|

Promoting Good Practice In Prevention
|
Submitted by Maggie Petito on behalf of drugwatch international
14 April 2026
Of late, numerous marijuana advocates state in the media that legalization for all marijuana is needed so that research can be done to determine marijuana’s effects. Recognition of who is advancing the argument indicates much about the quality of the argument -Maggie Petito
Washington Post article: by Sarah Klein – 14 April 2026:
As more states legalize recreational marijuana use, here’s what the research says about what cannabis is really doing to your brain.
Marijuana use seems to be more popular (or at least more openly talked about) than ever. Regardless of whether you’re on the gummy bandwagon, you might wonder how it really affects your brain after the buzz wears off.
About 15.4 percent of Americans older than 12 have used cannabis in the past month, according to 2024 data from the Substance Abuse and Mental Health Services Administration. That number has been increasing as new marijuana products hit the market and more states legalize its use, according to the Centers for Disease Control and Prevention.
Older adults — those 60 and older — are the fastest-growing group of cannabis users in the country. According to a 2022 study, adults over 60 who started using did so for medical reasons, including to treat pain and arthritis, sleep disturbances, anxiety and depression.
While more than three-quarters of those people found the cannabis either somewhat or very helpful, the question remains: What are the side effects? You may be particularly curious about brain effects, given concerns about cognitive decline. So what exactly does the research say?
Cannabis use is linked to worse working memory
This probably isn’t too surprising, but cannabis can affect your ability to retain information in the short term. This makes some intuitive sense to anyone who has tried it: “If you smoke cannabis, afterward, if you do a working memory test where you’re trying to maintain some piece of information, like a phone number or a short list of words, you’re less good at doing that while you’re acutely intoxicated,” said Joseph Schacht, associate professor of psychiatry and co-director of the Division of Addiction Science, Prevention and Treatment at the University of Colorado School of Medicine.
But lifetime use seems to have a similar effect. Consistent cannabis users tend to have lasting memory deficits compared with nonusers, he said. In a January 2025 study in JAMA Network Open, the largest of its kind, researchers looked at the effects of cannabis use on more than 1,000 adults ages 22 to 36 using brain imaging. Heavy lifetime users exhibited lower brain activity during a working memory task compared with nonusers after excluding recent users.
There isn’t much research on potential long-term memory effects, but it’s a growing area of study as more older adults use cannabis. “Essentially baby boomers who grew up using cannabis are [now] using it in older age but experiencing some of those effects on working memory,” Schacht said. Available research suggests no overarching association between cannabis use and cognitive decline or dementia risk, although larger and longer studies are needed on this topic.
It’s tied to changes in brain volume
Long-term cannabis use has also been associated with changes in brain volume. This is most pronounced in people who started using cannabis in adolescence, when the brain was still developing. “Cannabinoid exposure during that developmental window probably interferes with some of those normal brain development functions,” Schacht said.
Some research shows changes in the white matter of the brain in people who started using cannabis before the age of 16. White matter connects and facilitates communication among various regions of the brain. Younger users show more difficulty with cognitive tasks requiring executive function, such as inhibition control, linked to lower integrity of certain parts of white matter and higher behavioral impulsivity, said Staci Gruber, director of Marijuana Investigations for Neuroscientific Discovery at McLean Hospital in Belmont, Massachusetts, and associate professor of psychiatry at Harvard Medical School. Gruber is the study’s lead author.
In a 2026 meta-analysis of 77 studies in the journal Addiction, cannabis use was linked with reduced volume in the amygdala in particular, a region of the brain involved in processing and regulating emotions. But this study didn’t include information on when people started using the drug.
In adults ages 40 to 70 who began using cannabis after roughly 25 years of age, lifetime cannabis use is actually associated with greater brain volume, according to research published this year in the Journal of Studies on Alcohol and Drugs. That’s particularly true in areas of the brain with receptors for cannabinoids, the active compounds in cannabis that modulate things such as pain, mood and appetite. The study authors concluded this may be a sign of the “neuroprotective” benefits of cannabis in older adults, given that brain atrophy is common with age and is linked to cognitive decline and lower quality of life.
Those neuroprotective benefits could at least partly explain why cannabis use isn’t associated with dementia risk.
We need more data on how cannabis affects mood disorders
In a review in Lancet Psychiatry, researchers found no help or harm from specific cannabinoids with relation to a number of mood-related concerns, including anxiety and post-traumatic stress disorder. It also concluded there wasn’t enough data to study any potential effects on bipolar disorder or depression.
Gruber, however, noted that the study looked at either THC alone, CBD alone or a combination of THC and CBD, not the potential risks and benefits of the entire cannabis plant. (THC, or delta-9-tetrahydrocannabinol, is the psychoactive cannabinoid associated with the high caused by marijuana, while CBD, or cannabidiol, is a nonintoxicating cannabis compound.) “The idea that we would look primarily at single extracted compounds for things like anxiety is one that isn’t necessarily going to be as successful as when we look at multi-compound products,” she said. “The synergistic action of these things all together is significantly greater than the sum of its parts,” much like how sports teams are more successful with multiple players on the field.
Schacht notes that some people use cannabis as a way to mitigate symptoms without addressing the underlying cause. “As someone who has worked in addiction and substance use for a number of years, depression and anxiety are frequently reasons that people use a number of substances, such as cannabis, alcohol and nicotine,” he said. “Those drugs can be helpful in relieving those symptoms in the short term, but over the long term, I think it’s fairly clear that they are not helpful and, in some cases, actually exacerbate the problem that led people to turn to them in the first place.”
Using marijuana as a teenager or young adult is linked to a greater risk of some serious mental health problems. “People who start using cannabis when they are young and who have any kind of a family history of psychosis or severe mental illness are at risk for developing psychosis and severe mental illness themselves because of the cannabis use,” Schacht said. The greatest association with psychosis and other severe mental illnesses is also typically strongest in the heaviest cannabis users.
Ultimately, Gruber said, more studies are needed — both larger studies and those that focus on the entire cannabis plant.
And, yet, researching cannabis is challenging because it is categorized federally as a Schedule I drug, meaning that, according to the U.S. Drug Enforcement Administration, it has “no currently accepted medical use and a high potential for abuse.” The risk of abuse decreases as the schedule number gets higher. The government’s strict regulations on studying these substances limit research opportunities. “It would be so much easier if people could use those things in the laboratory, for example, but we can’t generally do that,” Schacht said.
That would also help researchers investigate whether the method of cannabis delivery matters. More research is needed to know whether smoking, vaping or oral administration make any difference in cognitive (or other) effects.
Age matters when it comes to problematic cannabis use
To many people, other Schedule I drugs such as heroin and LSD sound much more concerning. But research suggests that 22 percent to 30 percent of people who use cannabis have cannabis use disorder, a type of substance use problem.
The risk of developing cannabis use disorder is higher in people who start using marijuana in adolescence and use it frequently. “It doesn’t mean that every single person who uses cannabis at an early age is going to have a problem, but our work and the work of others demonstrates that earlier onset of recreational cannabis use, along with more frequent and higher magnitude of use, is usually associated with worse potential outcomes,” Gruber said.
To her, future research should focus on whether the potential therapeutic benefits of cannabis can be harnessed without increasing the risk of harm to improve upon current standards of care. It will take time for research to catch up to the increasing popularity of this plant, Gruber said, but that very popularity points to some benefit: “If people didn’t yield something from it, why would they keep using this?”
In the meantime, without more research, it can be challenging for some people to decide whether cannabis might benefit them. “The best thing we can hope for is good, sound, empirical data that helps to drive individuals’ decisions as opposed to hearing somebody say ‘That should never be used,’” Gruber said. If you’re concerned about a specific aspect of your brain health, such as dementia risk, and how cannabis may affect you, consider talking to your doctor before trying legal products.
Source: www.drugwatch.org
“So many times, tobacco treatment doesn’t get addressed and those with mental health conditions and substance use disorders continue to smoke at much higher rates,” explains UConn School of Social Work doctoral candidate Elizabeth “Liz” Jurczak Goldsborough. “Treating tobacco use alongside other substance use is a more holistic approach to care and can improve both quality of life and longevity of the groups that social workers serve.”
Goldsborough, who is also a predoctoral fellow in the NIH/NIDA-funded Behavioral Sciences Training in Drug Abuse Research (BST) program at New York University, focuses her research on the intersection of tobacco use and substance use treatment—an area she says is often overlooked.
Understanding the Bigger Picture
In a recent study, “Examining the bidirectional relationship between food insecurity and cigarette smoking: Evidence from a cross-lagged panel analysis,” published in the American Journal of Health Promotion, 2026, Goldsborough and her colleagues examined the relationship between food insecurity and cigarette smoking among mothers participating in the collaborative Future of Families and Child Wellbeing Study.
Their goal was to better understand a long-observed connection: does spending money on cigarettes contribute to food insecurity, or does the stress of food insecurity lead to increased smoking?
“What we found was that it’s not smoking causing food insecurity—or food insecurity causing smoking,” Goldsborough explains. “This widely observed link may instead be explained by underlying poverty, financial stress, and mental health challenges, since both depression and economic hardship affect food access and smoking behavior.”
The findings highlight a more complex reality—one in which structural factors, rather than individual choices alone, shape health outcomes.
Improving Treatment in Practice
That systems-level perspective carries into Goldsborough’s dissertation, tentatively titled “Tobacco Treatment Practices in Substance Use Care Settings: Provider and Organizational Factors.” Her research examines how treatment programs address tobacco use—an often-overlooked component of substance use care.
Despite strong evidence supporting integrated treatment, she found that tobacco care is not consistently implemented by behavioral health providers in Connecticut.
In a survey of 374 providers, more than 87% reported offering tobacco treatment at least some of the time. However, many also reported gaps in knowledge, attitudes, and confidence—factors that influence how often they provide care.
“These are things we can change,” Goldsborough says. “If we improve training, build provider confidence, and create supportive organizational policies, we can strengthen how tobacco treatment is delivered.”
She emphasizes that social work education should include competency-based tobacco treatment training, while agencies should adopt clear policies that support evidence-based care.
From Practice to Research
Goldsborough’s commitment to improving systems is rooted in her own experience. A first-generation college student, she grew up in Poland and New York City. After earning her MSW from Rutgers University, she worked as a medical social worker and later as a clinical research counselor—experiences that shaped her interest in research.
Source: https://today.uconn.edu/2026/04/the-overlooked-addiction-uconn-researcher-targets-tobacco-use-in-substance-use-care/
(Max Pemberton is a consultant psychiatrist and columnist for the Daily Mail)
Some days I wonder if I’m going mad – and you don’t need to be a psychiatrist to know that’s not a good sign. I work in a specialist NHS service for people experiencing first episode psychosis – young people at their most vulnerable, teetering on the edge of severe and enduring mental illness, some of them already sliding towards schizophrenia. Day in and day out, I watch how cannabis has destroyed people’s minds. It is, frankly, heart-breaking. So you can perhaps imagine how I feel when those same patients mention, almost in passing, that a private doctor has prescribed them cannabis. Not for cancer pain, not for the muscle spasms of multiple sclerosis, not for the intractable epilepsy of a child for whom nothing else has worked (the conditions where there is at least a credible clinical argument) but for their mental health. For depression. For anxiety.
I’m sorry, what? We are handing this stuff out on prescription for the very conditions it is known to cause and worsen. It is, and I do not use the phrase lightly, a prescription for disaster. Despite the protests of the powerful pro-cannabis lobby, it has now been proved beyond any reasonable doubt that cannabis use is directly associated with depression, anxiety, psychosis and avolition, a grinding loss of motivation that can hollow a person out completely.
Just recently I had a patient who had a history of psychosis. She’d been watching TikTok and become convinced that cannabis was the answer to her ADHD. A private clinic had given her a prescription without checking her notes, without calling me, and without calling her GP. It came out only by chance, in conversation. I sat there absorbing this information, thinking: a private doctor has prescribed her a powerful drug that is directly contraindicated for her condition, without contacting a single one of the clinicians actually responsible for her care. How is this right?
The latest figures, published in the Times, should alarm anyone who cares about how medicine in this country is practised. Since cannabis was legalised for medical use, just ten private doctors have signed off more than half of all cannabis-based prescriptions in the country. Ten doctors. One consultant alone accounted for one in every ten prescriptions nationwide, getting through nearly 46,000 in the first five months of last year. Do the arithmetic and that works out at roughly one every two working minutes. I’ll leave you to draw your own conclusions about how rigorous those consultations could possibly have been.
To understand how we’ve ended up here, it’s worth remembering that the story of medical cannabis in this country started in a genuinely sympathetic place. In 2018 the government legalised cannabis-based medicines following the case of Billy Caldwell, a severely epileptic child experiencing hundreds of seizures a day, for whom cannabis had worked when almost everything else had failed. The public outrage when his medication was confiscated at the border was entirely justified, and it was right to change the law. Cannabis does have legitimate medical uses for certain rare epilepsies, for chronic pain, and for patients who have exhausted every other option. Nobody sensible disputes this. What nobody could have anticipated was quite how rapidly and recklessly that door would be shoved open. Many doctors said so at the time, of course. When the law changed in 2018, there were plenty of voices in the medical profession warning that this was the thin end of the wedge; that however carefully the legislation was drafted, a private market would find ways to exploit it, that the definition of clinical need would be stretched until it was meaningless, and that the result would be cannabis available on medical prescription to more or less anyone who wanted it. Those concerns were dismissed as scaremongering. They were, it turns out, entirely justified. You can now claim some suitably vague condition, sit through a brief online consultation, and walk away with a prescription for cannabis at a potency you would struggle to obtain from the finest drug dealer in the country. The word ‘medical’ does a great deal of heavy lifting in all of this.
The prescription numbers tell the story. From a standing start in 2018, monthly figures climbed slowly at first, then accelerated sharply, reaching around 10,000 a month by mid-2022 and surging to nearly 100,000 a month by early 2025. Almost none of this growth has been driven by epilepsy or chronic pain. At Mamedica, one of the largest private cannabis clinics in the country, over half of its 12,000 patients are being prescribed cannabis for psychiatric conditions. (Mamedica says that cannabis treatment can be ‘game changing’ for these patients and has led to improvements in mood, hope and functioning. Its CEO says that ‘At Mamedica, every patient undergoes full clinical assessment, shared decision-making and ongoing monitoring under strict governance. This is structured, accountable medicine, not volume prescribing.’)
Professor Sir Robin Murray of King’s College London, who has spent his career studying the catastrophic relationship between cannabis and psychosis, has been watching all of this with undisguised alarm. He has warned bluntly that certain private clinics are ‘causing harm to the people they are claiming to help’. But it’s another observation of his that really cuts to the heart of the matter. ‘Usually,’ he has pointed out, ‘if a person has a medical condition, they see a doctor who specialises in a particular area of medicine, for example, respiratory or kidney disease. After diagnosis, the doctor prescribes from a range of treatments’. That, of course, is how medicine is supposed to work. A condition is identified, an appropriate specialist assesses it, and a treatment is chosen on the basis of evidence. What is happening in these clinics is the precise opposite: the treatment comes first, the condition barely matters, and the evidence is nowhere to be seen.
A quarter of psychosis cases in South London were associated with skunk, according to Murray’s research at the Institute of Psychiatry. Oxford University has shown it raises the risk of depression in teenagers by 40 per cent. None of this is seriously contested, it is settled science. Last month a major review in the Lancet Psychiatry screened nearly 6,000 studies and found that cannabinoids showed no significant benefit for anxiety, PTSD, psychotic disorders or OCD. For depression – the single most common reason cited for prescription across most legalised markets – there were no randomised controlled trials to look at. None at all. Not a thin evidence base. No evidence base whatsoever. And still these prescriptions keep on coming.
Then there is the question of what, exactly, is being prescribed, because it is emphatically not the careful, pharmaceutical-grade product the word ‘medical’ implies. Many of these prescriptions are for high-potency products with THC content exceeding 30 per cent. One strain, cheerfully named Space Cake, clocks in at 34 per cent THC. Street skunk – the very stuff Sir Robin Murray and colleagues have spent years linking to psychosis – typically contains between 14 and 16 per cent. So we are prescribing considerably stronger products to people who are already mentally unwell, with no credible evidence that it does them any good. If this were happening with any other substance, there would be a public inquiry.
Make no mistake, the human cost of all this is not abstract. Oliver Robinson was 34 years old, a former property developer from Bury in Greater Manchester. He had been struggling with depression, bipolar disorder and anxiety, and was already under the care of NHS and Priory psychiatrists, both of whom were strongly opposed to him using cannabis, when he turned to a private clinic. A video consultation with Curaleaf was all it took. The clinic based its decision on a GP summary that was nine months out of date. It never contacted his other treating psychiatrists. It prescribed him cannabis. What followed was 18 months of deterioration as his dependency took hold, eventually costing him a £1,000 a month, until he could bear it no longer and was found dead at his home in November 2023.
The inquest, concluded in January this year, made for grim reading. Coroner Catherine McKenna ruled that the prescription had ‘probably contributed to his death’ and had ‘acted as an obstacle’ to him receiving appropriate psychiatric care, giving the drug, in her words, a sense of legitimacy that made it harder for him to engage with the clinicians who were actually trying to help him. She issued a Regulation 28 Prevention of future deaths report to Curaleaf, finding that the prescribing doctor was a children’s and adolescent psychiatrist with no experience of treating adults with Oliver’s complex presentation. His brother Alexander said afterwards that he believed profit had been prioritised over his brother’s life. It is thought to be the first time a coroner has formally linked a private cannabis prescription to a patient’s death. It will not, I fear, be the last. Sir Robin Murray, responding to the verdict, was characteristically direct. These clinics, he said, are ‘nothing more than drug dealers for the middle classes’. Some clinics seem almost proud of how easy they make it to get a prescription. The industry, when challenged, responds with the usual blizzard of patient testimonials and wellness language, insisting people have every right to try whatever they believe is helping them. Let’s be honest about what this is: it’s retail with a prescription pad.
Of course, cannabis has over the past decade acquired a sort of halo. It became the anti-establishment option, the natural remedy, the thing your GP would never prescribe because of Big Pharma and vested interests and all the rest of it. It has latched onto the broader conversation about mental health in the same way recreational ketamine has managed to: cynically and with considerable commercial savvy. The moment it put on a white coat, a great deal of critical thinking went out of the window.
To its credit, the NHS has stayed sceptical. There are only around 5,000 NHS prescriptions for licensed cannabis medicines each year, limited to conditions with genuine evidence behind them, and Nice has declined to recommend it for the vast majority of conditions the private clinics are happily treating. So the private market has simply flourished in the gap, turning NHS caution into a marketing opportunity and positioning itself as the enlightened alternative to a stuffy, out-of-touch establishment. It’s a cynical trick and it has worked spectacularly.
I’ve sat with families trying to make sense of how their bright, funny, perfectly healthy child ended up psychotic. I’ve watched patients who started smoking skunk as teenagers and never quite came back. And now I find myself watching those same patients – or patients just like them – being sent home with a prescription for something considerably stronger than what broke them in the first place, signed off by a doctor churning out one every two working minutes. It’s utter madness. It really is.
SOURCE: https://spectator.com/article/the-madness-of-using-cannabis-to-treat-mental-health/
 United Nations – Office on Drugs and Crime Country Office in Afghanistan
United Nations – Office on Drugs and Crime Country Office in AfghanistanCombining love and boundaries in my parenting, and guiding my child with care, not with punishment, are the most valuable lessons I learned in just three days of the Strong Families Programme.
My name is Roya*, and two months ago, I joined the Strong Families Programme, where we learned practical lessons about positive parenting, stress management, and understanding our children’s emotions. I especially enjoyed the calm breathing exercise, a simple practice to bring peace and relaxation. Sharing family challenges with other mothers made me realize that I am not alone and that together we can stay strong and support one another.
This new understanding has changed my relationship with my daughter. I realized this when one day I couldn’t afford to buy her a new school bag. In the past, she might have cried or shouted, but this time she stayed calm and said, “Mother, I will go to school with the same bag this year.”
Her reaction touched me deeply and showed how much she has learned. This new understanding between us is priceless and gives me a feeling of peace and pride as a mother. It makes me confident that she will go out and make healthy decisions in her life. I believe more families should have the chance to join programmes like Strong Families. Many parents face stress and family problems, and this programme shows simple ways to build healthier children’s behavior and a happier, more peaceful home.
Through funding support by the Republic of Korea, UNODC successfully scaled up the global Strong Families Program (SFP) (A family skills drug use prevention programme for families living in stressful and challenged settings) in Kabul and Nangarhar provinces, adapted to the Afghan context and reaching 180 highly vulnerable families from low-resource, internally displaced, poppy-farming communities.
Through structured sessions, participating families gained practical skills to manage stress, strengthen parenting practices, prevent violence, and foster positive, age-appropriate family dynamics. As a result, the intervention led to improved emotional well-being, stronger caregiver-child relationships, and enhanced household resilience, all of which are protective factors against drug use initiation.
These achievements are expected to directly contribute to national drug prevention priorities and integrated into broader family support and drug prevention initiatives, ensuring long-term sustainability and wider impact.
Source: https://www.unodc.org/coafg/en/stories/2026/strong-families-porgramme-a-family-based-drug-use-prevention-intervention-helping-mothers-to-have-a-strong-bonding-with-their-children.html
“Rhino tranq” is an emerging, highly-risky street drug. It’s a mix of fentanyl with the animal tranquilizer medetomidine.
“Can be dangerous when people use it, because it can increase the rate of overdose, it can increase the rate of low blood pressure and other cardiovascular complications,” said Dr. Brian Hurley, the medical director of substance abuse prevention and control with the L.A. County Department of Public Health.
He compared it to “tranq,” which is a combination of fentanyl and another veterinary relaxant called xylazine. Hurley said medetomidine, which is found in ‘rhino tranq,’ is far more dangerous.
“Medetomidine is actually more potent than xylazine is, and they both seem to be associated with increased risk of overdose,” Hurley said.
The CDC issued a new warning to health care professionals on Thursday. Medetomidine, which is also known as “mede” or “dex,” is being picked up in seized drugs and wastewater samples. The highest concentration is in the Northeast.
“So it’s not present here at the same degree that is present in other cities on the East Coast, like Philadelphia,” Hurley said. “At the same time, we do think it’s important that the public and the medical providers here in Los Angeles be aware that medetomidine is here.”
He said when people experience a fentanyl overdose with medetomidine, they don’t respond effectively to the opioid reversal drug naloxone.
“Naloxone doesn’t address medetomidine intoxication, nor does it touch medetomidine withdrawal. So, that’s why people will need other supportive care,” Hurley said.
Overall in L.A. County, fentanyl-related deaths have dropped 37% in 2024 compared to 2023. But far too many overdoses are still happening and Hurley said people need to know “rhino tranq” is out there.
“The safest thing is to not use drugs, but if somebody is thinking about using, never use a loan, have naloxone on hand, and consider using test strips to look at what’s in the drug supply,” he said.
He said the county provides free fentanyl testing strips through their community health stations located at various schools, hotels and churches. You can see those locations on their website.
According to the Drug Policy Alliance, overdose deaths are decreasing most in places where harm reduction practices are at work.
Dasgupta is a scientist studying drug overdose deaths at the University of North Carolina, Chapel Hill.
Use-prevention efforts such as honest school-based awareness programs, prescription drug monitoring programs, improved access to affordable mental healthcare, even data collection efforts that help guide the conversation — it all helps.
For that matter, access to affordable healthcare in general — particularly in a state that relies so much on physical laborers who face the risk of injury and chronic physical pain daily — is essential. Even better if alternative means of pain management are encouraged rather than squashed.
But perhaps one of the least considered when there is so much lower-hanging fruit for politicians are the “deaths of despair,” and the role hopelessness and dismal economic prospects have played in this plague. Deep generational poverty, socio-cultural assumptions about both education/job training AND substance use, and the perpetual failure to bring any momentum to the expansion and diversification of our economy have been crippling.
As the abstract for one Marshall University study on “The opioid epidemic: Effects on recidivism in West Virginia,” put it, “the opioid epidemic was just a by-product of a much larger issue found in West Virginia.”
Now, tens of millions of dollars have been distributed across the state in the early stages of the West Virginia First Foundation’s mission of “Empowering West Virginians to prevent substance use disorder, support recovery, and save lives.”
According to Chairman Greg Duckworth, “These investments are not just funding grants, they are strengthening an ecosystem. We are supporting foster families, peer recovery networks, workforce pipelines, diversion strategies, wraparound youth services, and the long-term capacity needed to change outcomes for generations.”
Here’s hoping the goal is that one day the foundation will run out of money after having completed its mission and happily close up shop.
But until that day, no one can let what looks like success over the course of one year lull them into letting off the gas. We’re not even out of the driveway.
Source: https://www.newsandsentinel.com/opinion/local-columns/2026/03/editors-notes-harm-reduction-effort-working/
|
Forwarded by Maggie Petito – From UK Spectator – February 23, 2026
The truth about Mexico’s cartel wars
Spectator UK – February 23, 2026 by Joshua Treviño. (Treviño is the chief transformation officer at the Texas Public Policy Foundation and a senior fellow of the Western Hemisphere Initiative at the America First Policy Institute).
To understand the latest disturbing spasm of violence in Mexico, it helps to go back six years to an ultra-wealthy colonia called Lomas de Chapultepec, near the heart of Mexico City.
Lomas de Chapultepec is protected, partly by a large security apparatus net that has been thrown around it, and partly by the pacto de narco, which protects the high-income neighborhoods in which both cartel leadership and their political partners live, along with their families.
Not long ago, former Mexican president Andres Manuel Lopez Obrador was publicly threatening to use the Mexican armed forces to defend cartels
That was why it was surprising when, on June 26, 2020, Mexico City’s chief of police Omar Garcia Harfuch was attacked on the Paseo de la Reforma by a hit squad armed with heavy-caliber weaponry. Wounded, he escaped with his life, although two accompanying policemen did not.
This shocking eruption of military-grade violence inside Mexico City’s wealthiest colonia was swiftly attributed to the bloodthirsty and sociopathic leader of the Cártel de Jalisco Nueva Generación (CJNG), Nemesio Rubén Oseguera Cervantes: the man known as El Mencho.
Yesterday, Omar Garcia Harfuch – who is now Mexico’s Secretary of Security and Citizen Protection – struck back. El Mencho failed to kill him, therefore he has killed El Mencho.
The Mexican state’s account of events holds that El Mencho and his men attacked the force sent to arrest him, and that the CJNG boss died of wounds en route to treatment. Mexico also said that the United States forces provided intelligence and unspecified support to the Mexican effort, without any presence on the scene. One may or may not believe this. Those in the know are not issuing the press statements.
What’s clear is that the targeting of El Mencho was meant to address and appease two mutually antagonistic parties. One is the Americans, who demand ever-greater deliverables from the Mexican state in the cartel wars. The other is the ideological core of Mexico’s ruling Morena party, which is fundamentally anti-American and would react to a US presence with something close to revolt. It was not so very long ago – the spring of 2023, in fact – that the creator and central figure of Morena, former Mexican president Andres Manuel Lopez Obrador, was publicly threatening to use the Mexican armed forces to defend cartels against any American action against them.
If his successor, current Mexican President Claudia Sheinbaum, has allowed direct American action now, it is an epochal break with her own benefactor who bestowed the office upon her. As things stand, the effort to both claim and disclaim American involvement carries a sense of protesting too much.
Two consequences of the hit now present themselves. The first and most-dramatic is the spasm of violence across much of Mexico, including well-known tourist areas. CJNG personnel are swarming into areas previously considered off-limits to the cartel wars. The organization that violated the peace of Lomas de Chapultepec is now doing the same to international airports, to Puerta Vallarta, to Guadalajara and beyond.
The actions appear to be comparable to those one might expect of heavy infantry units, equipped with anti-armor and anti-aircraft weaponry. The Mexican armed forces, clearly caught off guard, are slowly responding. But the reaction ought not to have been a surprise: in the Culiacanazo of October 2019, Sinaloa-cartel militia conducted a similar operation after an arrest of one of El Chapo’s sons. This is a known organizational response by major cartels when challenged by the state, and the state’s unreadiness can be explained by plain incompetence – or by an inability to trust the broader security apparatus with news of the impending raid.
As the fighting progresses, watch the speed at which the Mexican armed forces reassert control, as they likely will. Well-armed as CJNG and the major cartels are, the strongest force in the country remains the formal state. If the matter becomes pressing, America could offer intelligence and targeting assistance – none of which will become public knowledge.
Watch also the extent to which CJNG chooses to exact vengeance upon any of the several million US citizens in Mexico, now that the Mexican state has given the Americans partial credit for El Mencho’s death. The targeting of American citizens as such would of necessity draw in the direct and public involvement of the United States.
Various members of the Mexican and American establishments are proclaiming that the death of El Mencho is proof that the Mexican regime is, at long last, serious in its fight against the cartels. This is slightly naive. The traditional cartel partner of the Morena regime is the Sinaloa cartel, which, although presently in violent flux, has a perennial and bloody rivalry with CJNG.
The Mexican state will continue to offer up big-name cartel figures ad infinitum, but their elimination alone changes little. What would be transformative is bringing to account the politicians who enable, protect and promote cartels. These men are at the very heart of Mexico’s Morena regime. That is what a true strategic win would look like, and it is what the United States must resolutely pursue.
Source: www.drugwatch.org

Ms. B (identified by first initial of last name for privacy) had never told anyone about the sexual abuse she had suffered at the hands of her uncle as a young child. For years during her adolescence, the secret festered, driving her to run away from home, drop out of school, and begin drinking and taking opioids to numb the pain.
It wasn’t until she was sitting in a brightly lit room with other women at the clinic where she had started treatment for her opioid use disorder, surrounded by rainbow-colored positive affirmations, drinking a cup of hot coffee, and laughing at a joke the peer specialist had just told, that she felt safe enough to start telling her story.
Substance Abuse and Mental Health Services Administration (SAMHSA) grant funds had paid for the affirmation signs, the coffee, and the salary for the peer specialist. Ms. B was one of many women that year who benefitted from this care designed specifically to address the trauma that contributed to the development of their substance use disorders. And it was working.
Yet on January 13, that progress for Ms. B and many others was threatened. With no announcement or reasoning, the federal government abruptly cut $2 billion in already awarded grants to SAMHSA—an agency likely unfamiliar to most Americans, but one that undergirds and forms the safety net for the country’s behavioral health system. There was no warning for an agency already cut by $1 billion last year, hit with significant staff reductions, and poised to be subsumed under a new proposed entity, the Administration for a Healthy America, within the Department of Health and Human Services (HHS). Programs across the country were zeroed out overnight. Only after intense public outcry did the administration reverse course.
In early February, Congress passed bipartisan appropriations to preserve SAMHSA’s structure and funding, clearly signaling the little agency and its work is essential to the nation’s behavioral health system. This is welcome relief to the uncertainty just weeks ago. Adding to a recent focus on behavioral health, President Trump issued a related Executive Order, Addressing Addiction Through the Great American Recovery Initiative, on January 29. This order establishes a new interagency taskforce to provide recommendations and guidance for better coordination and alignment of relevant federal programs. On February 2, HHS Secretary Kennedy announced a new $100 million SAMHSA grant program, the Safety Through Recovery, Engagement, and Evidence-based Treatment and Supports, or STREETS Initiative, to fund outreach, mental health care, medical stabilization, crisis intervention, and linkages to housing for people experiencing homelessness and addiction.
These are welcome, if unclear, actions, and they come on the heels of the whiplash caused by mass grant cancellation and reversal—a terrifying stress test that exposed just how fragile America’s behavioral health infrastructure has become.
This is juxtaposed with recent data from the Centers for Disease Control and Prevention that demonstrated another remarkable and welcome increase in life expectancy in America on the heels of reductions in overdose mortality. However, much of the federal infrastructure that contributed to this progress was nearly dismantled overnight.
What happened in mid-January reveals a deeper misunderstanding of how behavioral health care actually works in America, and why weakening SAMHSA puts lives at risk.
Despite progress, substance-related conditions, including accidents and unintentional injuries, and suicides remain among leading causes of death for people ages 25–64 in the United States. Millions of Americans continue to struggle with untreated or inadequately treated substance use disorders and mental illness. And communities everywhere—urban, rural, tribal—are grappling with shortages of trained providers, fragmented systems, and rising demand for services.
SAMHSA is the only federal public health agency whose sole mission is to address the full continuum of behavioral health needs—from prevention to treatment to supporting individuals in recovery. Its work does not replace direct clinical care. It often funds services that fall outside of traditional insurance models yet exist as glue in a system.
Take overdoses, for instance. SAMHSA funding has enabled states to saturate their communities with naloxone, a life-saving overdose reversal medication. SAMHSA investments have supported training for first responders and community organizations on how to recognize and respond to overdose. These investments are not abstract. They show up in emergency departments, resulting in fewer fatal overdoses, and in communities where people survive long enough because of SAMHSA funding to engage with treatment and sustain recovery.
As former career federal officials at SAMHSA and as physicians who continue to see patients, we’ve seen the agency’s work and impacts firsthand at the individual, family, and community levels. We’ve also seen how the programmatic expertise SAMHSA brings has helped other federal agencies make major systems level changes; examples include 1) the Drug Enforcement Administration’s regulatory flexibilities allowing for telehealth initiation of buprenorphine for the treatment of opioid use disorder, and 2) the Centers for Medicare & Medicaid Services promulgating a new billing code for peer support services in the 2024 Physician Fee Schedule. SAMHSA’s unique focus on the behavioral health needs of the country is what makes its role and work so special.
SAMHSA also recognizes that the work of saving lives and improving behavioral health wellbeing is done on the ground by trained and knowledgeable individuals. Few federal agencies other than SAMHSA fund the ongoing training and technical assistance needed to make sure the public health, public safety, and health care professionals serving people with, or at risk for, behavioral health conditions are up on the latest research and best practices. For example, grant programs such as the Addiction and Prevention Technology Transfer Centers, Center for Mental Health Implementation Support, and Opioid Response Network have provided cutting-edge support to thousands of public health and health care professionals, first responders and other public safety officials, state level professionals, and policymakers.
Many of these services and training/technical assistance grants were on the chopping block just a few weeks ago. Even though the cuts were ultimately restored, the whiplash furthered an unnerving sense of instability that began in spring 2025 with Secretary Kennedy’s announcement of a planned new Administration for a Healthy America that would comprise SAMHSA and several other HHS operating divisions. Collectively, these actions have undermined workforce morale, disrupted planning, and eroded trust in the federal government being a reliable partner. The grant funds were restored; the trust was not.
The next question is what happens now that the fiscal year funding has passed.
Appropriations language alone does not ensure implementation. Take, for instance, the prior massive workforce reductions at the agency and the sudden $1 billion cut last year that required 23 states and the District of Columbia to file suit and obtain injunctions to continue the flow of funding. Most recently, on January 23, $5 billion in essential public health infrastructure funding by CDC to local health departments around the country was suddenly paused and then “unpaused” 24 hours later; these dollars were also appropriated by Congress. And a recent article in Health Affairs Forefront found that SAMHSA had spent only 34.6 percent of its FY 2025 budget allocation, based on a review of USAspending.gov accounts.
Congress must exercise sustained oversight to ensure the administration fully executes on the will of Congress, that grants are reliably administered, and that the workforce and technical assistance infrastructure are rebuilt rather than quietly hollowed out. Such robust oversight and accountability functions have been lacking. Thus, it will be important for SAMHSA grantees, state behavioral health administrators, family members, and others with a vested interest to raise issues and concerns with their Congressional representatives regularly and urgently when there are future drastic changes to funding and programs. Ensuring that individuals, families, and communities impacted by substance use get the help they need is a bipartisan concern.
We also need hearings on what has happened, as well as Office of Inspector General and Government Accountability Office reports on the work SAMHSA and related agencies are doing and where they are falling short. We need active engagement with Congressional representatives where these dollars are awarded (and that’s every state and territory in the United States) to ensure that the money allocated is being disbursed by the government and reaching the communities it is intended to serve. The lesson of January is that sustained advocacy works, but vigilance is required to ensure follow-through on Congressional intent for appropriated funding.
SAMHSA may be little known to the general public, but its work touches millions of lives. Weakening it when the nation is finally turning the corner on the overdose crisis is a risk we cannot afford to take. Saving it once is not enough; ensuring its stability is the next test. Ultimately, the measure of our national commitment will be whether Congress secures long-term stability for SAMHSA.
Ms. B found her voice in a room funded by a government grant. We must ensure that those healing spaces continue to exist, the lights are still on, and the peer specialist is still employed when the next person walks through the door seeking help.
Manatt Health works with a diverse group of clients, including states; state and federal policy makers and agencies; payers; health care providers and systems; foundations; associations; consumer organizations; and pharmaceutical, biotech, and device companies.
Dr. Olsen is a member of the American Society for Addiction Medicine (ASAM), serves on an ASAM Criteria Implementation Committee, and has a small clinical advisory role with them.
Source: https://www.healthaffairs.org/content/forefront/congress-has-preserved-substance-abuse-and-mental-health-services-administration-samhsa
Adolescents who use cannabis could face a significantly higher risk of developing serious psychiatric disorders by young adulthood, according to a large new study published today in JAMA Health Forum. The longitudinal study followed 463,396 adolescents ages 13 to 17 through age 26 and found that past-year cannabis use during adolescence was associated with a significantly higher risk of incident psychotic (doubled), bipolar (doubled), depressive and anxiety disorders. The study was conducted by researchers from Kaiser Permanente, the Public Health Institute’s Getting it Right from the Start, the University of California, San Francisco and the University of Southern California, and was funded by a grant from NIH’s National Institute on Drug Abuse (R01DA0531920).
The study analyzed electronic health record data from routine pediatric visits between 2016 and 2023. Cannabis use preceded psychiatric diagnoses by an average of 1.7 to 2.3 years. The study’s longitudinal design strengthens evidence that adolescent cannabis exposure is a potential risk factor for developing mental illness.
“As cannabis becomes more potent and aggressively marketed, this study indicates that adolescent cannabis use is associated with double the risk of incident psychotic and bipolar disorders, two of the most serious mental health conditions,” said Lynn Silver, M.D., program director of the Getting it Right from the Start, a program of the Public Health Institute, and a study co-author.
Cannabis is the most used illicit drug among U.S. adolescents. The Monitoring the Future study shows use rising with grade level — from about 8% in 8th grade to 26% in 12th grade — and according to the 2024 National Survey on Drug Use and Health, more than 10% of all U.S. teens aged 12 to 17 report past-year use. At the same time, average THC levels in California cannabis flower now exceed 20%, far higher than in previous decades, and concentrates can exceed 95% THC.
Unlike many prior studies, the research examined any self-reported past-year cannabis use, with universal screening of teens during standard pediatric care, rather than focusing only on heavy use or cannabis use disorder.
“Even after accounting for prior mental health conditions and other substance use, adolescents who reported cannabis use had a substantially higher risk of developing psychiatric disorders — particularly psychotic and bipolar disorders,” said Kelly Young-Wolff, Ph.D., lead author of the study and senior research scientist at the Kaiser Permanente Division of Research.
The study also found that cannabis use was more common among adolescents enrolled in Medicaid and those living in more socioeconomically deprived neighborhoods, raising concerns that expanding cannabis commercialization could exacerbate existing mental health disparities.
SOURCE: https://www.phi.org/press/study-adolescent-cannabis-use-linked-to-doubling-risk-of-psychotic-and-bipolar-disorders/
###
A 9-year-old boy in Washington lives in a tent with his fentanyl-addicted parents. He waits outside in the bushes while his mother exchanges sex for money and drugs. He doesn’t attend school or see a doctor. He appears underweight and ill.
Repeated offers of assistance — including housing — from social workers are refused by his parents. Now what?
The state’s answer is clear: the child protection system (CPS) will do nothing to protect this child because homelessness and drug use are “not neglect.”
Chronic drug use is increasingly seen as something that can be managed alongside caring for children, even medically fragile newborns. Parents in Oregon are encouraged to ask for naloxone (Narcan) without fear of stigma so that they can revive their children if their drug supply is inadvertently ingested. Lock boxes are recommended or distributed by CPS and other public agencies, often under the pretext of preventing accidental ingestions of prescription fentanyl, legal cannabis or other medications. America’s Poison Centers reminds adults who use fentanyl that naloxone can be safely used on children.
At a recent national forum, a former New Mexico state legislator described how CPS safety plans often ask parents to please dispose of their foils and clean their spoons before their children return home from school or child care. Parents in Arizona, Connecticut, Illinois, New Mexico, New York and Texas (to name just a few) are led — consistent with CAPTA-funded federal trainings and guidance — to believe that despite their addiction, they are capable of implementing “safety plans” alongside continued use of their drug of choice.
In a growing number of jurisdictions, CPS agencies tell doctors they do not have to report a parent or newborn’s positive drug test, while telling other community members that an active substance use disorder is not a basis for investigating whether a child has been harmed or endangered.
Parent advocates who argue that “drug tests are not parenting tests” seem to have convinced child welfare leaders across the political spectrum that, even though it is illegal to drive a car while intoxicated, parenting under the influence should not evoke similar concerns. Even the federally funded National Center on Substance Abuse and Child Welfare discourages the use of drug testing to inform whether it is safe to retain young children in the home: “The punitive use of drug testing can inhibit recovery and prove harmful to families,” noting also that “drug tests can perpetuate stigma about substance use disorders.”
These practices fall under the umbrella of harm reduction. Harm reduction is a normative framework that “centers the lived and living experience of people who use drugs” and focuses on “minimizing the negative consequences associated with substance use without requiring abstinence.” Influential groups such as the Drug Policy Alliance describe harm reduction as “simply common-sense safety,” no different than “seatbelts, bike helmets, sunscreen, or flu shots.” The Harm Reduction Coalition describes a “movement for social justice built on a belief in, and respect for, the rights of people who use drugs.”
Under this framework, we are obligated to assume that people who use drugs “know their own bodies” and “are capable of making rational choices”; the assertion that drug use poses a danger to children or that treatment must be mandated is stigmatizing and therefore counterproductive.
These harm reduction strategies focus on reducing harms to adults who use drugs, not on safeguarding children who may be endangered by parental substance use.
Prioritizing expressed preferences of the parent to continue their drug use over the long-term health and safety of both parents and children has foreseeable consequences. In 2023 in Westchester County, New York, an early term, jittery, cocaine-positive newborn was deemed “unaffected” by substance exposure and released to her parents. Despite several subsequent calls to CPS about the parents using heroin and other drugs while caring for the child, the subsequent birth of a drug-exposed sibling, and parents’ nonparticipation in voluntary services, agency lawyers prevented caseworkers from petitioning for court intervention because there was “no impact” on the child.
The infant girl died of drug ingestion shortly after caseworkers requested to petition the court and were denied — for the third time. The parents were charged with manslaughter.
Some may argue that the cases of the 9-year old in Washington and this Westchester infant reflect aberrations in practice, and that taking these failures seriously will inevitably lead to unnecessary removals. Yet, statements from agency personnel rationalizing their decisions not to intervene reveal a consistent logic.
Prior advocacy sought — reasonably — to ensure that CPS approached addiction as a chronic disease in need of treatment rather than a character flaw. Now, the message is that parents’ untreated addiction is not the business of CPS. Empowered with pieces of paper listing possible services, and legally unenforceable safety plans, parents are left to figure it out on their own. Even recent federal efforts to expand access to medication-assisted treatment may be read as a signal that getting parents to begin medication is enough — and that CPS need not remain involved — despite high rates of discontinuation, relapse, overdose and concurrent use of other illicit drugs.
No one is suggesting that a single positive drug test or instance of drug use should automatically trigger the removal of children from the home. But we must abandon the delusion that parents who are drug-addicted will enter treatment voluntarily before serious harm falls to them or their children, or have the capacity to make their addiction safe and inconsequential while parenting. Such beliefs are contradicted by the neuroscience of addiction, the massive death count of the opioid epidemic, and piles of research and personal accounts documenting what happens to children reared by parents with active drug addictions.
Let’s be honest. The same people defending this hands-off approach would be terrified to have their own children spend five seconds in a tent full of fentanyl and strange men soliciting sex — much less live there indefinitely. This is a classic example of luxury beliefs — the privileged gain status by espousing tolerance of harmful environments and behaviors, while they and their loved ones remain fully insulated from the consequences. In the understandable desire to avoid being punitive about the struggles of drug addiction, we have perhaps forgotten that there are worse things than parents being coerced into drug treatment or experiencing a temporary separation from their child. As Pennsylvania child protection advocate Cathleen Palm observed, “There is nothing more punishing than a dead baby and a prosecuted mom.”
by Shane Varcoe – Feb 17, 2026
Every day in Australia, we lose nine people to suicide. The connection between substance use, mental health, and suicide is undeniable – trauma drives people to self-medicate, substance use deepens isolation and depression, and what starts as numbing pain can end in taking one’s life. Yet research shows us something remarkable: the vast majority of people contemplating suicide don’t actually want to die. They just want the suffering to stop. And that’s where intervention can change everything.
In this context, I spoke with Rob Nicholls and Jenny Nicholls, a couple whose personal journey through trauma and substance use has equipped them to train ordinary Australians to recognise the signs and save lives. Rob is an ASIST Trainer with Living Works, the world’s leading suicide prevention organisation, and Jenny is the author of Shattering Deception and Revealing Truth, a powerful memoir of her journey through childhood abuse, trauma, and the destructive coping mechanisms that followed.
Shattering Deceptions & Revealing Truth – Seeking a Healthy Out from Trauma – A Conversation with Suicide Preventionists
Jenny grew up in a home marked by her mother’s occult involvement, alcoholism, drug use and violence. Rob’s early years were shaped by party culture and alcohol as a social lubricant. Both understand firsthand how substance use becomes an escape from pain, how trauma creates patterns of self-medication, and how exclusion – whether through disability, mental illness, or addiction – increases suicide risk. The constant hypervigilance from Jenny’s childhood created patterns of anxiety that eventually led to her own suicide attempts.
Key Takeaways:

