov.au/internet/main/publishing.nsf/Content/health-pubhlth-publicat-document-metadata-tobccamp.htm/$FILE/tobccamp_c.pdf
4 Stark , Jill The Age, 22.5. 2011 http://www.theage.com.au/victoria/now-butt-out-new-push-seeks-to-outlaw-cigarettes-20110521-1ey2s.html#ixzz1OBTg5SRQ
5 http://gma.yahoo.com/blogs/abc-blogs/200-million-people-illicit-drugs-study-finds-120123343–abc-news.html
6Executive Office of the President, Office of National Drug Control Policy. What America’s Users Spend on Illegal Drugs. December 2001.
7 Executive Office of the President, Office of National Drug Control Policy. The Economic Costs of Drug Abuse in the United States, 1992-1998. September 2001.
8 NIDA: Lessons from Prevention Research, August 2011 http://www.drugabuse.gov/publications/drugfacts/lessons-prevention-research
9Substance Abuse and Mental Health Services Administration. (1999). National household Survey on Drug Abuse: Main Findings, 1997 (Office of Applied Sciences). Rockville, MD.
10 Substance Abuse and Mental Health Services Administration. (2010). Results from the 2009 National Survey on Drug Use and Health: Volume I. Summary of National Findings (Office of Applied Studies, NSDUH Series H-38A,HHS Publication No. SMA 10-4856Findings). Rockville, MD.
11United Nations Office on Drugs and Crime. (2007). World Drug Report 2008. Vienna: United Nations Office on Drugs and Crime. Retrieved June 23, 2011 from http://www.unodc.org/documents/wdr/WDR_2008/WDR_2008_eng_web.pdf
Mr. Shane W. Varcoe – Executive Director, Dalgarno Institute May 2012
Source: Shane W. Varcoe www.dalgaroinstitute.org.au May 2012
Peter Bensinger is former administrator, of the U.S. Drug Enforcement Administration and former director of the Illinois Department of Corrections. Andrea Barthwell is former deputy director of the Office of National Drug Control Policy.
The marijuana bill the Illinois legislature is considering does away with the Food and Drug Administration process, and the legislature assumes the role of the FDA.
The FDA has concluded that marijuana has a high potential for abuse, has no accepted medical use and lacks an acceptable level of safety even under medical supervision. The FDA has approved Marinol, which is not smoked, but is marijuana in pill form.
Over a century ago, people bought all sorts of stuff from salesmen selling heroin, cocaine, marijuana — out of the back of a wagon. Often called Snake Oil Salesmen, they sold products touted as painkillers.
We had almost 3 million heroin addicts in the early 1900s. The Harrison Narcotics Act passed in 1914, then the Food, Drug and Cosmetic Act, the FDA was established and Charles Walgreen opened a drugstore.
Today people know where they can get medicine approved by the FDA as safe and effective — at drugstores — and manufacturers list the ingredients, directions, side effects and warnings. This bill would make medical marijuana available to 18 year olds, but it won’t be with a prescription or at a drugstore.
Marijuana as medicine means more use and more abuse. Each cardholder can get 2.5 ounces of marijuana every 14 days (2.5 ounces makes 183 joints). Medical marijuana cardholders will either sell their marijuana or give it to others. This is not debatable; this will happen. Based upon Michigan’s experience, Illinois could expect more than 270,000 medical marijuana cardholders.
Research documents that regular users of marijuana have twice the motor vehicle crashes as non-users. In Colorado, since medical marijuana was introduced, the number of drivers causing fatal motor vehicle crashes testing positive for marijuana has more than tripled.
Substance Abuse Treatment centers for children report marijuana as the leading cause for admission. Marijuana is second only to alcohol at adult substance abuse treatment centers.
Illinois employers responsible for a safe work environment prohibit employees from coming to work under the influence of alcohol or illegal drugs. Employers would now have new problems dealing with employees and applicants using marijuana. Can employers maintain a safe work environment when people with marijuana in their system come to work under the influence or stoned, threatening the safety of the workplace and co-workers?
Since when is smoking good for your health? Marijuana is fat soluble and stays in the fatty tissues and the brain 75 times longer than a drink of alcohol.
If smoked marijuana is good for cancer, glaucoma and multiple sclerosis patients, why do national associations representing these patients oppose marijuana as medicine? The legislation sponsors argue that marijuana can provide relief from those suffering untreatable pain, but as the U.S. Court of Appeals ruled on January 22 “no adequate and well controlled studies exist on marijuana’s medical efficacy.”
This is about whether Illinois citizens want the legislature to decide on how to approve and dispense medicine instead of the FDA. The medical marijuana lobby has put together myths and money that will not make for a safe or healthier Illinois. The proposal endangers our youth, our highways and our workplaces and increases costs for employers and taxpayers. It is bad medicine.
Source: Springfield, Illinois, State Journal-Register April 12, 2013
Legal marijuana may not bring in enough money to cover the societal costs of legalization, a new study from a Colorado State University think tank concludes.
The analysis was conducted by the university’s Colorado Futures Center in response to Colorado passing an amendment back in November . The study argues that revenue from marijuana taxes won’t do much to help Colorado’s budget and that money generated for new school construction won’t reach the $40 million annual target that supporters of marijuana legalization set when campaigning for legalization.
“These questions are of even more concern in light of our expectation that the most productive marijuana tax years will be the years just after legalization,” the center wrote in its report.
The study is one of several seeking to predict the unpredictable: What will the state look like with legal marijuana.
“[T]he future holds more unknowns than knowns,” four national marijuana-policy experts wrote in a recent editorial examining the implications of legalization votes in Colorado and Washington.
The predictions largely hinge on how much legal marijuana people will buy and smoke in Colorado. The Colorado Futures Center, citing federal studies on drug use and other references, estimates that demand for pot in Colorado will hit 2,268,985 ounces a year — more than 70 tons.
Using a retail price of $157 per ounce before taxes — and assuming that proposals for a 15 percent excise tax and a 15 percent special marijuana sales tax pass with both lawmakers and voters — the center estimates annual tax revenues starting in 2014 at about $130 million.
That is well above what the state’s nonpartisan Legislative Council found in its voter-guide analysis of Amendment 64, although its $5 million to $22 million annual estimate didn’t include an excise or a special sales tax. The center’s estimate also is above the $60 million annually in savings and extra revenue that the Colorado Center on Law and Policy predicted initially for Amendment 64 — although it, too, didn’t consider revenue from a special sales tax.
The Colorado Futures Center concludes in its report that the costs of regulating recreational marijuana — plus possible extra costs for law enforcement, public health and human services — may exceed the tax revenue from the recreational marijuana industry. The center also estimates that tax revenue from the industry will level off or fall, “as the ‘wow’ factor erodes over time and any marijuana tourism begins to decline, particularly if other states follow Colorado and Washington and legalize marijuana.”
Smart Colorado, a group opposed to all but the most limited implementation of legal marijuana, jumped on the analysis as proof that Amendment 64 was a bad deal.
“The latest research just confirms that marijuana proponents’ promises to Colorado voters that Amendment 64 would be a financial gain to the state were empty,” Diane Carlson, one of the group’s leaders, said in a statement. “Even if voters approve the recreational-marijuana tax, the new pot market could be a net drain on the state’s budget, the study indicates. That means funds for education, roads and other top priorities could be diverted to marijuana regulation.”
Department of Revenue officials, who would regulate recreational marijuana businesses under a proposal before the legislature, have pushed for the special sales and excise taxes — arguing the regulations must be funded if they are to be effective. Still, they told lawmakers Wednesday during a hearing for a bill on proposed regulations that they still don’t have a handle on how much money they will need.
“The challenge that we have,” said Ron Kammerzell, the Revenue Department’s enforcement director, “is that it is very difficult to predict demand.”
jingold@denverpost.com 23.04.13
WHITE MOUNTAINS – Experts in Colorado are starting to study the impact medical marijuana has had on teen drug use in their state. Medical marijuana sales are scheduled to begin in April in Arizona. Fifteen states and the District of Columbia now have medical-marijuana programs.
Two recently released national surveys, the National Survey on Drug Use and Health conducted by the Substance Abuse and Mental Health Services Administration and the University of Michigan’s Monitoring the Future data have shown increases in teen marijuana use, marked by a decreased perception of harm in the drug.
“The basic rule with any drug is if the drug becomes more available in the society, there will be more use of the drug,” said Thomas Crowley, a University of Colorado psychiatry professor and director of the university’s Division of Substance Dependence. “And as use expands, there will be more people who have problems with the drug.”
In Colorado treatment centers, clinicians are treating more and more teens for marijuana
addiction since the state legalized marijuana for medicinal use. At the Denver Health Medical
Center, treatment referrals have tripled with 83 percent of the teens that smoke pot daily saying they obtained it from a medical marijuana patient. Navajo County Drug Project (NCDP) tracks youth drug use through the biannual Arizona Youth Survey, conducted by the Arizona Criminal Justice Commission. In the 210 survey, 29.2 percent of participating Navajo County youth, in eighth to 12th grade reported having used marijuana in their lifetime. This was down from 42.1 percent in 2008 and 29.3 percent in 2006. “These statistics show a steady decline of marijuana use among Navajo County youth,” said NCDP Director Debe Campbell. “We won’t have parallel data until 2012, when we expect to see escalation of use,” she added.