Shattering Deception and Revealing Truth by Jenny Nicholls shares her lived experience of childhood trauma, substance use, suicide struggles, and her journey toward healing and recovery.
Source: Shane Varcoe – Executive Director for the Dalgarno Institute
Forwarded by Maggie Petito (Drug watch International)
Article by London Telegraph – Sarah Newey – Global health security correspondent – 17 February 2026
“Chinese triads, Mexican cartels and Australian biker gangs are all operating, even collaborating, in a “thriving criminal ecosystem” that exploits the region’s porous coastlines, weak law enforcement and widespread corruption. Yachts, narco-subs and drones have all been used across the network of air and maritime routes.”
Fiji’s spiralling health crisis is linked to an explosion in methamphetamine that threatens to turn the Pacific into a ‘semi-narco region’
Ben took his drugs ‘on the rocks’. Instead of diluting the methamphetamine with water, he’d draw blood into a syringe, dissolve the crystals, and inject himself. Sometimes it was his blood, sometimes a friend’s, and the needle was rarely new. That hardly seemed to matter.
It was 2021 and Ben, whose name has been changed, was living on the streets in Suva – Fiji’s faded seaside capital. Then 20, he’d fled his home after his father and five brothers tried to beat away his bisexuality. Crystal meth’s numbing high became an all-consuming escape from the painful memories. “I just felt like the love I was looking for was in the streets, it was not at home,” Ben, now a tall, measured 24-year-old, told the Telegraph. “I didn’t consider [safety] at all… I just continued taking [meth]. For me, when I took drugs, it transformed my mind – I was in another world altogether.”
But that world of euphoric highs and shared syringes left its mark long after Ben abandoned Suva’s shabby streets.
By late 2023, he had developed a persistent cough, his hair was falling out, and he was losing weight rapidly – dropping from a waist size 42 to just 22. When he was hospitalised with severe pneumonia, doctors diagnosed Ben with late-stage HIV, then transferred him to a ward notorious in Fiji as the place men go to die. “That’s how ill I was,” he said, sipping Coca-Cola on the seafront earlier this month. “Lying in that bed with no hope, everything seemed lost and fading.”
As recently as 2020, stories like this were relatively rare in Fiji, a former British colony best known as a paradise archipelago with pristine beaches and a vibrant culture. But now, the small Pacific nation has a grim new accolade: it is struggling to stem the world’s fastest growing HIV outbreak. “This is the ugly side of Fiji,” said Paulo, another of the five people living with HIV who spoke to the Telegraph in Suva – where children as young as 10 have contracted the virus from injecting drugs, as HIV rips through a country caught off guard.
According to data shared by the Ministry of Health, 147 people were newly diagnosed with the disease in 2020. Just four years later, that number had jumped to 1,583 – and in the first six months of 2025 alone, 1,226 cases were reported. Overall, infections have risen by 3,000 per cent since 2010.
While still a relatively small total compared to Fiji’s population – roughly 930,000 people – patchy testing means diagnosed cases are only the tip of the iceberg. And the trajectory of the outbreak looks ominous: the health department estimates that, without urgent interventions, the country could see 25,000 cases a year by 2029.
“I never thought I’d see another epidemic like this in my lifetime,” said Prof Lisa Maher, an epidemiologist at the Kirby Institute in Sydney, who worked on the HIV response in New York in the 1980s and later in southeast Asia, and is now supporting Fiji. “It came out of nowhere, because there was no data and no surveillance in place.”
‘A thriving criminal ecosystem’
The escalating crisis is linked to a boom in drugs that threatens to turn the Pacific into a “semi-narco region”, according to Associate Professor Jose Sousa-Santos, director of the Pacific Regional Security Hub at the University of Canterbury in New Zealand.
The region has long been a strategic stop-off point on a ‘drugs superhighway’ from the Americas and southeast Asia to Australia and New Zealand, where high demand and prices equate to lucrative profits. Yet the route’s popularity is increasing, with organised crime in the Pacific “evolving faster than any previous point in history”, according to a report from the United Nations Office on Drugs and Crime (UNODC).
Chinese triads, Mexican cartels and Australian biker gangs are all operating, even collaborating, in a “thriving criminal ecosystem” that exploits the region’s porous coastlines, weak law enforcement and widespread corruption. Yachts, narco-subs and drones have all been used across the network of air and maritime routes.
Alongside Tonga and Papua New Guinea, a key foothold is Fiji – the transport hub is dubbed the ‘gateway to the Pacific’, while four coups since 1987 have eroded democratic institutions and left them open to infiltration.
Recent seizures by the authorities, including 4.8 tonnes of crystal meth and 2.6 tonnes of cocaine, give a sense of the scale of drugs flowing through the archipelago. Police have also confirmed “wash-ups” of drug packages on outer islands – one story circulating suggests unaware locals in one remote village used the “white stuff” as washing powder after it swept ashore.
Yet the nation is no longer simply a stopover point for criminal syndicates: drugs, predominantly methamphetamines, are also spilling into a booming domestic market.
“A transit country doesn’t usually stay as a transit country,” said Megumi Hara, a regional advisor on transnational organised crime at UNODC, based in Suva. “Eventually, it also becomes a destination – and that’s what we’ve seen here.”
The Telegraph witnessed the thriving trade firsthand. As a deep orange sunset spread above Suva on a Sunday evening, two contacts (on the condition we didn’t name them or the places) took us on a “sightseeing tour” of the city’s many drug-dealer hang outs: behind a grey block of social housing, at a nondescript bus stop on a busy road, and a lush green village just outside town.
“This is one of the drug red zones in Fiji,” said one of our well-connected escorts, as the car spluttered up a steep hillside in the village, past a group of boys lurking under a palm tree. “Even the police are scared to come here… they can’t do anything because the drug lord is the landowner. His children, his brother, his brother’s son – they’re all selling drugs.”
When we paused outside a modest wooden house, a gaunt man in a hoodie immediately sauntered up to the car window – in one hand was a red burner phone, in the other six small sachets of crystal meth. The 28-year-old wasn’t there to talk – he scuttled away as soon as another car pulled up, hoping the driver of the white Toyota might make a better customer.
‘A runaway problem with meth’
The sheer volume now circulating on the archipelago is unprecedented. Although surveillance data on use remains limited, the number of cases involving meth reported by the Fiji Police Force jumped 36-fold between 2015 and 2024 – from just 10 arrests to 366.
“Fiji went from having a small number of users, to now having a runaway problem with methamphetamines,” said Prof Sousa-Santos, adding that the market was a deliberate construction.
When organised crime first operated in the Pacific, they developed a network of facilitators – usually people from commercial elites, or with links to law enforcement and government. These connections run deep – between January 2023 and October 2025, the Ministry of Policing said 27 police officers were charged with drug-related offences.
For a fee, corrupt facilitators would ensure the smooth passage of drug shipments through the country. But, as the quantity of drugs grew, criminal syndicates offered to pay in product instead of cash.
From there, local gangs emerged and became increasingly professionalised – by 2018 and 2019, the “white stuff” was not only on the streets but was starting to be sold on university campuses as “study aids”, and to elites as a sex drug. This trade only accelerated when the pandemic disrupted supply routes into and out of the country.
“If you get paid in the drugs, you have the opportunity to triple or quadruple your return,” said Prof Sousa-Santos. “But to do that, you need a local market. In Fiji, the first market that was targeted was sex workers. It grew and grew from there.”
Perched on the curbside of a dark road in east Suva as friends and customers come and go, a charismatic “drug lord” explains how this market operates on his turf.
Simon, whose name has been changed due to ongoing criminal cases, mainly sold and smoked marijuana but swapped the “green stuff” for the “white stuff” when meth started to hit the streets. The upbeat, 48-year-old reggae musician said he was dealing to “put food on the table” for his children, and make sure users had access to “high quality stuff”.
Now the market “has exploded”, Simon said, his eyes wide. Although he was vague about where he gets the meth he hawks from, there are two main distribution routes.
The first is to sell the substance to other “small-time pushers” at a wholesale price – $2,500 Fijian (£835) for seven grams. These dealers then split the meth into at least a dozen small sachets, generally containing 0.08g of crystals, which they peddle on the streets for $50 Fijian (£17) – effectively doubling their money.
Simon and his partners also employ people to work on their patch, running two four-hour shifts a night. Pushers are paid $50 per shift, during which they’d generally sell at least 14 bags of crystal meth – in Fiji, the national minimum wage is $5 per hour.
‘A bin fire became a bushfire’
But methamphetamines alone do not trigger an HIV crisis: the virus – which spreads through bodily fluids – has found fertile ground because of the way the drugs are being used. Widespread sharing of blood, needles and syringes has transformed a small, background epidemic spreading via unprotected sex into an explosive outbreak.
The shift emerged rapidly. In 2021, the country’s two main sexual health hubs in Suva and Lautoka did not report a single HIV case transmitted through drug use – by 2024, 48 per cent of new HIV infections nationally were among people injecting meth, according to UNAIDS.
“You had a lot of young people, very young people, initiating injecting with no context, no information, no awareness and no access to sterile equipment,” said the Kirby Institute’s Prof Maher, who led a Rapid Assessment on injecting drug use and HIV in Suva, commissioned by the UN and published last year. “A bin fire has become a bushfire.”
While sleeping rough on the seafront in 2021 and again in 2023, Ben engaged in many of the risky drug practices that fueled this “bushfire” – sometimes motivated by intrigue, sometimes culture, and sometimes necessity.
One trend at the time was “bluetoothing”, he said, where friends pooled money to buy a single bag of meth, before one person injected the drug. Once they were high, another person drew blood from the initial user and injected themselves, chasing a secondary rush from the traces of meth in the bloodstream. But while a cost-saving (and headline grabbing) concept, bluetoothing is now uncommon as users found it rarely worked.
Instead, some people have reported using blood, rather than water, as the solvent to dissolve methamphetamine. This involves inserting the needle into a vein and repeatedly “flushing” the plunger back and forth to draw enough blood into the syringe to dilute the crystals, before injecting the entire mixture.
“It gives a stronger high… it gives us a lot of energy,” said Ben, explaining the appeal. He still called this practice “bluetoothing”, but most drug users who spoke to the Telegraph and the Rapid Assessment team referred to the approach as “on the rocks”, “dry” or “koda” – a Fijian word which translates to “raw”, and a nod to a traditional raw fish dish called kokoda.
The rampant HIV transmission has also been driven by sharing of mixing paraphernalia – for instance, using the same bottle caps or mugs to dissolve the meth in water – as well as needles and syringes. In that instance, scarcity has partly been caused by a police crackdown based on a misinterpretation of the law.
“The police started coming down hard on pharmacies for selling needles and syringes to anyone wanting one,” said Renata Ram, the Pacific HIV adviser at UNAIDS in Fiji. “That’s when [the HIV] caseload started increasing as well, in late 2021 and 2022.
“If you really want a hit, you’ll find a way to get it – sharing needles was people’s only option,” she said, adding that selling sterile equipment was never actually illegal. “We’ve heard people saying they would share needles about 15 times, or use the same one 15 times.”
She added that stigma is high but knowledge around HIV is low, with a “whole generation” unaware of transmission risks. Some do not know that treatment exists, so see no reason to test, others diagnosed shun anti-retrovirals in favour of traditional Fijian medicines or prayer.
Meri – who, like Ben, asked for her name to be changed because of pervasive stigma in the conservative country – has seen the human cost of the syringe shortage more clearly than most. Within four months last year, she buried three of her closest friends; they were only 33, 42 and 44.
The group started buying methamphetamines just after the pandemic, when they were living on the streets in Lautoka – a city some 120 miles from the capital, on the western side of Fiji’s largest island.
Meri had long been a marijuana smoker, but had never tried the “white stuff” before. Soon the 55-year-old was hooked – she loved “the brightness” and besides, staying awake was useful for long shifts selling cigarettes (some nickname the meth here “mileage”, as it keeps you up for days). But the friends were rarely able to buy sterile equipment – while drugs were everywhere, clean needles and syringes were a luxury.
“They were hard to find, so nearly every time we just shared,” said Meri, sitting cross-legged on a woven mat in a small courtyard at the Survival Advocacy Network (SAN) in Suva. “We washed them, but sharing was kind of [a] necessity.”
Sesenieli Naitala, the founder of SAN, said sharing is also common as it’s hardwired into Fijian life through the custom of “kerekere”, which obliges people to share resources with close friends and relatives. People frequently pass a single cigarette or marijuana joint around a group, while kava – a traditional psychoactive drink – is shared in a single cup.
But in February 2024, Meri tested positive for HIV. She was scared and blamed herself, although she didn’t want to show it – Meri, who wears a cap over her bleach blond pixie cut, attempts an air of nonchalance. She immediately phoned her friends, who still lived on the streets – none of them had considered the risk of blood-borne infections until then.
By the time they were tested, the virus had progressed to Aids. They received treatment, but didn’t stop taking drugs or drinking alcohol and gradually their immune systems faltered. Meri said a final goodbye to two of them in July, and one in October.
“[When I buried them] I was thinking about myself, that I had to change and just leave it behind for good. Because I know if I [keep using] too… it’ll be the same as what my friends went through,” she said softly. “It’s a hard thing to stop [taking meth]… but I had to think of my life.”
‘The epidemic changed, the response did not’
It is now more than a year since the Ministry of Health declared a national HIV outbreak and set up a dedicated taskforce to respond, putting Dr Jason Mitchell, a Fijian doctor who’s worked on HIV across southeast Asia and the Pacific, at the helm.
“The way I describe what’s happened here in Fiji is that the epidemic changed, but programming in response to the epidemic did not,” he said. “So our responsibility here in this unit… is to set up an appropriate response for the new epidemic we’re facing.”
The government unlocked $10 million Fijian (£3m) to do so – up from a budget of $200,000 a year – while international support has ramped up, including £1.7m from New Zealand and £2.6m from Australia, who have also invested £25m in a broader Pacific-wide programme. These countries are also supporting law enforcement operations to counter the flow of drugs into Fiji.
But with key elements of the health response beset by delays, critics say the glacial pace is only giving the virus more time to spread, amplifying the “tsunami of infections” they fear is on the horizon. There are also concerns that punitive attitudes and moral framing of drug use is a continued barrier.
There is still no needle and syringe exchange programme, no pre-exposure prophylaxis (PrEP) available, and no rehab centre. There are also major gaps in testing and treatment. UNAIDS estimates that just 36 per cent of people living with HIV in Fiji were aware of their status in 2024, and only 24 per cent were taking antiretrovirals (there have also been sporadic stockouts of the treatment).
Meanwhile the virus is seeping into new groups: in the first half of 2025, 33 babies were born with HIV, signalling broader weaknesses in the health system.
Dr Mitchell conceded that progress has been slower than hoped, and is clearly frustrated by elements of government bureaucracy.
“The outbreak is so large now that it has the potential to impact the country as a whole, the economy and all of the industries that we rely on – such as tourism, which [is where] 40 per cent of our GDP comes from,” the 47-year-old said animatedly, warning there are also signs HIV is starting to spread to other Pacific island nations.
“So it is an emergency. The most frustrating thing is [that] during Covid… things just happened overnight, approvals just happened, finances just flowed, all of that was fast tracked. That has not happened for the HIV response… Why? It’s a question I can’t actually answer.”
But despite red tape, Dr Mitchell stressed there has been major progress behind the scenes to re-build the capacity, expertise and systems needed to respond (while Fiji once had a robust programme to keep HIV at bay, it was gradually sidelined as cases remained low, new health threats emerged and donor funding for HIV was diverted elsewhere).
He is also optimistic that the much needed needle and syringe programme will launch in the second quarter of the year, once the supplies arrive in March, and hopes PrEP will become available for high risk groups within six months.
In the meantime, 11 new HIV care teams have been established at hospitals across the country, free condom pick-up points have been rolled out, and peer-to-peer education programmes are targeting those most at-risk – including the Angels Collective, a group of drug users who are hitting the streets to teach others about safe injecting practices and HIV.
‘We don’t know what Fiji’s future holds’
For Dr Kesaia Tuidraki, director of Medical Services Pacific, some of the most important programmes are those taking services directly to communities at risk – whether that’s in the Suva’s suburbs or a remote island three days away by boat, where cases are also emerging.
“If you want to reach people you have to go to where they are, because accessibility has always been an issue,” she said, in an office overlooking the capital’s busy port at the NGO’s modest hillside clinic. “Economical issues, unemployment, challenging backgrounds, geographic isolation, stigma – all these things are stopping people from coming forward.
“This means we’re only seeing the tip of the iceberg, there are a lot more [cases] going unnoticed,” she said, adding that many people only test positive once their infection has deteriorated into Aids. According to government data, more than half of the people who died of HIV-related causes in 2024 found out their status the same year.
And so, as evening rush hour traffic eased, a bus kitted out as a mobile clinic set off to a housing project in the densely populated Suva-Nausori corridor. This is the Moonlight programme, which is trying to stem the glaring testing gap that’s hindering the response.
Within half an hour of arriving, a long queue has formed and HIV, hepatitis and syphilis screening gets underway. Outside the bus, health care workers under a bright hanging torch ask preliminary questions, then prick people’s index fingers and transfer the blood to a rapid test. Some 15 minutes later, results are delivered in private inside the compact mobile clinic.
“Well, we caught some tigers,” Vilisi Uluinaceva, the nurse practitioner, said at the end of a long night. Two of 50 tests came back positive – samples will now be sent to the hospital lab for confirmation, and the patients referred to the main clinic for treatment.
That number is lower than previous screenings – at one, mainly among sex workers, 19 of 25 tests came back positive. But the team is pleased so many young people turned up, as cases in this group are surging: in the first half of 2025 alone, 174 children and teenagers aged between five and 19 were diagnosed nationally. Mrs Uluinaceva has treated patients as young as 13.
“We just have to create more awareness on this issue, because if all these children are going to have HIV, there’ll be no future for Fiji,” she said, holding back tears. “Of course I worry and sometimes I’m really emotional – we just don’t know what the future holds.”
But for Ben, the future finally feels exciting again – he’s found a job and a flat share, and is considering re-enrolling at university. It’s a far cry from the weeks after his diagnosis, when the loneliness felt crushing and thoughts of suicide dominated his mind.
“I have come to understand that HIV is just a sickness like any other,” he said, adding that he has been taking antiretroviral treatment for more than 18 months. “We can all be diagnosed with different illnesses, but what matters is how we accept our condition and maintain a positive mindset.”
Walking through the shallow waters less than two miles from the seawall where he used to sleep rough, Ben also shared uplifting news: last week he found out that, for the first time, his HIV viral load is so low it’s undetectable, thanks to the anti-retrovirals. It doesn’t mean the virus has gone, but it means Ben’s condition is stable and he can no longer pass HIV onto someone else. “Here I am today, just living my life like any other normal person,” he said, beaming.
Source: Maggie Petito – Drug watch International
__

In a newly published statement, scientists from EFSA’s Panel on Nutrition, Novel Foods and Food Allergens set the limit at 0.0275 mg/kg of body weight per day. For an average adult weighing 70 kg, this equates to a maximum daily intake of approximately 2 mg.
The new limit is considerably lower than the previous 10 mg provisional limit for an average 70 kg adult, suggested by the UK’s Food Standards Agency (FSA) in late 2023. This stricter European threshold implies that certain products currently on the market may require significant reformulation or relabeling to comply with the emerging EU safety standards.
“This provisional safe dose applies solely to food supplement formulations with CBD purity ≥ 98%, without nanoparticles, for which the production process is considered safe, and genotoxicity is ruled out,” outlines the statement.
“The Panel concludes that, based on all available data, the safety of CBD for individuals under 25 years of age, pregnant or lactating women, and those on concurrent medications cannot be established.”
This 2026 update follows a 2022 statement where EFSA halted all CBD authorizations due to a lack of safety information. While the new report acknowledges that there are still many data gaps around CBD, it performed “benchmark dose modeling” based on recent studies up to June 2024. The team applied an uncertainty factor of 400 to determine its toxicological reference point.
“Concerns [in 2022] focused on potential adverse effects on the liver, gastrointestinal tract, endocrine, nervous, and reproductive systems,” the report authors detail.
“Pharmacokinetic studies confirmed that CBD’s bioavailability is variable, influenced by delivery matrix and food intake. Its ability to cross the placenta and accumulate systemically raises further safety concerns. Animal studies revealed consistent liver toxicity, with liver weight and histopathological changes emerging as sensitive endpoints.”
Human trials indicated hepatotoxic potential, particularly when CBD is used in combination with other medications, EFSA warns. Human trials indicated hepatotoxic potential, particularly when CBD is used in combination with other medications, the authors note. Gastrointestinal effects were reported at higher doses, while neurological and psychiatric safety data remain insufficient.
Meanwhile, animal studies have demonstrated reproductive and developmental toxicity. However, EFSA notes that the extent to which these effects occur in humans is still uncertain, particularly in women of childbearing age and in young adults aged 18 to 25 whose neuronal systems are still developing.
The authors also highlight that neurodevelopmental effects following prenatal exposure were observed in research, suggesting “long-lasting, sex-specific outcomes.” These included endocrine disruptions, such as altered thyroid hormone levels and adrenal histopathology.
EFSA concludes that a safe level cannot be established for individuals under the age of 25, pregnant or lactating women, and consumers taking concurrent medications.
In terms of bioavailability, the agency warns that CBD absorption is highly variable and increases significantly when taken with fatty foods, which complicates setting a fixed safe dose.
The guidance also comes with product specifications. The 0.0275 mg/kg of body weight per day provisional limit applies only to CBD isolates with a purity of 98% or higher, which do not contain nanoparticles and have been cleared of genotoxicity.
EFSA states it will continue to review this provisional level as applicants provide new, high-quality toxicological data to fill the remaining gaps on the nervous and reproductive systems.
Governments have set varying guidance on the safe intake levels for CBD. In the US, the substance remains in a state of regulatory limbo. While the FDA officially maintains that CBD is not authorized for use in foods or supplements under existing federal law, the agency has admitted its current rules are “not appropriate” for the substance.
EFSA concludes that a safe level cannot be established for individuals under the age of 25, pregnant or lactating women, and consumers taking concurrent medications.
Consequently, while the FDA has called on Congress to create a new regulatory pathway specifically for hemp-derived products, thousands of CBD items continue to be sold across the country under a patchwork of state-level laws and federal enforcement discretion.
In Switzerland, the Federal Department of Home Affairs and the Federal Food Safety and Veterinary Office issued a letter in 2021 recommending a maximum daily oral dose of 12 mg CBD for adults. The Swiss authorities are also calling for stricter regulation and more toxicological studies to ensure consumer safety.
Australia’s Therapeutic Goods Administration (TGA) approved low-dose CBD-containing products for over-the-counter access as of Dec 15, 2020. This allows TGA-approved low-dose CBD-containing products, up to a maximum of 150 mg/day, for use in adults to be sold over the counter by a pharmacist without a prescription.
For Canada, the Science Advisory Committee on Health Products Containing Cannabis concluded in 2022 that CBD is safe and tolerable for short-term use (a maximum of 30 days) at doses from 20 mg/day to a maximum dose of 200 mg/day via oral administration for healthy adults, provided they discuss the use of all other medications and substances used with their pharmacist.
Source: https://www.nutritioninsight.com/news/eu-efsa-cbd-cannabidiol-safety-novel-food.html
by WRD News Team February 6, 2026
Between 1980 and now, something fundamental has shifted in how we approach drugs, and understanding this transformation requires examining the historical record with clear eyes. Peter Stoker’s peer-reviewed paper, published in The Journal of Global Drug Policy and Practice in 2007, and very recently merged from a three-part in the Journal version into a single document, republished in the NDPA Website, traces the harm reduction history that changed everything, and his analysis, backed by over 250 references, makes for profoundly uncomfortable reading.
Back in 1980, America had just pulled off something remarkable in public health terms. Through coordinated prevention efforts involving parent groups and community organisations, drug use had dropped by 60%, with approximately thirteen million people stopping entirely. Parent groups had mobilised thousands of families around clear messaging that worked precisely because it was straightforward and uncompromising.
Today we’re told that same approach is not only outdated but fundamentally impossible to replicate. Prevention doesn’t work, the contemporary consensus insists, and the only realistic option is managing drug use rather than preventing it. Schools now teach children how to use drugs “more safely” instead of why they shouldn’t use them at all, representing a philosophical shift so profound that many who lived through both eras struggle to explain how it happened.
So what changed between then and now, and more importantly, how did such a dramatic reversal occur in barely more than a generation?
When Prevention Actually Worked
The 1970s were extraordinarily rough for American communities grappling with escalating drug use across virtually all demographic groups. By 1979, one in three teenagers had tried illegal drugs, whilst among high school seniors the figure approached an alarming two in three. Parents watched their children getting swept up in drug culture and recognised that something fundamental had to give.
Groups like the National Federation of Parents for Drug-Free Youth and PRIDE refused to accept this trajectory as inevitable or irreversible. They developed coordinated responses centred on three straightforward goals: stop kids starting, help users quit, and ensure treatment was available for those who genuinely needed it.
The results, documented across multiple independent studies, speak powerfully to the effectiveness of well-implemented prevention. Between 1980 and 1992, overall drug use fell 60%, representing one of the most successful public health interventions in modern American history. This wasn’t achieved through complex interventions or expensive pharmaceutical solutions, but through clear messaging and communities working together around shared values.
Then, almost imperceptibly at first but with gathering momentum, the tide began turning in a different direction entirely.
Liverpool’s Place in Harm Reduction History
Liverpool in the 1980s was struggling with profound challenges that had been building for years. The Toxteth riots of 1981 had left deep psychological and economic wounds, leaving the city angry, economically battered, and desperately searching for new answers to seemingly intractable problems.
A group of activists saw an opportunity to advance a radically different approach. Peter McDermott, now an editor at the International Journal on Drug Policy, later admitted with remarkable candour what they’d really been pursuing. The goal, in his own words, was to “signify a break with the philosophy that placed a premium on seeking to achieve abstinence,” and this moment would prove absolutely pivotal in harm reduction history.
What happened next is profoundly telling about the unintended consequences that emerge when ideology drives policy ahead of careful evaluation. Liverpool’s heroin users had historically smoked their drugs, a pattern that carried risks but avoided the particular harms of injection. After new programmes started handing out unlimited needles, the city shifted dramatically towards majority injecting use, and Hepatitis C rates climbed sharply during the same period.
A Liverpool mother whose two children battled heroin addiction told Stoker what she saw firsthand. Workers gave out needles “by the bag full,” and they even supplied known drug dealers who’d been promised they wouldn’t be arrested if caught carrying equipment.
The question nobody seemed willing to ask, or perhaps didn’t want to face honestly, was whether this represented genuine public health intervention or something else entirely.
Following the Money
George Soros, operating through various philanthropic entities under his control, had spent over $90 million by 1997 specifically pushing for fundamental changes in drug law and policy. Current estimates, based on tracking available records, put the cumulative total somewhere closer to $200 million invested over subsequent years in supporting liberalisation efforts.
That substantial financial backing funded major advocacy organisations including the Drug Policy Alliance, the Lindesmith Institute, and countless international conferences that shaped policy discourse globally. The money paid for glossy publications reaching policymakers, sustained media campaigns influencing public perception, and full-time lobbyists who could dedicate themselves entirely to advancing liberalisation agendas.
Prevention groups, by stark contrast, operated almost entirely on modest donations and small grants, and the financial mismatch was absolutely crushing in its practical effects on policy influence.
When you can afford international conferences bringing together hundreds of policymakers, employ professional PR firms that understand media dynamics, and fund sympathetic academic research whilst your opponents scrape by on volunteer hours, the playing field isn’t merely uneven. It’s tilted at such an extreme angle that meaningful competition becomes virtually impossible.
How Harm Reduction History Shaped Education
England and Wales had approximately 100 drug education coordinators serving 50 million people during the 1980s, which isn’t a particularly large number to convince if you’re attempting to shift fundamental policy direction. Focused advocacy groups recognised this vulnerability and exploited it systematically.
By the 1990s, British schools were incorporating materials suggesting “drug use is fun” and encouraging students to explore “the benefits of drug taking” without corresponding emphasis on risks. One widely distributed curriculum posed the question: “If adults drink alcohol why should I not take Ecstasy?” without providing any framework for evaluating the obvious differences in legal status, risk profiles, and social consequences.
Australia went considerably further, making these approaches mandatory components of school-based education across entire state systems.
The philosophical groundwork had been carefully laid over preceding decades through broader changes in educational theory. Carl Rogers had developed “values clarification” with the worthy intention of helping students discover values that would serve their development and communities. In practice, however, it morphed into something quite different, as external moral guidance came to be characterised as “anti-democratic” imposition. The new orthodoxy insisted that children should work out their own values largely independently, without what was dismissively termed “interference” from adults.
Rogers himself, watching how his concepts were being implemented and recognising troubling outcomes, later expressed profound reservations. He referred to what his work had enabled as “this damned thing” and questioned publicly whether he’d unwittingly initiated something “fundamentally mistaken.”
By the time Rogers voiced these concerns, however, the educational approaches his work inspired had already achieved such widespread implementation that reversing course would have required acknowledging systemic failure on a scale that bureaucracies rarely prove willing to contemplate.
What the Research Actually Shows
Needle exchange programmes consistently get presented as obvious public health victories, yet the accumulated research tells a considerably more complicated and often quite troubling story.
In Vancouver, HIV rates amongst participants jumped from 2% in 1988 to 23% in subsequent measurements. The city now holds the unfortunate distinction of Canada’s highest overdose death rate, and more than a quarter of participants continue sharing needles despite regular access to sterile equipment.
Montreal found participants had a 33% probability of HIV infection, whilst comparable non-participants showed only 13% probability, raising serious questions about whether participation might actually increase risk.
In India, baseline measurements before programme implementation showed HIV prevalence of 1%, Hepatitis B of 8%, and Hepatitis C of 17%. Following several years of operation, these figures had risen to 2%, 18%, and a truly alarming 66% respectively.
Analysis of 131 American programmes found that of nearly 20 million needles distributed, over 7 million were never returned, leading researchers to characterise many initiatives not as genuine exchanges but as distribution programmes.
Meanwhile, rigorous studies indicated that standard addiction treatment focused on reducing or stopping injection provided substantially superior protection against HIV and Hepatitis C compared to needle programmes operating without treatment components. This finding, however, doesn’t fit comfortably within the preferred narrative and consequently receives minimal attention.
Sweden’s Different Path
Sweden’s experience provides particularly instructive contrast. Following experimentation with permissive policies after World War II and evaluation revealing unfavourable outcomes, Sweden implemented comprehensive prevention-focused strategies as national policy.
The measurable results demonstrate what’s possible when commitment remains consistent over extended periods. Sweden maintains Europe’s lowest substance use rates across virtually all categories and age groups, a remarkable achievement sustained over several decades. Treatment centres operating both voluntary and court-mandated programmes achieve comparable success rates, suggesting quality matters more than admission pathway. Education systematically prioritises preventing initiation rather than teaching “safer” consumption methods.
The Swedish experience demonstrates conclusively that prevention can achieve substantial results when adequately resourced, systematically implemented, and sustained through consistent policy commitment over the time periods required for cultural change to take root.
The Power of Words
Language plays an extraordinarily significant role in shaping how different policy approaches are perceived by stakeholders, from policymakers to the general public. Certain terminology choices have proven remarkably influential precisely because the terms themselves carry implicit assumptions that bypass critical evaluation.
The term “soft drugs” implies substantially reduced harm potential, creating categorical distinctions that research doesn’t necessarily support. “Recreational use” frames consumption within normative leisure contexts, stripping away the reality that we’re discussing powerful psychoactive substances with genuine addiction potential. “Medical use,” when applied to smoking unprocessed plant material rather than tested pharmaceutical preparations, deliberately borrows credibility from established medical practice.
Perhaps the cleverest rhetorical trick has been characterising prevention as “prohibition,” a term that deliberately evokes 1920s American alcohol policy. The word triggers immediate images of gangsters and policy failure, despite substantial historical evidence that actual prohibition achieved measurable public health improvements.
Historical analysis by Robert Peterson demonstrates that prohibition outcomes contradicted common perceptions. Cirrhosis mortality decreased by over a third, alcohol-related psychosis declined markedly, and contrary to widespread belief, murder rates rose far more slowly during prohibition than before or after.
These facts receive minimal attention in contemporary discourse, strongly suggesting that terminology choices serve rhetorical rather than analytical functions, designed to trigger emotional responses rather than encourage careful evidence evaluation.
What Users Actually Want
Professor Neil McKeganey at Glasgow University’s Centre for Drug Misuse Research did something that should be standard practice but apparently represented something quite radical. He systematically surveyed substantial cohorts of drug-dependent individuals, directly asking what services they actually wanted.
The findings revealed patterns that fundamentally contradicted prevailing assumptions underlying current service delivery. The overwhelming majority didn’t request expanded needle programmes or indefinite methadone prescriptions. Instead, they expressed clear desire for clinical assistance in achieving complete cessation and sustained recovery, essentially asking for help to stop entirely rather than support for continued use under marginally safer conditions.
This peer-reviewed finding, published in respected journals and subjected to standard methodological scrutiny, contradicts the entire philosophical rationale underlying approaches focused on managing ongoing use. The research demonstrates that when you actually ask users what they want, they articulate goals aligning much more closely with prevention and treatment than with harm reduction philosophies. These findings, however, have received remarkably limited attention in subsequent policy development and funding decisions.
Europe’s Funding Games
The European Union formally maintains that drug policy falls outside its competence and remains under member state authority through subsidiarity principles. In practical operation, however, the EU exercises considerable influence through strategic funding decisions, policy recommendations carrying significant political weight, and coordination mechanisms shaping national development.
Former Swedish MEP MaLou Lindholm systematically documented troubling patterns in how these mechanisms operate. The European Cities on Drug Policy, representing approximately 30 cities favouring liberalisation, received substantial EU funding sustained over multiple years. Meanwhile, the European Cities Against Drugs, representing over 250 cities supporting UN conventions and prevention strategies, received outright rejections on multiple applications despite membership nearly ten times larger.
The Italian Radical Party, focused explicitly on drug liberalisation advocacy, maintains permanent office space within the EU Parliament building itself. The organisation utilises Parliament telecommunications, internet, and facilities, all taxpayer-funded, to lobby elected officials who often lack detailed policy knowledge.
Analysis suggests most elected representatives possess remarkably limited knowledge of harm reduction history and policy evidence, potentially increasing susceptibility to focused lobbying from well-resourced organisations that can afford professional staff dedicated entirely to influencing legislative processes. Most politicians know almost nothing substantive beyond simplified talking points provided by whichever advocacy groups reach them first.
The Evidence Double Standard
For decades, advocates attacked prevention for supposedly lacking sufficient evidence and failing to demonstrate effectiveness through rigorous evaluation. Demanding evidence-based policy certainly represents legitimate practice, and holding prevention to high standards is entirely appropriate.
What makes this problematic is the glaring double standard in how evidentiary demands get applied depending on which approach is under scrutiny. Anna Bradley, former Director of Britain’s Institute for the Study of Drug Dependence, acknowledged publicly in the late 1990s that “there is no research base for harm reduction,” essentially admitting that programmes promoted as evidence-based alternatives lacked the systematic evaluation their advocates demanded from prevention.
Stoker personally observed a 1988 presentation by Alan Parry, a Liverpool activist, who forcefully demanded rigorous proof from prevention programmes whilst simultaneously acknowledging his own programmes had no evaluation protocols due to “limited funding.” Assessment relied on subjective impressions that approaches appeared “working well.”
This differential standard continues characterising policy discourse in ways seriously undermining claims that contemporary drug policy is genuinely evidence-based. Prevention faces relentless demands for rigorous trials and demonstrated effectiveness, whilst approaches managing active use operate with substantially reduced scrutiny and minimal evaluation requirements.
Why Opposition Got Crushed
The massive resource differential created constraints so severe that fair debate on policy merits became virtually impossible. Well-funded liberalisation groups, backed by hundreds of millions, maintained capacity for activities prevention groups could barely imagine.
They organised international conferences attracting hundreds of participants, providing networking and coordinated messaging shaping global discourse. They afforded professional publication and distribution through established channels. They employed full-time staff and structured lobbying operations developing long-term policymaker relationships. They ran sustained media campaigns across multiple platforms. They funded research programmes and academic positions generating ostensibly independent scholarship supporting preferred directions.
Prevention organisations, operating primarily through volunteer contributions and modest grants, simply couldn’t compete effectively. When prevention advocates secured media attention, they frequently received characterisation as punitive and moralistic. Liberalisation advocates, meanwhile, benefited from portrayal as compassionate, evidence-based, and appropriately pragmatic.
These treatment patterns both reflected and substantially reinforced underlying disparities, creating self-reinforcing cycles where funding advantages translated into media advantages which further entrenched funding advantages through enhanced credibility.
The Cultural Shift Behind Harm Reduction History
Understanding harm reduction history comprehensively requires considering much broader cultural transformations occurring simultaneously. Substance use behaviours don’t occur in isolation but are substantially shaped by prevailing cultural environments and normative frameworks.
From the 1960s onwards, individual rights received progressively increasing prioritisation over community responsibility and collective wellbeing. Traditional authority figures experienced progressive reduction in societal influence. Non-judgementalism became increasingly elevated as paramount virtue, to the point where making moral distinctions between choices became culturally problematic.
Values-based education underwent substantial transformation towards pure individualism. Young people received consistent messaging that external moral guidance constituted “anti-democratic” imposition inappropriate in pluralistic societies. They were systematically encouraged to develop autonomous values without reference to adult perspectives or accumulated cultural wisdom.
Family structures underwent profound changes including dramatically increased divorce rates and single-parent households. Community bonds providing support networks and shared identity weakened substantially as people moved more frequently and participated less in traditional institutions. Materialistic values and immediate gratification became increasingly dominant. Self-focused outlooks progressively superseded concern for collective wellbeing.
Into this comprehensively transformed environment, creating what might be characterised as a moral vacuum, came messaging suggesting drug use represented merely another legitimate lifestyle choice. The message insisted it required professional management rather than moral evaluation or prevention efforts, fitting perfectly within broader currents elevating individual choice whilst dismissing traditional frameworks as outdated.
Drug policy didn’t change in isolation but was intimately connected to cultural shifts creating the environment where harm reduction history could unfold precisely as it did.
Where Things Stand
British drug education reflects substantial influence from approaches systematically prioritising managing use over preventing initiation. DrugScope, receiving up to £3 million annually in government funding, has consistently promoted these approaches whilst prevention perspectives receive substantially marginalised treatment in policy forums and funding decisions.
The Drug Education Forum and Drug Education Practitioners Forum, influential bodies shaping practice across thousands of schools, have been substantially influenced over extended periods by individuals known for publicly opposing prevention priority. Schools consequently receive official guidance tending systematically to undermine clear anti-drug messaging in favour of approaches focused on purported harm reduction.
Australia implemented similar approaches as mandatory national policy several years prior, whilst Canada systematically redirected substantial prevention funding towards programmes serving active users rather than preventing initiation. Across European jurisdictions, prevention organisations face persistent resource constraints whilst liberalisation advocacy receives substantial EU funding.
Nevertheless, recent developments suggest potential for significant reassessment. McKeganey’s research on user preferences created evident discomfort amongst groups claiming to represent user interests authentically. Sweden’s sustained success maintaining remarkably low rates through consistent prevention remains extremely difficult to dismiss. Some former advocates, speaking privately, have begun acknowledging limitations and disappointing outcomes of current approaches, though such admissions rarely translate into policy reversals.
What Harm Reduction History Teaches Us
Stoker’s analysis, drawing systematically on over 250 references spanning decades across numerous jurisdictions, establishes several key evidence-based conclusions deserving serious consideration.
Prevention demonstrates measurable effectiveness when adequately implemented and sustained over sufficient time periods. America’s dramatic 60% reduction during the 1980s provides powerful evidence that prevention works at population scale when communities mobilise around clear messaging. Sweden’s sustained low rates maintained consistently across decades offer additional compelling confirmation.
Current approaches focused predominantly on managing active use whilst neglecting prevention have produced disappointing outcomes across multiple domains. These approaches have demonstrably failed to align with stated user preferences, whom research indicates primarily desire complete cessation rather than indefinite management. They’ve failed families experiencing profound disruption from member addiction. They’ve failed communities experiencing elevated drug-related crime and social disorder.
The substantial financial advantage enjoyed by liberalisation organisations, sustained through foundation funding counted in hundreds of millions, requires explicit acknowledgement and strategic response if prevention voices are to receive fair hearing. Without comparable resources enabling professional operations and sustained engagement, prevention groups will continue facing persistent structural disadvantages.
Media treatment patterns systematically favouring liberalisation require critical examination and direct challenge. The assumption that liberalisation automatically represents compassionate pragmatism whilst prevention represents punitive moralising fundamentally lacks empirical foundation. Genuine compassion would logically prioritise preventing harmful initiation over managing consequences of initiated use.
Educational approaches require systematic reorientation towards messaging clearly communicating evidence-based realities: drugs present genuine health risks, initiation is demonstrably preventable, and young people deserve meaningful protection from exploitation and misguided frameworks normalising harmful behaviours.
Fundamentally, broader cultural renewal merits serious consideration. Shared values, despite contemporary dismissal as outdated, serve crucial protective functions. Community bonds provide essential support structures and accountability mechanisms. Clear guidance from caring adults serves essential protective functions during developmental periods when young people establish lifelong patterns.
Young people benefit substantially from learning that certain choices produce demonstrably better outcomes, not through judgementalism but from genuine concern for their wellbeing and ability to build lives worth living.
The Bottom Line
Stoker’s analysis reveals a well-funded, strategically sophisticated campaign that transformed drug policy over four decades. This transformation wasn’t driven by evidence or user preferences. Research shows users want help to quit, not indefinite management of continued use.
Instead, the shift was driven by ideological commitments backed by unprecedented funding from philanthropic sources, promoted through captured institutions, and facilitated by sympathetic media.
The consequences are troubling. Millions of lives have been negatively impacted by substance use that prevention might have forestalled. Families have been torn apart. Communities struggle with drug-related crime and social disorder. Billions have been allocated to approaches producing limited results whilst prevention remains underfunded.
But it’s not predetermined. Sweden proves prevention works when properly resourced. McKeganey’s research shows academic questioning is emerging. Parent organisations are growing.
The question is whether sufficient will exists to learn from harm reduction history’s lessons. Prevention produces results when adequately funded. Alternative approaches have proven expensive whilst producing disappointing outcomes, despite compassionate rhetoric.
The evidence points towards clear conclusions for anyone genuinely committed to reducing harm.
Source: www.wrdnews.org
Submitted by Maggie Petito – Drug watch International – 01 February 2026
By Nav Rahi with Ben Simon in Toronto – AFP NEWS Jan 31, 2026
Over 35 years as a drug user, Vancouver resident Garth Mullins said he’s had “hundreds and hundreds” of interactions with police, and long believed drug decriminalization was smart policy.
“I was first arrested for drug possession when I was 19, and it changes your life,” said Mullins, who is now in his 50s and was an early backer of Canadian province British Columbia’s decriminalization program that ended on Saturday.
“That time served inside can add up for a lot of people. They do a lifetime jolt in a series of three‑month bits,” he told AFP.
BC’s three-year experiment with drug decriminalization, which launched in 2023 and shielded people from arrest for possession of up to 2.5 grams of hard drugs, was ground-breaking for Canada.
Many praised it as a bold effort to ensure the intensifying addiction crisis devastating communities across the country was treated as a healthcare challenge, not a criminal justice issue.
But on January 14, BC’s Health Minister Josie Osborne announced the province would not be extending the program.
“The intention was clear: to make it easier for people struggling with addiction to reach out for help without fear of being criminalized,” Osborne said.
The program “has not delivered the results we hoped for,” she told reporters. For Mullins, the province’s desired results were never realistic.
The former heroin user, who currently takes methadone, is an activist and broadcaster who co‑founded the Vancouver Area Network of Drug Users (VANDU), which advised BC’s government on decriminalization.
At VANDU’s office in Vancouver’s Downtown Eastside neighborhood, home to many drug users, the walls are full of pictures honoring those who have died from overdose.
“The idea behind decriminalization was one simple thing: to stop all of us from going to jail again and again and again,” he said.
Breaking the cycle of arrests is crucial because criminal records make it more difficult to find work and housing, often perpetuating addiction, experts say.
But thinking decriminalization could help steer waves of users into rehab was misguided, and misinforming the public about the possible outcomes of the policy risked a backlash, Mullins said.
“For everybody out there, in society, sending fewer junkies to jail might not sound like a good thing to do.”
After the province announced the program’s expiration, Canadian media was filled with critics who said it had been mishandled.
Vancouver police chief Steven Rai said his force had been willing to support the plan, but “it quickly became evident that it just wasn’t working.”
Decriminalization “was not matched with sufficient investments in prevention, drug education, access to treatment, or support for appropriate enforcement,” he added.
Cheryl Forchuk, a mental health professor at Western University who has worked on addiction for five decades, said BC “never really fully implemented” decriminalization because the essential complementary programs — especially affordable housing supply — were never ramped up. “It was like they wanted to do something, but then really didn’t put the effort into it and then said, gee, it didn’t work,” she told AFP.
BC’s experience mirrors that in the US state of Oregon, which rolled back its pioneering drug decriminalization program in 2024 after a four-year trial.
Like in Oregon, BC’s program faced fierce criticism, with many saying public safety was threatened by a tolerance of open use.
A flashpoint moment in the western Canadian province was a 2024 incident where a person was filmed smoking what appeared to be a narcotic inside a Tim Hortons, the popular coffee shop chain frequented by families across the country.
Local politicians in Maple Ridge, BC, attributed the incident to a permissiveness about drugs ushered in by decriminalization. But for Mullins, the incident spoke to broader misconceptions about the intent of the policy.
Decriminalization did not allow for drug use inside a restaurant, and the person could have been arrested. Drug user advocates, he added, don’t want policy that makes the broader public feel threatened.
“We need something where everybody feels safe, right? If people who are walking with their kids don’t feel safe, that’s a problem for me,” he said. But, he added, security also matters to users for whom “the world feels very scary and unsafe.”
Source: www.drugwatch.org
—
by Erikka Loftfield, PhD, MPH – NIH – January 26, 2026
Key takeaways:
An analysis of more than 88,000 U.S. adults provides new insights into how duration and extent of alcohol consumption may affect colorectal cancer risk.
Current and consistent heavy alcohol intake throughout adulthood appeared associated with a near-doubling of risk compared with current, consistent light drinking, data from a population-based randomized screening trial showed.
Data derived from O’Connell CP, et al. Cancer. 2026;doi:10.1002/cncr.70201.
Higher lifetime alcohol consumption also appeared associated with significantly higher risk, particularly for rectal tumors.
In addition, the findings suggested benefits of alcohol cessation, including lower odds for colorectal cancer or nonadvanced adenomas.
Erikka Loftfield states that “The findings of this study support — and really give empirical weight to — guidance from internationally recognized bodies that recommend limiting or abstaining from alcohol intake to reduce cancer risk,” .
Filling an evidence gap
Research has intensified over the past several years into alcohol’s role in cancer development.
A population-based study led by International Agency for Cancer Research linked alcohol consumption to more than 740,000 new cancer diagnoses in 2020, equivalent to 4% of cases worldwide.
Loftfield and colleagues analyzed data from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial — designed to determine the effects of screening on cancer-related mortality among cancer-free adults — to estimate the association between lifetime alcohol consumption and incident colorectal cancer or adenoma.
“Prior studies have established that alcohol consumption is associated with increased risk of cancer, but there’s very little data regarding how lifetime patterns of drinking affect colorectal adenoma and cancer risk,” Loftfield said. “We wanted to try to fill that gap. We know a lot about how smoking cessation lowers cancer risk, but we wanted to learn more about what reduction or cessation of alcohol drinking means for future cancer risk.”
In the PLCO trial, researchers randomly assigned people aged 55 to 74 years to cancer screening or standard care. Colorectal cancer screening consisted of flexible sigmoidoscopy at baseline, and again either 3 years or 5 years later.
Trial participants completed risk factor and dietary history questionnaires. They reported alcohol intake during four age periods —18 to 24 years, 25 to 39 years, 40 to 54 years, and 55 years and older — using 10 predefined frequency categories, as well as current drinking frequency at baseline.
Loftfield and colleagues categorized participants as current drinkers, former drinkers or never drinkers.
They used multiple categories to quantify average lifetime drinking — less than one drink per week, one to less than seven drinks per week, seven to less than 14 per week, or 14 or more per week — and they used past and current drinking frequency to define broader alcohol intake patterns through adulthood.
They used sex-specific U.S. dietary guidelines to classify light drinking (less than 14 drinks per week for men, less than seven per week for women), moderate drinking (14 to 21 drinks per week for men, seven to 14 per week for women) and heavy drinking (22 or more per week for men, 15 or more per week for women).
‘Timely’ findings
During 20 years of follow-up, 1,679 incident colorectal cancer cases occurred among 88,092 PLCO trial participants.
Current drinkers who had an average lifetime alcohol intake of 14 or more drinks per week exhibited a 25% (HR = 1.25; 95% CI, 1.01-1.53) higher risk for colorectal cancer than those with average lifetime intake of one drink or less per week.
Those with higher average lifetime alcohol intake had nearly double the risk for rectal cancer (HR = 1.95; 95% CI, 1.17-3.28).
“This finding is timely because we are seeing increasing rates of colorectal cancer among younger people, and that increase has been driven predominantly by rectal tumors,” Loftfield said.
Consistent heavy drinking appeared associated with a near-doubling of colorectal cancer compared with light drinking (HR = 1.91; 95% CI, 1.17-3.12).
The data also suggested benefits of alcohol cessation.
Former drinkers who had been moderate to heavy drinkers earlier in life exhibited similar colorectal cancer risk as light drinkers.
An analysis of about 12,000 PLCO trial participants who had negative baseline screens compared former drinkers with current drinkers who averaged less than one drink per week in their lifetime. Results showed former drinkers had numerically lower risk for any adenoma (OR = 0.78; 95% CI, 0.59-1.02) and significantly lower risk for nonadvanced adenoma (OR = 0.58; 95% CI, 0.39-0.84).
“From a clinical perspective, that is pretty robust evidence to support that there is a benefit to drinking cessation,” Loftfield said.
The mechanisms of alcohol’s impact on cancer risk have been well studied, specifically related to how alcohol in the body converts to acetaldehyde, a known carcinogen. Less is known about how alcohol affects the gut microbiome and the impact that may have on colorectal cancer risk, Loftfield said.
Loftfield and colleagues hope to conduct additional research exploring the impact of lifetime alcohol use — and alcohol cessation — on other malignancies, such as liver cancer.
Further study into the effects of alcohol cessation on people who average one to two drinks per day also could be valuable, Loftfield said.
“We know a lot more about heavy drinkers who quit drinking or reduce their alcohol intake,” she said. “A better understanding of what happens for moderate drinkers, and how their biology changes when they reduce or quit drinking, may help inform what we know about cancer prevention.”
Source: Herschel Baker – International Liaison Director, Queensland Director, Drug Free Australia
One in four U.S. adolescents is exposed to violence in their neighborhood, and those teens are more than twice as likely to use cigarettes, alcohol or drugs to cope, according to a new study from The University of Texas at Arlington.
Published in the Journal of Affective Disorders, the study was led by UT Arlington School of Social Work Professor Philip Baiden and drew on national data from the 2023 Youth Risk Behavior Survey. Researchers analyzed responses from 20,005 adolescents ages 12 to 18, offering new insights into early pathways to substance use, a persistent public health concern.
“Our study reminds us that violence is not a rare or isolated experience for many young people—it is a daily reality,” Dr. Baiden said. “Youth exposed to neighborhood violence often carry the psychological weight of chronic stress, fear and trauma. Many turn to alcohol, marijuana, vaping or other substances to self-medicate or numb the emotional impact of these experiences.”
According to the 2024 National Institute on Drug Abuse annual report, 58.3% of individuals ages 12 or older reported using tobacco, vaping nicotine, alcohol or an illicit drug in the prior month. Substance misuse contributes to preventable illness and death nationwide.
Catherine LaBrenz, coauthor of the study and a UTA School of Social Work associate professor, noted that previous research has shown neighborhood violence can alter how the brain processes emotions.
“When teens experience chronic fear or trauma, it can increase vulnerability to substance use,” Dr. LaBrenz said.
The researchers examined five substance categories: cigarette smoking, alcohol use, electronic vaping products, marijuana use, and prescription opioid misuse. Exposure to neighborhood violence was associated with higher odds of using all five substances, even after controlling for demographics, mental health symptoms, physical activity and bullying involvement.
The study also revealed several notable patterns. Cyberbullying is more strongly linked to substance use than traditional school bullying. In addition, students who participate in team sports tend to report higher rates of alcohol use.
“Cyberbullying is distinct in that it follows adolescents everywhere—there is no escape,” Baiden said. “If someone is bullied on a school playground, it’s traumatizing but you could brush it off and might be able to outgrow it. When it is cyberbullying, it spreads widely, persists indefinitely and you don’t know who has access to it, which makes its emotional impact even more traumatic. You can’t just delete it.”
Related: Researchers uncover surprising link to stroke risk
The study also identified a nuanced relationship between team sports and substance use. Participation in team sports such as football, for example, was linked to increased alcohol use.
“Team sports can offer structure, belonging and social support, but they also expose adolescents to peer cultures where alcohol use may be normalized,” Baiden said. “That helps explain why we see increased odds of drinking among youth who participate.”
Baiden and LaBrenz said the findings could help inform policies and prevention strategies aimed at reducing substance use among adolescents. Further research will focus on specific populations and potential interventions.
“It’s not enough to document adverse effects,” Baiden said. “We want to identify interventions that counselors, mental health professionals and social workers can use when working with youth who experience neighborhood violence.”
UTA Social Work professors Angela J. Hall and Joshua Awua were contributing authors to the study.
About The University of Texas at Arlington (UTA)
The University of Texas at Arlington is a growing public research university in the heart of the thriving Dallas-Fort Worth metroplex. With a student body of over 42,700, UTA is the second-largest institution in the University of Texas System, offering more than 180 undergraduate and graduate degree programs. Recognized as a Carnegie R-1 university, UTA stands among the nation’s top 5% of institutions for research activity. UTA and its 280,000 alumni generate an annual economic impact of $28.8 billion for the state. The University has received the Innovation and Economic Prosperity designation from the Association of Public and Land Grant Universities and has earned recognition for its focus on student access and success, considered key drivers to economic growth and social progress for North Texas and beyond.
Source: https://www.uta.edu/academics/schools-colleges/social-work/news/releases/2026/01/28/one-in-four-teens-face-violence-higher-substance-use