The National Institute on Drug Abuse (NIDA) allocated money for health advocates to study the effects of medical-marijuana policies on broader drug use and public health. NIDA officials decided to offer the funding after seeing a rapid change in marijuana policies across the country.
Source: http://www.wmicentral.com/news/latest_news/medical-potlaws Jan. 17. 2011
Substance-abuse experts, alarmed by the rapid growth of Colorado’s medical-marijuana industry, are intensifying their efforts to study the industry’s impact on drug use. The experts say they especially worry that increasingly permissive attitudes surrounding marijuana use might be leading to higher teenage drug use and addiction rates.
That has been an often-voiced concern during debates over medical marijuana in Colorado. But substance-abuse-prevention workers say evidence from their clinics seems to bear it out. And they point to a recent study showing an increase in teenage marijuana use nationwide and a decrease in perceptions of its risk as further evidence of a need to examine the issue.
“The basic rule with any drug is if the drug becomes more available in the society, there will be more use of the drug,” said Thomas Crowley, a University of Colorado psychiatry professor and director of the university’s Division of Substance Dependence. “And as use expands, there will be more people who have problems with the drug.”
At his substance-abuse-treatment clinic for adolescents at Denver Health Medical Center, Christian Thurstone said he has seen hard evidence of the trend. Since the summer of 2009, roughly when Colorado’s medical-marijuana boom began, Thurstone said he has seen treatment referrals triple, from five to 15 per month. The large majority of those teens are referred — either by the criminal justice system, social services or other means – because of marijuana, he said.
Worried by the increase, Thurstone conducted a survey of 76 kids in his program. Of those, 60 said they knew someone with a medical-marijuana card, and 37 said they have obtained pot from a medical-marijuana patient, though none were patients themselves.
What’s more, Thurstone said teens who got marijuana from a patient were more likely to report smoking pot daily than those who didn’t. About 83 percent of the teens who scored pot from a patient reported daily use, compared with about 56 percent of those who didn’t get marijuana from a patient.
“It looks like it’s increasing access,” Thurstone said of the state’s medical-marijuana program.
“It looks like it’s making social norms more positive for marijuana. And it looks like it’s increasing frequency of use.” Thurstone said he intends to apply for federal grant funding to more fully examine the subject.
Source: The Denver Post www.denverpost.com 01/01/2011
Canada’s ban on marijuana was effectively upheld Friday when Ontario’s top court struck down the country’s laws related to medicinal pot much to the chagrin of activist groups.
In overturning a lower court ruling, the Court of Appeal ruled the trial judge had made numerous errors in striking down the country’s medical pot laws.
Among other things, the Appeal Court found the judge was wrong to interpret an earlier ruling as creating a constitutional right to use medical marijuana.
“Given that marijuana can medically benefit some individuals, a blanket criminal prohibition on its use is unconstitutional,” the Appeal Court said.
“(However), this court did not hold that serious illness gives rise to an automatic right to use marijuana.”
Currently, doctors are allowed to exempt patients from the ban on marijuana, but many physicians have refused to prescribe the drug on the grounds its benefits are not scientifically proven.
The Canadian HIV/AIDS Legal Network called the decision a disappointing missed opportunity.
Source: The Canadian Press – Friday, February 1 2013
In the light of the recent attempt to legalise drug laws in the UK (via the HASC report) we must continue to be vigilant and inform the public and our politicians of the harms – not just to individual users but to society as a whole – deriving from the use of illegal drugs and the irresponsible use of alcohol.
The following perceptive article was received from a colleague in the United States.
Please note that the people of Colorado have just put the right to use marijuana into their state constitution, on the same level as the right to assemble, freedom of speech, and freedom of religion. What a great day for the children of Colorado, and all of us.
Someday, in the not-too-distant future, we will look back at this moment like we looked back at the 60s and early 70s at one point in our history, and we will view this day as evidence of a massive and destructive social experiment that careened predictably out of control. But until then, we may have to endure the fact that many lives will be lost in the aftermath of a cultural tsunami, led by counter-culture anti-heroes who preach their religion of pot from the concert stage, movie set, political podium (and sometimes shamefully from a law enforcement website).
At one point in our history, we rejected the notion of a drug culture and made impressive strides in educating America. And like our success with tobacco education, these educational efforts led to fewer people using and abusing drugs – because EDUCATION WORKS. But now, with millions of dollars being used for the dumbing down of America in a haze of marijuana smoke, we may have to relearn the same lessons before we all wake up and fight back.
The saddest part of this is that our federal government has always had the ability to shut this down. As a federal drug prosecutor of almost 25 years, I know that we never had to endure a decade or more of so-called “medicinal” marijuana before the pretense was dropped and full legalization efforts began. For the price of a postage stamp and some paper, the federal government could send a notice of forfeiture to marijuana landlords. This would be most effective in states like Arizona and New Jersey where only one dispensary exists (at this point). Other enforcement action could be taken against the New Barons of Pot who were so interestingly portrayed in Newsweek not too long ago. And the barons would get the message that there is a new Sheriff in town and their looting of the candy store would have to stop. Surprisingly, these new pot entrepreneurs are willing to brag about their millions and even be the stars of TV shows. In the old days, we would have treated these episodes as “confessions” and would have used their own videotapes to convict them.
When the feds have taken decisive action, they have achieved wonderful results, which have been greatly appreciated by municipalities and counties going bankrupt trying to reign in the circus. But these efforts have been too few, too late, and almost nonexistent in some states.
Instead, with limited exceptions, the feds have chosen to “fiddle as Rome burns” while complicit state officials think of ways to launder drug proceeds disguised as tax revenue. In the meantime however, our children our being spoon fed a pop culture by pro-drug anti-heroes masquerading as enlightened people – because it is “cool” to be for pot.
As the marijuana industry has amassed millions, and purchased the souls of politicians and pundits who either ignorantly or purposely point to significant “tax revenues”, the end of drug cartels, and the emptying of prisons from all of those non-existent marijuana user prison inmates, our voting public has been duped into believing them. It isn’t hard to imagine how this happened when the Washington pro-marijuana campaign spent more than $6,000,000 to reach out to soccer moms. What political candidate could have successfully faced this foe with a measly $16,000 in their bank account?
So, on the day that Colorado joins Washington in the revelry, let me add my hope that the quickest solution manifests itself immediately – that the federal government simply enforces the law. This action by President Obama and DOJ would be a welcome relief to everyone who knows that sober children learn better, sober drivers drive better, and sober parents parent better. And it may give the drug prevention coalitions time to catch up.
For this to occur in time, some miracles will have to to happen. But during a season that is defined by miracles, perhaps this is our best hope for a drug free future.
Source: Monte Stiles Retired Federal Organised Crime/Drug Enforcement Task Force USA
About 100 members of the Somali community have demonstrated outside Downing Street to call on the government to ban a herbal high.
Khat, which is illegal in the US and many countries in Europe, has been chewed for centuries in east Africa and the Middle East. The campaigners said it caused medical problems and family breakdowns.
The Advisory Council for the Misuse of Drugs is currently reviewing the harms associated with khat.
Effects of chewing the leaves of the khat plant include euphoria and extreme talkativeness, but side effects can include dizziness, heart problems and anxiety.
Fears have been raised that the stimulant is contributing to mental health problems within the communities that use it. Richard Hamilton, Africa editor for the BBC World Service, attended the demonstration.He said research suggested that more than a third of the over 100,000 Somalis in the UK have admitted to consuming khat on a regular basis.
The demonstrators said that the drug caused mental illness, depression, cancer and death from liver failure. They added that the social impact of khat has kept men away from work and led to the disintegration of families and local communities. Abukar Awale, who organised the demonstration, is himself a former khat addict.
“The number of families who are breaking down due to khat is beyond your imagination,” he said. There is clear evidence of medical and social harm.
“I’d like to bring to your attention a report which came out in 2011, called ‘khat related deaths’ there are fourteen cases – all young men, all of them died of liver failure.
“They are not related. The one factor they all have in common is excessive khat use, which leads us to believe there is huge evidence of medical harm.”
A Home Office spokesman said: “The Advisory Council for the Misuse of Drugs (ACMD) is currently reviewing the harms associated with khat. The government is required to consult the ACMD and will not prejudge this advice. The home secretary will consider the advice fully when it has been received, which is likely to be later this year.”
Source: www.bbc.co.uk/news 1st Nov 2012
Thailand will employ a proactive strategy in tackling drugs, the secretary of the National Narcotic Prevention and Supression Commission, Pol General Pongsapat Pongcharoen, said.
The offensive will take place throughout the Kingdom, starting with 12 communities in Klong Toei slum, and will involve monitoring those who have been treated after they were found to have drug addiction, he said.
Pongsapat, who is also a deputy chief of the National Police, said in the weekly television programme “PM Yingluck meets the people” that over the past year many big-time drug dealers had been arrested. But he was still concerned about drug addiction and trafficking in communities in Bangkok and its surrounding provinces.
This, he said, had led to the designation of various communities in order to better tackle the problem and many youths have given tips to the authorities while some of those affected in communities were yet to receive proper care that should include post-addiction livelihood training.
Pongsapat cited Klong Toei slum as the most drug-prone, especially in areas called Lock 1-3 and Lock 4-5 over a 70-rai area and occupied by some 7,000 to 8,000 people.
Some 3,000 youths were thought to be at risk, said Pongsapat, and the authorities had surrounded the communities to “x-ray every inch over a 90-day period”, which began on October 1. That includes police patrols, installing CCTV cameras and officers at all the 18 entrance and exits. This, he said, had led to many arrests so far.