Fentanyl has become one of the greatest health, social, and security challenges of the 21st century. This synthetic opioid, originally created for medical purposes, is now at the center of an unprecedented crisis that is hitting the United States particularly hard and is beginning to spread alarmingly to other countries around the world
More potent than heroin and morphine, cheap to produce, and extremely addictive, fentanyl has transformed the illegal drug market and caused hundreds of thousands of overdose deaths in the last decade. Its impact extends far beyond public health: it affects security, the economy, social stability, and international relations.
Origin and medical use of fentanyl
Fentanyl was developed in the 1960s as a pain reliever for hospital use. In the medical field, it remains a key tool for treating severe pain, especially in surgery, palliative care, and cancer patients. Under medical supervision, its use is safe and effective.
The problem arises when this substance leaves the legal market and begins to be produced clandestinely. On the black market, fentanyl is manufactured without controls, in unpredictable doses, and is mixed with other drugs such as heroin, cocaine, or methamphetamines, often without the user’s knowledge.
The fentanyl crisis in the United States
The United States is the epicenter of the crisis. In recent years, fentanyl has become the leading cause of overdose deaths in the country. Its low cost and enormous potency have made it attractive to criminal networks, which use it to enhance other drugs and maximize profits.
The social impact is devastating. Entire families are experiencing irreparable losses, healthcare systems are overwhelmed, and whole communities, both urban and rural, are facing profound decline. The crisis does not discriminate based on age, social class, or region: it affects young people, adults, and the elderly.
Why is fentanyl so lethal?
The main reason it’s dangerous is its potency. A minimal dose can be enough to cause a fatal overdose. Furthermore, when mixed with other substances, the user loses all sense of the amount ingested.
Another key factor is how quickly it acts in the body. Fentanyl depresses the respiratory system, which can lead to death within minutes if there is no immediate intervention.
The role of drug trafficking and illegal production
The illegal production and distribution of fentanyl is a global phenomenon. The chemical precursors are typically manufactured in different countries, then assembled in clandestine laboratories, and finally distributed through transnational networks.
This has turned fentanyl into a geopolitical problem. Governments must coordinate efforts to control chemical precursors, combat drug trafficking, and strengthen borders, while also recognizing that this is a public health crisis.
The challenge for the rest of the world
Although the United States accounts for the majority of deaths, other countries are beginning to register warning signs. In Latin America, Europe, and Asia, cases of drugs adulterated with fentanyl are increasingly being detected, raising the risk of overdose even among occasional users.
The American experience serves as a warning. Without preventative policies, prepared health systems, and international cooperation, the crisis could be replicated in other regions.
Prevention, treatment and public policies
Addressing the fentanyl problem requires a comprehensive approach. Prevention is key, especially through education and information. Many deaths occur because people are unaware they are using an extremely dangerous substance.
Access to addiction treatment, the availability of medications to reverse overdoses, and the strengthening of healthcare systems are fundamental pillars. At the same time, it is necessary to combat the criminal organizations that profit from this drug.
A threat that demands a global response
Fentanyl is not just a problem in the United States. It is a global threat that challenges governments, healthcare systems, and entire societies. Its spread demonstrates how quickly drug trafficking adapts to market opportunities, even at the cost of thousands of lives.
The fight against this deadly drug requires international cooperation, evidence-based policies, and a human-centered approach that understands addiction as a public health problem. Otherwise, the world risks facing an even greater crisis in the coming years.
Source: https://www.aurora-israel.co.il/en/fentanyl-lethal-drug-United-States/
A new publication by the United Nations Office on Drugs and Crime (UNODC) finds that drug use in Afghanistan remains dominated by traditional substances, while the use of synthetic substances and misused pharmaceutical drugs is increasing. In this assessment, men most frequently cited cannabis (46%) and opium (19%) as the drugs used in their communities, while “Tablet K” (11%) and methamphetamine (7%) were also mentioned.
This publication is the third and final volume of UNODC’s National Survey on Drug Use in Afghanistan (NSDA), funded by UNDP. It builds on two earlier health-focused volumes on mapping of facilities for treatment of substance use disorders and assessing high-risk drug use. The last national measurement of drug use in Afghanistan was in 2015.
The findings highlight the economic burden of household dependence. The cost of substances such as methamphetamine and opium can exceed a full day’s wage. For example, one day of methamphetamine use can cost up to 138% of a casual worker’s daily income or 67% of a skilled worker’s wage. Respondents linked ongoing drug use mainly to poverty, unemployment, and financial hardship. They also cited physical pain and ill health, psychological distress, family challenges, and dependence. Overall, the results show strong links between substance use and wider socio-economic pressures.
“Our findings show drug use is closely linked to poverty, unemployment, and untreated health needs. Effective responses must integrate treatment and harm reduction with primary health care, mental health support, and social protection to reduce harmful self-medication and support recovery”. Said Mr Oliver Stolpe, UNODC Regional Representative, Regional Office for Afghanistan, Central Asia, Iran, and Pakistan.
“This national survey gives us a clear picture of the realities of drug use in Afghanistan and the challenges people are facing. The findings will help shape stronger policies and programmes to address the health dimensions related to drug use, support recovery, and tackle the root causes of drug use, including lack of jobs and economic opportunities. It also shows what we can achieve when UN agencies work together, combining our strengths to deliver better results for the Afghan people.” Said Mr. Stephen Rodriques, UNDP Resident Representative in Afghanistan.
Earlier findings from UNODC’s High-Risk Drug Use Survey emphasis the health risks associated with Afghanistan’s changing drug landscape. The survey found that 8% reported having injected drugs in their lifetime, and among those who injected, more than 75% reported sharing needles and around half reported inconsistent access to sterile equipment, pointing to gaps in harm reduction coverage.
A gender gap was also evident, with only 29% of women reporting treatment compared with 53% of men, underscoring the need to expand women-specific services.
While de facto authorities report treating large numbers of people who use drugs, the first volume in this series, UNODC’s mapping of facilities for treatment of substance use disorders, shows that major gaps persist in distribution, accessibility, quality, and gender coverage. Nearly two-thirds of facilities serve men only, 17.1% serve women only, and in the 32 provinces surveyed, just over one-third have services available for women. The mapping also found ongoing constraints, including shortages of qualified health professionals and insufficient infrastructure.
“These studies are essential to further guide the response of the de facto authorities, donors, UN and partners to this extremely serious problem. The study recommends a people-centred response: putting people first by ending the stigma and discrimination surrounding drug use,” said Georgette Gagnon, Officer in Charge of UNAMA and Deputy Special Representative of the UN Secretary-General in Afghanistan. “We reiterate that prevention is the most essential, cost-effective strategy to halt the flow of drugs, protect communities, and reduce demand.”
Based on the three volumes and international standards, UNODC recommends expanding voluntary, rights-based treatment and harm reduction services for men and women, alongside investments in health worker training and minimum facility standards. Responses should be linked to primary health care, mental health and psychosocial support, and social protection and employment assistance to address poverty, pain and distress. Interventions should also be tailored to provincial drug market patterns and reduce the burden on households through family-centred services and livelihood support for people in treatment.
The three reports can be accessed via the links below:
Source: https://www.unodc.org/coafg/en/Press-Release/unodc-report-finds-drug-use-in-afghanistan-is-shifting-toward-synthetic-drugs-and-the-misuse-of-pharmaceutical-drugs.html

A Vancouver overdose prevention site has closed less than two years after it moved from its previous location, raising concerns among health officials and harm reduction advocates as the province sees record number of overdose calls to emergency services.
The Thomus Donaghy Overdose Prevention Site, located at 1060 Howe St., shut its doors Saturday, according to Vancouver Coastal Health.
The health authority says the owner of the building, Prima Properties, notified them to leave the property by the end of January after hearing a number of complaints from nearby residents.
CBC News reached out to the building’s owner to understand the scope and nature of the complaints but did not hear back by deadline.
Dr. Patricia Daly, VCH’s chief medical health officer said the health authority took steps to address neighbourhood concerns, including hiring security, conducting needle sweeps, and placing staff on the sidewalk to prevent disorder.
“I myself frequently went down and observed that things seemed to be operating as they should,” Daly said.
The Howe Street location opened after the site was moved from Seymour Street in Yaletown in April 2024 following public safety concerns and backlash from nearby residents.
“It was actually a very good location, not visible to people on the street,” Daly said.
It was the only one of its kind in what VCH calls the Vancouver City Centre area, which includes most of downtown, the West End and Fairview.
“That neighbourhood has the second highest rate of overdose deaths in our region, and the third highest rate in the entire province,” Daly said.
Daly says the OPS typically saw about 400 to 500 visits per week and has reversed more than 300 overdoses since its opening.
Across Vancouver, there are 12 overdose prevention sites, most of them located in the Downtown Eastside. But with the latest closure, that number drops to 11.
People who relied on the site will be directed to services in the Downtown Eastside, which is about a 30-minute walk away.
************
Earlier this week, the B.C. Centre for Disease Control issued a province-wide drug alert, noting new substances in the unregulated drug supply are putting people at risk province-wide.
It says medetomidine, used primarily by veterinarians to sedate animals, is now being mixed with opioids like fentanyl.
Harm reduction and recovery advocate Guy Felicella said closing overdose prevention sites at a time like this is “disappointing and sad.”
“With the drug supply this deadly, not only you’re going to see people consuming substances out in the community, we could also witness people dying out in the community,” he said.
“I struggled in this area and the Downtown Eastside for decades and I was brought back to life multiple times at these services,” he said.
Daly says the health authority is working with the City of Vancouver and other partners to identify a permanent or at least a temporary replacement location but she says it has become increasingly difficult to find a location that would host overdose prevention services.
“We hope to have something available on at least a temporary basis within the next week or two,” she said.
Source: https://www.cbc.ca/news/canada/british-columbia/thomus-donaghy-overdose-prevention-site-closing-9.7069806

Four billboards with the Fentanyl Free America message have posted in Omaha, Nebraska.
OMAHA, Neb. – Four billboards designed to spark conversation about fentanyl popped up Feb. 2, in eastern Omaha in support of the Drug Enforcement Administration’s (DEA) Fentanyl Free America initiative. Fentanyl Free America is DEA’s commitment to protecting the United States from synthetic opioids, such as fentanyl, by disrupting supply chains, reducing availability and saving American lives.
In 2025, agents with the DEA Omaha Field Division removed approximately one million deadly doses of fentanyl from Nebraska communities, enough to kill the entire Omaha metropolitan area population. Among this tally were 46 pounds of fentanyl powder and 146,000 counterfeit pills. Nebraska followed a nationwide trend in which powder seizures were higher than the year prior. Agents continue seeing fentanyl mixed with other substances including heroin, methamphetamine and cocaine, with users often unaware of its presence. In encouraging news, DEA labs reported a decline in fentanyl powder purity dropping from 20% in 2024 to 10/3% in 2025.
The billboards in Omaha emphasize three pillars of the Fentanyl Free America initiative, Protect, Prevent and Support and feature a website for additional information, dea.gov/fentanylfree.
“Enforcement is what we do best,” DEA Omaha Field Division Special Agent in Charge Dustin Gillespie said. “Working with our state, local, tribal and federal law enforcement partners, we shoulder the responsibility of protecting neighborhoods from drug threats. We work investigations that lead us into Mexico and chip away at the cartels pushing lethal substances into Nebraska. Now, we’re calling on the public to help with prevention and support. Don’t assume that your friends know the consequences of fentanyl use. Tell them, remind them, continue the conversation. If we truly want to eliminate fentanyl, we need to support one another, working together through different channels to make a difference.”
Locations of DEA’s Fentanyl Free America billboards are listed below.
Billboard locations in Omaha
Source: https://www.dea.gov/press-releases/2026/02/03/deas-fentanyl-free-america-billboards-remind-omaha-community-local-threat

At a sumptuous resort just outside Washington, DC, on February 2 for “Prevention Day,” Health and Human Services Secretary Robert F. Kennedy Jr. announced his Safety Through Recovery, Engagement and Evidence-based Treatment and Supports (STREETS) Initiative. He opened by scapegoating people who use drugs as “negative producers” and “drags on the whole [health care] system.”
STREETS is billed as a $100-million investment to “solve long-standing homelessness issues, fight opioid addiction and improve public safety by expanding treatment.” It will be piloted in eight as-yet-unspecified cities, and is designed to operate in tandem with “assisted outpatient treatment” (AOT)—court-ordered psychiatric probation, similar to probation for drug violations. AOT saddles participants with the ever-present threat of being involuntarily committed to a psychiatric facility for noncompliance, or even just a technical violation. HHS will soon offer $10 million in AOT grants (though this amount has been higher in previous years).
Kennedy now wants provider organizations to “take charge of an addict” for a period of one to three years. Providers would receive bundled payments if they ensure that the people in their custody remain in compliance with an abstinence-only model. This will prove beneficial to providers with stake in urinalysis testing—possibly the most notorious financial scheme in the rehab industry—but is not likely to result in long-term abstinence. It also incentivizes providers to employ policies that are increasingly punitive, result in misleading data, or both.
“While ICE terrorizes our families and communities, STREETS will do little to address our addictions, mental health and homelessness crises.”
STREETS furthers President Donald Trump’s July 2025 executive order titled “Ending Crime and Disorder on America’s Streets,” which was widely condemned as a declaration of war on unhoused people. The Legal Defense Fund likened it to a resurrection of the Black Codes preceding today’s “vagrancy” laws.
The Housing First model, which does not require abstinence as a precondition of access to permanent supportive housing, was created to address the failures of the “tough on homelessness” approach favored in the 1980s. Trump’s HHS has characterized Housing First and harm reduction-based programs as “misguided,” falsely claiming that they’ve been ineffective and “enabled future drug use.” This is reminiscent of proponents of involuntary commitment falsely contending that deinstitutionalization failed, when it was never fully implemented and was arguably still the most successful decarceration effort in United States history.
“While ICE terrorizes our families and communities, STREETS will do little to address our addictions, mental health and homelessness crises,” former Substance Abuse and Mental Health Services Administration official Paolo del Vecchio told Filter, “turning away from proven harm reduction and Housing First approaches while embracing failed practices of coercion and criminalization.”
In red and blue jurisdictions alike, messaging is shifting from public health to public safety. Policymakers are expanding the reach of civil commitment laws to remove unhoused people from public view, disappeared into a vast system of coercive programs. Some fear these may include forced labor farms and detention camps.
Investment in faith-based treatment and “outcome-oriented” payment models all but guarantee increased coercion from providers.
In 2025 the White House announced its Faith Office, which supports “faith-based entities, community organizations and houses of worship” in competing on “a level playing field” for federal grants and other funding opportunities.
“Faith-based organizations play a critical role in helping people re-establish their connections to community,” Kennedy, a 12-step devotee, told the audience on February 2. The same day, Faith Center Director Monty Burks spoke at a separate, virtual event introducing STREETS to community stakeholders.
Several of the Prevention Day event speakers signaled the desire to phase out the health insurance industry’s current fee-for-service models, in which providers are reimbursed based on quantity, and instead use “outcome-oriented” or “values-based” payments that incentivize based on quality—and are still rife with inequities. The costs and administrative burdens of both approaches could be eliminated if we ditched the predatory health insurance industry in favor of Medicare for All.
Investment in faith-based treatment and “outcome-oriented” payment models all but guarantee increased coercion from providers, potentially in violation of the First Amendment.
In January, a separate executive order establishing the “Great American Recovery Initiative” (of which Kennedy is a co-chair) warned that most people who need treatment don’t think that they do. It appears that the public is being primed for the widespread involuntary detention of unhoused people who use drugs and/or have visible symptoms of mental illness.
“We intervene early,” Kennedy told Chris Cuomo of News Nation on February 3. “We catch people on the street and channel them into treatment, out of crisis through detox, treatment, outpatient and into sober housing.”
Cuomo gently pushed back: “You can’t make people get treatment if they don’t want to.”
“We have a community care program that involves the courts,” Kennedy retorted. This, he said, is a more “efficient, economic and humane” approach to those who refuse services.
Source: https://filtermag.org/hhs-streets-initiative-treatment-prevention-day/amp/
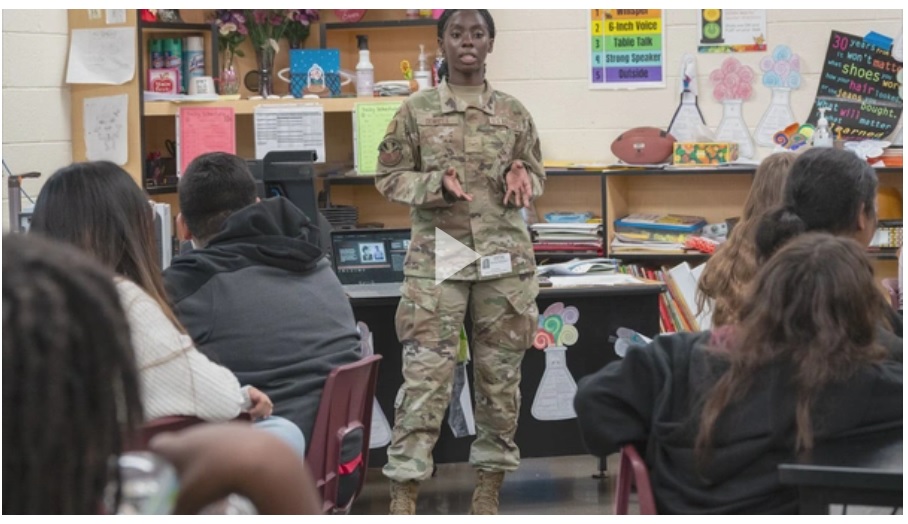
Red Ribbon Week, the nation’s largest and longest running drug prevention campaign, serves as a reminder of the importance of prevention, education, and community involvement.
Observed annually from Oct. 23 through Oct. 31, the campaign brings together schools, families, and organizations nationwide to promote drug-free lifestyles and encourage young people to make healthy choices.
The campaign was established in honor of Drug Enforcement Administration Special Agent Enrique “Kiki” Camarena, who was killed in 1985 while investigating drug cartels in Mexico. His sacrifice sparked a national movement symbolized by the red ribbon, which represents a collective stand against substance misuse and a commitment to protecting future generations. Since then, Red Ribbon Week has educated millions through educational programs, student pledges, rallies, and prevention-focused activities.
In Arizona, the Counterdrug Task Force’s Drug Demand Reduction and Outreach (DDRO) program has played an increasing role in Red Ribbon Week by expanding statewide prevention efforts and access to education and outreach services.
In 2023, DDRO recorded 8,107 engagements during Red Ribbon Week, along with 8,050 student pledges. In 2024, those numbers tripled to 25,183 engagements and 11,110 pledges. In 2025, DDRO reached a new milestone, achieving 82,829 engagements and 28,236 student pledges during the campaign.
These figures represent more than attendance totals, they reflect points of connection where prevention messaging reached students, families, and communities. Engagements included in-person classroom presentations, community outreach events, public service announcements, online interactions, YouTube views, and joint outreach efforts conducted with the Drug Enforcement Administration (DEA). DDRO also expanded access through virtual presentations, ensuring schools and organizations unable to host in-person events could still participate.
A major enhancement in 2025 was DDRO’s decision to extend Red Ribbon Week outreach beyond the traditional calendar. Instead of limiting activities to a single week, prevention efforts were expanded from Oct. 1 through Nov. 5. This extended timeframe provided schools greater flexibility to participate, increased accessibility for underserved communities, and amplified statewide impact.
According to Daniel Morehouse, Community Outreach Specialist with the U.S. Drug Enforcement Administration, collaboration between DDRO and DEA played a critical role in amplifying prevention messaging during this year’s Red Ribbon Week. He emphasized that the scale of reach achieved in 2025 would not have been possible without shared resources and coordinated efforts. When agencies work together, Morehouse noted, audiences, particularly youth, are more engaged and receptive.
“Our drive for a Fentanyl Free America requires not just the enforcement side of things, but also outreach and education,” Morehouse said, adding that DDRO’s professionalism and prevention expertise significantly strengthens DEA’s prevention tools and messaging.
The success of DDRO’s Red Ribbon Week is rooted in strong partnerships. Schools across Arizona coordinated schedules, engaged students, and supported prevention activities. Community organizations, prevention coalitions, and agency partners worked alongside DDRO to strengthen outreach and reinforce consistent prevention messaging.
Merilee Fowler, Executive Director of the Substance Awareness Coalition Leaders of Arizona, highlighted the importance of collaboration in achieving meaningful impact. She shared that it was inspiring to see the number of students and adults reached during the 2025 campaign; noting that students across Arizona proudly pledged to grow up safe, healthy, and drug-free.
Fowler emphasized that coordinated prevention efforts strengthen communities statewide. When prevention organizations and coalitions work together, she explained, they create collective impact that improves the ability to prevent and reduce substance use. She also stressed the importance of a comprehensive approach that balances enforcement with education and outreach.
“Preventing and solving drug problems in our communities is complex and requires a combination of enforcement, education, and outreach,” Fowler said. “Success depends on all of us working together as a united team.”
She further noted that effective prevention must include families as well as youth. Partnerships among DDRO, SACLAZ, DEA, and other organizations have expanded outreach to parents and caregivers, and open conversations at home about the real harms of substance use play a critical role in prevention, she said.
U.S. Arizona Air National Guard Senior Master Sgt. Michael Gunderson, serves as the Non-Commission Officer in Charge of Arizona DDRO. In this role, Gunderson oversees the planning, coordination, and execution of statewide substance-use prevention and education efforts, working closely with schools, community coalitions, law-enforcement agencies, and prevention partners.
“At the heart of Red Ribbon Week and DDRO’s expanding efforts are the students themselves. Each pledge represents a personal commitment, and each engagement reflects a conversation that may influence future decisions,” said Gunderson. “The continued growth of DDRO’s Red Ribbon Week outreach demonstrates the power of prevention when communities unite around a shared purpose, protecting youth, honoring legacy, and building healthier, safer futures.”
As DDRO continues to grow, the program remains committed to refining its practices through evaluation, evidence-based strategies, and flexible delivery methods tailored to community needs. These efforts ensure prevention messaging remains accessible, relevant, and effective.
Source: https://www.dvidshub.net/news/556965/arizona-red-ribbon-week-expands-reach-spreading-prevention-awareness
In past years, the U.S. said that women could have up to one drink per day and men could have up to two drinks per day if they chose to drink alcohol. But the new guidelines removed those specific daily limits. Now, the main message is that people should “consume less alcohol for overall better health.” There’s no fixed number of drinks in the new advice.
The change doesn’t mean alcohol is “healthy.” It’s simply because the government no longer lists a safe number of drinks per day. Instead, it focuses on general moderation and a healthy diet that includes better food choices.
Not all health experts agree with this change. Many doctors and public health groups are concerned for several reasons:
Some healthcare providers also worry that the changes were influenced more by the alcohol industry than by science, which could weaken the health message.
As a comparison, Canadian health authorities have shared a risk-based system that tells people how health risks change with how much alcohol they drink:3
This shows a clear scale of risk — from no drinking at all to higher risk — so people can see how their drinking might affect their health.
In the U.S., the removal of drink-specific targets leaves American adults without clear numbers to guide their daily drinking choices. Some healthcare professionals find this to be less helpful for preventing harm.
If you choose to drink alcohol, these guidelines mean it’s important to:
In other words, health experts still agree that drinking less is better for your health — even if the exact wording and approach are changing. Learn more about alcohol, its relationship to cancer and other health risks, and how to reduce the harms around drinking in our Alcohol Resource Center.
SOURCE: https://drugfree.org/article/new-u-s-alcohol-guidelines-2025-2030-why-some-doctors-are-concerned/
As the federal government begins to loosen restrictions on cannabis, a new study found that removing legal barriers to cannabis use may reduce daily opioid use and, thus, the risk of opioid-related overdoses among people who inject drugs
Legalizing cannabis for both medical and recreational use may lead to a decline in daily opioid use among people who inject drugs in the United States, according to a new study led by a Boston University School of Public Health researcher (BUSPH).
Published in the journal Drug and Alcohol Dependence, the study found that US states that legalized marijuana for medical and adult recreational use saw a 9-to-11-percentage-point decline in daily opioid use among this population, compared to states that legalized marijuana for medical use only.
While the harms and benefits of cannabis use and cannabis reform continue to be debated on the national stage, these findings highlight one major potential advantage of widespread access to marijuana: this increased access may enable people to substitute their use of the unstable and toxic opioid supply with comparatively safer cannabis and, thus, lower their chances of experiencing opioid-related harms or dying from an overdose. In the US, opioids contribute to more than 75 percent of fatal drug overdoses.
The study was published on the heels of a significant shift in US drug policy that will indeed lower restrictions on cannabis. Last December, President Donald Trump signed an executive order to downgrade cannabis from a Schedule 1 classification (assigned to drugs such as heroin and ecstasy) to a Schedule 3 classification, which refers to drugs that pose minimal to moderate risk of physical or psychological dependence. Nearly all US states and Washington, DC have legalized cannabis for medical use, while 48 percent of states allow cannabis for adult recreational use.
People who inject drugs are part of a population that is at the epicenter of the opioid crisis in America, and they stand to benefit the most from policies that increase access to cannabis. By focusing on this group, the study builds upon past research on cannabis use and opioid mortality that has primarily examined the general population—which has a lower risk of experiencing opioid-related harms—with mixed results.
“The magnitude of decrease in opioid use that we observed among a population that is experienced with opioid use and likely to experience unpleasant withdrawal symptoms after reducing this use is very profound and important,” says study lead and corresponding author Dr. Danielle Haley, assistant professor of community health sciences at BUSPH.
The takeaway, she says, is that creating a safe and regulated supply of a substance is a valuable overdose prevention tactic because it can reduce use of non-regulated and more dangerous substances. “Legalized cannabis tends to be higher quality and more potent. As these products become more available and cheaper, people might be able to reduce their opioid use even without increasing how often they use cannabis.”
For the study, Dr. Haley and colleagues utilized data from the Centers for Disease Control and Prevention’s National HIV Behavioral Surveillance, including self-reported use of cannabis and non-medical opioid use among within the last 12 months among nearly 29,000 people who inject drugs, comparing data from states that did not legalize cannabis, legalized it for medical use only, or legalized it for both medical and adult recreational use. The data spanned 13 states in four waves: 2012, 2015, 2018, and 2022.
The decline in opioid use was equivalent across all racial and ethnic groups, as well as among males and females.
“This study adds to a growing body of evidence that sensible changes to our outdated drug policies can have a positive health impact, especially among some of our most vulnerable neighbors,” says study coauthor Dr. Leo Beletsky, professor of law and health sciences at Northeastern University.
The team did not observe overall links between cannabis legalization and daily cannabis use, but cannabis use did increase by five percentage points among White participants living in states that transitioned from no legalization to legalizing cannabis for medical use only. This increase among White participants could reflect long-standing racial inequities in healthcare that make it easier for White people to navigate health systems and services than people of other races, the researchers say.
Understanding how policies related to substance use benefit the health of people who use drugs is essential for effective cannabis reform.
“What this study shows is the potential impact of decriminalization paired with access to a regulated supply,” says Stephen Murray, adjunct clinical assistant professor of community health sciences at BUSPH, who is also an overdose survivor and former paramedic with expertise in overdose prevention. Murray was not involved in the study. “When legal barriers are removed and people have safer alternatives available, we see meaningful reductions in daily opioid use—even among people with long histories of injection drug use. That’s a powerful signal.”
But the findings also serve as a reminder that the design and implementation of these policies matter, he says. “Commercialized access to cannabis does not benefit all communities equally, and without intentional equity-focused policy, longstanding racial disparities in healthcare access and criminalization can persist even under legalization.”
The researchers say future research should further investigate links between legal medical and recreational cannabis and reduced opioid use, as well consider benefits in other areas, such as a reduction in cases of blood-borne infections through injection.
The study’s senior author is Dr. Hannah Cooper, Rollins Chair of Substance Use Disorders Research and professor of behavioral, social, and health education sciences at Emory University’s Rollins School of Public Health.
**
About Boston University School of Public Health
Founded in 1976, Boston University School of Public Health is one of the top ten ranked schools of public health in the world. It offers master’s- and doctoral-level education in public health. The faculty in six departments conduct policy-changing public health research around the world, with the mission of improving the health of populations—especially the disadvantaged, underserved, and vulnerable—locally and globally.
SOURCE:
by Deborah Brauser, Medscape Medical News – January 16, 2026
Researchers have identified the specific number of weekly delta-9-tetrahydrocannabinol (THC) units beyond which the risk for cannabis use disorder (CUD) increases.
Using standard THC units — defined as 5 mg of THC per unit — the investigators found that consuming more than 8.3 units per week among adults (about 41 mg of THC) and more than 6.0 units per week among adolescents (about 30 mg of THC) represented the optimal cutoffs for increased risk for any CUD.
Higher thresholds — 13.4 units per week for adults and 6.45 units per week for adolescents — were associated with the risk for moderate-to-severe CUD. The UK study, which included adults and teens, showed the accuracy of using weekly standard THC units to identify CUD was high across all models assessed.
Lead author Rachel Lees Thorne, MD, Addiction and Mental Health Group, Department of Psychology at the University of Bath, Bath, England, noted that 8 units per week equate to approximately 0.33 g of herbal cannabis on the UK market.
“This will likely be a lower amount than people who use cannabis regularly would typically consume and highlights that CUD can occur even with relatively lower levels of consumption,” Thorne told Medscape Medical News.
She added that although the findings may not be generalizable to other settings where cannabis products and use patterns differ, the investigators hope that framing use in THC units could help clinicians have more informed conversations with patients and better track cannabis-related behaviors.
The investigators also noted that theirs is the first study to estimate risk thresholds for CUD based on standard THC units mirroring the way alcohol units are used to calculate higher risk for drinking.
The findings were published online on January 12 in Addiction.
Risk Threshold
About 22% of individuals who use cannabis go on to develop CUD, a pattern of use that leads to clinically significant distress and/or impairment. The investigators noted that in the UK, cannabis use is cited as a problem drug by 87% of patients younger than 18 years who are in drug treatment programs.
A paper published in 2019 proposed that in the US, a “standard THC unit” should be set at 5 mg of THC across all cannabis products and methods of administration.
In 2021, NOT-DA-21-049: Notice of Information: Establishment of a Standard THC Unit to be used in Research the US National Institutes of Health (NIH) agreed, defining a standard THC unit as “any formulation of cannabis plant material or extract that contains 5 mg of THC.” In its announcement, the NIH added that the definition would apply to any future applications proposing research on cannabis or THC.
In the current study, the investigators used data from the observational CannTeen study of 65 adults aged 26-29 years (54% men) and 85 teens aged 16-17 years (56% girls) from London who reported using cannabis at least once during the 1-year study period.
The Enhanced Cannabis Timeline Followback was used to estimate mean weekly THC units by assessing quantity, frequency, and potency of consumed cannabis. A diagnosis of CUD was assessed using the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, with “any CUD” describing a composite of mild, moderate, or severe versions of the condition.
Receiver operating characteristic curve models were used to determine how well weekly standard THC units could distinguish between no CUD and either any CUD or moderate/severe CUD.
Results showed an area under the curve (AUC) of < 0.7 for all models assessing discrimination accuracy of weekly standard THC units on CUD.
For determining no CUD from any CUD, the AUC was 0.79 in the adult-only model and an “outstanding” 0.94 for adolescents. The AUCs were 0.82 and 0.94, respectively, for determining no CUD from moderate/severe CUD.
The optimal risk cutoffs for any CUD were 8.3 units of THC per week for adults and 6.0 units per week for adolescents; for moderate/severe CUD, the optimal risk thresholds were 13.4 and 6.45 units per week, respectively.
Measuring cannabis use with standard THC units “appears to show good discrimination accuracy of [CUD] at different severities and in different age groups,” the investigators wrote.
“Safer levels of cannabis use, defined by low weekly standard THC unit consumption, could be recommended in lower risk cannabis use guidelines,” they added.
‘A Much Needed Start’
In an expert roundup by the Science Media Centre, Marta Di Forti, MD, PhD , Institute of Psychiatry, Psychology & Neuroscience at King’s College London in London, England, noted that using this type of standardized measurement could become an “important tool” in both research and clinical settings — in about the same way standardized alcohol units have become.
However, “it is important to remember that cannabis, unlike alcohol, does not contain only one active ingredient but over 144 cannabinoids,” said Di Forti, who was not involved in the current research.
Still, THC units are, “undoubtedly, a very important and much needed start,” she added.
David Nutt, DM, Edmond J. Safra Professor of Neuropsychopharmacology and director of the Neuropsychopharmacology Unit in the Division of Brain Sciences – Faculty of Medicine at Imperial College London in London, noted in the roundup that the analysis provided a “welcome update” on recreational THC risks that can lead to dependence.
“What needs to be done now is to facilitate recreational cannabis users in determining exactly how much they are using to help them control their risk,” Nutt said.
“The best way would be through a regulated cannabis market with clear product quality and identification of unit amounts…plus a credible and honest educational program,” he added.
Source: Medscape Medical News
by the Advisory Council on the Misuse of Drugs (ACMD) – 28 January 2026
The ACMD has advised the government ketamine should remain a class B controlled substance, but that police forces and health care professionals must receive greater support to better identify, prevent and respond to ketamine‑related harms.
In January 2025, the government asked the ACMD to review the prevalence and harms of the misuse of ketamine. After examining the latest evidence, engaging with people with lived or living experience with the substance, consulting stakeholders, and reviewing academic research, the ACMD concluded ketamine should not be reclassified and should remain in class B.
In reaching its decision, the ACMD noted that the acute harms of ketamine – such as toxicity and deaths – align with its current class B status.
The ACMD also expressed concern about the growing use of high‑dose ketamine – described in some cases as “chronic”- and the long‑term harms associated with it.
However, as these harms were established in the 2013 ketamine assessment, the group focused its discussions on identifying new and emerging risks.
The ACMD report highlighted that many acute harms experienced by ketamine users are likely to be significantly influenced by using other drugs at the same time, and that reclassifying ketamine in isolation would unlikely reduce prevalence or misuse.
Individuals with personal experience of ketamine use and harms who contributed to the review said they did not believe upgrading ketamine to class A would reduce its use. Health and social care professionals similarly, largely, voiced opposition to reclassification.
Ultimately, the ACMD concluded that a public health‑centred approach is essential for reducing ketamine-related harms. This approach requires co-ordinated action across public bodies, health services, and community organisations.
The ACMD Chair Professor David Wood said in relation to the report:
The ACMD report highlights the need for a ‘whole system approach’ through its recommendations to tackle issues related to ketamine use, as no single recommendation is sufficient to do this alone.
The ACMD’s recommendations are outlined in full in their report. This includes recommendations on classification, improving treatment of ketamine-related harms, international control, intelligence gathering, education and training, harm reduction and research.
Source: https://www.gov.uk/government/news/acmd-announces-decision-on-the-classification-of-ketamine
by Jan Hoffman, NY Times – 15.12.2025
Medetomidine, a veterinary sedative, mixed into fentanyl has sent thousands to hospitals, not only for overdose but for life-threatening withdrawal. It is spreading to other cities.
Joseph is newly in recovery from fentanyl mixed with medetomidine, a veterinary sedative. Philadelphia’s hospitals are strained by cases of medetomidine withdrawal, which have life-threatening symptoms.
Around 2 a.m., Joseph felt the withdrawal coming on, sudden and hard. He fell to the floor convulsing, vomiting ferociously. The delirium and hallucinations were starting.
He shook awake his friend, who had let him in earlier to shower, wash his clothes and grab some sleep. “Do you have a few dollars?” he pleaded. “I have to get right.”
The friend, a community outreach worker who had been trying for years to get him into treatment, looked up at him standing over her raving and unfocused.
“Either leave or let me call an ambulance,” she demanded.
At 34, Joseph (who, with his friend, recounted the evening in interviews with The New York Times) had been through opioid withdrawals many times — on Philadelphia streets, in jail, in rehab. But he had never experienced anything as terrifyingly all-consuming as this.
A new drug has been saturating the fentanyl supply in Philadelphia and moving to other cities throughout the East and Midwestern United States: medetomidine, a powerful veterinary sedative that causes almost instantaneous blackouts and, if not used every few hours, brings on life-threatening withdrawal symptoms.
It has created a new type of drug crisis — one that is occasioned not by overdosing on the drug, but by withdrawing from it.
Source: https://www.nytimes.com/2025/12/15/health/medetomidine-withdrawal-symptoms-treatment.html?
A new remote service has launched in Quebec to help prevent drug overdoses, offering callers access to counselors by phone or video in a province grappling with rising overdose deaths.
Quebec’s overdose crisis has reached alarming levels. A report from the province’s institute for public health shows there were 645 drug overdose deaths in 2024 alone, with projections for 2025 expected to exceed 600.
Drugs: Help and Referral recently introduced the Remote Service for Overdose Prevention (RSOP) to provide immediate support for those at risk.
“In Canada, we’ve seen a decrease of overdoses, in Quebec, we’ve seen the opposite!” said David Galipeau, assistant coordinator at RSOP.
RSOP counselors follow a structured approach, explaining rules to callers, obtaining consent to contact emergency services if necessary, assessing overdose risk, providing wellness checks when there’s no immediate danger, and deleting personal information once the call ends to maintain anonymity.
“Here is really a support,” said Galipeau. “So the person could just use substances completely in silence and will just be there and monitor and see if the person is still well and then punctually just check up on the person. We stay on the phone throughout the entire time. But sometimes, the person just wants to talk about what they’re feeling. Sometimes, it can bring out some emotions and stuff like that. Then we can intervene and we can support those types of cases. But the person can choose the level of which, the support that they get from our team.”
Counselors emphasize that the service is not about stopping drug use but preventing fatal overdoses.
“We’re not there to tell them what to do, we’re not there to stop them from using the drug, we’re not asking them to stop, we’re just asking them to do it with someone, to not do it alone,” said Karelle Chevrier, addiction counselor at RSOP.
Officials note that most overdose-related deaths in Quebec occur when people use drugs alone at home, which significantly increases the risk of a fatal outcome.
“Drug usage in general is very stigmatized in society, and some people, due to that stigmatization and self-stigmatization as well, experience loneliness,” said Galipeau. “It leads them to use substances alone in their house or elsewhere in the city in secluded areas.”
“The danger when we do it alone is so high and we just don’t want people to die basically so just call us to do it with us and we won’t judge you,” added Chevrier. “We’ll be there for you and we’re not going to tell you what to do.”
After the pilot project launched in June 2025 proved successful, RSOP has grown to nearly 30 employees handling 120 to 160 calls a day, with recent spikes reaching 200 daily calls.
“Frequency is slowly going up but it’s more the number of different people that is becoming bigger faster and also we did lose some of our callers because they ended up going to our other program so they used with us and then they stopped using and now they moved on to the regular line where they can talk about how they want to keep sober and they want to stay sober and they want to go to therapy,” said Chevrier.
The service is free, confidential, bilingual, and available seven days a week from 11 a.m. to 2:30 a.m. Callers can connect with an RSOP counselor by contacting Drugs: Help and Referral at 1-800-265-2626 and choosing option 2.
Source: https://montreal.citynews.ca/2026/01/25/quebec-launches-remote-service-drug-overdoses/
Published by Michigan State University College of Human Medicine:
Michigan State University College of Human Medicine. (2025). At least 1 in 6 pregnant Michigan women uses cannabis. MSUToday. https://humanmedicine.msu.edu/news/2025-at-least-1-in-6-pregnant-michigan-women-uses-cannabis.html
Marijuana use among pregnant women has exponentially increased over the last 20 years. According to the American College of Obstetricians and Gynecologists (ACOG), pregnant women, especially those from high-income countries like the United States, have reported use ranging from 3.9% to 22.6%. This change in the landscape of substance use is observed in states like Michigan where both medical and recreational marijuana are legal. As access expands and perception shifts, researchers are racing to understand the number of pregnant women using marijuana and what factors shape that decision.
A recent study from the University of Michigan analyzed data of self-reported marijuana use and urine toxicology testing from 1,100 mothers in Michigan between 2017 and 2023, finding that 1 in 6 pregnant mothers used marijuana and in some parts of the state, that number is as high as 1 in 4.
Other key findings include:
· 25% reported using marijuana 3 months prior to becoming pregnant
· 12.3% self-reported using marijuana while pregnant
· 13.3% tested positive from urine toxicology testing
When self-reported use was considered together with urine toxicology results, the prevalence reached 16.8%, substantially higher than the national average of 9.8%. This study also found that single pregnant individuals, those with lower educational attainment, individuals who presented with symptoms of depression, or who had a history of Adverse Childhood Experiences (ACEs) had a higher likelihood of prenatal marijuana use.
Why are pregnant women turning to marijuana?
· Perceived safety: nearly 1 in 5 pregnant women believed that weekly marijuana use poses “no risk”
· Affordability: Michigan’s cannabis market is one the largest in the country, with prices dropping from ~$267 to $65/ounce in 2025
· Symptom relief: 81.5% reported using it to relieve stress, anxiety
· Ease of acquisition: 91.7% of pregnant users said that it was easy to obtain
The increased prevalence of marijuana use discovered in this and many other studies, suggest that many pregnant individuals may not fully understand the risks or may be using marijuana for symptom relief without the guidance of their healthcare provider.
To learn more about the risks of marijuana use during pregnancy and parenthood, visit marijuanaknowthetruth.org/marijuana-and-pregnancy for science-based resources, including fast facts, videos, and the latest research.
Source: Drug Free America Foundation | 333 3rd Ave N Suite 200 | St. Petersburg, FL 33701 US
While serving a three-year prison sentence for meth trafficking, Matewood Gerald got the call that she’d soon be a grandmother.
Gerald started abusing drugs when she was just 13, and she says everyone in the small town of Irvine has seen her at her worst. But she had to become the best version of herself for her granddaughter.
“I would lay there and think, is she gonna like me? Am I going to be perfect whenever I get out?” Gerald says.
Less than five years later, she is a peer support specialist with Mercy Health Marcum and Wallace Hospital in rural Irvine, Kentucky. It’s the only hospital serving a four-county region, including Estill County. In this role, she and other medical professionals meet with people struggling with active addiction – people who almost always recognize her – and ensure they have clean supplies and are in a safe environment. They always offer rehabilitation services for anyone who’s ready.
Harm reduction measures, like syringe exchanges and narcan distribution, are gaining strength in Estill County. It became a state-certified ‘Recovery Ready’ county last month. The Irvine city council prohibited syringe exchange in 2020, so hospital officials and the Estill County Health Department found creative ways to reach people in active addiction, including a mobile clinic.
“It has not always been popular in our area. Actually, just about six months ago, [syringe exchange] wasn’t even allowed in the city limits,” says Trena Lynn Stocker, president of Mercy Health Marcum and Wallace Hospital in Irvine, Kentucky. “We are now garnering support at the city level. We didn’t always have that. We had a police chief that, at one point, if you had fentanyl testing strips, he was going to get you for paraphernalia.”
Across all of Kentucky, too, harm reduction is gaining traction. More than 30 of its counties are deemed ‘recovery ready,’ signifying they run accessible drug and alcohol abuse programs. More than half of the state has implemented harm reduction protocols. These numbers encourage the idea that the Commonwealth is taking steps to protect those battling addiction.
Estill County ranked fifth out of Kentucky’s 120 counties for drug overdose deaths per 100,000 residents in 2024. But that’s an improvement – Estill had the highest rate of overdose deaths statewide in both 2021 and 2023.
These practitioners explain that harm reduction, which brings resources and life-saving materials to people already abusing drugs, is helping save lives in rural Kentucky. Yet, it doesn’t get to the root cause of drug abuse. That’s why they showed up on a rainy Tuesday evening to the Estill Development Alliance’s second Parent Cafe.
It’s one piece of the Estill Pathfinder Initiative Coalition (EPIC), a holistic approach to drug prevention in the local youth that’s inspired by an evidence-based model from overseas. Officials say the Development Alliance supports this programming through its unique development model, focused on being a one-stop shop for community health and wellbeing.
“GIVE THEM SOMETHING TO DO”
Since 1983, the D.A.R.E program has been the standard for drug prevention across America. Police officers give lecture-style presentations to elementary schoolers about the dangers of drug and alcohol use, encouraging them to ‘just say no.’ D.A.R.E does not address root factors in individual communities or teach its students how to be safe if they do engage in drugs. Critics say that’s why the program has been ineffective. Yet, the curriculum is still actively used in many Kentucky schools.
Suzanne Waite has worked in the Estill County school system for years, so she saw these trends firsthand and sought out a different approach. Two years ago, she came across a better fit for residents’ needs, which inspired her to team up with the Estill Development Alliance and create EPIC.
The Icelandic Prevention Model was first conceptualized in the 1990s, when rates of drinking and drug use among European teenagers were at their peak. About 23% of 15- and 16- year olds in Iceland had reported smoking daily, and 42% had drank alcohol in the previous month.
In response, the Icelandic government decided to implement new regulations for its youth. A mandatory country-wide curfew for children under 16 was set, though that facet of the model hasn’t gained much traction outside of its home country.
What did stick: parental involvement and bolstering recreational programs for students. When Waite took on leadership of EPIC this year, that’s what she honed in on.
“It’s looking at your community, coming together to address this issue, and looking at things that are more preventative upstream”, Waite says.
The Icelandic prevention model has been adopted by organizations in 19 countries, though EPIC is one of the few official partners in the United States. The process starts with the same in-depth survey that the Icelandic Model uses, provided by a global group called Planet Youth.
Waite’s learned they can’t always take survey responses at face value, as many teens start off afraid to admit their own drug use.
“They do ask the questions in multiple ways, like many tests. It’ll say, ‘have you engaged in drugs?’ [and] 23% of them might say yes,” Waite explains. “But amazingly, 85% know a friend that has.”
She says it’s no wonder why kids turn to substance use instead of recreation. The small town of 2,000 has limited infrastructure; at first glance, it can be hard to find variety in activities, especially for kids.
“There’s no local movie theater. There’s no local bowling alley. There’s no local skating rink. You’ve got to go out of town for all of those things. And there’s not a community center that would just be [for] fun activity,” Waite says. “And then, there’s no public transportation.”
Many of these kids can only congregate with each other at school. So that’s where Waite started: a new leadership club at Estill County High School. In EPIC’s first two years, students launched and took full charge of the “Council of Engineers Leading for Tomorrow.”
“Our schools’ mascots are the engineers,” Waite explains. “Last year’s group, they did a color run to raise some funding [and] raise some awareness … Currently, we got a grant through the Kentucky Retail Survey Project. And we went out into the environment and did an environmental scan of the different tobacco retailer outlets here.”
These students are learning about environmental factors that correlate to certain shops selling tobacco products to underage customers. Another advantage of this ‘environmental scan’ is that they are eagerly engaging with the Estill County community and local leadership.
“We actually got them on the agendas for four different groups in the county,” Waite says. The club was signed up to present this environmental scan at the local city council, fiscal court, school board and Estill Development Alliance’s chamber meeting. “[I told them], ‘OK, you don’t have to do all four. But these are the adults that would like to hear from you and what you found out.’ And they said, ‘we’ll do them all!’”
It gives young students a sense of accomplishment and involvement, especially hard to find in a rural county, she says. That’s what resonated most with EPIC when its leaders learned about the Icelandic Prevention Model from Planet Youth.
“Drug abuse ends up being because something is broken. So, what is broken that you’re trying to fix?” Waite says. “We’re trying to let you see that you don’t have to be dependent upon some substance, to get that feeling of, ‘I feel good about myself,’ if you can get that from people in your life that do care about you.”
EPIC is planning a lot more activities; through a grant with Operation UNITE, she anticipates hosting a youth talent show in the spring, where local musicians will mentor students hoping to perform. And last year, the CELT club began working with Irvine City Council to build a city park on a vacant parcel of land in town.
In the next two years, officials with the Estill Development Alliance also hope to convert their facility into a gathering spot for youth to drop in as they wish. Once that’s complete, their offices will provide yet another service to their community.
ESTILL DEVELOPMENT ALLIANCE
EPIC is one of multiple divisions within the Estill Development Alliance. Even within such a small town, Estill Development Alliance communications director Payten Rice says, the Chamber of Commerce itself is bustling.
“We have about 104 businesses that are members of our chamber that serve to support our local economy. We always are doing events and fundraising in ways [so] businesses can get involved with the community,” Rice says.
In most cases, the local chamber of commerce is more connected to the city or county municipal government, often independent organizations that benefit from government support. The Estill Development Alliance instead hosts the Chamber of Commerce, which Rice says helps the organization avoid any sort of bias.
“It’s a working relationship, but we’re pretty independent,” Rice explains.
The money invested into the Chamber of Commerce gets a positive return; those funds, combined with grants, very limited local government contributions, and personal donations, have kept the Estill Development Alliance’s lights on for more than 20 years.
In turn, it powers the organization’s other divisions, like the outdoor-recreation based Estill County Action Group, the five-county regional leadership group LEAP, and several philanthropic and civic engagement initiatives. One division, the River City Players, leads a community theatre group and supports the revitalization of the local historic theatre.
“There’s not a lot of development alliances that have a very old movie theater that they’re rebuilding. And let me tell you, that’s a passionate group of people,” says Stocker. In addition to her role at Mercy Health, she is also a board member of almost every Estill Development Alliance division.
Stocker explains these branches may seem unrelated, but they all serve the purpose of strengthening the infrastructure and social health of their town. This further contributes to the mission of EPIC.
“We have it here,” Stocker says. “You just have to have some ownership in figuring out what is going on in your community.”
She says Estill County has enough economic momentum; it will take a combination of the preventative work from EPIC and Mercy Health’s harm reduction to help this money go toward local businesses instead of drugs.
“It goes hand in hand because of the amount of money that is being wasted on drugs by community members and the tax on the healthcare system,” Stocker says. “Nobody can get a job – or the money.”
GETTING PEOPLE IN THE DOOR
The Estill Development Alliance’s new Parent Cafe program is meant to provide a quiet space for parents to learn about warning signs of early drug addiction in their kids; the event was catered, and childcare was ready. Instead, the library basement sat empty, aside from the EPIC coordinators and Mercy Health members.
That’s a problem for drug awareness and prevention events in any place, Stocker says. Even when hosting events for the community’s only hospital, she says, attendance for these addiction-related events can be extremely volatile. Just last month, she saw it first hand.
“On a miserably rainy evening, [we] had over 160 people come to the recovery rally. But then a week later, we have the memorial event for those that we’ve lost this year [to addiction], and we had six show up,” Stocker says.
EPIC has great participation in the school system through the CELT club, and Waite and Stocker consistently secure new grants– soon they’ll have customized T-shirts, the youth talent show, and more recreational programs for kids to get immersed in.
The next challenge is getting their movement off the ground. EPIC is faced with a community that lacks public transportation and relies on social media algorithms to get the word out about local events. Leaders are working vigorously to build community trust – which is especially difficult in a small town, they explain – and get the word out.
EPIC’s current goal: Find the best way to get people, even adults, excited and ready to participate.
“I wish I knew,” Waite laughs. “[I] sat down with the board members, talked to them about, hey, what else can we be doing … what else have I not thought of?”
According to the “2026 Road Traffic Act” released by the National Police Agency on the 28th, people who have driven drunk twice or more within the past five years must install a DUI prevention device on their vehicle when they re-acquire their license after a two-year disqualification period.
The device prevents the vehicle from starting at all when alcohol is detected. The cost of installation is about 3 million won, and the police said they are in talks with the Korea Expressway Corporation to allow rental.
In addition, driving without installing preventive devices could result in up to a year in prison or a fine of up to 3 million won. It is also possible to revoke a driver’s license.
If another person is caught driving after avoiding alcohol detection by breathing instead, he or she will be sentenced to up to three years in prison or fined up to 30 million won.
According to the police, about 40% of drunk drivers have recidivism within five years. The police’s plan is to “block the source” as a device to prevent the possibility of such recidivism.
When drug driving is caught, it has been raised from “imprisonment of up to three years or a fine of up to 10 million won” to “imprisonment of up to five years or a fine of up to 20 million won.” A new provision has also been established that will result in “imprisonment of up to five years or a fine of up to 20 million won” for non-compliance with drug measurements.
The issuance of Type 1 licenses will also become stricter. Previously, if only the seven-year accident-free requirement was met, type 2 driver’s license holders could obtain type 1 licenses only by aptitude tests. Starting next year, you can get a type 1 license after an aptitude test only if you prove your actual driving experience with a certificate of auto insurance.
The standard for calculating the renewal period of a driver’s license will be changed from the existing annual unit (January 1st to December 31st) to six months for each individual’s birthday. The related system will also be adjusted so that trainees can legally train on the road to the places and courses they want without visiting the driver’s license academy in person.
Kim Ho-seung, director of the National Police Agency’s Living Safety Transportation Bureau, said, “We will strongly crack down on activities that threaten the lives of the people on the road and actively improve daily inconveniences.”
Opening Statement by National Drug Prevention Alliance – 11 Jan 2026:
This article, forwarded to NDPA by DWI’s Maggie Petito, is included in NDPA’s website to complete the contemporaneous picture around this extraordinary initiative by President Trump … it is noteworthy that the three main protagonists of this proposal were a CEO of a marijuana company which has donated $750,000 to the (presidential?) inauguration; a police sheriff who has become a supporter of legalising marijuana for recreational use (not just for medicinal use); and a long-term friend of the President in the Mar-a-Lago membership body. It has to be said that this whole episode smells of interest-led lobbying gaining what it wanted, rather than any research-based development of drug policy – this may be an uncharitable conclusion, but time will tell where the truth lies.
From: drug-watch-international – On Behalf Of Maggie Petito – Sent: 28 December 2025
Subject: The Wall Street Journal’sPiece12-28-25
Paraphrasing an article by The Wall Street Journal’s Josh Dawsey, in a front-page story (included below) Maggie Petito informs on details of how a concerted lobbying push by a cannabis CEO, a Florida sheriff and a Mar-a-Lago member helped persuade the president …
<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<>>>>>>>>>>>>>>>>>>>>>>>>>>>
After a two-hour Oval Office debate about marijuana in December, President Trump overrode some on the religious right, White House aides and senior Republican lawmakers and decided to reschedule the green leaf as a lower-level drug.
Trump watched as Kim Rivers, the CEO of Trulieve, a Florida-based marijuana company, Gordon Smith, a Florida sheriff, and Howard Kessler, a Mar-a-Lago member and longtime Trump friend, argued the president should reschedule marijuana, according to people with knowledge of the meeting… The decision to reschedule marijuana from a Schedule I drug to a Schedule III drug followed an aggressive 18-month lobbying campaign by Rivers. The CEO and her company cut large checks to Trump’s political groups, attended at least three fundraisers, repeatedly raised the issue with White House aides and hired influential lobbyists. Rivers’s efforts delivered the marijuana industry one of its biggest victories. In addition to making medical research easier, the order is expected to eliminate tax burdens that have made profitability an uphill battle for many cannabis companies. Cannabis executives say the order will help normalize the business environment for marijuana sellers and improve access for buyers… Rivers first met with Trump on marijuana in summer 2024, when she cut a seven-figure check to a political group helping him, people familiar with the meeting said. Trump then supported a referendum allowing recreational marijuana in Florida… Rivers hired lobbyists close to Trump, including Brian Ballard and Nick Iarossi. The lobbyists pitched conservatives to write positive op-eds about the marijuana push, among other things, and generate support within the administration. White House officials described Rivers as particularly aggressive in making her case. Trulieve gave another $750,000 to the inauguration. After Trump indicated to Rivers and other donors at a New Jersey fundraiser this summer that he would follow through on rescheduling the drug, industry officials were hopeful. That fundraiser was billed at $1 million a guest… A follow-up meeting was scheduled, and Rivers asked Gordon Smith, the sheriff of Bradford County—a small county in northern Florida between Jacksonville and Tallahassee—to join her. She also brought two cancer survivors and a Duke University professor. Smith had introduced Trump at a rally about a decade ago and had become one of the first conservative sheriffs to endorse recreational marijuana use.
Inside the Oval Office, Trump talked with Kessler, a financial executive who has advocated for medical cannabis, and others about expensive properties in Palm Beach, donations to the White House ballroom and a golf course he wanted to renovate in Washington, Smith recalled. Trump gave opinions on appearances from daughter-in-law Lara Trump on Fox News and talked about Sylvester Stallone’s climbing trees and hurting his back… Trump reviewed polling on rescheduling and said he had heard from many people—including boxer Mike Tyson—that he should reschedule. He continually reiterated they were not legalizing it. Smith said Dr. Mehmet Oz, who leads Medicaid and Medicare, Health Secretary Robert F. Kennedy, and White House chief of staff Susie Wiles also watched the debate… Smith’s brother, a military veteran, had been helped by medical marijuana, he said, and he believed it was safer than alcohol and other substances. The sheriff’s concern, he said, was fentanyl-laced marijuana that killed people. When Speaker Johnson called in, the president put him on the phone with the sheriff, who tried to persuade Johnson. `It’s a gateway drug,’ Johnson argued, according to the sheriff. Smith said Johnson was a `nice guy’ and he answered Johnson’s questions. Another person familiar with the meeting said Johnson cited studies and research. Oz argued for rescheduling as Schedule II, Smith and others said. Johnson declined to comment through a spokesman.”
Again from Dawsey: “…the order is expected to eliminate tax burdens that have made profitability an uphill battle for many cannabis companies. Cannabis executives say the order will help normalize the business environment for marijuana sellers and improve access for buyers.”
We do not have a fulsome roster of who or what these largesse-receiving “companies” are or do. “Normalizing” differing from “legalizing” loses its distinction when financial access for little known companies or rackets gain tax reductions and financial access, forbidden to similar rackets sometimes called vice or “businesses” and crypto/bitcoin’s opaque/unaccountable systems seeking false junctures with sound monetary structures. We do not know whose polling was applied. I do not check Trulieve’s financial statements.
THE WALL STREET JOURNAL ARTICLE: by Josh Dawsey Dec. 27, 2025
How Trump Became the Unlikely Champion of Easing Marijuana Restrictions – Concerted lobbying push by a cannabis CEO, a Florida sheriff and a Mar-a-Lago member helped persuade the president
The president agreed to make marijuana a Schedule III drug. Evan Vucci/AP
President Trump decided to reschedule marijuana as a lower-level drug after an Oval Office debate, overriding some Republicans and religious right figures.
After a two-hour Oval Office debate about marijuana in December, President Trump overrode some on the religious right, White House aides and senior Republican lawmakers and decided to reschedule the green leaf as a lower-level drug.
Trump watched as Kim Rivers, the CEO of Trulieve, a Florida-based marijuana company, Gordon Smith, a Florida sheriff, and Howard Kessler, a Mar-a-Lago member and longtime Trump friend, argued the president should reschedule marijuana, according to people with knowledge of the meeting. It was time to open the door for medical research and improve access to cannabidiol products, they argued.
House Speaker Mike Johnson (R., La.) on speakerphone urged the president against the decision and senior aides warned the move could be dangerous to some Americans.
After listening, Trump, a teetotaler who eschews alcohol and drugs, sided with the pro-marijuana camp and delivered the biggest softening of federal cannabis policy since U.S. states began legalizing recreational marijuana in 2012.
“It was a little surreal,” Rivers said in an interview.
The decision to reschedule marijuana from a Schedule I drug to a Schedule III drug followed an aggressive 18-month lobbying campaign by Rivers. The CEO and her company cut large checks to Trump’s political groups, attended at least three fundraisers, repeatedly raised the issue with White House aides and hired influential lobbyists.
Rivers’s efforts delivered the marijuana industry one of its biggest victories. In addition to making medical research easier, the order is expected to eliminate tax burdens that have made profitability an uphill battle for many cannabis companies. Cannabis executives say the order will help normalize the business environment for marijuana sellers and improve access for buyers.
“The president heard from many different people on this issue and ultimately felt it was the best policy and political decision to make for the country. On all issues, the president is the final decision maker,” said White House press secretary Karoline Leavitt.
Conservative and religious leaders, such as the Faith and Freedom Coalition’s Ralph Reed, had asked the White House not to reclassify the drug, saying it could be a gateway to other drugs and didn’t fit with the president’s agenda. Reed and allies argued medical studies had not shown health or medicinal benefits. Heidi Overton, a top aide on the conservative domestic policy council, repeatedly weighed in against it, including in the meeting where Trump made the decision, people with knowledge of the meeting said. Through a spokeswoman, she declined to comment.
Some White House officials, including deputy chief of staff James Blair, told Trump that many Republicans were opposed, and aides showed him a letter signed by 22 senators urging against it, White House officials said.
“The only winners from rescheduling will be bad actors such as Communist China, while Americans will be left paying the bill,” the senators wrote.
Leavitt, the White House spokeswoman, said that “it’s Blair’s job to convey to the president what the Hill thinks, and what the politics are, on every issue.”
For many months, the policy seemed on hold. Rivers first met with Trump on marijuana in summer 2024, when she cut a seven-figure check to a political group helping him, people familiar with the meeting said. Trump then supported a referendum allowing recreational marijuana in Florida. Trump also said on the campaign trail that he would reschedule the drug, but it wasn’t in his first slate of executive orders. Some in the industry grew frustrated, believing Trump’s staff was stalling.
Rivers hired lobbyists close to Trump, including Brian Ballard and Nick Iarossi. The lobbyists pitched conservatives to write positive op-eds about the marijuana push, among other things, and generate support within the administration. White House officials described Rivers as particularly aggressive in making her case. Trulieve gave another $750,000 to the inauguration.
After Trump indicated to Rivers and other donors at a New Jersey fundraiser this summer that he would follow through on rescheduling the drug, industry officials were hopeful. That fundraiser was billed at $1 million a guest. Behind the scenes, White House officials expressed frustration, people familiar with the matter said, and Trump waffled when publicly asked about rescheduling days later.
Rivers didn’t give up, and again came to a golf fundraiser for Sen. Lindsey Graham (R., S.C.) in November. She and Trump spoke briefly, and she asked for a White House meeting.
“When I’m there, it’s a natural conversation topic—he asks me about business and how things are going,” Rivers said of the fundraiser. “The president has been very consistent on this issue.”
Rivers’s efforts appeared to be bearing fruit when Trump invited her to the Oval Office to make her case. She was met in the Oval by Overton, who disagreed, and Trump didn’t make a final decision.
A follow-up meeting was scheduled, and Rivers asked Gordon Smith, the sheriff of Bradford County—a small county in northern Florida between Jacksonville and Tallahassee—to join her. She also brought two cancer survivors and a Duke University professor. Smith had introduced Trump at a rally about a decade ago and had become one of the first conservative sheriffs to endorse recreational marijuana use.
Inside the Oval Office, Trump talked with Kessler, a financial executive who has advocated for medical cannabis, and others about expensive properties in Palm Beach, donations to the White House ballroom and a golf course he wanted to renovate in Washington, Smith recalled. Trump gave opinions on appearances from daughter-in-law Lara Trump on Fox News and talked about Sylvester Stallone’s climbing trees and hurting his back.
Trulieve CEO Kim Rivers triumphed despite objections from some of those close to the president. Douglas R. Clifford/Zuma Press
“Some of the conversation was way above my pay grade,” Smith said. Kessler didn’t respond to requests for comment.
Trump reviewed polling on rescheduling and said he had heard from many people—including boxer Mike Tyson—that he should reschedule. He continually reiterated they were not legalizing it. Smith said Dr. Mehmet Oz, who leads Medicaid and Medicare, Health Secretary Robert F. Kennedy, and White House chief of staff Susie Wiles also watched the debate. Wiles left early. At one point, Trump zeroed in on Smith.
“He turned to me and said, ‘Sheriff, what do you think?’ ” Smith’s brother, a military veteran, had been helped by medical marijuana, he said, and he believed it was safer than alcohol and other substances. The sheriff’s concern, he said, was fentanyl-laced marijuana that killed people.
When Speaker Johnson called in, the president put him on the phone with the sheriff, who tried to persuade Johnson. “It’s a gateway drug,” Johnson argued, according to the sheriff. Smith said Johnson was a “nice guy” and he answered Johnson’s questions. Another person familiar with the meeting said Johnson cited studies and research. Oz argued for rescheduling as Schedule II, Smith and others said. Johnson declined to comment through a spokesman.
The president said Democrats should have rescheduled the drug “because it was really a Democratic issue.” The Biden administration started the process of reclassifying pot last year, but didn’t finish. After about two hours, Trump said he was going to reschedule the drug and said he wanted to post on Truth Social, the sheriff recalled. Trump said he wanted everyone on board.
“The lawyers and his staff, they started yelling, ‘No sir, you can’t yet; there’s a 30-day period, it’s gotta go through this and that,’ ” Smith said. “They had to stop him from posting.”
Trump then instructed the sheriff and staffers to go into another room and put together an executive order. Trump wanted to put the “real story of why we are doing this in the order,” Smith said.
“I was in awe of the whole thing,” he said.
Trump invited Smith to come back the next week and see him sign the order, but Smith said he couldn’t—he had to attend an execution in Florida that evening. Trump told others that Rivers had pushed him to do it, said people familiar with the matter.
Announcing the order from the White House podium on Dec. 18, Trump thanked Kessler, saying, “We have people begging for me to do this, people that are in great pain. I have probably received more phone calls on this, on doing what we’re doing.”
Source: www.drugwatch.org

The MTF survey is given annually to students in eighth, 10th, and 12th grades who self-report their substance use behaviors over various time periods, such as past 30 days, past 12 months, and lifetime. The survey also documents students’ perception of harm, disapproval of use, and perceived availability of drugs. The results were gathered from a national representative sample, and the data were statistically weighted to provide national numbers. The investigators collected 23,726 surveys from students enrolled across 270 public and private schools nationwide from February through June 2025. Students took the in-school survey via the web – either on tablets or on a computer.
For the fifth year in a row, use of most substances among teenagers in the United States has continued to hover around the low-water mark reached in 2021. Researchers detected a sharp decline in reported use of most drugs from 2020 to 2021. This substantial falloff was largely attributed to disruptions in drug availability and in the social lives of teens during the pandemic, when many were isolated at home with parents or other caregivers and spending less time with friends. The researchers also found that the percentage of teens currently abstaining from alcohol, tobacco, and nicotine use held steady at historically high levels.
Researchers maintain the slight increase in cocaine and heroin use warrants close monitoring. However, to put these current levels of use in context, they are leagues below what they were decades ago.
SAFE, Inc. is the only alcohol and substance abuse prevention, intervention and education agency in the City of Glen Cove. Its Coalition is conducting alcohol, tobacco and other drug use prevention awareness campaigns entitled, “Keeping Glen Cove SAFE,” to educate and update the community regarding alcohol, prescription and illicit drug use and its consequences. To learn more about the SAFE Glen Cove Coalition please follow us on www.facebook.com/safeglencove or visit SAFE’s website to learn more at www.safeglencove.org.
Source: https://patch.com/new-york/glencove/safe-gc-coalition-nida-reports-encouraging-news-regarding-youth-alcohol-substance
<drug-watch-international@googlegroups.com> on behalf of Maggie Petito – mlp3@starpower.net – 09 January 2026 13:47
This reportage derives from a UK newspaper item – published in the The London Telegraph on 09 January 2026 – -by Charles Hymas Home Affairs Editor and Meike Eijsberg Data journalist
Starmer accused of ignoring more significant safety issue while planning to cut drinking limit for motorists
Drugs are now a bigger factor in road deaths than alcohol, official figures show.
The number of deceased drivers who tested positive for drugs increased by 78 per cent, from 106 to 189, in the decade to 2023, according to the Department for Transport (DfT) and police data.
By contrast, the number of dead motorists with alcohol proved to be present in their system rose by 5 per cent in the same period, from 162 to 171.
Sir Keir Starmer, the Prime Minister, now stands accused of ignoring the bigger problem of drug-driving while planning to reduce the drink-driving limit, which critics fear will “strangle” struggling pubs.
The Government’s proposals have prompted a backlash from MPs and publicans, who say the move will put pubs under more pressure following an increase in business rates.
Britain lost an average of one pub each day in 2025, and industry bosses have warned that rising tax bills and wages, on top of higher energy costs, will drive hundreds more out of business.
The Telegraph has launched a campaign to save the nation’s pubs, calling on Labour to stop its assault on Britain’s locals, and to cut tax and red tape.
Ministers are now expected to announce a climbdown, saying they are working on relief measures to be announced in the coming days. But the about-turn relates to jumps in business rates for landlords, not the new drink-drive limit.
DfT figures show that the percentage of fatal collisions in which drink-driving was involved has been relatively stable over the past 10 years, at 13 per cent.
However, the proportion in which drug-driving played a role has doubled from 5 per cent in 2014 to 10 per cent in 2023.
While drug-driving convictions rose by 13.5 per cent in 2024 to 27,000, the number of drivers convicted of drink-driving offences fell by 6 per cent to 36,415.
Meanwhile, injuries from drink-driving incidents have significantly decreased since 1980, from around 20,000 annually to about 5,000 since 2020.
Despite this, the Government’s new road strategy proposes “taking tougher action on drink-driving” by reducing the legal limit of 80mg of alcohol per 100ml of blood to 50mg, or around a pint.
It would be the most significant reform to road safety laws since 1967, when the blood alcohol limit was first introduced.
Chris Philp, the shadow home secretary, said: “Labour are now proposing even more measures that will endanger country pubs.
“At the same time, the Government is completely failing to do more to address a more rapidly growing road safety issue – drug-driving. More drivers killed in a collision had drugs in their system than alcohol.
“The Government should prioritise toughening up on drug-drivers above measures which will strangle struggling country pubs.”
‘Further pressure’ on pubs
The British Beer and Pub Association warned that any toughening of measures on drink-driving would harm rural pubs in areas without public transport or reliable taxi services.
A spokesman said: “The pub sector continues to face huge challenges, so any additional policy measures that further impact trade will be of real concern to licensees, especially those in rural areas.”
Drug-drivers face similar penalties as those caught drinking, including a minimum 12-month driving ban and up to six months in prison for serious or repeat offences.
Limits for illegal drugs such as cannabis, cocaine, ketamine and heroin are set at extremely low levels, but not at zero, to account for accidental exposure.
However, Government-funded research has suggested that dangerous drug-drivers have been escaping prosecution – and putting lives at risk – because some police forces ration the number of testing kits issued to officers to just one a day.
The study, by the Parliamentary Advisory Council for Transport Safety, found there was a “geographical lottery” where the best-performing forces were catching 10 times more drug-drivers per head of population than the worst.
Drivers can also escape justice because of delays of four to five months in processing blood tests. Officers have only six months to prosecute. Dangerous driving penalties to be reviewed
The Government’s new road safety strategy proposes that there should be a review of penalties and mandatory training for drink and drug-driving offences.
It has also pledged to explore alternative processing and evidence collection for drug-driving to “improve speed of results, supporting more robust enforcement outcomes.”
A DfT spokesman said the strategy would “save thousands of lives by targeting the root causes of deaths, including the impact of both alcohol and drugs”.
They added: “We’re determined to crack down on drug-driving, and the strategy includes new measures to modernise how we tackle it, including new testing methods, and powers to suspend driving licenses for those caught under the influence.
“We do not expect the new limit to harm pubs; experience in Scotland shows such changes have minimal impact on local businesses while making roads safer.”
Source: Maggie Petito – mlp3@starpower.net
Muse Treatment Alcohol & Drug Rehab Los Angeles has published a new educational resource examining how opioid tolerance develops and why it plays a significant role in substance use disorder progression and treatment planning. The article, titled “How Does Opioid Tolerance Develop”, provides research-informed context for patients, families, and healthcare professionals seeking a clearer understanding of opioid-related risk, dependence, and recovery pathways.
According to the National Institute on Drug Abuse, opioid tolerance occurs when repeated exposure to opioids reduces the body’s response to the drug, leading people to require higher doses to achieve the same effect. This physiological adaptation is a central driver of escalating use and overdose risk. The Centers for Disease Control and Prevention reports that opioids remain a major contributor to drug-related mortality in the United States, with tolerance and dose escalation frequently cited in toxicology findings. Peer-reviewed research published in journals such as The New England Journal of Medicine further confirms that tolerance alters brain chemistry and reward pathways, making cessation more complex without structured treatment support.
The newly published resource outlines how tolerance develops at the cellular and neurological level, emphasizing that it is not a failure of willpower but a predictable biological response. This distinction is supported by guidance from the Substance Abuse and Mental Health Services Administration, which frames substance use disorders as chronic medical conditions requiring evidence-based care. By presenting opioid tolerance through a clinical lens, the article reinforces the importance of early intervention and medically appropriate treatment selection.
This educational release aligns with the clinical services at the Los Angeles location, where inpatient treatment programs are designed around evidence-based frameworks used in accredited addiction treatment facilities. Program information is available at Muse Treatment Los Angeles. Services include medically supervised care models that address alcohol and opioid use disorders through structured programming, including intensive outpatient alcohol rehab and partial hospitalization alcohol rehab. These levels of care reflect standards outlined by SAMHSA, which identifies continuity of care and treatment intensity matching as key predictors of positive outcomes.
Patients seeking care often come from across Los Angeles and surrounding communities, reflecting the regional need for accessible, medically grounded addiction treatment. People searching for drug rehab near me in LA frequently include residents from West LA, where proximity and flexible treatment scheduling influence engagement. Downtown LA is also represented among patients accessing services, highlighting the demand for structured care models that integrate clinical oversight with community-based recovery. East LA similarly relies on nearby treatment options that support consistent participation without extended travel.
The reach of care extends into neighborhoods such as Glendale,Westwood and Westwood Village, where patients often seek programs that balance privacy with evidence-based clinical support. Little Holmby and Holmby Hills are included as well, underscoring the role of localized treatment availability when families evaluate the best alcohol rehab centers and related services. Bel Air shows similar patterns, reinforcing the importance of geographically relevant care when people decide whether to initiate treatment and follow through.
National outcome data support the treatment approaches discussed in the article. The National Institute on Drug Abuse reports that relapse rates for substance use disorders are comparable to those of other chronic conditions, such as diabetes and hypertension, emphasizing that effective care focuses on long-term management rather than short-term detoxification alone. Programs offering partial hospitalization alcohol rehab and intensive outpatient alcohol rehab are well-positioned to support patients as they transition between levels of care, particularly when tolerance and withdrawal symptoms complicate recovery.
The article also contributes to broader public health education around opioid risk. The CDC notes that tolerance can lower perceived risk while increasing physiological danger, as higher doses strain respiratory and cardiovascular systems. Understanding this dynamic is critical for patients and families evaluating treatment options, particularly in regions with sustained opioid exposure.
Accreditation standards further inform the clinical framework reflected in the services described. Organizations such as The Joint Commission emphasize medication management, patient safety, and evidence-based treatment protocols as benchmarks for quality addiction care. Independent analyses have shown that accredited programs demonstrate stronger adherence to clinical guidelines and improved coordination between medical and behavioral health services.
As healthcare search trends continue to show rising interest in opioid tolerance, overdose prevention, and structured treatment pathways, educational resources grounded in third-party research play a critical role in informed decision-making. By publishing this article and integrating it within a broader continuum that includes intensive outpatient alcohol rehab and partial hospitalization alcohol rehab services, Muse Treatment reinforces the role of education as a foundation of effective addiction treatment.
The resource serves as a reference point for patients, families, and healthcare professionals seeking clarity on how opioid tolerance develops, while supporting broader efforts to reduce preventable harm and improve recovery outcomes through evidence-based care across Los Angeles and surrounding communities.
Source: https://markets.financialcontent.com/wral/article/pressadvantage-2026-1-1-opioid-tolerance-explained-in-new-educational-resource-published-by-muse-treatment
British Columbia’s overdose-prevention safer supply program underwent a significant shift Tuesday.
With a few exceptions, participants in the program will now need to ingest their prescribed alternatives to street drugs in front of a health-care professional—often a pharmacist.
It’s a change the opposition B.C. Conservatives say is an improvement, and an acknowledgment that safer supply isn’t really working.
“This is really just managing someone’s decline,” said Claire Rattee, the B.C. Conservative critic for mental health and addictions. “We don’t do this in any other area of mental health or medicine.”
The shift was announced in February, prompted by leaked documents confirming what critics had warned about and the NDP had disputed—that significant amounts of the prescribed alternatives were being diverted and sold on the streets.
“The government continues to paint this as a problem with bad actors in pharmacies, but the reality was that it was a government policy of giving out large quantities of highly addictive opioids,” said Elenore Sturko, the Independent MLA for Surrey-Cloverdale.
Sturko is the one who exposed the truth about diversion. She’s happy about the changes, but wants a public inquiry and more answers, including about the status of investigations into the dozens of pharmacies alleged to have enabled the diversion and how widespread it was.
“We need to have answers and clarity,” said Sturko on Tuesday. “Where is the accountability for those pharmacies that were under investigation?”
The latest stats show 150 lives lost to toxic drug overdoses in October.
Some worry Tuesday’s changes could actually add to those numbers, with street drugs becoming more convenient than prescribed alternatives.
“My concern is always that if people don’t go to get their prescription medications, then where will they go?” asked harm reduction advocate Guy Felicella.
The Health Ministry tells CTV News that investigations into the pharmacies began more than nine months ago and are ongoing. It says it remains committed to monitoring the program to ensure it’s working as intended to save lives in a crisis that’s already claimed more than 16,000 lives in nine years.
Source: https://www.ctvnews.ca/vancouver/article/critics-react-to-changes-to-bc-overdose-prevention-program/
The HOPI Substance Abuse Prevention Center reports great success with clients being successfully reintegrated as members of the community. Manager Bryan Humetewa says he has had the joy of seeing clients return to their homes, holding jobs and witnessing “the miracle” of being back with their children.
“Working with the community collaboratively is key, especially with limited resources,” he said.
The center works cooperatively with First Mesa Elementary School, Hopi Junior Senior High School, Hopi Court and the Navajo Department of Corrections in Tuba City. For those who need a higher level of care, they can be referred to Hopi Behavioral Health, Native Americans for Community Action, Sonora Prevention Works in the Phoenix area or Scottsdale Recovery Center.
Humetewa said the staff is committed to helping clients who have used illegal drugs and alcohol. “It depends on what the individual needs,” he said.
Of the 79 clients served last year, only five individuals were referred to higher levels of service. Humetewa says most of their clients are coming to them as part of their aftercare program.
Hopi Behavioral Health assesses the clients. “We utilize our lived experiences to provide evidence-based curriculum, utilizing our teachings and values,” he said.
Clients are influenced by where they grew up and their environment, says Humetewa. Generational disconnection has been a problem, he reports. Many individuals have problems living in the two worlds: One of their homeland and the other the Western European way of life.
“We use language and culture to reintroduce the values and teachings. They need to first find out where they were disconnected and then reconnect with their culture. They need to be right with themselves first before they can be in touch with a higher power.”
HOPI Substance Abuse Prevention Center offers a 12-step program. Also beneficial, he says, are community wellness programs. Humetewa says clients return to their communities to help and mentor others. Many have returned to education and earned degrees.
Humetewa has been through his own ordeal, but recently celebrated 21 years of recovery. He graduated from an Indian recovery program in 2004. He says he learned that sobriety and recovery are two different things: Sobriety is being sober, and recovery is realizing the work it takes to be well, physically, spiritually and psychologically.
Humetewa said finding transitional housing for those in recovery, especially on Hopi where housing is limited, can be a challenge. This is where peer support becomes crucial. “I’m working on this, but it’s not easy.”
Humetewa said it’s always encouraging to come home to help your people, but when people come home, they find few jobs or resources to help them. Still, Humetewa has seen many successes. “I enjoy watching the miracles of change and seeing people as they start looking well,” he said. “They share their stories of recovery. They work at getting well.”
The HOPI Substance Abuse Prevention Center is part of the Hopi Foundation and funded through grants It serves clients from the Navajo Nation, as well. Humetewa praises his staff and mentors Cordell Sakeva and Kristie Kewenvoyouma for the work they do.
The HOPI Substance Abuse Prevention Center provides daily support in recovery through programs, satellite locations and on-call services. It also promotes collaborative work that strengthens individuals, families and cultural values. FBN
Source: https://www.flagstaffbusinessnews.com/hopi-recovery-center-sees-miracles-of-change-through-culture-based-healing/
Teachers, frequently the first adults to sense that something is wrong, must be trained to recognise early warning signs and to respond with confidence.
A school ruled by punishment alone encourages concealment, whereas one that allows students to seek help without stigma and reprisal may prevent lasting harm. Strengthening life skills, particularly resistance to peer pressure regarding drugs, remains a practical and effective defence. The damage extends far beyond users. It spreads through public health, education and economic life, weakening each in turn. Careers are lost and communities lose capable members long before the problem is acknowledged.
Social stability is central to national identity and long‑term progress. Illegal drugs represent a serious threat to Omani society. The experience of North America and Europe offers a stark warning. There, widespread drug availability has contributed to rising addiction, increasing overdose deaths and the decline of once‑stable communities.
Drug dealers are everywhere, health services struggle with long‑term physical and psychological harm, families fracture and crime increases. Youngsters are especially vulnerable because judgement, concentration and emotional balance are still forming. Exposure to drugs at this early age can cause lasting impairment: academic failure, school dropout, mental illness and long‑term dependency.
Government action must therefore be firm and consistent. Drug trafficking thrives where enforcement is weak or uneven. Strong border controls, intelligence‑led policing, police departments dedicated to arresting drug dealers and swift prosecution send a clear message that trafficking will not be tolerated.
While users require rehabilitation rather than punishment, those who profit from supplying drugs must face severe penalties. Delay and denial allow the problem to grow quietly until it becomes deeply entrenched.
Rumours that illegal drugs in Oman are sold mainly by non‑Omani residents must be treated with caution. Assigning blame on the basis of nationality distorts justice and weakens enforcement. Responsibility must be determined by evidence and applied impartially to all involved: Omanis and expats.
Families can be the most influential line of defence. Young people who feel supported and connected to their families are far less vulnerable to external pressure.
Open discussion, clear boundaries, awareness of friendships and online influences and early intervention when concerns arise can prevent experimentation from becoming a habit.
Waiting for unmistakable signs is often waiting too long. International evidence also indicates that vaping devices are sometimes used to consume illegal drugs discreetly, increasing the need for awareness at home and in schools.
Protecting Omani youth requires coordinated effort rather than isolated gestures. Families, schools and authorities must act together. Oman’s stability has been built patiently over generations.
Allowing illegal drugs to spread would place that inheritance at risk. Early, decisive action remains far less costly than prevention attempted too late. What is needed immediately, especially for parents and their children, is a drug hotline which can be called for advice without fear of social repercussions.
Source: https://www.omanobserver.om/article/1181724/opinion/why-schools-must-act-early-against-drugs
Key points
The most consequential shift in cannabis policy in more than 50 years is now happening. A December 2025 executive order from President Trump has directed the federal government to down-schedule cannabis from Schedule I (illegal) to Schedule III (a lawful drug designation with a lower level of harm than Schedules I or II) . This is despite the alarming lack of research evidence for medicinal cannabis.
Rescheduling cannabis will provide significant tax advantages to the industry, allowing billions in previously banned business expense deductions that could hugely boost marketing efforts, research, or both. The executive order (EO) does not explicitly recognize cannabis as medicine. It also does not set national standards for cannabis labeling, dosages, or youth protection, all of which are essential.
Whether you view the EO as long overdue or ill-advised, the key questions now are how this change will be implemented, who will control the downstream effects of cannabis, and whether public health experts or lobbyists seeking to accelerate commercial momentum will define what happens next.
Currently, any cannabis warning labels are inconsistent across states, often minimal, and frequently omit critical risks, such as mental health effects, breastfeeding harms, and other dangers stemming from high-potency cannabis products.