Another measure is to campaign in the community that those addicted are like sick people and since October 14, 106 people, including parents and youths, had voluntarily sought drug treatment. These people were being sent to various treatment centres and it would take from 45 to 120 days for the rehabilitation process to conclude.
The Education Ministry has also been asked to help look after children who have no access to education in the areas. Deputy Premier Chalerm Yoobamrung has been appointed as director of Palang Paendin (Power of the Land) Centre that seeks to win the “war on drugs”.
Throughout the country, 878 districts will deploy a strategy similar to what is being used in a Klong Toei slum, including crackdowns on drug transport and trafficking. Three areas in Bangkok will be particularly targeted along with nine provinces.
More than 400,000 people have been rehabilitated so far and the government is trying to introduce a one-stop service centre.
Meanwhile, Prime Minister Yingluck went to a Klong Toei slum yesterday to inaugurate the Baan Unjai Project (Reassuring Home Project), coinciding with the crackdown on drugs in the area.
Yesterday morning, two drug users were arrested in the area for possessing “ice”.
Dusit Poll, meanwhile, revealed that a majority of respondents supported Priephan Damapong as deputy premier to tackle the drugs issue.
Source: www.asiaone.com 21st Oct.2012
By Matthew Hill BBC health correspondent
Some analysts suggest that lessons can be learned from Portugal’s drug laws. So how are things done differently there?
As she waited calmly with fellow drug users queuing for their weekly treatment in Lisbon’s main detox centre, Anna was happy to talk about the addiction that has blighted her for the past 15 years.
The 53-year-old drug user, who preferred not to give her surname, said she was now able to lead a normal life because of Portugal’s enlightened approach that favours public health over the criminalisation of drug users.
Anna visits Lisbon’s ‘Centro das Taipas’ each week to receive the heroin substitute methadone.
She explained: “I had a good life, and when I started taking drugs I spoilt my life and now I am drug-free again and I am well. When I feel ok I will stop methadone, if necessary on an in-patient basis.”
The change in law that led to this treatment was a response to a growing drug problem in the late 1990s.
‘No problem’
Portugal had developed a reputation as a gateway for drug trafficking, with more than three quarters of drugs seized destined for other European countries.
By 1999, it had the highest rate of drug-related Aids cases in the EU and there was a growing perception that the criminalisation of drug use was increasingly part of the problem.
So in 2001, the socialist government changed the law to turn possession of drugs into an “administrative offence”, sending those caught with drugs for personal use to a “dissuasion board” rather than face prosecution.
At one of these hearings was a 32-year-old man who had been caught in possession of hashish.
Paulo showed no regret as he explained his case to a social worker and psychologist, saying: “I don’t feel I have a problem with drugs, so I don’t feel I need to be here”.
As this was his first appearance before the board he was just given a warning. If he is caught again, sanctions will be applied.
But far more drug users are taking up treatment as a result of the change in law, an independent study by Dr Alex Stevens from theUniversity of Kentfound.
It said the overall numbers of drug users in treatment expanded in Portugal from 23,654 to 38,532 between 1998 and 2008. While between 2000 and 2008 the number of case of HIV reduced among drug users from 907 to 267.
“This is a highly significant trend which as been attributed primarily to the expansion of harm reduction services,” it concluded.
Radical change
The advisor of the management board of the Instituto of Drugs in Portugal, Dr Fatima Trigeiros, said its partners had feared decriminalisation would make people flock to Portugal to take drugs, but that did not happen.
“Before the law changed people with drug consumption would fear to come into the treatment structures because they were afraid they would be taken to court,” she said.
Continue reading the main story
We have a government that on paper at last is a dream ticket for actually putting in place substantive reforms”
End Quote Danny Kushlick Transform
“Also we were not tackling first-time users, those who were experimenting, because the time between being caught and the time they were taken to court was too long. Now they are being taken to the dissuasion boards in 72 hours.”
Would the British government ever entertain such a radical change? The Home Office says decriminalisation is not the answer; instead it wants to reduce drug use and drug-related crime and help addicts kick their habit.
But there is evidence the prime minister thought differently when he was in opposition. Eight years ago, David Cameron wrote in the Daily Telegraph, that “politicians need to get up from behind their barricades and look at what works, rather than what sounds good”.
He called for a declassification of some drugs so cannabis would move from class B to class C and ecstasy from A to B, even allowing some severe heroin users access to injecting rooms.
As a backbench MP, Mr Cameron called on the government to raise a debate at the United Nations on legalisation and regulation. It was the clearest indication ever given by a future British prime minister of a desire to rethink drugs policy.
The charitable think tank “Transform”, which is lobbying for a change in the law, is hoping the prime minister’s past views will prevail.
Its head of external affairs, Danny Kushlick said: “We have a government that on paper at last is a dream ticket for actually putting in place substantive reforms that are going to shift resources from criminal justice and towards public health.”
With difficult public sector cuts looming, drug reform may not be the first priority of the British government, but it is now consulting on the UK Drugs Strategy.
Reformers say if they want to reduce spending on drugs they could do worse than to look to Portugal.
Source bbc.co.uk/news 3rd Oct.2010
A rebuttal of information by John Stossel of Fox News. 2nd March 2012
Mr Stossel. You are welcome to publish my response if you wish.
Your article about drugs is not backed up by the evidence, there is plenty of scope for drugs use to increase under a change of system where drugs use is normalised (either decrimininalisation or various legalization models). The evidence is in the tobacco/alcohol model /as variously applied/ around the world. Tobacco and alcohol cause far more /total harm/ than the illegal drugs simply through prevalence.
Your remarks about Portugal are not supported by a critical examination of what has taken place there. All the hyperbole about Portugal as a model is based on one flawed study, assiduously reported around the world as a “meme” by the George Soros financed, world-wide, legalisation campaign. You have been hoodwinked. Not surprising really, millions of dollars have been spent to do that to you.
Portugal and decriminalisation appears now to be “the new orthodoxy” for those with a certain direction of travel and for those “user advocates” who want more freedom to use, regardless of the wider social effects.
Portugal is being misrepresented
1. The number of new cases of HIV and Hepatitis C inPortugalis eight times the average in other EU countries
2.Portugal has the most cases of injected drug related AIDS with 85 new cases per one million citizens. Other EU countries averaging 5 per million.
3. Since decriminalisation, drug related homicides have increased 40%.
4. Drug overdoses have increased substantially, over 30% in 2005
5. There has been an increase of 45% in post mortems testing positive for illegal drugs
6. Amphetamine & cocaine consumption has doubled in Portugal with cocaine seizures increasing sevenfold between 2001 and 2006.
Finally the suggestion made by some, that legalisation would somehow remove criminality from drug supply is ridiculous. Criminality loves use-reinforcing substances and behaviours. More than 20% of the UK tobacco market is smuggled, counterfeit, or both. In some other countries it is much worse.
Legalisation or decriminalisation, of substances unfit for human consumption, should only occur if a demonstrable “public good” can be evidenced.
The problem for the legalisation lobby is that it cannot.
David Raynes.
Member. International Task force on Strategic Drug Policy
http://www.itfsdp.org/members.php
“It’s extraordinarily simplistic for the Global Commission to advocate that decriminalising drugs will lead to reduced addiction rates and less crime. The idea that drug abuse is a victimless crime is also hugely over-simplifying things.
In Scotland there is a huge problem with drug addiction and this has become dramatically worse over recent decades. Such is the scale of the problem now that we have a detection rate of just 1 per cent of all the heroin that’s consumed in Scotland.
That’s a figure we should be hugely discomforted by and it gives us an idea of the scale of the problem we’re facing. The Global Commission’s recommendations seem to have given up on the idea of getting addicts off drugs and seem to be accepting it’s a problem that’s here to stay.
As things stand, we are already leaving too many addicts for too long on methadone, for example. We need to have a policy of supporting people to move from increased stability to abstinence. Legalising drugs would open the floodgates to more drugs problems and would be a catastrophe for the country.
There are areas in Scotland where drug use is already rife, such as some estates in the cities of Edinburgh and Glasgow. If drugs were no longer illegal this would spread rapidly and get out of all control very quickly, we would end up with a drug problem that’s of a similar scale to the one we currently have with alcohol.
The policy advocated by the Global Commission would also lead to higher levels of crime and would corrupt the economy, and there would be huge economic power left with these businesses selling drugs. The power of the drugs gangs would remain in place, but they would now be legitimate in the eyes of the law and would be more likely to diversify into other areas of crime.
We would also see some companies that are currently legitimate corrupted by their involvement in the drugs trade. This has already happened in Columbia, where the gangs have become more powerful and have influence over more parts of society.
Drug dealers and organised crime would all of a sudden have so much more influence and this would be hugely damaging to Scottish society as a whole. We have to look at how to solve the problems with drugs in a much more measured way and that means having joined up strategies in place to treat addicts, as well as an effective criminal justice system.
One of the biggest problems of all though is that we have become too accustomed to having a drug problem in Scotland over the past 20 years and have allowed the problem to get worse and worse. The last thing we want is any sort of knee-jerk reaction or a rushed decision that has come up with all the wrong sorts of ideas. Prevention of drug addiction through education and early intervention have got to be at the heart of any anti-drugs strategy.
But we need to be very clear that a 1 per cent detection rate for all the heroin use in Scotland is just not acceptable and needs to be dramatically improved. The approach put forward by the Global Commission is certainly not the route to go down, as it would just escalate our problems with crime and addiction.