The executive order simultaneously instructs federal agencies—particularly the National Institutes of Health and the Food and Drug Administration—to expand, streamline, and lower barriers to cannabis/cannabinoid research.
Indeed, the now-history LSD-like Schedule I status of cannabis imposed hurdles to research. Nevertheless, considerable research has been done, even though a special license was necessary to use the drug in studies. However, rescheduling marijuana doesn’t guarantee adequate research funding, FDA approval for cannabis, THC, or CBD, or high-quality research.
What Drug Experts Say
Among the EO’s most vocal critics is Kevin Sabet, drug policy expert who served both Republican and Democratic administrations and now president of Smart Approaches to Marijuana, who sees the order as devoid of public health wisdom. Sabet warns that rescheduling signals medical endorsement despite cannabis’s association with significant health risks, especially for young users. Sabet highlights that the EO moves cannabis from Schedule I (not legal) to Schedule III (controlled but legal), although the medicinal effects of cannabis have never been FDA-proven or approved.
Harvard’s Kevin Hill, M.D., supports rescheduling for improving research facilitation, arguing that current cannabis use lacks clinical guidance. He emphasizes funding as crucial for quality research. Hill ‘s position is pragmatic: Lack of scientific certainty is not a reason to avoid research—it’s the reason research is needed.
Hill also places responsibility for research funding on states and industry. Legal cannabis markets generate billions in revenue, yet only a fraction is reinvested in rigorous research, prevention, or treatment. Ethical stewardship, he argues, demands that those profiting from cannabis bear responsibility for understanding its risks and benefits.
Thirty percent of cannabis users, including adolescents, develop a substance use disorder, according to Mt Sinai School of Medicine’s Dr. Yasmin Hurd. She emphasizes the importance of pairing research expansion with clear regulations to avoid exacerbating risks linked with cannabis.
A crucial area for future research is safe and effective dosing of THC (the intoxicant in cannabis) amid imminently rising sales of high-potency products. Large-scale, longitudinal studies tracking neurodevelopmental outcomes in relation to timing and potency of cannabis exposure are essential.
At the same time, policymakers face a proliferation of unregulated intoxicating cannabinoids sold outside state-licensed cannabis systems. Products such as delta-8 and other synthetic or semi-synthetic cannabinoids are widely available in gas stations and convenience stores, often with minimal oversight. These products disproportionately attract youth, undermining consumer safety. Closing loopholes has become a public-health necessity.
Recognizing the Rising Risks
Some media reports suggest the EO was pushed through despite vociferous objections highlighting the risks of cannabis use among adolescents and young adults. The link between early-age cannabis exposure and increased risk of schizophrenia, mood disorders, and long-term functional impairment is no longer speculative. The disorders carry lifelong healthcare, social, and economic costs. Yet current data are insufficient to guide prevention efforts. Without guidelines, prevention efforts will remain reactive and politically vulnerable. Nowhere are the stakes higher than among adolescents and young adults.
One of the nation’s leading scientists and long-time vocal opponents of legalizing cannabis, Yale’s Deepak D’Souza, M.D., has focused on the increasing amount of cannabis, its increased potency, frequency of use, and duration of effects, causing severe consequences in young people. Cannabis and some of its constituents produce acute impairments in memory, attention, executive function, impulsivity and risk-taking behaviour, and psychomotor coordination, critical for driving a car. Nora Volkow, M.D., director of the National Institute for Drug Abuse (NIDA) has underscored the need for balanced research, acknowledging both benefits and risks of cannabis.
Dose is another urgent research priority, since higher THC concentrations are associated with increased risks of psychosis, cannabis use disorder, cardiovascular events, and cognitive impairment. More isn’t always better. A post-rescheduling agenda should include an investigation into minimum effective doses, upper safety thresholds, and the feasibility of reducing THC concentrations while preserving potential therapeutic effects.
Since rescheduling will be interpreted as an implicit medical endorsement, regardless of official intent, a national, evidence-based prevention strategy is needed, modeled on successful tobacco-control frameworks Such a strategy needs to include school-based education, clinician training, parental guidance, and public-health messaging that’s scientifically grounded rather than moralistic/alarmist.
Federal consumer protection agencies need to become empowered to monitor misleading cannabis advertising.
Finally, the integrity of emerging research depends on maintaining a firewall between scientific inquiry and commercial influence. Industry participation in research isn’t inherently problematic, but it must be governed by transparency, independent oversight, and conflict-of-interest safeguards.
Acceptance Without Complacency
The December 2025 executive order is now a reality. There is likely to be a huge cash infusion without regulation, causing a commercialization boom in cannabis, with the potential to harm our youth more than ever. Industry needs to step up and fund academic research.
Youth protection and guardrails are indispensable. A good start would be warning labels, funding of prevention efforts directed toward teens and young adults, and increasing NIDA’s funding for cannabis/THC/CBD translational research .
If cannabis products remain legal and available, consumers need clear, standardized warnings reflecting the best available evidence on cannabis use disorder and psychosis risk; impaired driving; memory effects; and adolescent brain vulnerability. Public health warnings should not be optional, nor diluted by marketing language implying medical endorsement where none exists.
Source: https://www.psychologytoday.com/au/blog/addiction-outlook/202512/marijuana-rescheduling-is-now-real
With the year 2025 coming to an end, it is a great pleasure to reflect on this year’s highlights and express our sincere appreciation for the support of all partners and collaborators of the Youth Initiative.
Friends in Focus
From the outset, 2025 has been a fruitful and exciting year for the Youth Initiative, with its reach expanding and its positive impact growing. Following the successful prototype development in 2024, UNODC’s new youth-based, peer-to-peer drug prevention programme, Friends in Focus, began its pre-pilot testing in 2025 with the support of local partners, UNODC field offices, and most importantly the youth participants across various countries. Friends in Focus is an evidence-informed prevention programme that equips youth with practical skills and knowledge in drug use prevention, encouraging them to act as positive peer influencers within their communities
The initial pre-pilot was launched in Serbia in February, marking the programme’s first transition from theory to practice. Building on this launch, the pre-pilot implementation expanded throughout the year to Italy (Trento and Piedmont, respectively) and Montenegro. In addition to these national and local efforts, UNODC also initiated regional trainings of Friends in Focus in Central Asia (involving youth from Kazakhstan, Kyrgyzstan, Tajikistan, Turkmenistan, and Uzbekistan) and in Central America (with youth from Guatemala, Costa Rica, and the Dominican Republic). These regional pre-pilots have been particularly valuable in making Friends in Focus available in widely spoken languages such as Russian and Spanish, creating opportunities for further scaling of the programme in these regions.
These pre-pilot implementations stand among the key achievements of 2025, enabling the initiation of the assessment of the programme’s feasibility and applicability globally. Moreover, the wide reach achieved across the globe provides UNODC with a valuable opportunity to hear perspectives from youth in diverse cultural and societal contexts, and to evaluate whether Friends in Focus continues to resonate and remain relevant across different settings
Youth Forum on Drug Use Prevention
As in previous years, the Youth Forum took place on the sidelines of the annual Commission on Narcotic Drugs (CND) in March 2025. With the participation of 32 youth from 25 countries, the Youth Forum provided a safe environment for the youth from diverse cultures to come together, learn, and exchange insights about evidence-based drug use prevention efforts in line with the UNODC/WHO International Standards on Drug Use Prevention. The youth participated in interactive sessions throughout the Forum, and also had the opportunity to get a glimpse of UNODC’s Friends in Focus programme.
Continuing a cherished tradition, the youth drafted and delivered their joint Youth Statement, underscoring the importance of their peers’ active involvement in prevention work. They emphasized that “Prevention efforts must not only be about us, but led by us,” and that “When prevention is a priority, resilience becomes a reality.” Watch the highlight video of the Youth Forum 2025 here.
DAPC Grants
In 2025, the Drug Abuse Prevention Center (DAPC) continued to provide steadfast support to NGOs around the world in implementing youth-focused prevention projects. This year, local implementing partners from Cambodia, Iraq, Sri Lanka, Zimbabwe, Guatemala, Costa Rica, the Dominican Republic, and the Philippines were recommended and selected to receive the DAPC grants. These new projects will be implemented in their respective communities, promoting health, drug prevention and peer support, through active engagement with local stakeholders and young people. These initiatives highlight UNODC’s commitment to fostering resilient and healthier communities shaped with the meaningful participation of young people.
This year, the Youth Initiative continued to thrive as Youth Alumni advanced their active involvement in prevention work. After her participation in the UNODC Youth Forum 2024, Habiba Raslan collaborated with the National Fund for Drug Control and Treatment of Addiction (FDCTA) in Egypt, delivering impactful prevention messages to children and teenagers. She also remained active in the UNODC MENA Youth Network, and was also involved in the launch of the Egyptian Youth Network, bringing together young people committed to substance use prevention.
In April, 2023 youth alumna Inês Costa Louro delivered a remarkable address at the ECOSOC Youth Forum 2025 on the role of youth in public health policy and the need to address the digital determinants of health, particularly in relation to substance use and mental well-being. In June, at the high-level conference commemorating 30 years since the Beijing Declaration and Platform for Action, Yeanoh Rukoh Bai-Kamara, a Sierra Leonean participant of this year’s Youth Forum, shared her perspectives as a young woman and highlighted her organisation’s efforts to empower women and support youth. She emphasized the inequalities women face in relation to drugs and the need to better address their specific needs. Later in the summer, Nathan Morris, another participant of the Youth Forum 2025 from Jamaica, contributed his perspectives as a youth advocate during the CND/CCPCJ joint side event at the 2025 High-level Political Forum, “Engaging children and youth in drug control, crime prevention and criminal justice efforts.”
Another key highlight of the year was the 2nd UNODC Youth Forum Alumni Reunion, which welcomed former Youth Forum participants from 20 countries. Notably, the event brought together participants from across the history of the Youth Forum, spanning from its early days in 2014 to the most recent cohort of 2025, marking over a decade of youth leadership. Through youth-led presentations and peer-to-peer discussions, the reunion reinforced the importance of mainstreaming youth perspectives and ensuring meaningful participation, strengthening young leaders’ roles as co-creators rather than merely beneficiaries of prevention efforts.
Looking Ahead
We extend our deep gratitude to all youth participants and alumni, DAPC grantees, local implementing partners of Friends in Focus, and supporters for their meaningful contributions to the Youth Initiative in 2025. This year was particularly significant, as we were able to reach far and wide through the new tools and resources, enabling youth to be more meaningfully engaged in prevention efforts. We look forward to continuing our collaboration with all partners and to the new possibilities that the coming year will bring, as we further strengthen youth engagement in prevention.
Source: https://www.unodc.org/unodc/prevention/youth-initiative/youth-action/2025/December/global-youth-leadership-in-drug-prevention_-key-highlights-from-2025.html
Teen use of alcohol, cannabis, and nicotine remained stable in 2025, while daily energy drink use rose and heroin and cocaine use showed small increases.
Substance use among adolescents in the United States has remained at historically low levels for the fifth consecutive year, according to new data from the Monitoring the Future (MTF) study conducted by the University of Michigan’s Institute for Social Research. The findings suggest that declines in teen drug use observed during the COVID-19 pandemic have persisted, rather than rebounding to pre-pandemic levels as many experts anticipated.1,2
The MTF study is an annual, nationally representative survey of substance use behaviors and attitudes among eighth, 10th, and 12th graders and has been supported by the National Institutes of Health for more than five decades. The 2025 report reflects responses from 23,726 students enrolled in 270 public and private schools across the United States, with data collected between February and June 2025. Students completed the survey online while in school, and results were statistically weighted to generate national estimates.
Researchers found that the proportion of adolescents abstaining from alcohol, tobacco, and nicotine remained stable at levels first documented in 2021, following a sharp decline in reported substance use between 2020 and 2021. That earlier decline was widely attributed to pandemic-related disruptions, including reduced social interaction, limited access to substances, and increased time spent at home with caregivers.
“One of the main findings from the survey this year is that teen use of the most common drugs has not rebounded after the large decline during the pandemic,” said Richard Miech, PhD, research professor at the Institute for Social Research and team lead of the MTF study. “Many expected teen drug use levels to return to pre-pandemic levels once the social distancing policies were lifted, but this has not happened.”
In 2025, abstinence from marijuana, alcohol, and nicotine in the past 30 days remained high across all grades. Among eighth graders, 91% reported abstaining, compared with 82% of 10th graders and 66% of 12th graders.
Alcohol use over the past 12 months also remained stable, reported by 11% of eighth graders, 24% of 10th graders, and 41% of 12th graders. Cannabis use showed a similar pattern, with 8% of eighth graders, 16% of 10th graders, and 26% of 12th graders reporting use in the past year.
The survey also assessed use of cannabis products derived from hemp, including intoxicating products such as delta-8-tetrahydrocannabinol. In the past 12 months, 2% of eighth graders, 6% of 10th graders, and 9% of 12th graders reported using these products.
Nicotine vaping remained stable across grades, with past-year use reported by 9% of eighth graders, 14% of 10th graders, and 20% of 12th graders. Use of nicotine pouches was less common but also stable, reported by 1% of eighth graders, 3% of 10th graders, and 7% of 12th graders.
One notable exception to overall stability was daily consumption of energy drinks or energy shots. Daily use in the past 30 days was reported by 18% of eighth graders, 20% of 10th graders, and 23% of 12th graders. Among 10th graders, this represented a statistically significant increase from 17% in 2024.
Use of heroin and cocaine remained uncommon across all grades but showed statistically significant increases compared with the previous year. Past-year heroin use was reported by 0.5% of eighth graders, 0.5% of 10th graders, and 0.9% of 12th graders, up from 2024 levels. Cocaine use remained stable among 10th graders at 0.7% but increased among eighth graders to 0.6% and among 12th graders to 1.4%.
“The slight but significant increase we see in heroin and cocaine use warrants close monitoring. However, to put these current levels of use in context, they are leagues below what they were decades ago,” Miech said.
Nora Volkow, MD, director of the National Institute on Drug Abuse, emphasized the importance of continued surveillance and prevention efforts, noting that overall levels of adolescent drug use remain low.
“It is encouraging that adolescent drug use overall remains relatively low and that so many teens choose not to use drugs at all,” Volkow said. “It is critical to continue to monitor these trends closely to understand how we can continue to support teens in making healthy choices and target interventions where and when they are needed.”
For pediatricians and other clinicians caring for adolescents, the findings underscore the value of routine screening, anticipatory guidance, and counseling tailored to emerging trends, including energy drink consumption and evolving cannabis products.
Source: https://www.contemporarypediatrics.com/view/teen-substance-use-remains-historically-low-in-2025-with-stability-across-most-drugs

Over the past decade, the illicit drug market in France has undergone unprecedented expansion, underscoring the magnitude of a phenomenon long underestimated by public authorities. A research note published in December 2025 by Christian Ben Lakhdar and Sophie Massin, professors at the University of Lille, estimates that the economic value of this market nearly tripled between 2010 and 2023, reaching approximately 7.9 billion U.S. dollars annually. This growth reflects not merely rising consumption levels but a profound restructuring of procurement dynamics: while cannabis remains dominant in terms of volume, cocaine has emerged as the most profitable substance, and synthetic drugs have experienced particularly rapid expansion. These trends point to the consolidation of criminal networks capable of optimizing pricing, purity, and distribution channels on an international scale. As a result, drug trafficking has become a major security and public health concern, extending well beyond the boundaries of conventional criminal activity. Understanding this contemporary landscape, however, requires a historical perspective, as today’s challenges are embedded in a longer continuum of State efforts to confront highly structured and adaptive criminal organizations in France.
The war on drugs in France has unfolded through multiple historical phases, each revealing shifts in criminal structures and governmental responses. During the 1960s and 1970s, a criminal network based in Marseille controlled the flow of heroin to the United States. This network, popularized globally by William Friedkin’s film The French Connection(1971), consisted of Corsican mobsters and Marseille traffickers operating clandestine laboratories where heroin was refined before being shipped by sea to New York and Boston . French authorities, cooperating closely with the U.S. Drug Enforcement Administration (DEA), relied on traditional intelligence methods: physical surveillance, infiltration, and monitoring of laboratories and transport routes. These operations identified key leaders, disrupted the trafficking network, and enabled the seizure of large heroin shipments. A notable example is the arrest of French TV presenter Jacques Angelvin in New York in 1962, resulting from a Franco-American joint investigation, which demonstrates how international collaboration facilitated the progressive dismantling of the French Connection while highlighting the interplay between domestic policing and transatlantic intelligence coordination.
Today, drug trafficking in France has become a pressing public health and security challenge, far more complex than in the 1960s. According to the French Monitoring Centre for Drugs and Drug Addiction, roughly 1.1 million people used cocaine at least once in 2023, while cannabis remained the most widely consumed illicit drug, with 5 million adults reporting use during the same year. Other substances, including heroin and synthetic drugs, circulate through ports, airports, and dense urban networks. Modern traffickers rely on encrypted communications and opaque financial flows to evade detection. Law enforcement agencies must sift through extensive data—from wiretaps and financial transfers to social media activity—to track the movement of drugs and identify key actors. Violence associated with trafficking is escalating, marked by targeted shootings, score-settling, and even acts of torture, underscoring the urgent need for multidimensional strategies to curb traffickers’ influence across France. The scale and sophistication of contemporary operations demand a response that combines physical, digital, and social interventions, illustrating that historical methods alone are insufficient for addressing modern organized crime.
A comparison between historical and contemporary criminal networks illuminates how organized crime has evolved and identifies levers for modern enforcement. The French Connection was dismantled due to its centralized structure and high visibility, but today’s networks require more sophisticated, adaptive approaches. Effective action now combines digital and field intelligence, targeted arrests, disruption of supply chains, financial tracking, and social initiatives to reduce traffickers’ appeal among vulnerable populations. International coordination is equally essential: France collaborates with Europol, Interpol, and other agencies to monitor drug and money flows across borders. Historical lessons provide a framework for evaluating the effectiveness of cooperation, infiltration, and criminal flow management, while also highlighting the necessity of adapting policing and judicial methods to technological innovation. By reconciling enforcement, prevention, and social protection, France aims to address current and future challenges in the war on drugs, reflecting the dynamic and multifaceted nature of modern trafficking networks.
Over the past decade, France has faced a worrying surge in drug-related violence, affecting both the suburbs of major cities and medium-sized towns. According to the Ministry of the Interior, more than 110 tons of narcotics were seized in 2024, including 53 tons of cocaine—more than double the previous year’s haul (). Cannabis seizures exceeded 50 tons, alongside the destruction of nearly 700,000 plants. Meanwhile, 110 drug-related deaths and several hundred injuries were reported. Cities historically less affected, such as Clermont-Ferrand (150,000 inhabitants) and Avignon (92,000 inhabitants), were designated “reinforced security zones” following fatal shootings, while metropolitan hubs like Nantes saw over 1,100 drug-dealing hotspots dismantled between September 2022 and September 2023. Marseille, long a hub for drug trafficking, continues to experience deadly incidents, including the November 2025 murder of 20-year-old Mehdi Kessaci, apparently intended to intimidate his brother, an anti-drug activist. This event sparked widespread local protests, highlighting the persistence and territorial reach of criminal networks despite sustained law enforcement efforts. The scale and visibility of these operations underscore the pressing challenge posed by modern trafficking, both in terms of public safety and operational complexity.
The social and economic consequences of rising drug-related violence are profound. In neighborhoods of Marseille, Lyon, and Nantes, fear shapes daily life: residents restrict movement, shops close earlier or intermittently, and families hesitate to let children travel alone. Police presence, though increased through patrols and identity checks, is often seen as inadequate, fostering feelings of abandonment and vulnerability. In areas sometimes described as “no-go zones,” minors as young as 14 are recruited by traffickers for final distribution, surveillance, or territorial security, perpetuating cycles of violence and criminality. Public demonstrations, such as those following Mehdi Kessaci’s assassination, reflect dual social demands: for a more visible and efficient justice system capable of deterrence and for community support programs that reduce trafficking’s appeal among vulnerable youth. Authorities themselves acknowledge the limits of their power in these contexts. These dynamics illustrate that modern drug violence is not merely a law enforcement problem, but a deeply rooted social and economic issue, requiring coordinated interventions that address both criminal operations and the broader community environment.
Despite intensified policing, repression alone proves insufficient against criminal networks, whose sophistication surpasses the French Connection. Traffickers rely on undetectable smartphones, encrypted messaging, and cryptocurrencies to obscure financial flows, complicating investigations and prolonging operational timelines. “XXL clean-up” operations in spring 2024 resulted in thousands of arrests and the seizure of weapons, narcotics, and criminal assets, demonstrating short-term effectiveness but failing to curb trafficking long-term. Experts advocate a multidimensional strategy that combines targeted enforcement, digital surveillance, financial control, prevention measures, and social reintegration programs. This holistic approach draws lessons from historical dismantling but must adapt to modern realities: criminal networks are flexible, decentralized, and technologically sophisticated, making AI-driven analysis of big data critical. The contrast with the French Connection underscores both continuity and evolution: the principles of disruption remain valid, but operational methods must now account for mobility, cryptography, and the fluidity of modern criminal ecosystems.
The French Connection, active primarily in the 1960s and 1970s, represents a historical model of organized crime built around a highly centralized supply chain. Groups based in Marseille controlled the production, refining, and export of heroin to the United States by importing morphine base from Turkey and the Middle East. Clandestine laboratories in the Marseille countryside transformed diacetylmorphine into highly pure heroin for U.S markets. The most notorious of these laboratories, the “Césari Lab,” linked to chemist Joseph Césari, was dismantled in March 1972 with nearly 100 kg of heroin seized. Cell leaders managed security, coordination, and transport, often relying on predictable routes: overland transfer to Marseille, concealment in shipments of fruit, textiles, or machinery, followed by maritime dispatch to the East Coast. While this organization enabled industrial efficiency, it also created vulnerability: fixed routes and concentrated production points made surveillance and interceptions easier, ultimately contributing to the network’s downfall. This paradox highlights the balance between operational efficiency and exposure in centralized criminal systems.
Authorities dismantled the French Connection through a three-pronged strategy. First, international cooperation with the U.S. DEA was significantly strengthened, ensuring continuous intelligence sharing on routes, laboratories, couriers, and financiers. This collaboration produced high-profile joint operations, including the January 1973 arrests of Jean-Baptiste Croce and Joseph Mari, key figures in Marseille’s heroin export to the United States. Second, French services applied classic intelligence techniques: surveillance, wiretapping, supply chain mapping, and meticulous monitoring of regional hubs. The investigations identified clandestine laboratories and intermediary networks. Third, targeted operations seized shipments, arrested chemists, and systematically dismantled production units, gradually weakening the network. These successive strikes revealed that what made the operation efficient also made it exploitable, demonstrating the inherent vulnerability of tightly centralized criminal structures.
These combined efforts exposed the internal weaknesses of a system the media depicted as sprawling. Dependence on fixed routes, the concentration of laboratories, and the public visibility of influential figures—including Marcel Francisci, a businessman and politician—facilitated intelligence work. By late 1973, these operations led President Richard Nixon to declare that Marseille heroin had effectively vanished from the American market. The French Connection provides a valuable framework for understanding contemporary criminal networks can be neutralized when flows, actors, and infrastructure are clearly identified, even without modern technology. Yet, comparing past and present highlights change: centralized, predictable structures have given way to fragmented and mobile networks using encrypted communications, digital services, and dispersed logistics. The enduring lesson is that law enforcement effectiveness depends on a combination of patient intelligence, international cooperation, and strategic adaptability—principles that remain essential for understanding today’s sophisticated criminal networks.
Drug trafficking in France today relies on far more fragmented structures than those of the French Connection. Contemporary criminal networks operate through autonomous, interchangeable cells capable of functioning independently and dissolving rapidly under intense police pressure. This flexible design allows traffickers to simultaneously exploit multiple supply chains: cocaine is imported by container in Le Havre, cannabis resin transits via the Iberian Peninsula, heroin arrives from the Belgian Dutch border region, and synthetic drugs circulate within party circuits. Clandestine apartments, storage units, and logistical hubs outside city centers are used to split shipments into smaller loads, reducing the risk of interception. The mobility of these networks complicates the identification of operational bases: a single network may coordinate transactions from Paris, store merchandise in Brittany, and redistribute it in Lille neighborhoods. Furthermore, the systematic use of encrypted phones, VPNs, and ephemeral messaging services makes surveillance increasingly difficult. This operational fluidity creates a decentralized criminal environment without visible ringleaders, compelling investigators to combine traditional physical observation with digital intelligence and financial tracking to monitor complex networks efficiently.
The sophistication of modern trafficking is not unique to France. Criminal organizations worldwide are increasingly adopting advanced technologies to secure supply chains, reducing the role of human couriers. In July 2025, the Colombian Navy intercepted the first unmanned narco-submersible near Santa Marta, remotely controlled via satellite and capable of carrying up to 1.5 tons of cocaine. Still in testing, the vessel sailed several hundred kilometers offshore, demonstrating the integration of civilian technologies, including satellite connectivity for real-time navigation. Coordinated tracking between patrol vessels and aerial drones allowed authorities to monitor its trajectory before interception. This operation highlights a new form of trafficking in which removing the human factor—a criminal network’s primary vulnerability—creates a “black hole” for intelligence services. France, confronting mobile and interconnected traffickers, must combine physical surveillance, digital monitoring, and technological anticipation to maintain operational effectiveness, demonstrating the growing need for multidimensional approaches to narcotics enforcement.
France’s response centers on the Office Anti-Stupéfiants (OFAST), the French Anti-Narcotics Office created in 2020. OFAST coordinates police, gendarmerie, customs, and international counterparts, enabling rapid intelligence sharing on ports, transit routes, and financial flows. Between 2023 and 2024, OFAST conducted nearly 4,000 operations, including long-term infiltrations, high-risk container tracking, and analysis of encrypted smartphones seized during arrests. Local units focus on mapping criminal networks, tracing financial flows via cryptocurrencies, and identifying clandestine warehouses. Asset seizures totaled more than US$140 million in 2024, reflecting a strategy targeting the economic core of criminal organizations. By integrating human, digital, and financial expertise, France has developed a comprehensive approach to decentralized and mobile trafficking, illustrating that effective law enforcement now requires coordination across multiple domains rather than isolated interventions.
Long-term strategies aim not only to arrest traffickers but also to disrupt the structural and logistical foundations of criminal ecosystems. Operations target transit points, warehouses, money-laundering networks, and suppliers of encrypted equipment, while monitoring digital communications. Legal measures reinforce enforcement: the 2025 anti-drug trafficking law allows authorities to seize crypto assets, freeze assets linked to money laundering, and temporarily close premises. Complementary social programs aim to prevent recruitment in vulnerable neighborhoods, providing community mediation, educational support, and personalized guidance for at-risk youth. This holistic strategy demonstrates that combating modern trafficking requires simultaneous action across economic, digital, logistical, and social dimensions, limiting traffickers’ adaptability while restoring state control over affected territories.
By contrast, the United States focuses primarily on securing entry points and intercepting shipments before they reach national territory. In August 2025, Operation Pacific Viper, led by the U.S. Coast Guard, seized 34 tons of drugs, including cocaine and marijuana. The operation relied on intensive maritime patrols, surveillance of suspicious vessels, and coordination with the U.S. DEA and other federal agencies. Under the Donald Trump administration, the strategy prioritized upstream disruption, aiming to stop drug flows at the source rather than intervening in urban areas. This contrasts with the French approach, which combines intelligence gathering, field operations, financial tracking, and social interventions. The comparison highlights a central point: the effectiveness of anti-drug operations depends on adapting methods to the mobility, fragmentation, and technological sophistication of trafficking networks. Revisiting lessons from the French Connection demonstrates how precise identification of key players and routes allows disruption of centralized criminal networks, providing a valuable framework for contemporary enforcement strategies.
Comparing the French Connection with today’s criminal networks reveals both enduring lessons and major structural shifts. Historically, the French Connection relied on a centralized, hierarchical organization with identifiable leaders and relatively fixed routes connecting laboratories, ports, and international markets. This visibility allowed targeted physical infiltrations and direct seizure of shipments, while communication remained limited to trusted messengers. Key principles—tracking flows, monitoring logistical hubs, and making targeted arrests—enabled authorities to disrupt the network for extended periods, demonstrating the importance of interagency coordination and precise intelligence. However, applying these methods directly to contemporary trafficking would be insufficient: the mobility, encryption, and decentralization of modern cells render the old model largely obsolete. Nevertheless, studying historical criminal networks remains invaluable for identifying the levers of action and disruption logic while cautioning against mechanically reproducing outdated practices in a vastly transformed technological and structural environment.
Modern trafficking operates through decentralized, autonomous networks functioning across multiple routes and territories. Leaders are no longer visible, cells can dissolve quickly, and financial flows move through shell companies or electronic wallets, evading conventional oversight. As Pamela F. Izaguirre noted regarding Mexico, the high-profile arrest of a cartel leader did not change the overall dynamics of criminal organizations, which continued to adapt and reconfigure themselves. Today’s criminal networks display even greater plasticity, forcing law enforcement to integrate traditional methods with advanced tools: physical surveillance and targeted interventions remain essential but must be complemented by cyber-surveillance, big data analytics, and financial tracing. The contrast with the French Connection is striking: predictability and centralization no longer simplify police operations. Contemporary strategies demand a combination of field operations, digital intelligence, and real-time international coordination to counter constantly evolving criminal structures.
Nevertheless, some principles persist: accurate intelligence, interagency cooperation, and sustained effort remain the foundation of effective enforcement. For instance, a 2025 joint operation between France and Spain, involving surveillance, electronic monitoring, searches, interceptions, and real-time intelligence sharing, led to the arrest of 24 network members, including leaders, and the seizure of more than 150 kg of drugs. This demonstrates that classic investigative methods—carefully adapted—retain relevance, while international coordination ensures rapid information exchange, harmonization of procedures, and mobilization of specialized teams. The evolution of trafficking also highlights the need to link coercive and social strategies. Unlike the export-focused, relatively invisible French Connection, today’s criminal networks operate within cities and suburbs, spreading violence and insecurity. A balanced approach combining law enforcement, technological innovation, and social intervention is therefore essential to restore territorial control and reduce traffickers’ adaptive capacity.
Almost every week, French media report drug-related violence, from gang shootouts and score-settling accompanied by torture to tense neighborhoods. In early December 2025, north of Paris, a fight between two gangs of traffickers erupted in a kindergarten playground, terrifying three-year-olds. The war on drugs has become a pressing reality at the heart of national debate, as President Emmanuel Macron concludes his term amid public confusion and limited popular support for his policies. Contemporary trafficking networks—decentralized, mobile, and technologically sophisticated—no longer follow the traditional models of the French Connection, rendering targeted arrests insufficient. French authorities now rely on advanced investigations, international cooperation, and digital monitoring. Europol, Interpol, and cross-border agencies enable near-instantaneous sharing of information on drug flows, financial transactions, and encrypted communications. Specialized units analyze this intelligence to trace supply chains, identify key players, and map trafficking hotspots. Revisiting historical practices demonstrates that lessons from the French Connection remain relevant, emphasizing the enduring value of combining patient intelligence, strategic coordination, and technological adaptation to combat modern, adaptive criminal networks effectively.
The social, legislative, and technological dimensions are equally critical for a sustained response, requiring strategies that go beyond immediate enforcement. Neighborhoods plagued by violence demand comprehensive prevention, educational support, community engagement, and targeted programs to limit the pool of potential recruits for dealers and lookouts—efforts supported by social organizations, local authorities, and political actors across the spectrum. Concurrently, French authorities are leveraging AI, predictive analytics, and financial tracking tools while reinforcing legislation on cryptocurrencies and money laundering to disrupt fluid and technologically sophisticated criminal networks. Logistical monitoring, mapping of hotspots, and coordinated international cooperation further strengthen these efforts. Beyond law enforcement, these measures aim to restore state authority, rebuild public trust, and address the structural vulnerabilities exploited by traffickers. Rising public demand for harsher repression risks polarizing society, yet solidarity and strategic foresight remain essential, particularly as Europe faces mounting geopolitical pressures, including the imperial ambitions of Vladimir Putin, demonstrating the inextricable link between domestic security and international stability.
Source: https://smallwarsjournal.com/2025/12/24/frances-war-on-drugs/
Opening statement by NDPA:
NDPA has mixed feelings about Harm Reduction – in one form, aiming to minimise harm in users while they consider cessation of drug use, it is something which NDPA supports, but in another form it is a ‘closet legalisation ploy’ – promoting the notion that drug use is valid and one should only seek to reduce the harm users experience – and NDPA clearly does not support this form. With this caveat, this article is included as an opinion piece for reading.
by Ricardo Fuertes, EATG member and representative at the EU Civil Society Forum on Drugs – December 17, 2025
Earlier this month, Mr Fuertes participated in the Civil Society Forum on Drugs as a representative of EATG. The discussions offered important insights into the current direction of EU drug policy and the conditions under which civil society organisations are operating.
The European Commission presented the new EU Drugs Strategy. From the perspective of many civil society organisations, the Strategy is notably unbalanced. While prevention, treatment, and social integration are clearly highlighted and structured as core pillars, harm reduction is treated differently. Rather than being recognised as a distinct and essential pillar, it is dispersed across the document, diluted in its language, and separated from the other approaches.
At the same time, the Strategy is highly detailed when it comes to security-related themes, threats, and supply reduction. Considerable attention is given to law enforcement and control measures, while approaches grounded in public health and human rights receive comparatively less emphasis. Decriminalisation and the legal regulation of drugs are entirely absent from the framework. In addition, the Strategy lacks a defined timeframe or end date, raising concerns about accountability and evaluation. It is also not accompanied by a dedicated budget or a comprehensive action plan beyond an Action Plan against drug trafficking.
These concerns have been explicited in a joint letter coordinated by the International Drug Policy Consortium and signed by a wide number of organisations, including EATG, as a tool to encourage negotiation with Member States.
Discussions throughout the Forum highlighted the need to better address systemic barriers affecting vulnerable populations. While HIV and viral hepatitis are mentioned within the EU Drugs Strategy, this is done in broad terms, without clearly identifying who is being left behind and why.
From EATG’s perspective, undocumented migrants must be explicitly included in prevention and treatment efforts. Legal precarity, fear of detection, and administrative barriers continue to exclude many undocumented migrants from access to drug services, HIV prevention, and care for viral hepatitis. A generic commitment to identifying systemic barriers is not sufficient; concrete measures are needed to ensure that prevention and treatment are accessible to all, regardless of migration status.
A noticeable decline in participation at this year’s Forum was also observed. This reflects the increasingly difficult conditions under which many civil society organisations are operating across Europe. Participants reported funding cuts, staff reductions and layoffs, as well as decisions to limit participation in international meetings. These pressures are forcing organisations to reduce activities and service provision, with harm reduction particularly affected.
Across the Forum, there was a shared sense that civil society space is narrowing and that critical voices are at risk of being marginalised.
As debates around the EU Drugs Strategy continue, EATG will continue to underline the importance of protecting civil society space, restoring harm reduction as a central pillar of drug policy, and ensuring that prevention and treatment genuinely reach the most marginalised, including undocumented migrants. A balanced, public health- and rights-based approach is not an abstract principle; it requires concrete actions, political commitment, and sustained investment.