If we imagine just how bad things have become in Scotland with drug addiction and crime, we should stop to think how much worse they could be if these proposals to decriminalise drugs are introduced. The crisis could get much worse unless we have a sensible approach that gets to the heart of the problem”.
lNeil McKeganey is a professor of drug misuse research at the University of Glasgow
Source: Scotsman.com 2nd June 2011
As a leader of a nationally prominent anti-drug coalition in San Diego County, I was thoroughly disappointed with the California Medical Association’s recent report endorsing marijuana legalization as a way to speed research into medical marijuana. Unfortunately, the CMA conflated those two very different issues by recklessly supporting the risky proposition of legalization.
First, it is important to discuss the disastrous impact marijuana legalization would have on our state. Marijuana is illegal because it is dangerous – not dangerous because it’s illegal. Recent studies link the drug with cognitive impairment (think memory loss and other brain dysfunction), motor skills impairment (think drugged driving accidents), and mental illness (like psychosis and schizophrenia). Indeed, marijuana negatively impacts the development of the adolescent brain, which is still maturing until about age 25.
We also know, according to a recent RAND report, that the price of marijuana would fall dramatically if it were legalized. Our experience with alcohol and tobacco tells us that lower price means greater use and addiction rates. And while about 1 in 10 adults who ever start marijuana will become dependent on it, according to the National Institutes of Health, that number jumps to between 1 in 4 and 1 in 2 when the drug is initiated in adolescence. Calling for legalization for adults only and thinking it will prevent drug use among kids is naive and dangerous – just ask any kid who has easy access to alcohol and tobacco today, despite age limits.
Finally, marijuana tax revenues would pale in comparison to the social costs of the increased use of the drug. Again, our two legal drugs, alcohol and tobacco, can be used as a reference point – they bring in about one-tenth of the social costs they produce.
That one opposes legalization does not mean that one has to be all for the status quo. Indeed, we need to invest more into prevention programs to stop marijuana use before it starts, intervene on early use, and treat marijuana addiction.
Nor does opposition to legalization signal acrimony toward increased medical research into the individual components of marijuana. This is where CMA makes its mistake. The organization reasoned that legalization is the only way to achieve this kind of research. And it is wrong.
Research into the active ingredients of marijuana – and there are hundreds of them – is an important area of science that should be explored. Indeed, today we have two such drugs derived from marijuana and the FDA is currently exploring others, like Sativex. Sativex is a tongue spray that is comprised of the active ingredient in marijuana – THC – and another ingredient called CBD. The THC in marijuana is what gets someone “high,” and the CBD counteracts that so that the drug is not dangerous or dependence-inducing. Late-stage trials of the drug show promise for spasticity related to multiple sclerosis and pain related to cancer. It has been approved in other countries for these purposes, too.
The bottom line is that one of CMA’s core arguments is a myth – that the government’s prohibition of marijuana prevents proper investigation into the drug’s therapeutic properties. The National Institute on Drug Abuse grows marijuana, in several different strains and varieties, for this exact purpose. According to the Drug Enforcement Administration, which issues licenses to deal with marijuana for research purposes, over 200 researchers have access to the drug.
So it is unfortunate that the California Medical Association – representing only a small number of their doctors who pushed a legalization position from the start – is now mixing politics with science. Advocating for legalization as the only route to research not only displays an ignorance of the drug-approval process, but it also represents a platform that will have untold consequences from a profession that should, first and foremost, “do no harm.”
Source: www.signonsandiego.com 6th Nov 2011
Next November, Californians will ballot on allowing people 21 years and older to possess, cultivate and transport cannabis for personal use, as well as enable its commercial production and sale. Professor Keith Humphreys of Stanford University School of Medicine’s psychiatry and behavioural sciences departments, discusses the potential consequences.
He recently returned to Stanford after a one-year stint in the White House as a senior adviser on national drug control policy – and was a key speaker at the UK/European Symposium on Addictive Disorders inLondon last May.
Click here for related facts, also CannabisSkunk Support.
Q: There are estimates that, with legalisation, marijuana use could rise 50-100 percent%. Are those projections reasonable?
Humphreys: We know very well from other commodities that if you make something illegal, the price of it goes up. And when you make it legal, it becomes much cheaper. So the findings are credible. Why they’re scary is that big drops in price tend to affect mainly people with less disposable income…teenagers, the unemployed, other people who have just a small amount of extra money. This will drop marijuana to something they could easily afford to do on a daily basis.
It is not just legalising consumption; it is legalising production. That means you’re going to have an industry, like the tobacco industry, that will have lobbyists and marketers and lots of money. In fact, I wonder if tobacco companies might go into this business. They are well-positioned. They have the outlets and the pricing power. It will become a mass-produced, very cheap product.
Q: But the proposition also allows people to grow their own marijuana…
Humphreys: For the vast majority of people, if there’s a refined product in a nice package down at the store that costs 1/10th as much, and you don’t have to water or worry about sunlight, then they will buy it.
Q: What about the argument that taxing marijuana will provide much-needed revenue?
Humphreys: We should be legalising child pornography and human trafficking? There’s lots of awful things that raise money, and that doesn’t make them right. The second point is that taxes never recoup the harm from substances. If you look at all estimates of alcohol and tobacco taxation, it never even touched a fifth of the amount of health damage. So you get a little money in the short term, but in the long term, someone’s got to pay for car accidents and kids flunking out of school and things like that.
Q: What about the notion that by legalising it you take it out of clandestine operations?
Humphreys: You will probably get rid of some gun violence, for example. But look at the example of a tobacco company. You could have substantially more death. There’s lots of ways to do violence in this world. You can weaken government regulations in a way that results in thousands of people dying.
In terms of its medical use, I have compassion for patients; I was a hospice worker for many years. But I don’t feel that’s the typical person getting medical marijuana. A paper in the Harm Reduction Journal that profiled about 4,000 such people said the prototypical patient was a 30-year-old male who had been smoking pot for about 15 years and wasn’t seriously ill – that group is riding on our compassion for the people who have Aids, MS or cancer.
To me, it’s a pretty big jump to go from saying that this plant has some medical value, to saying that its consumption — and also its production and advertising — should be legalised.
Source: Addiction Today August 6th2010
Position Statement – December 2011
The flawed proposition of drug legalisation
Various well funded pressure groups have mounted campaigns to overturn the United Nations Conventions on drugs. These groups claim that society should accept the fact of drugs as a problem that will remain and, therefore, should be managed in a way that would enable millions of people to take advantage of an alleged ‘legal right’ to use drugs of their choice.
It is important to note that international law makes a distinction between “hard law” and “soft law.” Hard law is legally binding upon the States. Soft law is not binding. UN Conventions, such as the Conventions on Drugs, are considered hard law and must be upheld by the countries that have ratified the UN Drug Conventions.
International narcotics legislation is mainly made up of the three UN Conventions from 1961 (Single Convention on Narcotic Drugs), 1971 (Convention on Psychotropic Substances), and 1988 (Convention against Illicit Traffic in Narcotic Drugs and Psychotropic Substances):
• The 1961 Convention sets out that “the possession, use, trade in, distribution,import, export, manufacture and the production of drugs is exclusively limited to medical and scientific purposes”. Penal cooperation is to be established so as to ensure that drugs are only used licitly (for prescribed medical purposes).
• The 1971 Convention resembles closely the 1961 Convention, whilst
establishing an international control system for Psychotropic Substances.
• The 1988 Convention reflects the response of the international community to increasing illicit cultivation, production, manufacture, and trafficking activities. International narcotics legislation draws a line between licit (medical) and illicit (non-medical) use, and sets out measures for prevention of illicit use, including penal measures. The preamble to the 1961 Convention states that the parties to the Convention are “Recognizing that addiction to narcotic drugs constitutes a serious evil for the individual and is fraught with social and economic danger to mankind”. The Conventions are reviewed every ten years and have consistently been upheld.
The UN system of drug control includes the Office of Drugs and Crime, the International Narcotics Control Board, and the Commission on Narcotic Drugs. The works of these bodies are positive and essential in international drug demand and supply reduction. They are also attacked by those seeking to legalise drugs.
It is frequently and falsely asserted that the so-called “War on Drugs” is inappropriate and has become a very costly and demonstrable failure. It is declared by some that vast resources have been poured into the prevention of drug use and the suppression of illicit manufacturing, trafficking, and supply. It is further claimed that what is essentially a chronic medical problem has been turned into a criminal justice issue with inappropriate remedies that make “innocent” people criminals. In short, the flawed argument is that “prohibition” monies have been wasted and the immeasurable financial resources applied to this activity would be better spent for the general benefit of the community.
The groups supporting legalisation are: people who use drugs, those who believe that the present system of control does more harm than good, and those who are keen to make significant profits from marketing newly authorised addictive substances. In addition to pernicious distribution of drugs, dealers circulate specious and misleading information. They foster the erroneous belief that drugs are harmless, thus adding to even more confused thinking.
Superficially crafted, yet pseudo-persuasive arguments are put forward that can be accepted by many concerned, well intentioned people who have neither the time nor the knowledge to research the matter thoroughly, but accept them in good faith. Frequently high profile people claim that legalisation is the best way of addressing a major social problem without cogent supporting evidence. This too influences others, especially the ill informed who accept statements as being accurate and well informed. Through this ill-informed propaganda, people are asked to believe that such action would defeat the traffickers, take the profit out of the drug trade and solve the drug problem completely.