Photo: Delegates at the Civil Society Forum on Drugs – December 17, 2025
Source: https://www.eatg.org/blogs/the-new-eu-drugs-strategy-an-unbalanced-approach-and-the-downgrading-of-harm-reduction/
by Robert F. Bukaty/Associated Press – Wall Street Journal The Editorial Board Dec. 9, 2025
Forwarded by Maggie Petito, DWI – 10 December 2025
Two new studies show that the ill effects of THC are increasing.
Here’s some surprising political news: A referendum campaign is gaining support in Massachusetts, of all places, to reverse the state’s 2016 legalization of recreational marijuana. Not coincidentally, two new studies report a surge in young pot users showing up at hospital emergency rooms.
Doctors at Mass General Brigham hospital found that the share of adolescents with psychiatric emergencies who tested positive for THC—the psychoactive ingredient in marijuana—jumped nearly four-fold after the drug was legalized for recreational sale and consumption in the state. The prevalence of other cannabis-related disorders among adolescents increased by a similar amount.
“Young people with mental health challenges are more vulnerable to the negative effects of cannabis use, which can catalyze or worsen psychiatric symptoms,” author Cheryl Yunn Shee Foo writes. She adds that legalization of the drug can lead to “greater accessibility, social acceptability, and advertising” that increases use among young people.
This last point is common sense. Legalization removes a stigma from marijuana use, as well as increasing its availability.
Meantime, a new study in the Journal of the American Medical Association (JAMA) finds a surge in young adults nationwide showing up at hospital emergency rooms with cannabinoid hyperemesis syndrome (CHS). This is cyclical vomiting, often with nausea or stomach pain, that is far more severe than what someone might experience after a night of binge drinking. It is caused by heavy marijuana use, especially at high potencies.
ER visits for the disorder increased nearly eight-fold in the spring of 2020 as Covid lockdowns took hold. Visits dropped some in 2022, but remained about five times higher than before the pandemic. The U.S. Northeast and West experienced the biggest spikes, perhaps not surprising since most states in those regions have legalized marijuana and they also imposed strict lockdowns.
California, New York and other progressive states allowed pot dispensaries to stay open during the lockdowns by deeming them “essential businesses.” Instead of working, young people got high at home.
The study notes that better awareness among physicians of the disorder may contribute to the increase in ER diagnoses. An earlier study found that patients with the syndrome visited the ER on average 18 times before getting diagnosed, costing on average $76,920 per patient. Maybe someone can investigate how much Medicaid is spending on treating pothead maladies.
An accompanying commentary in JAMA says that stopping marijuana use is the “cornerstone” of preventing the syndrome, but “abrupt discontinuation may lead to withdrawal and high rates of relapse.” Legalization proponents downplay marijuana’s negative effects and addictive potential, but daily marijuana use is more common than daily alcohol use, according to a Carnegie Mellon University analysis last year of national survey data.
A group in Massachusetts last week submitted more than 74,000 signatures for a ballot referendum next November to reverse the state’s legalization experiment. These days this is a counterculture cause, but it’s one that may gain momentum as the ills of pothead culture and especially from pot use among the young become more widespread.
Source: www.drugwatch.org
DESIGNATING FENTANYL AS A WEAPON OF MASS DESTRUCTION
By the authority vested in me as President by the Constitution and the laws of the United States of America, it is hereby ordered:
Section 1. Purpose and Policy. Illicit fentanyl is closer to a chemical weapon than a narcotic. Two milligrams, an almost undetectable trace amount equivalent to 10 to 15 grains of table salt, constitutes a lethal dose. Hundreds of thousands of Americans have died from fentanyl overdoses.
The manufacture and distribution of fentanyl, primarily performed by organized criminal networks, threatens our national security and fuels lawlessness in our hemisphere and at our borders. The production and sale of fentanyl by Foreign Terrorist Organizations and cartels fund these entities’ operations — which include assassinations, terrorist acts, and insurgencies around the world — and allow these entities to erode our domestic security and the well-being of our Nation. The two cartels that are predominantly responsible for the distribution of fentanyl in the United States engage in armed conflict over territory and to protect their operations, resulting in large-scale violence and death that go beyond the immediate threat of fentanyl itself. Further, the potential for fentanyl to be weaponized for concentrated, large-scale terror attacks by organized adversaries is a serious threat to the United States.
As President of the United States, my highest duty is the defense of the country and its citizens. Accordingly, I hereby designate illicit fentanyl and its core precursor chemicals as Weapons of Mass Destruction (WMD).
Sec. 2. Implementation. The heads of relevant executive departments and agencies (agencies) shall take appropriate action to implement this order and eliminate the threat of illicit fentanyl and its core precursor chemicals to the United States. This includes the following actions:
(a) the Attorney General shall immediately pursue investigations and prosecutions into fentanyl trafficking, including through criminal charges as appropriate, sentencing enhancements, and sentencing variances;
(b) the Secretary of State and the Secretary of the Treasury shall pursue appropriate actions against relevant assets and financial institutions in accordance with applicable law for those involved in or supporting the manufacture, distribution, and sale of illicit fentanyl and its core precursor chemicals;
(c) the Secretary of War and the Attorney General shall determine whether the threats posed by illicit fentanyl and its impact on the United States warrant the provision of resources from the Department of War to the Department of Justice to aid in the enforcement of title 18 of the United States Code, as consistent with 10 U.S.C. 282;
(d) the Secretary of War, in consultation with the Secretary of Homeland Security, shall update all directives regarding the Armed Forces’ response to chemical incidents in the homeland to include the threat of illicit fentanyl; and
(e) to ensure the United States uses the full array of appropriate counter-fentanyl tools, the Secretary of Homeland Security, as consistent with applicable law and in coordination with the heads of relevant agencies, as appropriate, shall identify threat networks related to fentanyl smuggling using WMD- and nonproliferation-related threat intelligence to support the full spectrum of counter-fentanyl operations.
Sec. 3. Definitions. (a) “Illicit fentanyl” means fentanyl that is manufactured, distributed, or dispensed, or possessed with intent to manufacture, distribute, or dispense in violation of section 401 and 406 of the Controlled Substances Act (21 U.S.C. 841, 846).
(b) “Core precursor chemicals” means the core chemicals that create illicit fentanyl and its analogues, such as Piperidone or other Piperidone-based substances.
Sec. 4. General Provisions. (a) Nothing in this order shall be construed to impair or otherwise affect:
(i) the authority granted by law to an executive department or agency, or the head thereof; or
(ii) the functions of the Director of the Office of Management and Budget relating to budgetary, administrative, or legislative proposals.
(b) This order shall be implemented consistent with applicable law and subject to the availability of appropriations.
(c) This order is not intended to, and does not, create any right or benefit, substantive or procedural, enforceable at law or in equity by any party against the United States, its departments, agencies, or entities, its officers, employees, or agents, or any other person.
(d) The costs for publication of this order shall be borne by the Department of Justice.
DONALD J. TRUMP
THE WHITE HOUSE,
December 15, 2025.
Source: https://www.dea.gov/documents/2025/2025-12/2025-12-15/fentanyl-designated-weapon-mass-destruction

A new and growing drug threat is quietly reaching communities across the country, including rural areas like ours. It’s being called “fentanyl-plus,” and it’s different from what many people think of when they hear the word fentanyl.
This danger is not limited to people seeking opioids. In many cases, individuals never intend to use fentanyl at all.
What is “Fentanyl-Plus”?
“Fentanyl-plus” refers to fentanyl mixed with other substances, such as:
Sometimes the mixing is intentional. Other times, it happens without the user knowing, especially when pills or powders are bought on the street or shared by friends.
National drug surveillance systems report that this type of drug mixing has become more common in the later stages of the opioid crisis, increasing the risk of overdose and death.
Why this matters in rural communities
Rural areas face unique risks when it comes to fentanyl-plus:
In Arkansas, youth prevention data already shows early experimentation with alcohol, vaping, marijuana, and prescription drugs. These substances can unintentionally expose young people and adults to fentanyl through contaminated or counterfeit products.
The hidden pill problem
One of the most alarming trends involves counterfeit pills. Fake Xanax and pain pills are being manufactured to look nearly identical to real prescriptions but often contain fentanyl or other dangerous drugs.
Someone may believe they are taking a pill to relax, sleep, or ease anxiety — but instead are exposed to a substance that can slow or stop breathing within minutes.
Parents, grandparents, and caregivers should know:
Not all pills are what they appear to be.
Naloxone helps — but it’s not enough
Naloxone (Narcan) saves lives and should always be used in an overdose emergency. However, some substances now found mixed with fentanyl do not fully respond to naloxone, especially when sedatives like benzodiazepines or xylazine are involved.
This makes prevention, awareness, and early education more important than ever.
What families and communities can do
Prevention begins with awareness and conversation. Health experts recommend:
A community responsibility
Churches, schools, civic groups, and families all play a vital role by creating safe spaces for education without stigma or shame.
This issue is not about blame. It is about protecting lives.
Fentanyl-plus is appearing in places many never expected — including small towns, farming communities, and close-knit neighborhoods. Awareness today can prevent tragedy tomorrow.
For more information about local prevention programs, parent education, or community trainings, contact Bridging The Gaps of Arkansas at 1.888.978.8441 or www.BTGArkansas.org
Sources & Data
This article is based on national and state public health data, including:
________________________________________
About Bridging The Gaps of Arkansas
Bridging The Gaps of Arkansas provides community-based substance misuse prevention, youth leadership development, and family education services across Southwest Arkansas, working with schools, churches, and local partners to build healthier, safer communities.
Source: https://www.eldoradonews.com/news/2025/dec/15/a-new-drug-danger-is-emerging-and-its-not-what/

 Kevin Sabet’s message is getting through. Credit: Getty
Kevin Sabet’s message is getting through. Credit: GettyThrough intensified enforcement operations and heightened intelligence, DEA is applying unprecedented pressure on the global fentanyl supply chain, forcing narco-terrorists, like the Sinaloa Cartel and CJNG Cartel, to change their business practices. This has led to encouraging signs of progress. DEA laboratory testing indicates 29% of fentanyl pills analyzed during fiscal year (FY) 2025 contained a potentially lethal dose, a significant drop from 76% of pills tested just two years prior in FY 2023. Additionally, fentanyl powder purity decreased to 10.3%, down from 19.5% during the same time period. These reductions in potency and purity correlate with a decline in synthetic opioid deaths to levels not seen since April 2020.
As of December 1, 2025, DEA has seized more than 45 million fentanyl pills, and more than 9,320 pounds of fentanyl powder, removing an estimated 347 million potentially deadly doses of fentanyl from our communities. DEA intelligence indicates a shift in cartel operations, with increased trafficking of fentanyl powder and domestic production of fentanyl pills. The seizure of more than two dozen pill press machines in October further highlights this trend.
“Fentanyl Free America represents DEA’s unwavering commitment to save American lives and end the fentanyl crisis, we are making significant progress in this fight, and we must continue to intensify efforts to disrupt the fentanyl supply and reduce demand,” said DEA Administrator Terrance Cole. “DEA is striking harder and evolving faster to dismantle the foreign terrorists fueling this crisis, while empowering all our partners to join the fight to prevent fentanyl-related tragedies. Together, we can achieve a fentanyl free America and create a safer future for generations to come.”
The DEA Los Angeles Field Division was one of 23 domestic field divisions and seven foreign divisions that initiated Operation Fentanyl Free America in October. This targeted enforcement effort resulted in the seizure of:
Brian Clark, Special Agent in Charge of the Los Angeles Field Division, said, “Our country will be safer, healthier, and more secure when fentanyl no longer threatens our communities. A fentanyl-free America is within reach thanks to increased enforcement, education, awareness, and prevention. We all play a critical role in the fight against fentanyl. We’ve made substantial progress, but we can’t stop now.”
The threat of poly-drug organizations; cartels that traffic a portfolio of drugs opposed to a single substance became even more apparent during Operation Fentanyl Free America. Aside from producing less potent fentanyl, the cartels have increasingly diversified their operations in an attempt to minimize their risks and maximize profits, an evolution driven by opportunity and greed.
DEA remains at the forefront of the fight to disrupt trafficking networks and strengthen the government’s response to this epidemic. Fentanyl Free America represents DEA’s heightened focus on enforcement, education, public awareness, and strategic partnerships. The goal of the campaign is clear: eliminate the fentanyl supply fueling the nation’s deadliest drug crisis. Since 2021, synthetic opioids have claimed nearly 325,000 American lives.
The Fentanyl Free America campaign also emphasizes the importance of public engagement. DEA encourages everyone from community leaders, clergy, educators, parents, physicians, pharmacists, and law enforcement to take an active role in raising awareness by protecting others through education; preventing fentanyl poisonings by understanding the dangers; and supporting those impacted. Free resources including posters, radio advertising, billboards, and social media resources are available at dea.gov/fentanylfree.
DEA’s efforts are part of a larger whole-of-government strategy to dismantle transnational criminal organizations and protect U.S. communities from fentanyl.
Source: https://www.dea.gov/press-releases/2025/12/03/dea-launches-fentanyl-free-america-initiative-combat-synthetic-drug-2
It isn’t just people — when given the chance rats may also use cannabis to cope with stress, according to a study by researchers at Washington State University.
Published in the journal Neuropsychopharmacology, the study was designed to examine cannabis-seeking behavior and found that rats with higher natural stress levels are far more likely to self-administer the popular recreational drug.
“We ran rats through this extensive battery of behavioral and biological tests, and what we found was that when we look at all of these different factors and all the variables that we measured, stress levels seem to matter the most when it comes to cannabis use,” said Ryan McLaughlin, associate professor in WSU’s College of Veterinary Medicine.
Looking at traits ranging from social behaviors to sex, cognition, reward, and arousal, McLaughlin and his team of undergraduate and graduate student researchers created a behavioral profile for each rat. Then, over the course of three weeks, rats were observed for one hour daily as they were given the option to self-administer cannabis by poking their nose in a vapor port to release a three-second dispersal of cannabis vapor in an air-tight chamber.
During that one-hour period, student researchers tracked the number of “nose-pokes” by each rat and found a direct correlation to the number of nose-pokes and baseline stress hormone levels.
By measuring the stress hormone corticosterone in the rodents, the equivalent to the stress hormone cortisol in humans, the team found rats with higher natural stress hormone levels were far more likely to self-administer cannabis.
“If you want to really boil it down, there are baseline levels of stress hormones that can predict rates of cannabis self-administration, and I think that only makes sense given that the most common reason that people habitually use cannabis is to cope with stress,” McLaughlin said.
He said it’s important to note that it was a rat’s resting baseline stress levels that were associated with cannabis self-administration, not stress that fluctuates in real time with exercise or mentally challenging tasks. Stress hormone levels were also calculated after exposure to a stressor and showed no significant link to cannabis-seeking behavior.
There were also significant relationships between rates of cannabis self-administration and measures of “cognitive flexibility”, which is our ability to adapt to changing rules.
“Animals that were less flexible in shifting between rules, when we tested them in a cognitive task, tended to show stronger rates of cannabis-seeking behavior,” he said. “So, animals that rely more heavily on visual cues to guide their decision making, those rats, when we tested their motivation to self-administer cannabis vapor, were also very highly motivated rats.”
The study also identified a link between high morning corticosterone and low endocannabinoid levels to cannabis self-administration, although not as strongly as baseline stress.
‘Our findings highlight potential early or pre-use markers that could one day support screening and prevention strategies’ – Ryan McLaughlin, associate professor, Washington State University
Endocannabinoids are compounds produced on demand to help the body maintain a state of physiological balance, or homeostasis.
“There’s some thought behind why people might be more prone to use cannabis, and that maybe THC serves as a reasonable substitute for endocannabinoids in individuals that have lower endocannabinoid levels,” McLaughlin said. “So, perhaps there’s more of a drive to supplement that with cannabis.”
With more and more states decriminalizing cannabis and legalizing recreational cannabis, McLaughlin said it’s critical to understand the effects of the drug and the grips of drug abuse.
“Our findings highlight potential early or pre-use markers that could one day support screening and prevention strategies,” McLaughlin said. “I could certainly envision a scenario where having an assessment of baseline cortisol might provide some level of insight into whether there’s an increased propensity for you to develop problematic drug use patterns later in life.”
Source:https://news.wsu.edu/press-release/2025/12/11/rats-may-seek-cannabis-to-cope-with-stress-wsu-research-finds/

LOS ANGELES – An operation led by the Drug Enforcement Administration Los Angeles Field Division in October uncovered 628,000 pills containing carfentanil. According to the DEA, carfentanil is a synthetic opioid approximately 10,000 times more potent than morphine and 100 times more potent than fentanyl. The majority of the pills were seized from one stash location in Los Angeles County. The operation also resulted in the arrest of one suspected drug trafficker.
Brian Clark, Special Agent in Charge of the DEA Los Angeles Field Division, said, “This is a massive seizure, 628,000 carfentanil pills taken from a single drug trafficker. Our agents, with vital backing from local partners, mitigated a catastrophic danger. The urgency of this matter cannot be overstated, another stark reminder to those vulnerable to drug misuse. Know what you’re taking, because one pill can kill.”
According to the DEA, carfentanil was originally developed for veterinary use, more specifically to tranquilize large animals such as elephants. The white powdery drug closely resembles other substances like fentanyl or cocaine and can come in several forms. The DEA warns that carfentanil and other fentanyl analogues present a serious risk to public safety, first responder, medical, treatment, and laboratory personnel.
This operation was led by DEA L.A. Field Division Southwest Border Group 1 special agents and task force officers, with key support from the Vernon Police Department, the Baldwin Park Police Department, and the Los Angeles County Sheriff’s Department. Testing of the seized pills was performed by the DEA Southwest Regional Laboratory.
According to DEA L.A. Field Division, local law enforcement and first responders have recently seen an increased presence of carfentanil in the illicit drug market, which has been linked to a number of overdose deaths in various parts of the country. According to the CDC, deaths involving carfentanil increased approximately sevenfold – from 29 deaths from January to June 2023, to 238 deaths from January to June 2024. Carfentanil has now been detected in 37 states.
The L.A. Field Division stands as one of the DEA’s most complex and high-impact divisions, covering Southern California, Nevada, Hawaii, and the U.S. Territories of Guam and Saipan.
For additional safety information, please see the resource below:
https://www.dea.gov/stories/2025/2025-05/2025-05-14/carfentanil-synthetic-opioid-unlike-any-other
Source: https://www.dea.gov/press-releases/2025/11/19/dea-operation-nets-628000-carfentanil-pills-la-county
A growing number of regular cannabis users in the U.S. are coming forward with accounts of a severe and little-known disorder linked to long-term marijuana use.
The condition, now officially recognized by global health authorities, has led some people to hospital with pain so intense they describe it as unbearable.
Holland & Barrett Tribiotic Mind Balance Capsules – 60 Capsules
As of 2023, roughly 17% of Americans reported using cannabis, with 24 states legalizing recreational use.
But while the drug is widely used for its therapeutic and recreational effects, doctors are increasingly treating patients who present with repeated vomiting, severe abdominal pain and dehydration.
The pattern has been identified as cannabis hyperemesis syndrome (CHS), a disorder seen primarily in people who use cannabis daily or near-daily over long periods.
UW Medicine says symptoms often appear within 24 hours of the most recent use and can persist for days.
The syndrome is sometimes nicknamed “scromiting,” a blend of “screaming” and “vomiting,” due to the intensity of the episodes.
George Vi British Empire Stamps Collection – 100 To 500 Different Used & Off Paper Collecting, Crafting
Many who have experienced CHS have shared their stories online.
One TikTok user described the onset as “the worst physical pain I’ve ever experienced… and I birthed a 9-pound baby.”
Another said she “almost died,” explaining she couldn’t keep food or water down for a week.
Despite the episodes, some users admitted they continued smoking, which only worsened the symptoms. One woman, now six months sober, said quitting was the only way to stop the cycle.
“Smoking nearly killed me,” she said.
Doctors still do not fully understand why the condition occurs.
The Cleveland Clinic says one leading theory is that chronic use overstimulates cannabinoid receptors in the body’s endocannabinoid system, disrupting normal digestive regulation.
The World Health Organization has listed CHS in its International Classification of Diseases, allowing clinicians to formally track cases for the first time.
Sage Intacct for Manufacturers – Sage™ Intacct® – Official Site – Unleash the Power of Intacct
Researchers say the new designation will provide more reliable data on cannabis-related health problems.
Beatriz Carlini of the University of Washington School of Medicine said the classification will help quantify a growing issue.
“A new code for cannabis hyperemesis syndrome will supply important hard evidence on cannabis-adverse events,” she noted.
Sources: UW Medicine; Cleveland Clinic; WHO ICD, Unilad
Source: https://www.msn.com/en-au/health/other/cannabis-users-warn-of-painful-syndrome-linked-to-long-term-use/ar-AA1Rya8d?
|
Through intensified enforcement operations and heightened intelligence, DEA is applying unprecedented pressure on the global fentanyl supply chain, forcing narco-terrorists, like the Sinaloa Cartel and CJNG Cartel, to change their business practices. This has led to encouraging signs of progress. DEA laboratory testing indicates 29% of fentanyl pills analyzed during fiscal year (FY) 2025 contained a potentially lethal dose, a significant drop from 76% of pills tested just two years prior in FY 2023. Additionally, fentanyl powder purity decreased to 10.3%, down from 19.5% during the same time period. These reductions in potency and purity correlate with a decline in synthetic opioid deaths to levels not seen since April 2020.
As of December 1, 2025, DEA has seized more than 45 million fentanyl pills, and more than 9,320 pounds of fentanyl powder, removing an estimated 347 million potentially deadly doses of fentanyl from our communities. DEA intelligence indicates a shift in cartel operations, with increased trafficking of fentanyl powder and domestic production of fentanyl pills. The seizure of more than two dozen pill press machines in October further highlights this trend.
The DEA Houston Field Division was one of 23 domestic field divisions and seven foreign divisions that initiated Operation Fentanyl Free America in October. During a period of a month, this targeted enforcement effort resulted in the seizure of:
350 Counterfeit pills
which is equivalent to 103 deadly doses
149 pounds fentanyl powder
3154 pounds methamphetamine
30 pounds of cocaine
36 firearms
$249,285 U.S. currency
“Operation Fentanyl Free America seizures in October highlighted the ongoing threat of fentanyl. Despite the steady decline in overdoses in most of the South Texas,” said Special Agent in Charge of the Houston Field Division Jonathan C. Pullen. Fentanyl is still an imminent threat, and we can’t afford to look the other way. We will continue to get this poison off the streets, ensuring safer communities for generations to come”
The threat of poly-drug organizations; cartels that traffic a portfolio of drugs opposed to a single substance became even more apparent during Operation Fentanyl Free America. Aside from producing less potent fentanyl, the cartels have increasingly diversified their operations in an attempt to minimize their risks and maximize profits, an evolution driven by opportunity and greed.
DEA remains at the forefront of the fight to disrupt trafficking networks and strengthen the government’s response to this epidemic. Fentanyl Free America represents DEA’s heightened focus on enforcement, education, public awareness, and strategic partnerships. The goal of the campaign is clear: eliminate the fentanyl supply fueling the nation’s deadliest drug crisis. Since 2021, synthetic opioids have claimed nearly 325,000 American lives.
The Fentanyl Free America campaign also emphasizes the importance of public engagement. DEA encourages everyone from community leaders, clergy, educators, parents, physicians, pharmacists, and law enforcement to take an active role in raising awareness by protecting others through education; preventing fentanyl poisonings by understanding the dangers; and supporting those impacted. Free resources including posters, radio advertising, billboards, and social media resources are available at dea.gov/fentanylfree.
DEA’s efforts are part of a larger whole-of-government strategy to dismantle transnational criminal organizations and protect U.S. communities from fentanyl.
SOURCE: https://www.dea.gov/press-releases/2025/12/03/dea-launches-fentanyl-free-america-initiative-combat-synthetic-drug-3
Coordinator for this subject : David G. Evans, Esq. Senior Counsel, Cannabis Industry Victims Educating Litigators (CIVEL)
Contribution from: thinkon908 via Drug Watch International <drug-watch-international@googlegroups.com>
Sent: 19 November 2025 15:27
Subject: FROM DAVE EVANS REPORT OF THE CANNABIS REGULATORS ASSOCIATION WHAT IS WRONG IN POT STATES?
FOR SOME OF YOU THE FILE ATTACHED WAS TOO LARGE – YOU CAN GET IT ONLINE – SEE BELOW:
https://www.ncdhhs.gov/national-landscape-cannabis-regulators-association-cannra-presentation/download?attachment
CRITIQUE BY DAVID EVANS:
They claim to be a national organization of cannabis regulators that provides policy makers and regulatory agencies with the resources to make informed decisions when considering whether and how to legalize and regulate cannabis.
However, in our experience, the state agencies protect the marijuana industry and not the public. They engage in a denial of the harms of marijuana use and its addictiveness. They falsely support the medical utility of cannabis and THC products.
THIS IS A SCANDAL THAT NEEDS TO BE EXPOSED
In their power point presentation to the North Carolina Cannabis Advisory Council, it notes specific problems:
SLIDE 6: The industry is innovative and fast moving (faster than science). THIS ALSO MEANS THE INDUSTRY ARE FASTER (AND SMARTER) THAN THE STATE AGENCIES
State regulatory agencies have been limited in their resources given the needs. THEY DO NOT HAVE ENOUGH RESOURCES TO ENFORCE REGULATION. THE LEGALIZATION BILLS SEE TO THAT BY NOT AUTHORIZING FUNDS.
SLIDE 25: There are regulatory gaps concerning these products:
Chemically derived impairing cannabinoids (Delta8, Delta-10. HHC, THCO, etc.)
THCA gap – Products being marketed with high levels of THCA that are indistinguishable from cannabis products.
0.3% gap – Impairing amounts of Delta-9 THO in products that meet the legal definition of “hemp” per the 2018 farm bill.
SLIDE 27: Consumer Safety Concerns
Consumer confusion
Molecules that are new and unknown
Lack of product testing and oversight
Medical claims that are not approved by the FDA and/or supported by research
IN OTHER WORDS, THEY HAVE NO IDEA WHAT THEY ARE DOING !!
SLIDE 29: State Regulatory Challenges from the Current Landscape
No or limited state regulatory authority over cannabinoid hemp products
Lack of research to help guide regulatory decisions on many of these molecules; insufficient surveillance for current landscape. IN OTHER WORDS, THEY HAVE NO IDEA WHAT THEY ARE DOING
Increased challenges understanding data on safety and adverse events. IN OTHER WORDS, THEY HAVE NO IDEA WHAT THEY ARE DOING
Enforcement challenges
Increasingly blurred lines with the illicit market; increased cartel activity. INABILITY TO CONTROL CARTELS. WASN’T LEGALIZATION SUPPOSED TO STOP THE CARTELS?
SLIDE 37: Research finds that cannabis smoke contains many of the same carcinogens as tobacco smoke.
<<<<<<<<<<<<<>>>>>>>>>>>
Comments by J. Coleman. PhD: drug-watch-international@googlegroups.com <drug-watch-international@googlegroups.com> Sent: 19 November 2025 16:38
To: thinkon908@aol.com;
David,
Good work exposing these folks as frauds. It’s a common strategy for cannabis promoters to recommend stringent rules, knowing full well they cannot be enforced. An example of this is the 2018 Farm Bill that legalized the production and distribution of “lawful hemp” and its derivatives. Reading the statute, one might think that the restrictions in the law, e.g., 0.3 percent or below THC content by dry weight in hemp, would keep commercial pot out of the market. The bill obviously was written by hemp lobbyists, knowing that the complex and confusing regulations would impress hardliners but have no practical effect on the industry because a) there were no resources in the bill to enforce them, and b) determining compliance with the statute would take expensive in-lab analysis that no one was likely to do.
Of course, now that we have seen the lawful hemp industry operate for several years, it’s evident that the controls initially included in the statute are now being ignored. Just last week, Congress had to revisit the 2018 Farm Act to tighten up the hemp provisions to prohibit hemp products with excessive levels of THC from being sold.
Enacting statutes that have no practical effect is one way to prevent the government from regulating the industry. Another way is getting Congress to include in its appropriations bills restrictions prohibiting the DEA from making so-called medical marijuana cases in states where this activity has become a surrogate for legalizing the drug.
For example, in each fiscal year since FY2015, a decade ago, Congress has included provisions in appropriations acts to prohibit the Department of Justice from using appropriated funds to prevent states, territories, and the District of Columbia from “implementing their own laws that authorize the use, distribution, possession, or cultivation of medical marijuana.” The FY2024 provision lists 52 jurisdictions, including every U.S. jurisdiction that has legalized medical cannabis use at the time it was enacted.
There seems to be a constitutional issue here, but I have no idea how to make it justiciable. Whether the issue is immigration or drugs, it seems like some states no longer recognize the Supremacy Clause or what it means.
According to the NSDUH: In 2023, 21.8 percent of people aged 12 or older (or 61.8 million people) used marijuana in the past year regardless of mode (Figures 12 and 13 and Table A.5B). The percentage was highest among young adults aged 18 to 25 (36.5 percent or 12.4 million people), followed by adults aged 26 or older (20.8 percent or 46.5 million people), then by adolescents aged 12 to 17 (11.2 percent or 2.9 million people). (See: Key Substance Use and Mental Health Indicators in the United States: Results from the 2023 National Survey on Drug Use and Health)
The same government survey (NSDUH) in 2013 reported: As noted in the illicit drug use section, an estimated 22.2 million Americans aged 12 or older in 2014 were current users of marijuana (Figure 1). The number of past-month marijuana users corresponds to 8.4 percent of the population aged 12 or older (Figure 3). The percentage of people aged 12 or older who were current marijuana users in 2014 was higher than the percentages from 2002 to 2013. This rise in marijuana use among those aged 12 or older may reflect the increase in marijuana use by adults aged 26 or older and, to a lesser extent, increases in marijuana use among young adults aged 18 to 25 compared with the percentages of young adults who reported marijuana use in 2002 to 2009 (See: Behavioral Health Trends in the United States: Results from the 2014 National Survey on Drug Use and Health).
Of interest here is the increase in use that appears linear with the expansion of the “legal” cannabis industry. The percentage of Americans 12 years or older reporting use of cannabis increased 178 percent, from 22.2 million in 2013, to 61.8 million in 2023.
I’ve often compared the cannabis industry to winemaking. With the latter, as anyone who’s ever tried making homemade wine knows, after adding the yeast to the mashed grapes, the yeast consumes the sugar and excretes alcohol in the process. At a certain level, the alcohol produced will kill off the remaining live yeast. There are ways of fortifying the wine, but left on its own, it will settle at about 11-14 percent alcohol, depending upon the sugar content of the source material. At some point in the future (hopefully soon), the cannabis industry may reach a level at which its success draws the attention of state attorneys general who will do the math and realize that the return in tax revenue is a lot less each year from pot than the potential return on suing the industry for harm and suffering, etc. The opiates MDL in Cleveland is a good model. Like those hapless wine yeasts, the action of the industry will have put itself out of business just by doing what it does.
John Coleman – www.drugwatch.org
If pot interferes with your daily life, health or relationships, those are red flags.
“The more that somebody uses and the higher potency that somebody uses, the higher the risk of that,” Das said.
It’s become more common as cannabis has gotten stronger in recent years. In the 1960s, most pot that people smoked contained less than 5% THC, the ingredient that gets you high. Today, the THC potency in cannabis flower and concentrates in dispensaries can reach 40% or more, according to the National Institute on Drug Abuse.
Cannabis use disorder is diagnosed the same way as any other substance use disorder — by looking at whether someone meets certain criteria laid out in the latest version of the Diagnostic and Statistical Manual of Mental Disorders, the main guide for mental health providers.
These include needing more of the drug to get the same effect, having withdrawal symptoms and spending a lot of time trying to get or use it.
“When we break it down into these criteria that have to do with the impacts of their use, it’s a lot more relatable,” Das said.
If you’ve met just two of the criteria for cannabis use disorder in the last year, doctors say you have a mild form of the condition. If you meet six or more, you have a more severe form.
Many marijuana users first come to Das for help coping with something else, like alcohol use disorder. Later, she said, they’ll often come back and mention a struggle with cannabis.
She assures them that there are effective treatments for the disorder.
Dave Bushnell, a retired digital executive creative director, started a Reddit group 14 years ago for people who, like him, had developed an addiction or dependency to cannabis and wanted help recovering. Its discussion forum has 350,000 members and continues to grow.
Doctors urged people who need help to get it, whether it’s with a professional or in a peer group.
As with alcohol, “just because something’s legal doesn’t mean that it’s safe,” Das said.
___
Associated Press reporter Leah Willingham in Boston contributed to this story.
Source: https://www.washingtonpost.com/health/2025/11/22/pot-cannabis-use-disorder-marijuana-addiction/dcfff9a4-c7ac-11f0-be23-3ccb704f61ac_story.html

Key Facts:
Source: Weill Cornell University
The roots of addiction risk may lie in how young brains function long before substance use begins, according to a new study from Weill Cornell Medicine.
The investigators found that children with a family history of substance use disorder (SUD) already showed distinctive patterns of brain activity that differ between boys and girls, which may reflect separate predispositions for addiction.
The research, published Nov. 21, in Nature Mental Health, analyzed brain scans from nearly 1,900 children ages 9 to 11 participating in the National Institutes of Health’s Adolescent Brain Cognitive Development (ABCD) Study.
“These findings may help explain why boys and girls often follow different paths toward substance use and addiction,” said senior author Dr. Amy Kuceyeski, professor of mathematics and neuroscience in the Department of Radiology and the Feil Family Brain & Mind Research Institute at Weill Cornell. “Understanding those pathways could eventually help guide how we tailor prevention and treatment for each group.”
To explore these neural differences, the researchers used a computational approach called “network control theory” to measure how the brain transitions between different patterns of activity during rest.
“When you lie in an MRI scanner, your brain isn’t idle; it cycles through recurring patterns of activation,” said first author Louisa Schilling, doctoral candidate in the Computational Connectomics Laboratory at Weill Cornell.
“Network control theory lets us calculate how much effort the brain expends to shift between these patterns.” This transition energy indicates the brain’s flexibility, or its ability to shift from inward, self-reflective thought to external focus.
Disruptions in this process have been observed in people with heavy alcohol use and cocaine use disorder, and when under the influence of psychedelics.
The study found that girls with a family history of SUD displayed higher transition energy in the brain’s default-mode network, which is associated with introspection. Compared with girls without such a family history, this elevated energy suggests their brains may work harder to shift gears from internal-focused thinking.
“That may mean greater difficulty disengaging from negative internal states like stress or rumination,” Schilling said.
“Such inflexibility could set the stage for later risk, when substances are used as a way to escape or self-soothe.”
In contrast, boys with a family history showed lower transition energy in attention networks that control focus and response to external cues.
“Their brains seem to require less effort to switch states, which might sound good, but it may lead to unrestrained behavior,” Dr. Kuceyeski said.
“They may be more reactive to their environment and more drawn to rewarding or stimulating experiences.”
Put simply, she said, “Girls may have a harder time stepping on the brakes, while boys may find it easier to step on the gas when it comes to risky behaviors and addiction.” Since the brain differences appeared before any substance use, they may indicate inherited or early-life environmental vulnerability rather than the effects of drugs.
The researchers emphasize the need to analyze data from boys and girls separately, since averaging results across both groups masked the contrasts. Separate analyses revealed distinct patterns, underscoring the importance of sex as a biological variable in brain and behavioral research.
The findings mirror what clinicians see in adults: women are more likely to use substances to relieve distress and progress more quickly to dependence, while men are more likely to seek substances to feel euphoria or excitement. Identifying early neural vulnerabilities in adolescence could help guide prevention before substance abuse begins.
“Recognizing that boys and girls may travel different neural roads toward the same disorder can help tailor how we intervene,” Dr. Kuceyeski said. “For example, programs for girls might focus on coping with internal stress, while for boys the emphasis might be on attention and impulse control.”
A: It is linked to distinct patterns of neural transition energy before any substance use begins.
A: They display opposing neural flexibility patterns in attention and introspection networks.
A: It suggests tailored early interventions targeting stress coping for girls and impulse control for boys.
Source: https://neurosciencenews.com/neurodevelopment-addiction-sex-differences-29965/
CADCA is proud to announce the recipients of its 2026 National Leadership Forum Awards. Every year, CADCA recognizes exceptional individuals that have made significant contributions to the field of substance use prevention and community coalition leadership. The awards will be presented during the 36th Annual National Leadership Forum, February 2-5, 2026 at the Gaylord National Resort and Convention Center in National Harbor, Maryland.
“Our honorees represent the very best of public service and community leadership, and we look forward to celebrating their achievements at our National Leadership Forum,” said CADCA President and CEO General Barrye L. Price, Ph.D. “These distinguished leaders have shown what it means to stand up for the well-being of our communities.”
This year’s honorees exemplify innovation and dedication to creating safer, healthier, and stronger communities.
Outstanding Youth Leader: Sharmada Venkataramani
Recognizes an outstanding young person for service to a coalition and their dedication to preventing substance misuse
Sharmada is a rising junior at South Forsyth High School, passionate about youth advocacy and prevention work. She began by publishing a piece on Big Pharma’s role in the opioid crisis for the state social studies fair and further engaged with the Forsyth County Drug Awareness Council. There, she launched the “Elevate with Awareness” campaign, highlighting the importance of teen marijuana use awareness. Sharmada also led students in advocating for nicotine regulation bill HB 1260. As the youth sector lead for the 2024-2025 school year, she guides 30+ students on various prevention projects.
Additionally, she collaborated with District 4 Commissioner Cindy Jones Mills to establish the Forsyth County Youth Mental Health Coalition, distributing over 750 mental health resource guides. Sharmada serves as the county organizing deputy director at the Georgia Youth Justice Coalition, representing over 1500+ students to advocate for youth-focused reforms. She is also the JV president of her school’s mock trial team, a state-level award winner, and an officer in her school’s Future Business Leaders of America Club. In her free time, she enjoys Indian classical dancing and spending time with friends. Sharmada aims to attend law school and pursue a career in securities law.
National Newsmaker Award: Amy Neville & Alexander Neville Foundation
Recognizes an individual or organization that has used their platform or media presence to bring national attention to substance use prevention issues
Amy Neville is the President of the Alexander Neville Foundation (ANF), an organization her family founded after the tragic loss of her 14-year-old son, Alexander. A drug dealer on Snapchat sold Alex a counterfeit pill laced with fentanyl that took his life. This unimaginable loss compelled Amy to confront the fentanyl crisis and the growing dangers of unregulated social media platforms.
Through ANF, Amy works closely with young people to co-create meaningful drug prevention and social media education programs. The foundation is rooted in youth collaboration and has become a guiding voice in efforts to curb substance misuse and reshape the digital environment for children and teens. Amy continues to speak nationally on synthetic drug dangers, social media harms, and the urgent need for corporate and legislative accountability.
In April 2025, Amy appeared in Bloomberg Media’s acclaimed documentary Can’t Look Away: The Case Against Social Media, which explores the real-life consequences of Big Tech’s unchecked power. Her powerful presence in the film underscores her message: “This is all about money… We need to take back the power from these companies.”
Amy has also shared her family’s story and insights on CNN, FOX, CBS, ABC, and in Rolling Stone’s investigative piece “Inside Snapchat’s Teen Opioid Crisis.” Her mission remains clear: to prevent more families from experiencing the devastation hers has endured and to ensure youth are protected both offline and online.
National Leadership Award: Kirk Lane
Recognizes leaders who have been longtime supporters of the community coalition movement and who use their voice and influence to educate the community about the importance of substance abuse prevention
Arkansas Drug Director Kirk Lane was appointed by Governor Asa Hutchinson on August 7, 2017. In his current role, Lane serves as the Director of the Arkansas Opioid Recovery Partnership (ARORP), which works to support communities across the state through innovative prevention, treatment, and recovery initiatives. Under his leadership, ARORP partnered with CADCA to help Arkansas coalitions build capacity to secure federal Drug-Free Communities (DFC) funding. As a result of this partnership, seven of 13 ARORP-supported coalitions were awarded DFC grants, bringing $4.3 million in federal investment to Arkansas communities.
Previously, Director Lane served as the Chief of Police for the City of Benton, Arkansas. Director Lane began his law enforcement career in 1982. In 1986, he worked for the Pulaski County Sheriff’s Office for 22 years rising to the rank of Captain. His assignments during this time period included Patrol, Narcotics, Investigations, SWAT and Honor Guard. In January of 2009, Lane retired from the Pulaski County Sheriff’s Office as the Investigation Division Commander and was appointed the Chief of Police of the Benton Police Department.
He attended the University of Virginia and the University of Arkansas-Little Rock. He is a graduate of the Arkansas Law Enforcement Academy, the Drug Enforcement Administration’s Drug Commander’s Academy and the FBI National Academy 197th session. He has served on boards representing Arkansas for the Regional Organized Crime Information Center and was the Chairman of the Arkansas Chief’s Association Legislative Committee. Director Lane also served on advisory boards for the Criminal Justice Institute, the Arkansas Prescription Monitoring Program and the Arkansas Alcohol and Drug Coordinating Council.
Director Lane is an active member of the Arkansas State working group for Prescription Drug Abuse Prevention and received the 2012 Marie Interfaith Leadership Award for his work in this area. He also serves on the CADCA Board of Directors.
CADCA Lifetime Achievement Award: Dr. Mark Gold
Honors an individual whose career and contributions have had a profound and sustained impact on the prevention field
Mark S. Gold, M.D. is a world-renowned expert on addiction-related diseases and has worked for 40+ years developing models for understanding the effects of opioid, tobacco, cocaine, and other drugs, as well as food, on the brain and behavior. Today, Dr. Gold continues his research, teaching, and consulting as an Adjunct Professor in the Department of Psychiatry at Washington University in St. Louis. He publishes a weekly article for Psychology Today that translates the latest science on addiction-related issues into easy to understand, accessible information for the general public that CADCA distributes to its members.
About CADCA
CADCA is the premier prevention association equipping coalitions with tools, knowledge, and support to create positive change in their communities. CADCA’s vision is safer, healthier, and stronger communities everywhere. Through our work we have built a network of more than 7,000 coalitions across the United States and over 28 countries. At the core of CADCA’s creation is the belief in the effectiveness and efficiency of local coalitions as catalysts for drug-free communities globally, combating substance misuse through the implementation of comprehensive strategies for community change.
Source: https://sg.finance.yahoo.com/news/cadca-honor-outstanding-leaders-substance-151500024.html
by Herschel Baker – 24 November 2025
The Taskforce has been making many submission over a number of years to all States and Federal Government the increase danger of Illicit drugs on Australian roads. But our so-called experts do not recognize overseas research data.
Now The Taskforce at last has some Australian evidence see below.
National Data reveals drug driving is now responsible for more deaths on Australian roads than drink driving.
Drug driving is now responsible for more deaths on Australian roads than drink driving. National crash data shows that between 2010 and 2023, fatal crashes involving drugs, including cannabis, methamphetamine, MDMA and cocaine, more than doubled to 16-point-8 percent. At least one of those drugs is being detected in about 1 in 5 motorcycle deaths. Over the same 13-year period, crashes linked to drink driving decreased significantly Continuing a long-term downwards trend. There were ten times more random breath tests last year than roadside drug tests, but a drug test was ten times more likely to yield a positive result. Testing for drugs using a saliva swab is more complicated and more expensive than a breath test but states and territories have been incorporating more of them into their testing regimes.
Source: https://drugprevent.org.uk/ppp/?p=20329&preview=true.
In her 25 years with InnerAct Alliance, a youth substance abuse prevention organization, Angie Ellison has witnessed the emergence of various drugs.
“We watch those things and try to let the community know about them because when it starts with college kids, it trickles down to high school and middle school,” said Ellison.
Ellison said energy drinks made with the synthetic form of kratom, known as 7-hydroxymitragynine (7-OH) are now widely available at gas stations, smoke shops and online.
“We’re just trying to make sure that everybody is aware of it, especially parents. Because a lot of times those drinks just look like maybe something to help you stay awake, but it could have very addictive traits to it,” said Ellison.
“It is a substance that can be dangerous when taken too much. It can cause dependence and addiction and when stopped, it can cause a pretty serious withdrawal syndrome,” said Dr. Eric Shamas, ER physician with Orlando Health Bayfront Hospital.
At the Crisis Center of Tampa Bay, they are seeing more college students experiencing withdrawal from the kratom byproduct.
“They get told to buy this kratom energy drink because it helped me get through studying for the finals. They start drinking it and then they get hooked. That’s when we find out it wasn’t containing natural kratom,” said Cameron Pelzel, community paramedic manager for Crisis Center of TampaBay.
Although Florida has recently made it illegal to sell 7-OH products, Pelzel said the ingredient can still be found in energy drinks, gummies and supplements.
“A lot of manufacturers are finding other synthetic compounds that mimic the 7-OH part, and they are adding it into it to get passed all the loopholes in the legal system so they can keep people buying these drinks. So we’re getting a lot of people that are solely addicted to it,” Pelzel said.
301 deaths. 301 names, ages, faces removed. 301 families, communities, homes (or home equivalents) emptied.
In 2023, there were 301 opioid-related overdose deaths in Alameda County. Standing alone, that figure isn’t alarming to those of us reading behind “safe” walls on our expensive devices.
Nothing exposes us to the truth more than cold numbers. This data-driven meta-analysis will show there is far more to concern about the complexities that eventually result in the plague of opioids claiming those 301, and thousands more, lives.
The acceleration of the Alameda County crisis
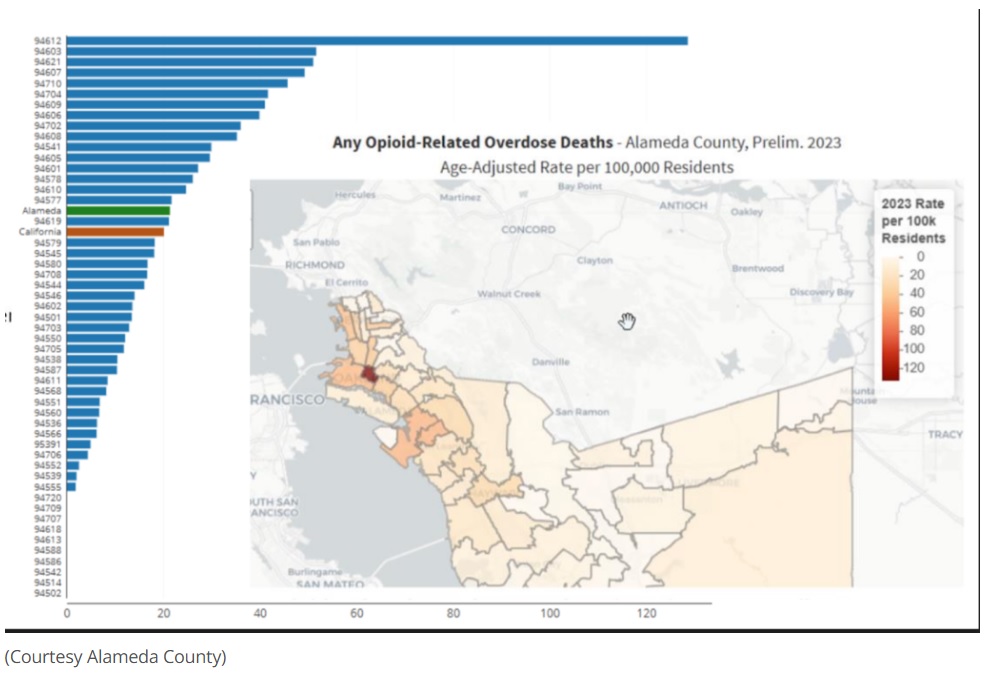
Those 301 Alameda County lives claimed by opioids in 2023 represent a 60% increase from 2022. Alameda County experienced the worst increase of all Bay Area counties in opioid overdose deaths from 2018-2021; Alameda’s rates tripled over this time while neighboring (Courtesy Alameda County)
There is an apparent inequity within the county. African-Americans’ fatal overdose rates are triple that of the county average, and the homeless comprise 30% of all overdose deaths.