The total case for legalisation seems to be based on the assertion that the government assault on alleged civil liberties has been disastrously and expensively ineffective and counter-productive. In short, it is alleged, in contradiction to evidence, that prohibition has produced more costs than benefits and, therefore, the use of drugs on a personal basis should be permitted. Advocates claim that legalisation would eliminate the massive expenditure incurred by prohibition and would take the profit out of crime for suppliers and dealers. They further claim that it would decriminalise what they consider “understandable” human behaviour and thus prevent the overburdening of the criminal justice system that is manifestly failing to cope. It is further argued irrationally that police time would not be wasted on minor drug offences, the courts would be freed from the backlog of trivial cases and the prisons would not be used as warehouses for those who choose to use drugs, and the saved resources could be used more effectively.
Types of drug legalisation
The term “legalisation” can have any one of the following meanings:
1. Total Legalisation – All illicit drugs such as heroin, cocaine, methamphetamine, and marijuana would be legal and treated as commercial products. No government regulation would be required to oversee production, marketing, or distribution.
2. Regulated Legalisation – The production and distribution of drugs would be regulated by the government with limits on amounts that can be purchased and the age of purchasers. There would be no criminal or civil sanctions for possessing, manufacturing, or distributing drugs unless these actions violated the regulatory system. Drug sales could be taxed.
3. Decriminalisation – Decriminalisation eliminates criminal sanctions for drug use and provides civil sanctions for possession of drugs. To achieve the agenda of drug legalisation, advocates argue for:
• legalising drugs by lowering or ending penalties for drug possession and use – particularly marijuana;
• legalising marijuana and other illicit drugs as a so-called medicine;
• harm reduction programmes such as needle exchange programmes, drug injection sites, heroin distribution to addicts, and facilitation of so-called safe use of drugs that normalize drug use, create the illusion that drugs can be used safely if one just knows how, and eliminates a goal of abstinence from drugs;
• legalised growing of industrial hemp;
• an inclusion of drug users as equal partners in establishing and enforcing drug policy; and
• protection for drug users at the expense and to the detriment of non-users under the pretence of “human rights.”
The problem is with the drugs and not the drug policies
Legalisation of current illicit drugs, including marijuana, is not a viable solution to the global drug problem and would actually exacerbate the problem. The UN Drug Conventions were adopted because of the recognition by the international community that drugs are an enormous social problem and that the trade adversely affects the global economy and the viability of some countries that have become transit routes.
The huge sums of illegal money generated by the drug trade encourage money laundering and have become inextricably linked with other international organised criminal activities such as terrorism, human trafficking, prostitution and the arms trade. Drug Lords have subverted the democratic governments of some countries to the great detriment of law abiding citizens.
Drug abuse has had a major adverse effect on global health and the spread of communicable diseases such as AIDS/HIV. Control is vitally important for the protection of communities against these problems. There is international agreement in the UN Conventions that drugs should be produced legally under strict supervision to ensure adequate supplies only for medical and research purposes. The cumulative effects of prohibition and interdiction combined with education and treatment during 100 years of international drug control have had a significant impact in stemming the drug problem. Control is working and one can only imagine how much worse the problem would have become without it. For instance:
• In 2007, drug control had reduced the global opium supply to one-third the level in 1907 and even though current reports indicate recent increased cultivation in Afghanistan and production in Southeast Asia, overall production has not increased.
• During the last decade, world output of cocaine and amphetamines has stabilized; cannabis output has declined since 2004; and opium production has declined since 2008. We, therefore, strongly urge nations to uphold and enhance current efforts to prevent the use, cultivation, production, traffic, and sale of illegal drugs. We further urge our leaders to reject the legalisation of currently illicit drugs as an acceptable solution to the world’s drug problem because of the following reasons:
• Only 6.1% of people globally between the ages of 15 and 64 use drugs (World Drug Report 2011 UNODC) and there is little public support for the legalisation of highly dangerous substances. Prohibition has ensured that the total number of users is low because legal sanctions do influence people’s behaviour.
• There is a specific obligation to protect children from the harms of drugs, as is
evidenced through the ratification by the majority of United Nations Member States of the UN Convention on the Rights of the Child (CRC). Article 33 states that Member States “shall take all appropriate measures, including legislative, administrative, social and educational measures, to protect children from the illicit use of narcotic drugs and psychotropic substances as defined in the relevant international treaties, and to prevent the use of children in the illicit production and trafficking of such substances”.
• Legalisation sends the dangerous tacit message of approval, that drug use is
acceptable and cannot be very harmful.
• Permissibility, availability and accessibility of dangerous drugs will result in
increased consumption by many who otherwise would not consider using them.
• Enforcement of laws creates risks that discourage drug use. Laws clearly define what is legal and illegal and emphasise the boundaries.
• Legalisation would increase the risks to individuals, families, communities and world regions without any compensating benefits.
• Legalisation would remove the social sanctions normally supported by a legal system and expose people to additional risk, especially the young and vulnerable.
• The legalisation of drugs would lead inevitably to a greater number of dependencies and addictions likely to match the levels of licit addictive substances. In turn, this would lead to increasing related morbidity and mortality, the spread of communicable diseases such as AIDS/HIV and the other blood borne viruses exacerbated by the sharing of needles and drugs paraphernalia, and an increased burden on the health and social services.
• There would be no diminution in criminal justice costs as, contrary to the view held by those who support legalisation, crime would not be eliminated or reduced. Dependency often brings with it dysfunctional families together with increased domestic child abuse.
• There will be increases in drugged driving and industrial accidents.
• Drug Control is a safeguard protecting millions from the effects of drug abuse and addiction particularly, but not exclusively, in developing countries.
• Statements about taxation offsetting any additional costs are demonstrably flawed and this has been shown in the case of alcohol and tobacco taxes. Short of governments distributing free drugs, those who commit crime now to obtain them would continue to do so if they became legal.
• Legalisation would not take the profit out of the drug trade as criminals will always find ways of countering legislation. They would continue their dangerous activities including cutting drugs with harmful substances to maximise sales and profits. Aggressive marketing techniques, designed to promote increased sales and use, would be applied rigorously to devastating effect.
• Other ‘legal’ drugs – alcohol and tobacco, are regularly traded on the black market and are an international smuggling problem; an estimated 600 billion cigarettes are smuggled annually (World Drug report 2009). Taxation monies raised from these products go nowhere near addressing consequential costs.
• Many prisons have become incubators for infection and the spread of drug related diseases at great risk to individual prisoners, prison staff and the general public. Failure to eliminate drug use in these institutions exacerbates the problem.
• The prisons are not full of people who have been convicted for mere possession of drugs for personal use. This sanction is usually reserved for dealers and those who commit crime in the furtherance of their possession.
• The claim that alcohol and tobacco may cause more harm than some drugs is not a pharmacokinetics of psychotropic substances suggest that more, not less, control of their access is warranted.
• Research regularly and increasingly demonstrates the harms associated with drug use and misuse. There is uncertainty, yet growing evidence, about the long-term detrimental effects of drug use on the physical, psychological and emotional health of substance users.
• It is inaccurate to suggest that the personal use of drugs has no consequential and damaging effects. Apart from the harm to the individual users, drugs affect others by addiction, violence, criminal behaviour and road accidents. Some drugs remain in the body for long periods and adversely affect performance and behaviour beyond the time of so-called ‘private’ use. Legalisation would not diminish the adverse effects associated with drug misuse such as criminal, irrational and violent behaviour and the mental and physical harm that occurs in many users.
• All drugs can be dangerous including prescription and over the counter medicines if they are taken without attention to medical guidance. Recent research has confirmed just how harmful drug use can be and there is now overwhelming evidence (certainly in the case of cannabis) to make consideration of legalisation irresponsible.
• The toxicity of drugs is not a matter for debate or a vote. People are entitled to their own opinions but not their own facts. Those who advocate freedom of choice cannot create freedom from adverse consequences.
• Drug production causes huge ecological damage and crop erosion in drug producing areas.
• Nearly every nation has signed the UN Conventions on drug control. Any government of signatory countries contemplating legalisation would be in breach of agreements under the UN Conventions which recognise that unity is the best approach to combating the global drug problem. The administrative burden associated with legalisation would become enormous and probably unaffordable to most governments. Legalisation would require a massive government commitment to production, supply, security and a bureaucracy that would necessarily increase the need for the employment at great and unaffordable cost for all of the staff necessary to facilitate that development.
• Any government policy must be motivated by the consideration that it must first do no harm. There is an obligation to protect citizens and the compassionate and sensible method must be to do everything possible to reduce drug dependency and misuse, not to encourage or facilitate it. Any failures in a common approach to a problem would result in a complete breakdown in effectiveness. Differing and fragmented responses to a common predicament are unacceptable for the wellbeing of the international community. It is incumbent on national governments to cooperate in securing the greatest good for the greatest number.
ISSUED this 21st day of December, 2011 by the following groups:
Drug Prevention Network of the Americas (DPNA)
Institute on Global Drug Policy
International Scientific and Medical Forum on Drug Abuse
International Task Force on Strategic Drug Policy
People Against Drug Dependence & Ignorance (PADDI), Nigeria
Europe Against Drugs (EURAD)
World Federation Against Drugs (WFAD)
Peoples Recovery, Empowerment and Development Assistance (PREDA)
Drug Free Scotland
Following the Scottish example, England has piloted drug courts using specially trained magistrates to closely supervise treatment-based community sentences. This initial report found no major glitches but low throughput and uncertain cost-benefits.
Summary The Dedicated Drug Court framework for England and Wales provides for specialist courts which exclusively handle cases relating to drug misusing offenders from conviction through sentence to completion (or breach) of a community order with a Drug Rehabilitation Requirement (DRR). Two magistrates’ courts (Leeds Magistrates’ Court and West London Magistrates’ Court) have been piloting drug courts implemented in line with the Ministry of Justice’s framework.
The critical factors for implementation success are an understanding of local context and scale of need, the enthusiasm of the local judiciary and partner agencies, good partnership working, availability of resources to deliver the drug court and its associated treatment services, the depth of understanding by all staff of offender motivation and, in particular, recognition of the points at which an offender is most likely to make progress in reducing or stopping drug use. Continuity of judiciary is key to successful implementation of a drug court. It provides the focus for communication between the court and the offender and across magistrate panels. Continuity of judiciary was a strong planned feature of both courts. Based on analysis undertaken with data from the Leeds pilot, there is strong evidence that continuity of magistrates has a statistically significant impact on several key drug court outcomes. Greater continuity of magistrates experienced by offenders is associated with their being less likely to miss a court hearing, more likely to complete their sentence, and less likely to be reconvicted.
Break-even analysis showed that (compared to normal adjudication) an extra 8% of offenders seen by the courts would need to stop taking drugs for five years or more following completion of the sentence to provide a net economic benefit to the wider society, and 14% in order to provide a net economic benefit to the criminal justice system. A robust quantification of impact was not possible because of the difficulties in collecting sufficient data on a comparison group of offenders not processed through drug courts.
Findings Commissioned by the UK Ministry of Justice, the report describes the implementation rather than the outcomes of England’s pilot drug courts. In line with international understandings, the courts were intended to specialise in drug-related offenders, presided over by sentencers specially trained for this task who order treatment-based sentences and closely supervise the offender’s progress, aided by regular tests for illegal drug use. The aim is maximise the rehabilitative impact of the sentence by increasing compliance and engagement with treatment through criminal justice pressure (ultimately the prospect of receiving a more typical punishment-based sentence if the drug court’s order fails) and rewards (of which one of the most powerful seems to be the unfamiliar experience of being congratulated by a judge or magistrate).
The report identified no critical fault lines in the implementation of the courts. However, these were particularly promising sites: the Leeds court built on a pre-existing system and in London, court staff were enthusiastic about the proposal and had already been working towards creating a drug court. Nevertheless, offender throughput was lower than expected. Over the 17 months of the evaluation, the London court sentenced just 60 new offenders while in Leeds the total was 276. Low throughput raised costs per offender. Compared to a standard 12-month drug rehabilitation requirement order implemented through normal adjudication, supervising the order through the drug courts cost £4633 extra per offender.
With no comparison group of normally adjudicated offenders, the evaluation was unable to say whether this was money well spent. They were, however, able to calculate the drug use reductions the courts would have to ‘buy’ in order to meet their extra costs – as noted in the abstract, the answer was 8% of offenders ceasing drug use for at least five years compared to the numbers doing so on a normally adjudicated drug rehabilitation requirement order. This calculation though excludes the base costs of normal adjudication and of a normally supervised drug rehabilitation requirement order. This seems to mean that the 8% would also have to be over and above the proportion of offenders who remain abstinent after normal judicial processing. The report gives no indication of how much success would be needed to match the total costs incurred by the criminal justice system in implementing all the elements of a drug court-supervised drug rehabilitation requirement order.
The report’s emphasis on offenders seeing the same magistrate(s) for their sentencing and throughout subsequent progress reviews is backed by evidence from Leeds that continuity is substantially associated with better compliance and drug use and crime outcomes. Steps were taken to reduce the risk that continuity was caused by high compliance and good progress rather than vice versa. However, without actually allocating offenders at random to see or not see the same magistrates, it is impossible to eliminate this possibility. Assuming the effect was real, it is of concern that organising continuity was a challenge, and especially so for ‘breach’ hearings dealing with unacceptable failures to comply with the order, which national regulations required to occur within a set period. Unfortunately, these crucial junctures are just when continuity is most needed, requiring an understanding of whether the offender will do better on a revised order, or the order has failed and should be revoked, often resulting in imprisonment.
A final caution over any such report is that some leading criminologists accuse the UK government of manipulating and distorting criminological research for political gain, to the point where the professor of criminology at the Open University has called for a boycott of government-commissioned work. The featured report was commissioned by the UK Ministry of Justice, a ministry carved out in part from the Home Office, one of the main targets of these accusations.
Scotland preceded England in formally piloting drug courts in Glasgow from 2001 and in Fife the following year. As in England, implementation was not entirely smooth but better than might have been expected. There was a high but it was thought acceptable failure rate, probably aided by Scotland’s more flexible application of drug treatment and testing orders, predecessors to the drug rehabilitation requirements used later by the English courts. However, crime impacts were questionable. Within one year 50% of drug court offenders had been reconvicted and within two years 71%, and the average frequency of reconvictions only slightly dipped in the two years after the order was imposed compared to the two years before. There was no clear crime-reduction benefit from supervising the orders through the drug courts (at an average cost of nearly £18,500 per order) as opposed to normal adjudication. But, as in England, the costs imposed on society by persistent, high-rate offending and drug-related mortality and morbidity, are such that even modest improvements might be cost-beneficial overall.
International experience and research relating to drug courts suggests it is important for courts to emphasise rewards as well as punishments, see offenders frequently enough to apply these swiftly in response to progress, deploy a range of rewards and sanctions short of revocation which are consistently applied, have a strong and sure ultimate sanction when the programme fails, make these consequences absolutely clear to offenders, have rapid access to a range of treatment options, maintain continuity in the judge dealing with the case, and to attend to the range of the individual’s needs. Willingness to continue despite some initial offending makes the structure imposed by stringent requirements and monitoring a positive feature rather than one which leads most offenders to fail. Consistent judicial supervision, the fact that this forces addicts (back) in to treatment, and drug testing which provides a shared measure of how treatment is progressing, probably all play their parts.
Source: www.findings.org.uk March 2009
The fashionable party drug mephedrone has been linked to up to 98 recent deaths in Britain, the Government’s advisers warned last night, as they called for tougher action to combat the proliferation of legal highs.
The Advisory Council on the Misuse of Drugs (ACMD) said unscrupulous manufacturers made a mockery of the law by falsely advertising addictive substances as “plant food” or “bath salts”. Its chairman, Professor Les Iverson, warned young users of “designer drugs” were playing “Russian roulette” with their lives – and said the effects were already being seen in hospitals. He said: “We are not seeing just a nice party drug but something that can kill.”
Prof Iverson released figures showing that in the past two years mephedrone had been confirmed as a factor in 42 deaths and had not been ruled out as contributing to another 56.
Users of designer drugs – created in labs to mimic the make-up of banned substances such as ecstasy and amphetamines – suffered such extreme side-effects that they had to be sedated. They had also been treated for paranoia, psychosis, high heart rates and raised blood pressure, he said. He added: “Users are playing Russian roulette. They are buying substances marked as research chemicals. The implication is that you should do the research on yourself to find out whether they’re safe or not. This is a totally uncontrolled, unregulated market.”
The first large quantities of legal highs, or psychoactive drugs – many made in China – appeared in Britain two years ago. They can be easily bought online or from shops selling drug paraphernalia and herbal goods. Some undergraduates also sell them to fellow students. The ACMD said: “Many people importing these new substances appear to have had no previous involvement in the illicit drug trade and are just in it to make a quick buck. They have included students who have set up websites to supply nationally and who also supply the local student population.”
Ministers have outlawed several such substances, but the ACMD warned that producers were sidestepping the bans by tweaking the composition of drugs. It backed creating a new system of broader bans in which all substances chemically similar to controlled drugs were automatically made illegal. The ACMD also called for suppliers to have to demonstrate that legal highs were not being produced for human consumption and for a fresh drive to alert the public to their dangers.
Roger Howard, chief executive of the UK Drug Policy Commission, backed the proposals. He said: “We have rapidly growing numbers of psychoactive drugs on the market and it’s increasingly difficult for police to identify the different drugs they are finding.”
The Home Office said it was considering the recommendations and added: “The Government is leading the way in cracking down on legal highs by outlawing not just individual drugs but whole families of related substances.”
By numbers…
2009 The year police made first seizure of mephedrone. It was banned in 2010.
£15 Approximate price of a gram before it was classified.
98 The number of deaths recently linked to mephedrone.
Source: The Independent 26th October
More than 20 cannabis farms and factories were discovered by police every day last year as they seized drugs which could sell for £100 million on the streets, figures showed today.
Senior police chiefs said the size and scale of the farms were reducing as criminals producing cannabis were spreading the risk and minimising losses by employing a large number of so-called gardeners to manage small sites across multiple residential areas.
Over the two years since the last report by the Association of Chief Police Officers (Acpo), some 1.1 million plants have been seized with a street value of £207.4 million.
A total of 7,865 farms were found across the UK in 2011/12, up 15% from 6,866 in 2009/10 and more than a 150% increase from the 3,032 identified four years ago, the study by the Association of Chief Police Officers (Acpo) found.
There has been a “move back to the use of residential property” and dismantling factories was seen as “a short term solution, with missed opportunities for further investigation into potentially linked factories”, the police chiefs said.