The teen paradox: Less use, more deaths
The focus is on teens, right? That would make sense. After all, teen substance use excluding cannabis is DOWN, compared to the 20.9% of high school juniors in 2002, the 8% figure of 2022 represents major improvement.
Despite this, death rates are not improving. In fact, teen overdose deaths doubled in the eight short months between August 2019 and March 2020. As of 2022, 22 teens were dying WEEKLY from drug overdose in the United States. And overdoses are now the third leading cause of death for the youth, after guns and cars.
Fentanyl changed it all.
Now, over 75% of teen overdose victims’ lives are claimed by fentanyl. There was nearly a 300% INCREASE in fentanyl deaths aged 15-19 from 2018 to 2021.
The problem isn’t necessarily addiction. It’s contamination.
84% of teen overdose deaths are unintentional, and around a quarter of teen overdose deaths involve fake prescriptions. Fatal drugs like fentanyl spread through adult markets due to their potency and make their way to teens by accident. Most teens do not even get hooked onto the drugs that kill them.
Treatment inequality and solutions
Teen treatment right now is almost a scandal. While 42% of adults aged 45+ receive medications for opioid use disorder within three months of diagnosis, only 5% of teens do. Out of every five teens with substance use disorder, only one gets treatment.
Regardless of everything, prevention programs are still a solution. Project Towards No Drug Abuse (Project TND) has shown a 25% reduction in hard drug use. Medication-Assisted Treatment (MAT) reduces overdose deaths by 70-80%. Endless life-saving rescues by naloxone have been documented by near-death survivors.
It is not that there are no solutions. Ironically, teens are the ones with the least access to drugs. We know what works, and Alameda County cares for its people. The change to prevent teen opioid overdose deaths must originate in expanding access and awareness to the systems proven to save lives.
Source: https://www.pleasantonweekly.com/alameda-county/2025/11/17/the-data-driven-paradox-of-prevention/
This article was written as part of a program to educate youth and others about Alameda County’s opioid crisis, prevention and treatment options. The program is funded by the Alameda County Behavioral Health Department and the grant is administered by Three Valleys Community Foundation.
The Government’s new mandate to carry out random oral-fluid roadside drug testing marks a milestone in New Zealand’s road safety policy
Under recently passed laws, police can now stop any driver, at any time, to screen with an oral swab for four illicit substances: THC (cannabis), cocaine, methamphetamine and MDMA (ecstasy).
Police will begin the rollout in Wellington in December, with nationwide coverage expected by mid next year.
Drivers will face an initial roadside swab taking a few minutes; a positive result triggers a second test. If confirmed, the driver will face an immediate 12-hour driving ban and have their initial sample sent to a lab for evidential testing.
With nearly a third of all road deaths involving an impairing drug, moves like this are clearly aimed at a serious problem.
Efforts by the previous Labour-led government stalled because no commercially available oral-fluid device met the evidentiary standards required at the roadside.
The government now appears to have what it needs to begin roadside testing. But it remains unclear whether this policy will achieve its goal of preventing truly impaired driving.
The research on cannabis and driving impairment is mixed. Many studies show an associative rather than causal link: people who use cannabis more often tend to report more crashes, but not whether those crashes happened while they were impaired.
Unlike alcohol – where blood-alcohol concentration closely tracks impairment – no such relationship exists for THC. Cannabis is fat-soluble, so traces linger in the body and appear in saliva long after any intoxicating effect has passed, making saliva testing a relatively poor proxy for impairment.
For the other targeted drugs – the stimulants methamphetamine, cocaine and MDMA – the connection to driving impairment is also unclear. At lower doses, stimulants can even improve certain motor skills. The risks are instead tied to perceptual shifts or lapses in attention, which a saliva test cannot detect.
Because cocaine and meth remain illegal globally, it is difficult to conduct the controlled studies needed to link presence and impairment.
The policy’s focus on just four illicit drugs also raises questions of scope. In practice, these are among the easiest and most visible substances to target: the low-hanging fruit.
Yet impairment from prescription medications such as sedatives or painkillers is far more common and remains largely self-policed.
Responsibility falls to individuals and their doctors to decide when it is safe to drive – a much bigger problem than many realise.
Police expect to conduct about 50,000 tests a year – around 136 a day nationwide – compared with more than four million alcohol breath tests annually.
While that’s a modest number, the introduction of roadside breath testing in the 1980s proved transformative. Alcohol consumption, which had been rising for decades, peaked around 1980 and then began to fall after the combined impact of breath testing and public awareness campaigns.
Whether the new drug-testing programme can produce a similar deterrent effect – without that level of visibility or education – remains to be seen.
Even if it does, the overall impact may be small. Drug use and drug-driving are far less common than alcohol use ever was, so the scope for large behavioural change is limited.
Another pressing question is what happens when the test detects traces of cannabis long after impairment has passed. THC can remain detectable in regular users for up to 72 hours, even though its intoxicating effects last only a few.
That means a medicinal cannabis patient who took a prescribed dose the night before – or a habitual user with high baseline levels – could therefore test positive while driving safely.
Although the law provides for a medical defence, there is still no clear procedure for proving a prescription at the roadside. Few people carry that documentation, and it’s uncertain whether digital GP records would be accepted.
In practice, some law-abiding drivers will inevitably be caught up in the process simply because of residual traces that pose no safety risk. Conversely, an inexperienced cannabis user may feel heavily impaired yet return a low reading.
This uncertainty reflects a deeper flaw in the system. When the previous government first designed the policy, it intended to test for impairment.
Because no devices could meet the evidentiary standard, the law was amended to test only for presence.
Perhaps the resulting regime’s relatively low-level penalties – such as a $200 fine and 50 demerit points for the confirmation of one “qualifying” substance – will help it withstand legal scrutiny, but they also highlight its scientific limitations.
Other jurisdictions have taken a different path. Many have returned to behavioural assessments of impairment – the traditional field-sobriety approach of observing coordination, balance and attention.
In the United States, for instance, officers often rely on such behavioural indicators because the law there still centres on proving a driver was impaired, not simply that they had used a substance.
In the end, a test that measures presence rather than impairment risks confusing detection with prevention – and may do little to make New Zealand’s roads any safer.
Author: Joseph Boden, Professor of Psychology, Director of the Christchurch Health and Development Study, University of Otago
Source: https://www.1news.co.nz/2025/11/17/will-drug-testing-drivers-really-make-nz-roads-safer/
At some point, just about every business will face the challenge of an employee struggling with substance use. While these situations can be complex and emotional, they also present an opportunity for employers to show compassion, strengthen their workplace culture, and retain valuable talent. Supporting an employee through treatment and recovery isn’t just the right thing to do; it’s also good business.
The U.S. Department of Labor’s Recovery Ready Workplace program asserts that “workers with SUDs take nearly 50% more days of unscheduled leave than other workers and have an average annual turnover rate 44% higher than the workforce as a whole.”1 While it may seem like the best choice is to terminate an employee with a substance use disorder, workers who are in “SUD recovery average nearly 10% fewer days of unscheduled leave per year than other workers. And, the turnover rate for employees in recovery is 12% lower than the overall average.”
Employees in recovery who feel supported often bring loyalty, commitment, and a strong work ethic. All of this helps to demonstrate the tangible labor and economic benefits of supporting employees through treatment and in recovery within your workplace. As an employer, understanding the basics of the treatment process can help you respond effectively.
Rehabilitation programs generally fall into two categories:
Employers should also remember that mental health conditions related to substance use disorders may qualify for protection under the Family and Medical Leave Act (FMLA) and the Americans with Disabilities Act (ADA).
Small business owners need to know that both the FMLA and ADA include important provisions related to treatment:
Navigating these laws can be tricky, and because city and state regulations also vary, consulting legal counsel before making major employment decisions is a smart step.
Even with clear policies in place, compassion should be at the heart of your response. Here are some ways small business owners can help employees in treatment and recovery:
Helping an employee navigate treatment and recovery is challenging, but it can also be one of the most meaningful things a small business owner can do. When you foster a culture of understanding and support, you strengthen your team, reduce turnover, and contribute to a healthier community.
Source: Drug Free America Foundation | 333 3rd Avenue N Suite 200 | St. Petersburg, FL 33701 US
Supplementary Source:
A continuing discussion on the opioid epidemic in the workplace – Part 3. (2024, February 26). JD Supra. https://www.jdsupra.com/legalnews/a-continuing-discussion-on-the-opioid-4776444/
NATIONAL DRUG-FREE WORKPLACE ALLIANCE
As the workplace division of Drug Free America Foundation, NDWA’s mission is to be a national leader in the drug-free workplace industry by directly assisting employers and stakeholders, providing drug-free workplace program resources and assistance, and supporting a national coalition of drug-free workplace service providers.
For more information and drug-free workplace resources, visit NDWA at www.ndwa.org.
The mistaken belief that people with substance use disorders (SUDs) must “hit rock bottom” has shaped addiction care for decades. This model contrasts with how medicine manages chronic illnesses, where early detection and proactive treatment are normal. The “bottom” in addiction is a moment of maximum despair and hopelessness. It also may be a life-changing event like getting fired, losing a relationship, or facing legal charges. It could mean a moment between considering changing one’s life or suicide.
For more than 30 years, I have proposed that addiction treatment must “move up the bottom” to reduce harm and have a better chance of working. Applying preaddiction logic holds promise for lowering SUD-related suffering, illness, and mortality. Denying early diagnosis and treatment may primarily stem from addiction stigma.
“Let them hit bottom” was (and is) the refrain in addiction care; suffering supposedly must crescendo before people with an SUD accept the need to stop using drugs. Whether arising from fear of people gaming the system and seeking opioids for fake injuries or the inherent austerity of public institutions, this belief still shapes policy and practice.
In the early 1970s, I encountered this idea as a medical student. People who came to the emergency room with overdoses were not admitted. Medicine had little to offer and might undermine a person’s journey toward readiness; a person might feel ready for treatment, but someone else decided they’d not hit bottom. How ridiculous is this?
But when physicians misuse substances, then early intervention, long-term monitoring, and structured support are considered necessary. These practices, codified in physicians’ health programs (PHPs) across the United States, help most physicians, yielding an excellent return-to-work rate and resumed function. The message is clear: The “rock bottom” model is neither ethical nor clinically efficient.
National Institute on Drug Abuse Director Nora Volkow has called the belief that someone must “hit rock bottom” before treatment “a myth that can have dire consequences.” While the rock-bottom narrative offers psychological neatness—drama, surrender, catharsis—it lacks scientific grounding. Substance use disorders rarely emerge overnight; they evolve with “use,” then “risky use,” often in adolescence or early adulthood. By the time someone meets all criteria for severe SUD, the hijacked brain is adept at finding and using drugs, and not getting caught or sent to treatment. The longer SUD continues, the more complex and complicated the reversal is.
Ethically, “waiting” is untenable. Delayed intervention amplifies harm, entrenches bad behavior, and puts family, friends, and others at risk of harm. An earlier intervention and treatment might prevent loss of friends, family, and job, as well as halt the addiction from becoming entrenched.
We don’t withhold antihypertensives until catastrophic bleeds occur. We don’t wait for myocardial infarction to begin statins. Medicine emphasizes upstream prevention and treatment. While many perceive addiction as a choice, impaired MDs will tell you they wish someone had intervened and helped them earlier.
The directors of the National Institute on Drug Abuse and the National Institute on Alcohol Abuse and Alcoholism proposed, in 2022, earlier identification and intervention for substance use and its consequences. Volkow, Koob, and McLellan introduced this preaddiction concept by paralleling prediabetes. These researchers used mild to moderate Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, SUD criteria to help define pre-addiction, allowing early detection, brief treatment, or intervention before addiction-related neurobehavioral and psychosocial collapses occurred.
Research shows that at mild to moderate levels of SUD severity, patients often retain executive function, can reassert control over drugs, and may still re-engage and preserve intact relationships, work roles, and decision-making. At this preaddiction point, brief interventions, outpatient treatment, or educational measures have great potential to resolve the preaddiction. Sometimes, treatment might comprise advice and education rather than weeks in a treatment facility. In addition, early interventions may not require anti-craving medications, detoxification, opioid treatment medications, hospitalization, or extensive monitoring.
Preaddiction thinking supports early engagement, attacks denial, and normalizes a preventive mindset. Preaddiction communicates risk while preserving agency, as with prediabetes. It gives clinicians a structured rationale to screen, counsel, and refer before severe illness.
Nowhere is “raising the bottom” more visible than in PHPs. These state-based programs often identify impaired doctors from anonymous reports of patients, staff, or other providers. They protect patients from impaired physicians by managing them through structured evaluation, mandated treatment, regular toxicology testing, workplace monitoring, and ongoing recovery support—often for five or more years.
This model is widely celebrated, even though its success depends partly on external leverage: Physicians are often told noncompliance may result in license suspension and loss of professional status. In a five-year, multi-state study, DuPont and colleagues found that more than 70 percent of the doctors returned to practice, sustaining functional recovery. The model used early identification, accountability, structured care, serial urine testing, and long-term follow-up. It’s preventive, continuous, and outcome-driven.
The PHP system contradicts the “hitting bottom” mantra. It’s a real-life demonstration of what addiction care could be: long-term, hopeful, and outcome-driven, but with accountability. The limited application of such systems beyond professional circles reflects a profound inequity—not a clinical limitation.
Physician colleagues have moral, ethical, and legal obligations to report coworkers whose impairment threatens patients. Avoiding “punishment” and promoting sharing, shame reduction, and physicians helping each other in camaraderie while in treatment is critical to the success of physician programs.
When structured and ethical, coercion may paradoxically enhance autonomy by restoring capacity. Treat coercion as a clinical tool—not punishment. Integrate preaddiction into medical education, focusing on prevention, brain changes, and ethical duties.
“Bottom” need not be the destination just before treatment. Waiting or delaying intervention until full disorder or voluntary self-referral risks disease progression, more entrenched brain/behavior changes, worse prognosis, and higher costs.
To align addiction with other chronic medical conditions, SUD screening must be routine for every healthcare, clinic, or emergency department visit. Duration, age of initiation at use, and severity should be assessed. The preaddiction concept provides a teachable inflection point rather than the binary “normal vs addicted,” and intervention may change the trajectory. Brief interventions may be the only treatment needed if interventions start early enough.
Medicine should abandon the myth that people with SUDs must earn the right to be helped by suffering “enough.” Medicine has shown numerous benefits of early screening, intervention, and assisting patients in changing. If we can intervene early for hypertension, for type 2 diabetes, and for breast and colon cancer, we can do the same for addiction. What’s holding us back?
Source: https://www.psychologytoday.com/us/blog/addiction-outlook/202511/preaddiction-intervention-could-save-lives

Opening Statement from NDPA:
Commentary on psychiatry and its interaction with drug problems: Whilst this article sometimes includes CCHR’s campaigning rhetoric (and CCHR do much good work) there is also much of generic interest and usefulness on this specific subject – both in the article text and in the sources listed. For this reason, we include this in NDPA’s archive. (CCHR’s background and work can be reviewed via info@cchr.org.uk)

LOS ANGELES, Calif., Nov. 3, 2025 (SEND2PRESS NEWSWIRE) — Each May and October, millions are urged to “raise awareness” for mental health through national and international campaigns, including World Mental Health Day in October. Yet, according to the mental health industry watchdog, Citizens Commission on Human Rights International (CCHR), many of the advocacy campaigns driving these observances are dominated by pharmaceutical interests and a biomedical model reliant on psychotropic drugs, electroshock, and even psychosurgery. The outcome has been catastrophic: more than 76 million Americans take psychiatric drugs, and an estimated 100,000—including children as young as five—are electroshocked annually.
CCHR warns that modern mental-health awareness campaigns are not about understanding the mind but promoting psychiatry’s drug-driven model of “treatment.” Since its founding in 1969, the organization has used these awareness months to expose psychiatric abuse and coercion—particularly the drugging, electroshocking, and violent restraint of children in behavioral facilities. Working with parents, doctors, and lawmakers, CCHR has helped establish hundreds of laws globally to protect against psychiatric harm, including the first U.S. bans on electroshock for minors in California (1976) and Texas (1993), and the 1983 prohibition of Deep Sleep Treatment in Australia following 48 patient deaths—now a criminal offense to administer it in New South Wales and Western Australia.
CHALLENGING DRUG-INDUCED VIOLENCE
CCHR has documented the tragic outcomes of psychiatry’s drug-based approach, including its potential links to acts of senseless violence. It testified before the first inquest into the deaths of eight victims of a Kentucky mass shooting in 1989, where the perpetrator’s psychiatrist acknowledged that the antidepressant Prozac (fluoxetine) potentially contributed to the crime. A decade later, CCHR obtained confirmation that Columbine ringleader Eric Harris had the antidepressant Luvox in his system—despite clinical trials showing the drug could “form of psychosis characterized by exalted feelings, delusions of grandeur…and overproduction of ideas.”[1]
The watchdog’s efforts led to a 1999 Colorado government hearing on psychiatric drugs and violence, with the chair, State Rep. Penn Pfiffner, stating: “There is enough coincidence and enough professional opinion from legitimate scientists to cause us to raise the issue and to ask further questions.”[2] Working with Patricia Johnson, then-member of the Colorado State Board of Education, CCHR helped obtain a precedent-setting resolution urging academic—not chemical—solutions for classroom issues.[3]
CCHR also joined with medical experts and parents to press the U.S. Food and Drug Administration to issue its 2004 “black box” warning that antidepressants can cause suicidal behavior in children, which was later expanded in 2007 to include young adults up to age 24. Today, studies confirm that 46–71% of antidepressant users experience emotional blunting, dulling empathy, and increasing detachment—a factor present in numerous violent tragedies.[4]
Further reforms followed. In 2004, CCHR helped secure the federal Prohibition of Mandatory Medication amendment, banning schools from forcing children to take psychotropic drugs as a condition of education. Three years later, language CCHR helped introduce into the FDA reform bill required pharmaceutical ads to direct consumers to report drug side effects, causing adverse drug reporting to increase by 33 percent.[5]
CCHR’s investigations have also helped expose corruption and abuse in the psychiatric hospital and “troubled teen treatment” industry. Working with whistleblowers and journalists, it uncovered coercive admissions and insurance fraud within major private psychiatric hospital chains, leading to multiple state and federal investigations, criminal penalties, and closure of hundreds of abusive facilities. New laws were enacted to prohibit “bounty hunter” practices used to capture insured individuals for involuntary commitment and billing exploitation.[6]
Raising awareness, CCHR emphasizes, means parents can make better-informed choices and seek non-invasive, evidence-based help for their children. One expert has described the psychiatric polypharmacy trend as creating “a generation of child guinea pigs.” As The New York Times reported, “many psychiatric drugs commonly prescribed to adolescents are not approved for people under 18. And they are being prescribed in combinations that have not been studied for safety or for their long-term impact on the developing brain.”[7]
In 2013, nearly 8.4 million American children were taking psychiatric drugs.[8] By 2020, the IQVIA Total Patient Tracker Database showed that number had dropped to 6.1 million[9]—a notable decline that CCHR attributes in part to heightened public awareness, stronger warnings, and parental advocacy. However, millions of children remain drugged, underscoring that while progress has been made, the systemic overreliance on psychotropic drugs continues.
In addition to its feature-length documentaries, CCHR produces short educational videos on its YouTube channel to inform the public about mental health abuses and their prevention. Working alongside doctors, whistleblowers, parents, consumers, and civil and human rights organizations, CCHR continues to supply legislators and government agencies with documentation exposing psychiatric abuses and driving legislative reform to safeguard consumer and patient rights.
Today, both the World Health Organization (WHO) and United Nations agencies are calling for an end to coercive psychiatric practices—particularly those inflicted on children. Yet much of the mental-health establishment, including “patient-advocacy” groups with deep pharmaceutical ties, remains silent—endorsing mass drugging instead of confronting its documented dangers.
For more than five decades, CCHR International, which was originally established by the Church of Scientology and eminent professor of psychiatry, Dr. Thomas Szasz, has been a catalyst for reform, exposing human-rights violations in psychiatry and helping to achieve legislative and cultural change that has already begun to reduce child drugging and public acceptance of coercion. Its continuing campaigns seek a mental-health system based on transparency, informed consent, and respect for human dignity—affirming that lasting mental health will come not through drugs or shocks, but through compassion, truth, and accountability.
To learn more, visit: https://www.cchrint.org/2025/10/31/cchr-exposes-harms-behind-todays-mental-health-awareness-campaigns/
Sources:
[2] https://www.cchrint.org/2023/01/16/school-mental-health-programs-questioned-after-6-year-old-shot-teacher/; Kelly P. O’Meara, “A Different Kind of Drug War,” Insight Magazine, 13 Dec. 1999
[3] https://www.cchrint.org/2023/01/16/school-mental-health-programs-questioned-after-6-year-old-shot-teacher/; “Resolution: Promoting the Use of Academic Solutions to Resolve Problems with Behavior, Attention, and Learning,” Colorado State Board of Education, 11 Nov. 1999
[4] https://www.cchrint.org/2022/09/05/the-travesty-of-6-million-youths-on-psychotropics-a-expert-calls-it-a-generation-of-child-guinea-pigs/; https://www.verywellmind.com/can-antidepressants-make-you-feel-emotionally-numb-1067348
[5] https://www.cchrint.org/about-us/cchr-accomplishments/
[6] https://www.cchrint.org/about-us/cchr-accomplishments/
[7] https://www.cchrint.org/2022/09/05/the-travesty-of-6-million-youths-on-psychotropics-a-expert-calls-it-a-generation-of-child-guinea-pigs/; https://nypost.com/2022/08/29/the-ny-times-suddenly-discovered-were-giving-kids-dangerous-drugs/; https://www.nytimes.com/2022/08/27/health/teens-psychiatric-drugs.html
[8] https://www.cchrint.org/2016/11/30/cchr-launches-parents-know-your-rights-campaign/
[9] https://www.cchrint.org/psychiatric-drugs/children-on-psychiatric-drugs/
Source: https://www.yourvalley.net/stories/cchr-warns-mental-health-awareness-masking-drug-and-shock-abuse,630679


The first issue relevant to this paper is the category of ‘drug’ itself. The question is whether this category—central to the Brain Disease Model of Addiction (BDMA)—is rooted in hermeneutic injustice. A useful starting point is the work of British drug historian Porter (1996). In a paper tracing the historical origins of the “drug problem” in Britain, Porter argues that the concept of a drug is historically contingent:
“If you had talked about the ‘drug problem’ two hundred years ago, no one