The number of offences related to cannabis production is also increasing, up from 14,982 in 2010/11 to 16,464 last year.
Scotland Yard Commander Allan Gibson, the lead on cannabis cultivation for the police chiefs, said: “Commercial cannabis cultivation continues to pose a significant risk to the UK .
“Increasing numbers of organised crime groups are diverting into this area of criminality but we are determined to continue to disrupt such networks and reduce the harm caused by drugs.
“This profile provides a detailed analysis of the current threat from commercial cultivation of cannabis and the work undertaken by law enforcement agencies to combat the threat.”
The highest number of farms (936) were found in the West Yorkshire force area, equivalent to 42 factories per 100,000 people, the Acpo figures showed.
But South Yorkshire had 64 farms per 100,000 people, the highest ratio in the UK , with 851 farms.
The two forces were followed by other heavily-populated force areas, including West Midlands (663 farms, or 25 per 100,000 people), the Metropolitan Police (608 farms, or eight per 100,000 people) and Avon and Somerset (653 farms, or 40 per 100,000 people).
But the Devon and Cornwall force recorded the highest rise in the number of farms since the last report in 2009/10, with the number of farms identified rising 1,664% from 11 to 183 (11 farms per 100,000 people)
Source: www.Independent.co.uk 30th April 2012
Latest in an impressively coherent and persistent series of studies of how US courts specialising in supervision and treatment of drug-related offenders can do more to reduce drug use and crime. Triaging offenders to more or less intensive programmes and then adjusting based on actual progress made significant differences.
Summary Drug courts specialise in closely supervising (through regular urine tests and court appearances) and ordering the treatment of drug-related offenders to improve compliance with treatment as an alternative to prosecution or imprisonment. Judges impose sanctions or offer praise or more tangible rewards and adjust treatment depending on progress. However, in the USA this intensive process is available to only a small minority of potentially suitable offenders. Extending the reach of drug courts may be more feasible if intensive supervision and treatment are reserved for offenders who need them in order to do well, and if these decisions can to a degree be routinised rather than made on an individual basis.
Background to the study
One step towards this is to match intensity to the risk that the offender will fail to meet the requirements of the court, imposing stricter supervision on offenders assessed as high risk before the start of their sentences. As described by Findings, this has been trialled by the research group responsible for the featured study. They found that high risk (antisocial personality disorder or a history of treatment for drug abuse problems) offenders were more likely to test negative for drugs and to complete their court orders when they had been randomly assigned to fortnightly court progress hearings rather than hearings ‘as needed’ in response to infractions. A further trial implemented this matching procedure and again found better outcomes among high risk offenders matched to fortnightly hearings.
However, predicting in advance how offenders will react to different drug court requirements is an imperfect science. Another step forward is to adapt these to how offenders actually do respond, if possible based on pre-set criteria derived from research findings. For example, if a participant misses a set number of counselling sessions, an ‘adaptive’ regimen might stipulate a motivational enhancement intervention. Treatment staff retain authority to override or alter an adaptation, but typically have to explain their decisions. The featured study was the first major test of adaptive programming in a drug court.
Deciding who needs more supervision or treatment
The criteria for adapting the drug court regimen and the adaptations were developed by the drug court team and research staff with a view to being feasible as well as effective. As in earlier studies in the series, first offenders were categorised as high or low risk and assigned on this basis to fortnightly or as-needed hearings. Monthly assessments identified those who did not comply with the court’s requirements, indicated by two or more unexcused missed counselling sessions or failures to provide a valid urine specimen. In these instances it was assumed that judicial supervision was inadequate and it was stepped up to fortnightly or, if already fortnightly, further infractions would result in conviction for the original offence.
At other times offenders might attend treatment and comply with tests, but still carry on using illegal drugs, indicated by two or more positive urine tests. In these instances it was assumed that the treatment A minimum of four months (approximately 18 weeks) of weekly group psychoeducational counselling sessions covering the pharmacology of drug and alcohol use, progression from substance use to dependence, the impact of addiction on the family, treatment options, HIV/AIDS risk reduction, and relapse prevention strategies. Participants could also attend group or individual treatment sessions based on clinical need. was inadequate and its intensity was stepped up to include clinical case management entailing an additional two therapeutic group sessions per week and one individual session per month focused on motivational enhancement and relapse-prevention techniques.
A pilot study demonstrated the feasibility and promise of this approach, paving the way for the featured study.
About the study
Essentially the featured study tested whether in addition to triaging based on starting risk levels, adjusting treatment and supervision based on the offender’s actual progress improved outcomes. Both the pilot and the featured study were conducted in a drug court in the city of Wilmington, the largest in the USstate of Delaware. It accepted adult local residents charged with a misdemeanour Less serious offences such as possession or use of cannabis or possession of equipment related to drug use. without a history of a serious violent offending, and who drug court treatment staff assessed as meeting criteria for substance abuse or dependence. Defendants plead guilty but will be absolved if they satisfactorily complete Minimum requirements are attending at least 12 weekly group counselling sessions, providing at least 14 consecutive weekly drug-negative urine specimens, remaining arrest free, obeying programme rules and procedures, and paying a $200 court fee. the drug court programme and are not arrested for the next six months. Failing this they are convicted, have a criminal record, stand to lose their driving licences, and to be sentenced to a period on probation.
In 2009 and 2010 researchers approached 335 consecutive drug court defendants of whom 130 agreed to join the study (risking allocation to more intensive supervision and treatment than usual) and 125 actually started the programmes it tested. All were triaged based on their risk levels As in previous studies, antisocial personality disorder or prior treatment for drug problems indicated high risk and fortnightly hearings. to fortnightly or as-needed hearings and their progress was monitored monthly by researchers and reported back to the drug court.
Using the criteria outlined above, for a randomly selected 62 offenders, these monthly assessments determined Unless the drug court team or judge decided otherwise. whether those failing to comply with attendance and testing requirements were subject to more frequent or stricter supervision, and whether those still using drugs were directed in to more intensive treatment. Remaining offenders were subject to the court’s usual procedures.
Primarily at issue was whether adapting treatment/supervision to progress reduced drug use, as indicated by weekly urine tests over the first 18 weeks of the drug court sentence, the minimum needed to complete it.
Main findings
The key finding was that offenders subject to the predetermined adaptations were less likely to use illegal drugs. Of the urine tests they took, 68% indicated they were drug free compared to 49% of comparison offenders. Assuming missed tests would have indicated drug use, the figures were 61% and 46%. Under either assumption, offenders whose supervision and treatment were adapted to their progress were over twice as likely as other offenders to submit a urine test negative for illegal drugs, a statistically significant difference, and one which was apparent over the entire 18 weeks.
In contrast, the proportions of offenders who satisfactorily completed the drug court programme within 18 weeks (31% in the adaptive regimen, 23% of the remainder) or within a year (68% and 67% respectively) did not significantly differ.
Just over a third of both sets of offenders at some time failed to meet criteria for complying with attendance or urine test requirements. These infractions were much more likely (64% v. 30%) to be responded to by the court when offenders were subject to the adaptive regimen and the court had been alerted to the infraction by the researchers. Also, roughly the same proportions (a fifth to a quarter) of offenders continued to use illegal drugs, though in this case the court was no more likely impose consequences on offenders in the adaptive programme.
There was a (not statistically significant) tendency for more offenders in the adaptive programme to see the drug court’s procedures as fair, but otherwise no differences in perceptions of how effectively these acted as deterrents, attitudes to the judge, and satisfaction with drug court services, all of which were generally positive.
The authors’ conclusions
Findings confirmed that adaptive programming can promote abstinence from illegal drugs among misdemeanour offenders sentenced by a drug court. This improvement in drug abstinence rates appears to have been attributable to more intensive supervision of offenders who failed to comply with attendance and testing requirements, rather than to more intensive and individualised treatment in response to continued drug use.
As intended, the criteria set for adapting the regimen, alerts to when these were breached, and the clear structure for how the court should respond, seem to have helped staff identify and rectify mismatches between offenders and the supervision schedule they had been assigned to on the basis of their anticipated risk of failure. In theory, drug court staff could have made these adjustments on their own initiatives, but were much less likely to do so without the guidance and assistance of the adaptive structure. Lacking this, they imposed consequences in respect of less than one in three of the times when offenders failed to show up for treatment or testing, a ratio unlikely to optimally promote compliance with supervision requirements. The adaptive regimen meant fewer offenders ‘slipped through the cracks’ to continue noncompliant behaviour with relative impunity. There was no indication (if anything, the reverse) that this greater strictness jaundiced offenders’ views of the court or its procedures.
Strangely, while offenders whose programmes were adapted were more likely to test abstinent, they were no more likely to satisfactorily complete the drug court programme, despite the fact that a run of 14 ‘clean’ urine tests was perhaps the primary requirement. It could be that the adaptive regimen failed to affect the other criteria offenders had to meet to satisfy the court and expunge their offence, or that the court took other factors in to account in making these decisions.
One methodological concern is that under 4 in 10 of the offenders asked to join the study did so, reducing the degree to which the findings can be assumed to be representative of what would happen if such procedures were applied across the board. It seems likely that refusers were less motivated to comply with the court’s requirements or felt (perhaps due to their addiction) that they would be unable to satisfy the court if more intensively supervised. Also, rather than persisting impacts, these findings reflected periods when many offenders had recently ended or were still on drug court sentences.
There may be scope to improve criteria used to adapt supervision and treatment. For example, the assumption that non-attendance for counselling or testing does not require more intensive treatment may be false if offenders who have lapsed try to hide this by not turning up. And while supervision and treatment could be intensified in response to poor progress, there was no mechanism for good progress to trigger the reverse.
Marlowe D.B., Festinger D.S., Dugosh K.L. et al.
Criminal Justice and Behavior: 2012, 39(4), p. 514–532.
This is the latest in an impressively coherent and persistent attempt to evidence howUSdrug courts can do more to reduce drug use and crime, including ways to conserve resources by reserving intensive intervention for offenders who need it. These studies have shown that triaging on the basis of initial risk and then adjusting in the light of experience, based on simple and clear criteria and feasible treatment and supervision enhancements, are both possible for US drug courts and effective in promoting abstinence from illegal drugs. In turn this finding confirms that some kind of courts are more effective than others. Generally drug court sentences are associated with lower crime and drug use rates than comparison sentencing options, but there are not enough rigorous and convincing studies to be sure that this is due to drug court procedures as opposed to the type of offenders seen by drug courts or some other factor. Feeling more the weight than the quality of the evidence, generally reviewers have cautiously concluded that drug courts are more effective then conventional sentencing, but this largely US evidence is of doubtful relevance to the UK, where negative findings from Scotland may have contributed to a waning in enthusiasm at a national level for extending the drug court model to more offenders. Details below.
About the study
While the strategies tested by the featured study and its predecessors may seem obvious, deciding on the criteria for risk, the dividing line between poor versus good progress, and corresponding adjustments to supervision and treatment, is not straightforward. In the US context, and particularly in the context of a court trying less serious offences, triaging on the basis of antisocial tendencies and prior drug treatment and then adjusting on the basis of two missed appointments or urine tests had in some respects the desired impact. As the authors pondered, the puzzle is why this impact did not extend to what for the offender is probably the critical outcome – successfully completing the sentence.
For society and Britainin particular, crime-reduction is probably the critical outcome. Whether the full adaptive regimen reduced criminal recidivism is as yet unreported, but a prior study found that the first step – triaging high-riskUS misdemeanour offenders to fortnightly supervision – did not do so to a statistically significant degree. According to their confidential accounts to researchers, among high-risk offenders in this study the reduction in the proportion who offended was greater (down by 23% v. 7%) when they had been left to the court’s usual (roughly monthly) hearings.
The authors of the featured study suggest that rather than intensified treatment, imposing tighter supervision and more certain sanctions was how the adaptive regimen helped offenders avoid illegal drug use. This raises the issue of whether for these types of offenders, treatment can be dispensed with altogether and supervision and sanctions relied on to enforce compliance. For what seems to have been a mainly methamphetamine using caseload, this was essentially the proposition tested in Hawaii. Where the featured study reserved more intensive treatment for offenders with positive urine tests, inHawaii they took this a step further by reserving treatment as such. There intensive urine testing allied with swift and certain but not severe sanctions for non-compliance dramatically curbed drug use, prison time and re-arrest rates among a high risk group of drug using offenders. Treatment was available for offenders who wanted it or whose repeat positive drug tests suggested it was needed, but few did want or need it – perhaps 1 in 10.
British policy and experience
In the featured study’s drug court it seems that most offenders confined their regular illegal drug use to cannabis. In Hawaii, a stimulant was the main problem drug and opiate use was rare. These caseloads are very different from the dependent heroin users who have committed serious and/or repeated offences who constitute the major part of the caseload in drug courts in England and Scotland. It seems unlikely that many in the UK would be considered at low risk of reoffending, that fortnightly classes would be considered an adequate treatment for their addictions, or that many could sustain four months without registering some form of illegal drug use in at least two weekly urine tests. Generally they would be considered to warrant at least the intensity of treatment reserved for the minority of poor responders in the featured study. Though this means that in the British context, risk criteria and adaptive responses would have to be different, the principle of establishing these, and doing so on the basis of evidence rather than intuition, is likely to be applicable. If costly sentence failure and imprisonment are to be avoided, it seems critical that such adjustments are made before offenders get to the point where their breaches lead the court to revoke the drug court order and re-sentence for the original offence.
Drug courts have operated in Englandand Scotlandfor several years but are not widespread. In six pilot English courts, involved offenders and professionals felt the courts were a useful addition to the range of initiatives aimed at reducing drug use and offending. They set concrete goals for offenders to meet, raised self-esteem, and imposed a degree of accountability for their actions on offenders. They were also seen as facilitating partnership working between agencies. However, Scottish courts too were seen as useful and effective, yet there was no reliable evidence that (despite costing substantially more per order and per successfully completed order) their sentences were any more effective than similar orders made by other courts, as assessed by the proportions of offenders reconvicted and the frequency of convictions.
The 2010 English drug strategy made no specific mention of drug courts. For more details on criminal justice policy it referred to a Ministry of Justice green paper, which warned that drug courts “will only be continued if they genuinely make a difference and are cost effective”. Evidence gathered for the paper was equivocal about the applicability of international evidence to England and Wales and did not list drug courts among its “promising approaches”. The applicability of reasonably promising evidence from overseas (primarily the USA) was also questioned by the UK Drug Policy Commission in its review of programmes for problem drug-using offenders.
Scotland’s drug strategy published in 2008 looked forward to the assessment of the country’s pilot drug courts cited above, which found no reliable crime-reduction impact but increased cost. A review of interventions for drug using offenders produced for the Scottish Government accepted these findings, and warned that the most rigorous international trials which randomly allocated offenders to drug courts or other judicial options found only weak crime reduction impacts which fell short of statistical significance.
Given the negative crime reduction findings in Scotland, the lack of evidence in the rest of Britain, and doubts about the validity and applicability of mainly USinternational evidence, the national-level impetus apparent a few years ago for trying drug courts in Britainmay have waned. Treatment allied with urine or other biological tests for drug use remain high on the UKagenda, but drug courts no longer appear to be seen as a prime means of ensuring and supervising such programmes. Nevertheless, such courts could be seen as one way to ensure offenders enter and comply with the treatment programmes (and specifically addiction treatment) the Ministry of Justice saw as effective in reducing the costs of crime, or one way local areas may choose to pursue the crime reductions which it suggested could attract financial rewards in ‘payment by results’ schemes.
Recent reviews
Reservations in the Scottish review cited above over the evidence for drug courts from randomised trials were echoed in a review conducted by British experts for the Swedish Council for Crime Prevention. It was able to synthesise crime-reduction results from just two high quality trials. Together these registered an advantage for drug courts versus comparison judicial options, but not one which was statistically significant. According to this analysis, treatment in general had been shown to reduce drug-related crime, but the same could not yet be said of treatment delivered via a drug court.
Mandated by USlaw, in 2011 the USGeneral Accounting Office investigated how well US adult drug courts have reduced crime and substance use and their associated costs and benefits. They reported that compared to alternative dispositions, generally studies found drug courts were associated with lower rates of criminal recidivism and relapse to drug use, but few studies were free of possible bias arising from non-random selection of drug court versus comparison offenders. Due mainly to reduced future victimisation and justice system expenditures, benefits to society expressed in financial terms usually but not always outweighed costs. This balance was partly dependent on the expense of the alternative disposal; if community sentences supervised by a drug court replaced prison, the cost savings were likely to be positive and substantial.
In hedging its cost-benefit findings, the General Accounting Office touched on a fundamental criticism of US drug courts – that most exclude violent or drug dealing offenders or those with extensive criminal histories and serious mental health issues. The upshot is often a caseload of low-level drug offenders who are otherwise generally law-abiding, many of whom might have been more cheaply and appropriately diverted out of the criminal justice system altogether. The report also echoed a general finding in other research syntheses – that the more sound the study, the less likely it is to find any substantial recidivism reductions due to drug courts.
How far most studies fall short of the gold standard randomised controlled trial was commented on by (at the time of writing) the latest synthesis of drug court studies. Among this “methodologically weak” body of work, just three of 92 studies of courts Other than those dealing with traffic-related offences. trying adults had randomly allocated offenders to these versus alternative judicial procedures. Across these three, recidivism was lower among drug court offenders, but the finding was not statistically significant. The next most sound studies typically attempted instead to match drug court and comparison offenders on key variables, or to adjust the findings for their relative risks of offending. Across these 20 studies, recidivism was modestly and significantly lower among drug court offenders, but such research designs have limited power to iron out the most important differences between offenders who are or are not referred to (or choose to be processed by) drug courts. Presumably crucial variables – like how committed the offenders is to succeed, their social and family support, or professional assessments of how well suited they are to a drug court regimen – are rarely available to researchers. Echoing the featured study, this synthesis found that drug use was lowest in courts which supervised offenders frequently and which – like the court in the study – could hold out the prospect that success would expunge the original offence. These too were among the effective ingredients identified in a major study funded by the US Department of Justice of 23 drug courts.
For Findings drug court analysis run this search. In particular see these background notes with a detailed consideration of one of the most methodologically rigorous studies to date, conducted in Baltimore with a caseload unusually relevant to the UK because it consisted mainly of heroin addicts with extensive criminal records. Though methodological concerns remained, it found that over the three years after offenders had been allocated to the court or to normal proceedings, the average numbers of new arrests and charges were significantly fewer among drug court offenders and drug use was lower.
Source www.findings.org.uk 30 March 2012
Powered by WordPress