Source: https://rollingout.com/2025/10/13/ways-parents-protect-teens-from-drugs/
Young people are being warned that they risk irreparable bladder damage, poisoning and even death if they take ketamine, synthetic opioids or deliberately contaminated THC vapes, as part of a new anti-drugs campaign.
Launching today (16 October 2025), the campaign, which includes online films, will target 16 to 24 years olds and social media users, following a worrying rise in the number of young people being harmed by drugs. There has been an eight-fold increase in the number of people requiring treatment for ketamine since 2015.
Supported by £310 million investment in drug treatment services, this initiative directly supports the government’s Plan for Change mission to create safer streets by reducing serious harm and protecting communities from emerging drug threats.
Health Minister Ashley Dalton said:
Young people don’t always realise the decision to take drugs such as ketamine can have profound effects. It can destroy your bladder and even end your life.
We’ve seen a worrying rise in people coming to harm from ketamine as well as deliberately contaminated THC vapes and synthetic opioids hidden in fake medicines bought online.
Prevention is at the heart of this government’s approach to tackling drugs and this campaign will ensure young people have the facts they need to make informed decisions about their health and safety, so they think twice about putting themselves in danger.
As part of the campaign, experts will highlight particular risks, including the:
Resources will be available for schools, universities and local public health teams with content available on FRANK, the drug information website.
There are growing concerns about novel synthetic opioids, particularly nitazenes, which are increasingly appearing in counterfeit medicines sold through illegitimate online sources. Users purchasing these products are typically younger and more drug-naïve.
Reports of harms from THC vapes have also increased, with many products containing synthetic cannabinoids (commonly known as ‘spice’) that have higher potency and unpredictable effects.
Katy Porter, CEO, The Loop, said:
The Loop welcomes the further investment in evidence-based approaches and support to reduce drug-related harm.
Providing accurate, non-judgemental information equips and empowers people to make safer choices and can help reduce preventable harms.
Drug poisoning deaths reached 5,448 in England and Wales in 2023, the highest number since records began in 1993. The campaign emphasises that while complete safety requires avoiding drug use altogether, those who may still use substances should be aware of the risks and know how to access help and support.
The campaign underlines that ketamine’s medical applications do not make illicit use safe, with urologists increasingly concerned about young people presenting with severe bladder problems from recreational ketamine use.
Resources will be distributed to local public health teams, drug and alcohol treatment services, youth services, schools and universities. The campaign provides clear information on accessing help and support for those experiencing drug-related problems or mental health issues.
This year the Department of Health and Social Care is also providing £310 million in additional targeted grants to improve drug and alcohol treatment services and recovery support in England, including specialist services for children and young people.
For information and support on drug-related issues, visit www.talktofrank.com or call the FRANK helpline on 0300 123 6600.
How to watch this YouTube videoThere’s a YouTube video on this page. You can’t access it because of your cookie settings.You can change your cookie settings or watch the video on YouTube instead:Ket: while each high lasts minutes, for some the damage to their bladder could last forever
How to watch this YouTube videoThere’s a YouTube video on this page. You can’t access it because of your cookie settings.You can change your cookie settings or watch the video on YouTube instead:Synthetic opioids: what are they and why are they so dangerous?
Additional resources for professionals and educators will be available through local public health networks.
The £310 million additional funding for drug treatment services is separate from the public health grant.
Source: https://www.gov.uk/government/news/young-people-given-stark-warning-on-deadly-risks-of-taking-drugs
A popular class of therapies for treating diabetes and obesity may also have the potential to treat alcohol and drug addiction, according to a new paper published in the Journal of the Endocrine Society.
The therapies, known as Glucagon-Like Peptide-1 Receptor Agonists (GLP-1RAs), present an encouraging approach to treating alcohol and other substance use disorders.
“Early research in both animals and humans suggests that these treatments may help reduce alcohol and other substance use,” said lead researcher Lorenzo Leggio, M.D., Ph.D., of the National Institute on Drug Abuse (NIDA) and the National Institute on Alcohol Abuse and Alcoholism (NIAAA), both part of the National Institutes of Health (NIH) in Bethesda, Md. “Some small clinical trials have also shown encouraging results.”
Current Treatment Options Are Limited
Substance use disorders are diagnosed based on criteria that can be grouped into four categories: physical dependence, risky use, social problems, and impaired control.
The negative consequences of substance use disorders represent a global problem, affecting individuals, families, communities, and societal health at large. For instance, research indicates that alcohol is the most harmful drug, with consequences that extend beyond individual health to include related car accidents as well as gun and domestic violence, researchers note.
Despite the high prevalence and consequences of alcohol and other substance use disorders, less than a quarter of people received treatment in 2023.
Underutilization is due to a variety of barriers at the patient, clinician, and organizational levels, not the least of which is the stigma associated with substance use disorders, according to the study. “Current treatments for [alcohol and other substance use disorders] fall short of addressing public health needs,” the researchers wrote.
GLP-1s and Their Potential to Treat Addiction
GLP-1 therapies have gained widespread renown in recent years for their ability to address obesity and significantly reduce weight.
In addition to its inhibitory effects on gastrointestinal systems, GLP-1 has key functions in the central nervous system, the study notes. Among them, GLP-1R activation within the central nervous system curbs appetite and encourages individuals to eat when hungry and stop eating when they are full.
Some forms of obesity have been shown to present biochemical characteristics that resemble addiction, including neurocircuitry mechanisms, the study says, acknowledging that such conclusions are controversial.
“Pathways implicated in addiction also contribute to pathological overeating and obesity,” the study says.
With this pathway in mind, researchers in recent years have looked at GLP-1s as a potential therapy to address substance use disorders. Preclinical and early clinical investigations suggest that GLP-1 therapies modulate neurobiological pathways underlying addictive behaviors, thereby potentially reducing substance craving/use while simultaneously addressing comorbid conditions.
Studies that examine GLP-1 effects on substance use disorders include:
Leggio and his colleagues caution that more and larger studies are needed to confirm how well these treatments work. Additional studies will help unveil the mechanisms underlying GLP-1 therapies in relation to addictive behaviors and substance use.
But that hasn’t dampened the optimism for these therapies to address the serious problems found in substance use disorders.
“This research is very important because alcohol and drug addiction are major causes of illness and death, yet there are still only a few effective treatment options,” Leggio said. “Finding new and better treatments is critically important to help people live healthier lives.”
Other study authors are Nirupam M. Srinivasan of the University of Galway in Galway, Ireland; Mehdi Farokhnia of NIDA and NIAAA; Lisa A. Farinelli of NIDA; and Anna Ferrulli of the University of Milan and Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS) MultiMedica in Milan, Italy.
Research reported in this press release was supported in part by NIDA and NIAAA. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Source: https://www.endocrine.org/news-and-advocacy/news-room/2025/glp1s-show-promise-in-treating-alcohol-and-drug-addiction
by Gabrielle Humphreys & Natalie Finch – BMC (BioMedCentral) –
Lived experience recovery organisations (LEROs) are social support services facilitated by those who have shared lived experience. Typically, they aim to build shared identity and reducing stigma in this area, although there is limited knowledge on the experiences of those using LEROs, with research rarely permitted into these groups. The current study aims to provide insight into these groups, examining the experiences of service users in a UK-based LERO focussed on substance use disorder recovery.
Fifteen service users were interviewed about their experiences attending this LERO. Transcripts from these semi-structured interviews were thematically analysed by authors, with an inductive approach adopted.
Eight themes and 10 sub-themes were identified. Themes were; Feeling supported in recovery, Experiencing life outside of substance use disorder, Fun, Skills acquisition, Preventing relapse by filling time, Gaining a sense of community, Psychological impact, and Changes in public perception. Participants reported having a positive experience within this LERO, particularly in comparison to traditional treatment pathways. Specifically, participants highlighted feelings of self-worth, belongingness, and enjoyment from this LERO – experiences they felt made this treatment pathway unique.
This paper highlighted the importance of peer support in substance use disorder recovery. Embedding those with lived experience into services was highly valued by participants and generated a unique culture of comfort, hope and opportunity. Although the scope of this study was limited to participants only currently attending this organisation, those interviewed significantly valued this LERO, highlighting their future potential to alleviate the lack of satisfaction reported by some around traditional treatment methods.
To access the full article, please click on the ‘Source’ link below:
Source: https://substanceabusepolicy.biomedcentral.com/articles/10.1186/s13011-025-00671-9
![]()
Received: 09 October 2025
The American College of Obstetricians and Gynecologists (ACOG) has released new clinical consensus guidance recommending universal screening for cannabis use across all reproductive stages—pre-pregnancy, pregnancy, and postpartum—with a clear message: there is no safe level of cannabis use for mothers or infants.
Despite mounting evidence of risk, cannabis use during pregnancy and lactation is increasing, fueled by legalization, social acceptance, and a lowered perception of harm. ACOG emphasizes that no medical indications exist for cannabis use during pregnancy or after birth.
To support prevention and care, ACOG’s clinical consensus on Cannabis Use in Pregnancy and Lactation provides evidence-based guidelines for screening, counseling, and reducing use.
Below are key takeaways from ACOG’s new clinical consensus.
Risks to Fetus and Newborn
· THC, the psychoactive component, crosses the placenta and reaches the fetus; THC also transfers into breast milk.
· Prenatal cannabis exposure is associated with:
· Increased risk of low birth weight, small-for-gestational-age infants, NICU admission, perinatal mortality
· Altered neonatal behaviors (arousal, regulation, excitability)
· Possible long-term neurocognitive, behavioral, and memory challenges, ADHD, and greater susceptibility to psychiatric disorders or substance use later in life
· While more research is needed, existing evidence shows clear cause for concern.
Risks During Lactation
· Data on cannabis use while breastfeeding are limited; ACOG discourages use during lactation due to THC transfer into breast milk and potential developmental impacts.
· Clinicians should encourage cessation while continuing to support breastfeeding.
Recommendations for Clinicians
1. Universal Screening & Counseling
· Screen all patients (pre-pregnancy, pregnancy, postpartum) via interview or validated tools (e.g. TAPS, CRAFFT, S2BI).
· Avoid biologic testing (urine, hair, etc.) as a routine screening tool.
· Educate that cannabis has no medical indication during pregnancy or postpartum.
2. Advise Cessation or Reduction
· Encourage patients to stop or reduce cannabis use during pregnancy and breastfeeding, offering nonjudgmental support.
3. Supportive Behavior Change Strategies
· Use motivational interviewing, address social determinants, and identify barriers to quitting.
· Provide access to home visits, CBT, and digital or text-based supports for behavior change.
4. Legal, Ethical, and Equity Considerations
· Policies on drug testing, child protective services (CPS) reporting, and criminalization vary widely.
· Black and minority birthing people are disproportionately subject to drug testing and CPS referrals, despite similar substance use rates.
· Clinicians should ensure informed consent, understand local policies, and work to reduce bias in maternal care.
Source: Drug Free America Foundation | 333 3rd Avenue N Ste 200 7278280211101 | Saint Petersburg, FL 33701 US
by Ryan Hesketh – Talking Drugs – Posted on September 15, 2025
In November, the World Health Organisation (WHO) will issue its long-awaited recommendation on whether the coca leaf should remain listed under the UN’s most restrictive drug controls.
For decades, the coca leaf has been treated in international law as little more than raw material for cocaine. The 1961 Single Convention on Narcotic Drugs, following the advice of a deeply flawed 1950 WHO report, placed coca in Schedule I, equating its potential harm from use with that of heroin. This decision criminalised traditional use by Indigenous peoples in the Andes, despite millennia of practice, ignoring both its cultural and medical significance.
Now, with WHO experts due to report their findings in September, attention is turning to whether the organisation can finally correct the record.
Critical timeline
Bolivia’s government initiated the review in 2023, arguing that coca’s scheduling was based on flawed information and infringed on indigenous rights. Since then, the WHO has tasked independent experts with conducting research on coca, its harms, and the potential impacts of change. Those experts are due to report their findings to the Executive Committee in late September, a crucial step on the pathway to potential change.
From there, the Expert Committee will meet in late October, finalising its report and recommendation in time for member states to consider ahead of the UN Commission on Narcotic Drugs’ (CND) reconvened session in December. The formal vote on coca’s scheduling, however, won’t take place until March 2026 in Vienna.
Luis Arce, the former president of Bolivia, holding coca leaves in 2022. Author: Vice Ministry of Communication of Bolivia
Uncertain outcomes
There are essentially three potential outcomes from the review. First, no action. Either the WHO makes no recommendation, which would result in no possibility of a vote, or states vote to maintain coca’s current Schedule I classification. Few expect the WHO to recommend keeping coca in its current schedule. “It’s hard to imagine they’d come to the conclusion that coca belongs where it is,” according to John Walsh, Director for Drug Policy and the Andes at the Washington Office on Latin America (WOLA).
If the review recommends a change in Coca’s scheduling, it would likely move down to either a Schedule II or III – still keeping its classification as a ‘narcotic drug’ subject to most treaty provisions. However, such a move would allow for certain traditional uses of coca and could be seen as a political compromise between those favouring full rescheduling and those favouring prohibition. This would create a clear difference in the scheduling for Coca and cocaine, similar to how opium products and the opium poppy are scheduled. Opium poppies are in Schedule II, while heroin is in Schedule I, reflecting the differing harms of the plant and its derivatives. Though rescheduling might be the most politically expedient outcome, and may align more closely with the UN’s Declaration on the Rights of Indigenous Peoples, it would still be very short of full removal, according to Walsh.
Finally, the result hoped for by many states and drug policy reform advocates: coca could be completely removed from the drug control treaties. This would mean that coca “would no longer be considered a controlled substance. It would open the way to legal natural commerce,” according to Walsh.
While the size of such a market is hard to estimate, its significance would be massive. Coca teas, flours, and medicinal extracts already circulate domestically in the Andes – only legally within Bolivia as the country had left and re-joined the UN drug control conventions in 2013 – but international markets remain blocked by treaty restrictions.
Yet there are also risks. Walsh cautions: “There’s a concern, even among those who want coca removed, that those who have guarded the tradition could be undermined.” Comparisons to the cannabis market loom large, where capital from the Global North has quickly moved into spaces originally meant by marginalised communities. The vision of a future un-criminalised market for coca opens future concerns, such as control mechanisms that avoid biopiracy and endorse fair benefit-sharing, particularly with communities that have been destroyed by the plant’s prohibition. The Nagoya Protocol, which addresses protections against the exploitation of genetic resources and Indigenous knowledge, is often cited as a model for future control.
Even in the case of full removal, coca wouldn’t be completely free of international prohibition. “Coca destined to become cocaine would still be illegal; that wouldn’t be optional,” according to Walsh. Better controls to determine the end use of coca would have to be developed.
Politics and removal
In theory, removing coca from Schedule I requires only a simple majority of CND member states. In practice, however, bloc politics loom large. “As a formal matter, there’s no veto. But in a practical matter, the EU looms large,” Walsh explains, given the bloc’s significant role in driving global demand for cocaine. If European states vote together against rescheduling, the motion would be unlikely to pass. However, if the EU allows states to vote individually, the change is much more likely to happen.
The United States’ position is also critical. As Walsh puts it, “It would be difficult to imagine if the US would be supportive of removing coca entirely.” But, though the US was once the world’s biggest supporter of draconian drug laws, its international influence may be waning. The current administration’s defunding of global aid, much of which supported harm reduction and drug prevention programmes, have reduced the US’ ability to enact soft power internationally. President Trump’s “transactional” politics, according to Walsh, may be a signal to countries that they can go their own way on policy while the US is pursuing a more isolationist approach to international relations.
Russia, too, will be notably absent. Having not achieved sufficient votes to remain part of the CND in April 2025, Russia will not be voting on UN drug-related matters from 2026 onwards. Walsh said that “Russia has taken the mantle from the US as ‘drug warrior’” and could’ve stood staunchly against coca’s reclassification. Their absence, therefore, may open new horizons.
The coca review is primarily supported by Bolivia and Colombia, with Canada, Czechia, Malta, Mexico, and Switzerland publicly supporting their position. Some coca-producing nations, notably Peru, are not in favour of reclassification. The country’s drug control agency, DEVIDA, recently argued that reclassifying coca “could become a perverse incentive to increase its diversion to the production of cocaine,” as well as increasing deforestation and food insecurity, especially for indigenous people.
But for some, Peru’s lack of support for the review has more to do with its political priorities than any attempt at harm reduction. “Peru’s denial to support this is indeed very odd, but is a reflection of the kind of political regime it is living under,” says Pien Metaal of the Transnational Institute (TNI). “The Boluarte government is the typical white Lima elite that has ruled Peru over the past decades, with no connection to the hearts and minds of the Peruvian people.”
Indigenous resistance
The roots of the current review go back to decades of Indigenous advocacy. The UN Declaration on the Rights of Indigenous Peoples recognises the right to maintain and protect traditional medicines and cultural practices. Yet international drug treaties continue to criminalise coca chewing and related practices in many countries.
“There has never been a credible medical or scientific basis for the prohibition of coca leaf,” according to Metaal. “Its inclusion in the 1961 Convention was a political act, not a scientific one.”
Underlying the review is a reckoning with the colonial assumptions that shape global drug control to this day. The 1950 WHO study that underpinned coca’s prohibition dismissed Indigenous practices as harmful and regressive, ignoring evidence of its benign cultural role. For many advocates, the current review is an overdue opportunity to correct that record. As Metaal argues, “This is not just about drug policy. It is about dignity, cultural survival, and Indigenous rights.”
Impending Change
For coca-using and growing communities, the implications are immediate. Continued criminalisation undermines cultural practices, justifies militarised eradication, and fuels human rights abuses. Removing the plant from international control could finally legitimise its traditional use, defund eradication policies, and unlock new economic opportunities grounded in heritage rather than prohibition.
As Walsh reflects: “In five years, I hope that we’re able to see a genuinely growing understanding of how natural coca products can really bring a lot of help to people around the world. I hope those markets can open up and can be beneficial to those communities that are most identified with coca.”
With the WHO’s deadlines fast approaching, the question is whether the international drug control system can rise to meet the moment—or whether it will once again fall back on outdated prejudices, leaving another generation of Indigenous peoples to fight for recognition of what they already know: that prohibition, not the coca leaf, is the problem.
===============================
Source: https://www.talkingdrugs.org/upcoming-who-coca-review-a-turning-point-for-global-drug-policy/
Authors: Cyntia Duval, Brandon A. Wyse, Noga Fuchs Weizman, Iryna Kuznyetsova, Svetlana Madjunkova & Clifford L. Librach
Published by: Nature Communications
Published: 09 September 2025
Abstract
Cannabis consumption and legalization is increasing globally, raising concerns about its impact on fertility. In humans, we previously demonstrated that tetrahydrocannabinol (THC) and its metabolites reach the ovarian follicle. An extensive body of literature describes THC’s impact on sperm, however no such studies have determined its effects on the oocyte. Herein, we investigate the impact of THC on human female fertility through both a clinical and in vitro analysis. In a case-control study, we show that follicular fluid THC concentration is positively correlated with oocyte maturation and THC-positive patients exhibit significantly lower embryo euploid rates than their matched controls. In vitro, we observe a similar, but non-significant, increased oocyte maturation rate following THC exposure and altered expression of key genes implicated in extracellular matrix remodeling, inflammation, and chromosome segregation. Furthermore, THC induces oocyte chromosome segregation errors and increases abnormal spindle morphology. Finally, this study highlights potential risks associated with cannabis use for female fertility.
Introduction
Cannabis consumption for both medicinal and recreational use and legalization have been rising globally1. Cannabis contains several classes of chemicals with cannabinoids being the most prominent; among these, tetrahydrocannabinol (THC) is the primary psychoactive compound and the most studied2. Notably, the concentration of THC in cannabis products has increased significantly, from an average of 3% (by weight) in the 1980s to around 15% in 2020, with some strains reaching 30% of THC2. The increase in frequency, ease of availability, and escalation in potency raises concerns about broader impacts on global human health, including reproductive health. Indeed, the main apprehension regarding THC and reproductive health stems from the importance of the endocannabinoid system in human reproduction3. Endocannabinoids, including N-arachidonoylethanolamide and 2-arachidonoylglycerol, are endogenous cannabinoids that play a central role in both male and female reproduction3, whereas THC is an exogenous cannabinoid. Extensive research has documented the effects of THC on male reproduction, highlighting an impact on sperm deoxyribonucleic acid (DNA) methylation 4,5,6,7 and sperm parameters8 including sperm concentration 9,10,11, morphology 12,13,14 and motility14. As for female health, literature reports the impact of cannabis use during pregnancy on pregnancy outcomes 15,16,17,18, placental development 18,19,20 and offspring health 18,20,21,22. However, to our knowledge, no studies have investigated the impact of cannabis on the human female gamete, the oocyte, a gap partly due to the challenge associated with obtaining these samples.
During in vitro fertilization (IVF) treatment, exogenous gonadotropins are administered in a process called “controlled ovarian hyperstimulation” which recruits multiple follicles and induces follicle growth. These recruited follicles, each containing an oocyte, are then collected by a physician in a procedure called oocyte retrieval. Oocytes are collected along with their surrounding microenvironment, including follicular fluid (FF) and supportive somatic cells (granulosa cells). The oocytes are isolated, and mature oocytes are used for subsequent in vitro fertilization. Using FF, our group has previously quantified Δ9-THC and its metabolites, 11-OH-THC and 11-COOH-THC 23,24, demonstrating that these compounds could reach the follicular niche. This is significant as it suggests that THC may directly alter the microenvironment where the oocyte matures. Furthermore, our group has shown that THC exposure altered human granulosa cell methylation in a concentration dependent manner23, and in vitro exposure modulated cannabinoid receptor dynamics in granulosa cells24. However, no human studies and only a few animal model studies have investigated the impact of cannabis directly on oocyte development with conflicting results 25,26,27,28,29.
Maturation of the oocyte is a unique and highly specialized process beginning in utero during fetal development. It is widely accepted that female neonates are born with a finite number of oocytes, which, following menarche, are recruited to mature in cohorts with each menstrual cycle30. Although oocytes are protected in the ovary by the blood-follicle-barrier, they remain highly sensitive to environmental factors31. Given their essential role in reproduction, any perturbations in their development and maturation could have profound effects on fertility and on future generations. Thus, understanding the impact of THC on oocyte health is critical for providing informed guidance and counseling to patients of the potential risks to their fertility and future offspring.
In this study, we determine the impact of physiologically relevant concentrations of THC on oocyte maturation, elucidate the transcriptomic changes induced by THC exposure and its effect on chromosome segregation, and compare our findings with a retrospective cohort study. Our investigation will aid in bridging the knowledge gap in our understanding of the sex-specific reproductive consequences of cannabis use and contribute to more effective and evidence-based patient counseling.
To read the full article, please click on the source link below
Source: https://www.nature.com/articles/s41467-025-63011-2
by Liz Mineo – Harvard Staff Writer -September 16, 2025
Study examining potential solution to treatment gap — especially in rural areas — gets federal funding cut
Between 1999 and 2023, approximately 806,000 Americans died from opioid overdoses, according to the Centers for Disease Control and Prevention. Yet of the estimated 2.4 million U.S. adults with opioid use disorder, only one in four receives medications that can reduce overdose risk.
Telehealth has shown promise as a potential tool to prevent opioid overdose deaths, but funding for a study launched last year by health economist Haiden Huskamp examining its use and impact was terminated as part of the mass cancellation of federal research grants by the Trump administration in May.
“A lot of our research, including that for this grant, is looking at why so few people are getting evidence-based treatments for substance use disorder,” said Huskamp, Henry J. Kaiser Professor of Health Care Policy at Harvard Medical School. “Medications for opioid use disorder are highly efficacious. They reduce opioid use; they reduce overdose risk and other negative outcomes. These medications save lives.”
A shortage of clinicians specialized in treating opioid use disorders — particularly in rural areas — presents a major barrier to receiving care, she said.
“Our work has been trying to understand, since the pandemic in particular, who was using telemedicine for opioid use disorder,” said Huskamp, “and whether the availability of care, via telemedicine, has meant that clinicians who treat substance use disorders are now seeing more patients in areas where there aren’t enough doctors who do this work.”
217Americans, on average, died each day from an opioid overdose in 2023, according to the CDC
For the past five years Huskamp, Ph.D. ’97, has been studying telemedicine as a strategy to expand access to opioid use disorder treatment and life-saving medications such as methadone, buprenorphine, and the quick overdose-reversal drug naloxone.
“Given the opioid epidemic that we are still in the middle of, telemedicine might be an answer because it could address a number of barriers to treatment access,” said Huskamp.
Although in May the CDC reported that opioid overdose deaths dropped from 83,140 in 2023 to 54,743 in 2024, the death toll remains high. According to the CDC, in 2023, on average, 217 people died each day from an opioid overdose.
The goal of Huskamp’s terminated four-year study, launched last year with a team of 15 researchers, was to provide evidence-based information on the efficacy of telemedicine that can guide policymakers as they address the opioid epidemic. It was a renewal of a previous grant, which yielded 24 different publications whose findings have informed new rules by the Drug Enforcement Agency to expand telemedicine access for treating opioid dependence. Funded by the National Institute on Drug Abuse, the latest research sought to examine quality of care and clinical outcomes by analyzing data from Medicare, Medicaid, commercial insurance, and national pharmacy claims.
Telemedicine for opioid use disorder became more widespread across the country during the COVID-19 pandemic, and researchers have been eager to probe the data to find out if it improved access to care for patients in remote areas, and how the quality of care compared to traditional in-person care.
“Anything we can do to try to improve the healthcare system to more effectively allow people to access care and to do so in a more efficient way is really important,” said Huskamp. “We need research like this to guide policymaking, so that we can improve the system as much as possible for people to get the treatment that they need.”
Source: https://news.harvard.edu/gazette/story/2025/09/only-1-in-4-addicted-to-opioids-takes-life-saving-meds-why/
By Neuroscience – September 21, 2025
The findings were significant, Thanos explains, because not only did the HIIT animals exhibit a preference for the saline chamber, they exhibited a clear aversion to the cocaine chamber. Credit: Neuroscience News
Summary: A new study shows that high-intensity interval training (HIIT) is more effective than moderate exercise at protecting adolescent lab animals from cocaine use. Animals exposed to HIIT developed a preference for non-drug environments and an aversion to cocaine, linked to increases in ΔFosB, a molecular switch involved in addiction.
These results suggest exercise intensity matters in shaping the brain’s reward system and its response to drugs. The findings may inform new strategies for using exercise as a personalized tool in substance use disorder prevention and treatment.
Key Facts
Source: University at Buffalo
People with substance use disorder who participate in recovery running programs have shown improved success in maintaining their sobriety and reducing their risk for relapse.
Those observations led Panayotis Thanos, a University at Buffalo neuroscientist who studies the brain’s reward system, to try to figure out the brain mechanisms behind that phenomenon.
In a new study published today in PLOS One, Thanos, PhD, senior research scientist in the Clinical and Research Institute on Addictions in the Jacobs School of Medicine and Biomedical Sciences at UB, and co-authors reveal that high-intensity interval training (HIIT) was more effective than moderate exercise in making adolescent lab animals avoid cocaine.
The researchers used adolescent lab animals because this is the age when most people who develop substance use disorder begin their exposure. The study focused on male rats only because previous observations have revealed some gender differences in drug-seeking behaviors between males and females. The researchers plan a future study on how HIIT affects females with regard to cocaine.
HIIT as personalized medicine
“The study shows that HIIT exercise, rather than moderate exercise, during adolescence may protect against cocaine abuse,” says Thanos, a faculty member in the Department of Pharmacology and Toxicology in the Jacobs School.
The findings provide evidence that HIIT could become a personalized medicine tool in drug abuse intervention.
“The key take-home is that not all exercise is created equal in terms of outcome,” Thanos says. “Exercise is not a binary therapeutic tool but rather we need to think about exercise as dose-dependent, the way we think of medicine as dose-dependent.”
In the study, rats exposed to HIIT exercise on a treadmill were compared to rats exposed to moderate treadmill exercise. Both groups then underwent a behavioral test called cocaine place preference, which trains the animal to discriminate between two chambers: one where they can access cocaine and one where they can access saline. Cocaine preference is when the animal spends more time in the cocaine chamber, while cocaine aversion is when the animal chooses to spend more time in the saline chamber.
The findings were significant, Thanos explains, because not only did the HIIT animals exhibit a preference for the saline chamber, they exhibited a clear aversion to the cocaine chamber.
Increase in a molecular switch for addiction
“We believe that the increase in aversion to cocaine happens in the HIIT animals,” Thanos says, “because of this exercise dose-dependent effect on the brain’s reward circuit that involves an increase we observed in ΔFosB.” ΔFosB is a transcription factor commonly referred to as a molecular switch for addiction and known to boost sensitivity to drugs of abuse.
“Our study showed that HIIT increased ΔFosB levels causing an aversion to consuming cocaine,” he adds.
The findings reveal new avenues that Thanos and his colleagues plan to explore, including how HIIT may affect brain metabolism.
“We know from recent studies in our lab with steady, moderate treadmill running that compared to sedentary animals, exercise decreased metabolism in the somatosensory cortex of the brain while activating other brain regions involved in planning and decision,” he says. “That activation may help dampen various aspects of cocaine abuse and relapse.”
The paper also discusses the need to better understand gender differences in preference for cocaine. “Future studies need to explore how HIIT affects cocaine preference in female rats,” Thanos says, adding that the literature in the field includes evidence that females seem to be more vulnerable to certain phases of addiction.
UB co-authors are Teresa Quattin, MD, UB Distinguished Professor in the Department of Pediatrics and senior associate dean for research integration in the Jacobs School; Nikki Hammond, a former graduate student; and Nabeel Rahman and Sam Zhan, former undergraduate students in Thanos’ lab. Other co-authors are from Washington University School of Medicine and Western University of Health Sciences.
Source: https://neurosciencenews.com/hiit-exercise-addiction-neuroscience-29715/
by Renata Glavak-Tkalić, Mara Šimunović, Katarina Perić Pavišić, Josip Razum, Desirèe Colombo – – 22 August 2025
ABSTRACT
Background
Substance abuse (SA) imposes a significant global health burden, demanding innovative and accessible interventions. Virtual reality (VR) offers a promising approach, providing engaging and personalized treatment experiences. However, rigorous evidence from randomized controlled trials (RCTs) on VR’s efficacy in the treatment and prevention of SA remains limited. This systematic review aimed to characterize VR interventions for substance-related disorders and evaluate their effectiveness.
Methods
To conduct this review, two researchers independently performed a comprehensive literature search across four databases using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Results
Twenty RCTs met the inclusion criteria, focusing on alcohol, nicotine and illicit drug use. These studies utilized diverse VR modalities, most frequently exposure therapy (n = 10) and cognitive-behavioural therapy (n = 5), followed by approach bias modification, skills training, cognitive rehabilitation, counterconditioning and psychoeducation. Interventions varied in level of immersion and interactivity. Although the evidence was mixed, 17 studies demonstrated positive effects on at least one outcome variable. Most studies focused on proximal outcomes (e.g., craving), which frequently showed improvement. Clinically meaningful outcomes (e.g., substance use reduction and abstinence) were less frequently assessed, with seven of 10 studies reporting improvement.
Conclusions
VR shows promise in addressing substance-related disorders, particularly for alcohol and nicotine. However, substantial heterogeneity in VR interventions highlights the need for further research to standardize methodologies, optimize treatment parameters and explore the underlying working mechanisms of VR interventions. Additional research is also needed to assess VR’s application to illicit drug use.
Summary
Virtual reality (VR)–based interventions, particularly those that integrate cue exposure therapy and cognitive behavioural therapy, show significant promise in reducing cravings and improving abstinence among individuals using alcohol and nicotine.
VR intervention and prevention programmes have positively impacted attitudes, intentions, cognitive function and physiological responses in substance users, indicating a broader therapeutic potential that extends beyond simply addressing addiction symptoms.
The considerable variability among VR interventions emphasizes the need for greater standardization in methodologies, treatment parameters and outcome measures.
Additional research is necessary to evaluate the applicability and efficacy of VR in the prevention and treatment of illicit drug use.
The full article can be accessed by clicking the ‘Source’ link below:
Source: https://onlinelibrary.wiley.com/doi/10.1002/cpp.70144?af=R
by Jan Hoffman – Published Aug. 25, 2025
Jan Hoffman is a health reporter for The New York Times covering drug addiction and health law.
San Francisco, Philadelphia and others are retreating from “harm reduction” strategies that have helped reduce deaths but which critics, including Trump, say have contributed to pervasive public drug use.
Safe drug-consumption materials distributed in the Tenderloin district of San Francisco, including naloxone, pipes and plastic straws.Credit…Mike Kai Chen for The New York Times
As fentanyl propelled overdose deaths to ever more alarming numbers several years ago, public health officials throughout the United States stepped up a blunt, pragmatic response. Desperate to save lives, they tried making drug use safer.
To prevent life-threatening infections, more states authorized needle exchanges, where drug users could get sterile syringes as well as alcohol wipes, rubber ties and cookers. Dipsticks that test drugs for fentanyl were distributed to college campuses and music festivals. Millions of overdose reversal nasal sprays went to homeless encampments, schools, libraries and businesses. And in 2021, for the first time, the federal government dedicated funds to many of the tactics, collectively known as harm reduction.
The strategy helped. By mid-2023, overdose deaths began dropping. Last year, there were an estimated 80,391 drug overdose deaths in the United States, down from 110,037 in 2023, according to provisional data from the Centers for Disease Control and Prevention.
Now, across the country, states and communities are turning away from harm reduction strategies.
Last month, President Trump, vowing to end “crime and disorder on America’s streets,” issued a far-flung executive order that included a blast at harm reduction programs which, he said, “only facilitate illegal drug use and its attendant harm.”
But his words, implicitly linking harm reduction to unsafe streets, echoed a sentiment that had already been building in many places, including some of the country’s most liberal cities.
San Francisco’s new mayor, Daniel Lurie, a Democrat who campaigned on a pledge to tackle addiction and street chaos, announced this spring that the city would step away from harm reduction as its drug policy and instead embrace “recovery first,” aspiring to get more people into treatment and long-term recovery. He banned city-funded distribution of safe-use smoking supplies such as pipes and foil in public places like parks. A year earlier, San Francisco voters had signaled their restiveness with pervasive drug use by approving a measure stipulating that some recipients of public assistance who repeatedly refused drug treatment could lose cash benefits.
Philadelphia stopped funding syringe services programs, which the C.D.C. has called “proven and effective” in protecting the public and first-responders as well as drug users. The city put restrictions on mobile medical teams that distribute overdose reversal kits and provide wound care for people who inject drugs, and stepped up police sweeps in Kensington, a neighborhood long known for its open-air drug markets and a focal point of the city’s harm reduction efforts.
Santa Ana, Calif., shut down its syringe exchanges; Pueblo, Colo., tried to do the same but a judge blocked enforcement of the ordinance.
Mayor Daniel Lurie of San Francisco, center, often walks through the Tenderloin district, where people experiencing addiction, mental illness and homelessness gather.Credit…Mike Kai Chen for The New York Times
Republican-dominated states have also been retreating from the approaches. In 2021, West Virginia legislators said that needle exchange programs had to limit distribution to one sterile syringe for each used one turned in and could only serve clients with state IDs. Last year, Nebraska lawmakers voted against permitting local governments to establish exchanges.
“Harm reduction” is a decades-old concept, grounded in the reality that many people cannot or will not stop using drugs. Since the 1980s, when AIDS activists began distributing sterile syringes to drug users to slow the spread of diseases, the expression has moved to the mainstream of addiction medicine and public health.
Over time, it has become shorthand for a wide range of approaches. Some are broadly popular and will certainly continue. In April, the White House’s office of drug control policy released priorities reaffirming support for drug test strips and naloxone, the overdose reversal medication that has become an essential item in first-aid kits in homes, restaurants and school nurse offices.
But critics contend that making drug use safer, with distribution of supplies and pamphlets directing how to use them, normalizes drug use and undercuts people’s motivation to quit and seek abstinence.
“The more you’re sort of funding and feeding the addiction, you’re going to get more addiction,” Art Kleinschmidt, now the head of the federal agency that oversees grants for substance abuse, said on a podcast last year. Such programs, he said, “definitely are breeding dependency.”
Others argue for nuance.
“Harm reduction is neither the singular solution to the overdose crisis nor a primary cause of public drug use and disorder,” said Dr. Aaron Fox, president of the New York Society of Addiction Medicine. “It’s one component of a spectrum of services necessary to prevent overdose deaths and improve the health of people who use drugs. But if communities want long-term solutions to homelessness, they need to work on expanding access to housing.”
Harm reduction supporters reject the notion that protecting people from the worst consequences of drugs encourages use.
“I don’t think the availability of sterile supplies really makes a difference about whether someone is going to start or continue using drugs,” said Chelsea L. Shover, an epidemiologist at the University of California, Los Angeles, who oversees Drug Checking Los Angeles, which tests the contents of drugs for individuals and public health agencies. “But I do think it will make a difference in terms of whether that person is going to be alive in a week or a month or a year, during which time they might get into recovery, whatever that may mean for them.”
Some addiction experts fear that a retreat from harm reduction will reverse the falloff in deaths from injection-related diseases.
“Hepatitis C and H.I.V. numbers will go up, and more people are going to die,” said Dr. Kelly Ramsey, a harm reduction consultant who practices addiction medicine at a South Bronx clinic.
While overdose deaths have fallen, it is unclear whether drug use itself has also slowed. In neighborhoods across the country, from Portland, Maine, to Portland, Ore., many residents complain that the harm to them from drug use, including crime and syringe street litter, has not been reduced.
Mr. Trump particularly called out a type of harm reduction known as “safe consumption sites” — sometimes labeled “overdose prevention centers.” They are supervised locations where people can inject drugs without fatally overdosing, found in Europe, Canada and Mexico. Often drug users can test their supplies right away and staff members can quickly administer overdose reversal medication if needed.
There are only three in the United States, and they make for easy political targets. In addition to many Republicans, prominent Democratic governors, including Gavin Newsom of California, Kathy Hochul of New York and Josh Shapiro of Pennsylvania, oppose them. The Pennsylvania senate voted to ban them. One, in Rhode Island, is protected by state and local law. But the other two, in New York City, which provide treatment referrals and support services, operate in a legal gray zone and could face federal scrutiny.
Opponents of harm reduction offer few specifics about how to get more people to stop using drugs and into treatment. Mr. Trump’s order directs the health secretary and the attorney general to explore laws to civilly commit addicted people who cannot care for themselves into residential treatment “or other appropriate facilities.” But it is silent about how such programs would be paid for.
The administration has already made major cuts to the Substance Abuse and Mental Health Services Administration, the federal agency that awards grants for prevention, treatment and recovery. It has slashed the agency’s staff and the grants it gives for a wide variety of prevention, intervention and treatment services.
Cuts to Medicaid included in the sweeping domestic policy bill enacted this summer are also likely to affect many people’s access to treatment and states’ ability to cover it. Robert F. Kennedy Jr., the health secretary, who is in recovery from a substance use disorder, has focused on nutrition, chronic disease and vaccines during his first six months in office and has said little about plans to address the drug crisis.
The battle over whether harm reduction should remain a primary goal or be secondary to getting users into treatment and restoring order to public streets has been joined most intensively in San Francisco.
There, ample social services and ferociously expensive housing had contributed to a large population living on the streets, many struggling with mental illness and addiction. Then, by 2020, fentanyl and Covid had slammed into the city.
At public meetings this spring, angry residents brandished signs, some reading “Harm Reduction Saves Lives” and others “Drug Enablism Kills.”
Although the city has adhered to regulations for state-funded Housing First programs, which offer permanent housing for homeless people without requiring them to be drug-free, Mr. Lurie recently presided over the opening of the city’s first transitional sober living residence, with 54 units for adults committed to abstinence.
The drive to adjust the city’s drug policy to recovery first has been led by Matt Dorsey, a member of the San Francisco Board of Supervisors, who is in recovery from a substance use disorder.
In an interview, Mr. Dorsey said he supports aspects of harm reduction, including the distribution of safe supplies. But he sees the strategy as more of a floor than a ceiling. “We need to make clear that the objective of our drug policy is a healthy, self-directed life free of illicit drug use,” he said.
The difficult challenge, he said, was how to attend to the rights of pedestrians who daily confront drug use, while also trying to “help people addicted to life-threatening drugs.”
To pay for additional treatment and services, he said, city officials are working on ballot measures to redirect tax revenue.
“Part of what gives me confidence that we will ultimately find the funding,” Mr. Dorsey added, “is that the alternative is unthinkable.”
Source: https://www.nytimes.com/2025/08/25/health/harm-reduction-san-francisco-trump.html

The discovery of a new painkiller offers relief with fewer side effects.
Morphine and other opioids are commonly used in medicine because of their strong ability to relieve pain. Yet, they also pose significant risks, including respiratory depression and drug dependence. To limit these dangers, Japan enforces strict rules that allow only specially authorized physicians to prescribe such medications.
In contrast, the United States saw widespread prescribing of the opioid OxyContin, which fueled a rise in the misuse of synthetic opioids like fentanyl. By 2023, deaths from opioid overdoses had exceeded 80,000, marking the escalation of a nationwide public health emergency now known as the “opioid crisis.”
Opioids may soon face competition. Researchers at Kyoto University have identified a new analgesic, named ADRIANA, that provides pain relief through a completely different biological pathway. The drug is now moving through clinical development as part of an international research collaboration.
“If successfully commercialized, ADRIANA would offer a new pain management option that does not rely on opioids, contributing significantly to the reduction of opioid use in clinical settings,” says corresponding author Masatoshi Hagiwara, a specially-appointed professor at Kyoto University.
The researchers drew their initial inspiration from compounds that imitate noradrenaline, a chemical released during life-threatening situations that activates α2A-adrenoceptors to reduce pain. While effective, these compounds carry a high risk of destabilizing cardiovascular function. By examining the relationship between noradrenaline levels and α2B-adrenoceptors, the team proposed that selectively blocking α2B-adrenoceptors could increase noradrenaline activity, stimulate α2A-adrenoceptors, and provide pain relief without triggering cardiovascular instability.
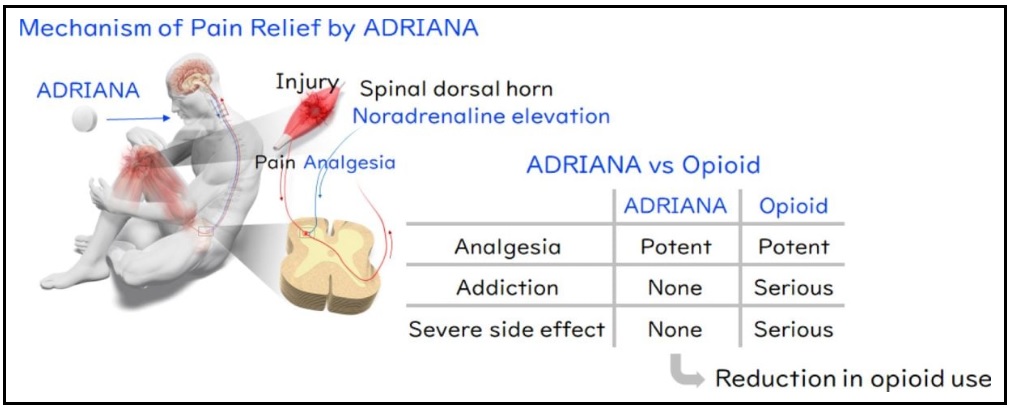
To test this idea, the scientists used a specialized method called the TGFα shedding assay, which allowed them to measure the function of different α2-adrenoceptor subtypes. Through compound screening, they succeeded in identifying the world’s first selective α2B-adrenoceptor antagonist.
After success in administering the compound to mice and conducting non-clinical studies to assess its safety, physician-led clinical trials were conducted at Kyoto University Hospital. Both the Phase I trial in healthy volunteers and the Phase II trial in patients with postoperative pain following lung cancer surgery yielded highly promising results.
Building on these outcomes, preparations are now underway for a large-scale Phase II clinical trial in the United States, in collaboration with BTB Therapeutics, Inc, a Kyoto University-originated venture company.
As Japan’s first non-opioid analgesic, ADRIANA has the potential not only to relieve severe pain for patients worldwide but could also play a meaningful role in addressing the opioid crisis — a pressing social issue in the United States — and thus contribute to international public health efforts.
“We aim to evaluate the analgesic effects of ADRIANA across various types of pain and ultimately make this treatment accessible to a broader population of patients suffering from chronic pain,” says Hagiwara.
Reference: “Discovery and development of an oral analgesic targeting the α2B adrenoceptor” by Masayasu Toyomoto, Takashi Kurihara, Takayuki Nakagawa, Asuka Inoue, Ryo Kimura, Isao Kii, Teruo Sawada, Takashi Ogihara, Kazuki Nagayasu, Takayuki Kishi, Hiroshi Onogi, Dohyun Im, Hidetsugu Asada, So Iwata, Jumpei Taguchi, Yuto Sumida, Suguru Yoshida, Junken Aoki, Takamitsu Hosoya and Masatoshi Hagiwara, 7 August 2025, Proceedings of the National Academy of Sciences.
DOI: 10.1073/pnas.2500006122
Funding: Japan Society for the Promotion of Science, Japan Science and Technology Agency, Japan Agency for Medical Research and Development
Source: https://scitechdaily.com/the-end-of-opioids-new-drug-could-change-the-way-we-treat-severe-pain/
by DAVID EVANS – 19 August 2025
There are established five schedules of controlled substances, to be known as schedules I, II, III, IV, and V.
(1) Schedule I–(A) The drug or other substance has a high potential for abuse.(B) The drug or other substance has no currently accepted medical use in treatment in the United States.(C) There is a lack of accepted safety for use of the drug or other substance under medical supervision.
(2) Schedule II–(A) The drug or other substance has a high potential for abuse.(B) The drug or other substance has a currently accepted medical use in treatment in the United States or a currently accepted medical use with severe restrictions.(C) Abuse of the drug or other substances may lead to severe psychological or physical dependence.
(3) Schedule III–(A) The drug or other substance has a potential for abuse less than the drugs or other substances in schedules I and II.(B) The drug or other substance has a currently accepted medical use in treatment in the United States.(C) Abuse of the drug or other substance may lead to moderate or low physical dependence or high psychological dependence.
(4) Schedule IV–(A) The drug or other substance has a low potential for abuse relative to the drugs or other substances in schedule III.(B) The drug or other substance has a currently accepted medical use in treatment in the United States.(C) Abuse of the drug or other substance may lead to limited physical dependence or psychological dependence relative to the drugs or other substances in schedule III.
(5) Schedule V–(A) The drug or other substance has a low potential for abuse relative to the drugs or other substances in schedule IV.(B) The drug or other substance has a currently accepted medical use in treatment in the United States.(C) Abuse of the drug or other substance may lead to limited physical dependence or psychological dependence relative to the drugs or other substances in schedule IV.
Moving marijuana to Schedule III would not legalize the drug, however, the change would greatly serve to benefit state legalized commercial marijuana companies who would no longer be subject to IRS Section 280E and thus could deduct business expenses and drastically increase their profit margins. This means more advertising and normalization. Not only would this mean that marijuana corporations would be able to deduct expenses for advertisements appealing to youth and the sale of kid-friendly marijuana gummies, but it would also dramatically increase the industry’s commercialization ability.
—
Source: www.drugwatch.org (drug-watch-international@googlegroups.com)
by UNODC – 20 August 2025

For over three decades, the United Nations Office on Drugs and Crime (UNODC) has supported non-governmental organizations (NGOs) in low- and middle-income countries implement substance use prevention projects that benefit youth around the world. This support has been made possible through the ongoing contributions of the Drug Abuse Prevention Centre (DAPC) in Japan since 1994. The DAPC Grants Programme enables civil society organizations to initiate and scale up prevention activities for youth and with youth aligned with the UNODC/WHO International Standards on Drug Use Prevention. The grants also empower young people to take active roles in supporting the health and wellbeing of their peers.
Following the 2024 Call for Proposals, which attracted more than 500 applications (more than double the previous year’s submissions), UNODC selected four new DAPC grant recipients through a multi-phased competitive process. Grantees from Cambodia, Iraq, Sri Lanka, and Zimbabwe will soon begin implementing their projects to support youth through locally grounded prevention efforts.
The Youth Aspire Development Trust, based in Zimbabwe, will be implementing their SPARK (Substance Prevention and Awareness for Resilient Knowledgeable Communities) project. The grantee will engage with schools and communities in the Chitungwiza region of Zimbabwe targeting students, teachers and parents. Teachers from local schools will receive training on classroom-based prevention strategies, early detection of risky behaviours, and ways to foster positive school climates. Students will also be selected as peer leaders and be equipped with life skills, refusal techniques, and resilience training to lead cascade sessions and positively influence other peers. Complementing these efforts, the grantee will also engage parents to strengthen their role in creating protective home environments for their family. And finally, to expand the reach of the programme, trained teachers and parents will conduct cascade trainings within schools and communities.
The Alcohol and Drug Information Centre (ADIC) in Sri Lanka will implement the project “Peer Power: Youth-Driven Substance Use Prevention and Resilience Building” in Colombo. Youth facilitators will be trained to mentor younger peer leaders, who will deliver interactive, skills-based workshops in local communities and schools with the support of ADIC’s resource persons. The project includes a baseline survey, capacity building for youth, creation of a tailored action plan, peer-to-peer education sessions, community and family engagement activities, and social media campaigns developed by youth. By combining in-person outreach with digital platforms, the project aims to enhance youth resilience and decision-making, empower and educate youth leaders, and strengthen community support for such initiatives.
In Cambodia, the grantee Mith Samlanh will implement its “Peer Prevention: A Youth-Driven Project Against Drugs” project by combining national and community-level initiatives. A national multimedia campaign, developed together with youth, will raise awareness about the risks of drug use through videos and prevention messages, reaching young people across social media platforms. In parallel, in-person awareness sessions will engage directly with communities in vulnerable areas of Phnom Penh, helping to bridge the digital divide and reach those who may not be active online. The grantee will also develop and integrate a Drug Prevention module into Mith Samlanh’s existing soft skills training for at-risk individuals, using evidence-informed methods to build resilience and enhance life skills. Additionally, a cascade Training of Trainers modality will strengthen local capacity by preparing teachers, social workers, youth champions, and local authorities to deliver prevention messaging and trainings to support youth and families across Phnom Penh.
In Iraq, the Bestan Child Society (Bustan Association) will implement the “Building Community Power to Prevent Youth Drug Use” project. The grantee will engage with community influencers such as teachers, sports coaches, youth leaders, and journalists to strengthen the local prevention capacity. Trained as prevention champions, they will integrate drug awareness and life skills into sports, arts, and peer-led activities that will be conducted in the target communities. Youth will also take part as informal peer educators through the 3S Initiative (Sport–Smile–Sleep), which will promote resilience and healthy lifestyles in young people. Also, youth co-created awareness materials will further extend the project’s reach through social media and community events.
UNODC is pleased to support these four new diverse projects under the DAPC Grants Programme. Each initiative reflects a strong commitment to prevention aligned with the Standards, youth engagement, and community-level action — key elements in building healthier lifestyles and safer environments for young people to grow and thrive in. For more information about the DAPC grants projects and the programme, please visit the Youth Initiative website and stay up to date through the UNODC PTRS social media channels (X, LinkedIn, Facebook).
Source: https://www.unodc.org/unodc/prevention/youth-initiative/youth-action/2025/August/introducing-new-dapc-grant-funded-projects.html
NEW YORK — U.S. Customs and Border Protection Deputy Commissioner John Modlin delivered remarks at a National Fentanyl Prevention and Awareness Day event today in Times Square.
The annual event, hosted by the nonprofit Facing Fentanyl, brings together impacted families and federal, state, and local law enforcement to draw national attention to the synthetic opioid epidemic.
“On behalf of the more than 65,000 fathers and mothers, and sons and daughters, who are also agents, officers and professional staff of CBP, we mourn with those who have lost a loved one to fentanyl poisoning,” said Deputy Commissioner Modlin. “Every hour of every day of the year, CBP is enforcing the law, across the land, in the air, and on the sea. Fentanyl is not just a public health threat – it’s a weapon. Any group that tries to poison Americans will face U.S. law enforcement and national security authorities.”
CBP supports the nation’s fight against fentanyl by prioritizing counter-fentanyl efforts across all operational environments. This includes stopping the ingredients, equipment, and the drug itself from entering or moving through the U.S. CBP has significantly increased its efforts to find and seize fentanyl at border crossings and checkpoints, using a variety of methods, such as officers’ instincts, drug-sniffing dogs, advanced scanning technology, artificial intelligence, and intelligence gathering to target and stop smugglers.
CBP’s approach to combatting fentanyl has grown to also include taking down the criminal groups that ship fentanyl, its ingredients, and pill-making equipment into the U.S. By working closely with law enforcement agencies both within the U.S. and in other countries, CBP helps investigate the larger criminal organizations, not just the individuals caught smuggling drugs at the border.
Fentanyl is a very dangerous drug that CBP first encountered in its final form around 2013-2014. Even a very small amount can be deadly. It’s cheap and easy to make, and there’s a high demand for it. Just one kilogram (about 2.2 pounds) of fentanyl already mixed into pills makes just over 9,000 pills. In contrast, one kilogram of fentanyl powder can make roughly 80,000 pills.
National Fentanyl Prevention and Awareness Day serves as a vital platform to highlight the devastating impact of synthetic opioids and the ongoing efforts to combat this epidemic. CBP’s participation underscores its unwavering commitment to protecting American communities and saving lives.
For more information on National Fentanyl Prevention and Awareness Day, visit DEA Fentanyl Awareness.
by Kevin Sabet August 22, 2025
In 2018, 27-year-old Bryn Spejcher, an inexperienced marijuana smoker in California, killed her boyfriend Chad O’Melia by stabbing him 108 times, a crime the local district attorney described as “horrific” and “one of the worst our medical examiner has ever seen.” A jury found Spejcher guilty of involuntary manslaughter, but she received only probation at sentencing because of a compelling presentation of her defense of cannabis-induced psychosis. Prior to the violent incident, Spejcher had taken two hits of legal marijuana from a bong, and claimed that she began “seeing things that weren’t there” and lost touch with reality. She also stabbed herself repeatedly in the neck, and stabbed her own dog. Law enforcement agents called to the scene had to break her arm with a metal baton to get her to let go of the knife; multiple Taserings had no effect.
Cases like Spejcher’s illustrate the stakes involved in the federal reclassification of marijuana. If President Trump follows through with such a move, the drug would remain illegal on the federal level, but would receive an imprimatur of being safer and face fewer restrictions, with significant commercial and social implications.
Yet voices across public discourse persist in asking: why should anyone care if President Trump does just that?
Celebrities like Mike Tyson and Joe Rogan and hedge-fund bosses like Andrew Lahde tell us that marijuana is no big deal. Numerous states have already legalized it for medical and recreational usage, and they claim to be regulating it well. If we are to believe the advocates, marijuana is a miracle cure for PTSD, anxiety, depression, and bipolar disorder — not to mention an unbeatable salve for the pain suffered by cancer patients.
So what sense does it make for this drug to sit in the same federal category as PCP and heroin? Isn’t marijuana’s placement in Schedule I, the most serious category, merely a relic of discredited thinking from the bad old days of the War on Drugs? It isn’t. To understand why it isn’t, and why a Trump move to reclassify weed would risk unmitigated harm to American health and safety, it’s first important to clear up some common misunderstandings around how and why drugs end up classified as they do.
Under the Controlled Substances Act of 1971, a five-part schedule was established for classification of potentially dangerous drugs. This schedule is emphatically not an index either of a drug’s “hardness” or a kind of unofficial charging and sentencing guide for prosecutors and judges. Placement is earned specifically through consideration of a drug’s accepted medical use and its abuse risk. Drugs with no accepted medical use and a high risk of abuse get placed in Schedule I.
That’s the commonality between marijuana and heroin; under federal law, the relevant agencies necessarily view them that way.
Neither has an accepted medical use, though both drugs have approved medicines derived from them that remain in lower schedules (the medicine dronabinol, for example, is synthesized THC, the active ingredient in marijuana, and is in Schedule III). Both have high risks of abuse. The argument that one is a “hard” drug and the other is not — which is debatable, especially given today’s ultra-high-potency weed — simply doesn’t come into play.
Nor does the criminal-justice question. Keeping marijuana in Schedule I isn’t, as critics have it, a carceral strategy; conversely, moving it into Schedule III isn’t a de-carceral one. Under a move to Schedule III, the drug would remain federally illegal, still subject to the enforcement power of the Drug Enforcement Administration and the Department of Justice. No low-level offender would see his sentence commuted. This is sort of beside the point anyway, since most low-level marijuana users never receive a sentence for anything.
But how can it be, another objection runs, that the drug has no medical use? Most US states currently allow doctors to recommend it.
That, again, is technically correct. But the decisions those states made to allow doctors (and in some cases, “designated caregivers”) to recommend marijuana to treat pain and other issues were political decisions, not medical or scientific ones. Voters stated a preference; that has no effect on how federal agencies are required by current law to view the question. The facts of just how those recommendations get handed out drive home that political aspect. In 2022, Pennsylvania saw some 132,000 medical-marijuana certifications, a third of the state’s total for that year, issued by only 17 doctors.
Those decisions, taken in the aggregate, don’t constitute an accepted medical use. Or at least, they didn’t until October 2022. That was the month the Biden administration directed its Department of Health and Human Services to look into a possible reclassification of the drug.
“This schedule is emphatically not an index either of a drug’s ‘hardness’ or a kind of unofficial charging and sentencing guide.”
Again, history is important here. Before the Biden process, the federal government had used an eight-factor test to determine how to schedule various drugs. Those factors focus on what the current and historical patterns of its abuse look like, as well as what that means for individual users, what risk it presents to public health, how likely it is to cause dependence (either physical or psychological), the state of the science around the drug and its pharmacology, and whether it’s a chemical precursor or “analogue” of another controlled substance.
By these metrics, marijuana is precisely where it belongs in Schedule I. The best science shows that it isn’t an effective medical treatment. One of the most frequent conditions it’s used to treat is chronic pain. But the 2017 study cited to prove its efficacy there has seen dozens of subsequent meta-analyses and reviews fail to support its conclusions; a 2022 study of a decade’s worth of surgical records from a Cleveland hospital even found that using marijuana actually increases pain after surgery.
The data also demonstrate that marijuana poses a significant risk of dependency: addiction rates are around 30% of all users and rising. Addiction in this case means exactly what it does for other substances: inability to quit, a need for ever more of the drug to achieve the same effect, and even withdrawal symptoms. Given the recent avalanche of data cataloguing marijuana’s harms specifically to cardiac and mental health — like a June British Medical Journal review connecting it to a two-fold risk of cardiovascular death or the massive Danish study from 2023 suggesting that as much as 30% of schizophrenia cases among men between 21 and 30 were linked to cannabis-use disorder — its wider public-health risks are glaringly clear.
The Biden administration supplanted the eight factors with a new system seemingly designed to push the drug into a less restrictive schedule. The Biden recommendation — likely a political compromise between the status quo and full legalization, timed just before Joe Biden’s re-election bid — also incorporated the shaky argument that because so many states have made political decisions to allow medical marijuana, that constitutes an accepted medical use.
An incisive article in JAMA Neurology, by the Harvard addiction scientist Bertha Madras, took a hard look at the process and found disturbing evidence of politicization. This included the fact that a high-ranking Biden DOJ official, Acting Assistant Attorney General Peter Hyun, argued that “cannabis has not been proven in scientific studies to be a safe and effective treatment for any disease or condition” — six months before the rescheduling directive appeared. Yet the science Hyun cites certainly had not changed in the interim.
The federal government has long held the position Hyun laid out. Under the Obama administration, Jay Inslee and Gina Raimondo — then the governors of Washington and Rhode Island, respectively — petitioned the federal government to reclassify marijuana. The administration’s response made clear that federal drug schedules reflect what the science says, not “danger” or “severity.” Obama’s then-DEA chief, Chuck Rosenberg, announcing the denial of the petition, used language Hyun would later echo: “This decision isn’t based on danger. This decision is based on whether marijuana, as determined by the FDA, is a safe and effective medicine . . . and it’s not.”
Suggested reading
I have seen the damage cannabis does
By Peter Hurst
But let’s assume, for the sake of argument, that Trump reverses years of federal precedent to follow the logic of the rescheduling argument. What happens then?
The truth: no one knows.
It’s clear that the marijuana industry believes that rescheduling will be an enormous benefit to its shareholders. In one sense, that’s likely correct. Businesses selling substances in Schedule I face severe commercial restrictions under the tax code. A provision of the tax code prevents any such business from taking normal deductions at tax time on expenses like advertising. Lifting those restrictions seems sure to provide an enormous boost to revenues and reach for businesses selling marijuana products.
The impact on society is a different matter. The available evidence suggests that this will be a significant negative for society, especially given the research around how the young start using the drug: data published in June by researchers from the University of Southern California and Rutgers University show that exposure to marijuana social-media content plays a huge role in teens initiating use.
But there are other externalities in play.
If marijuana moves into Schedule III, it will be the only substance there without Food and Drug Administration approval. Will that play out in a similar way to the case of opium-poppy straw (i.e., the entirety of the plant, as it exists prior to the processes that turn it into heroin or opium)? Poppy straw is listed in Schedule II, but it also lacks an FDA approval — and it’s regularly seized by drug and border authorities, with a massive shipment grabbed up just in May. Though weed entrepreneurs clearly expect smooth sailing after a reclassification, they may well be in for a rough ride.
Then there’s the fact that substances listed in Schedule III face additional regulatory and enforcement power: Not only from the DEA and DOJ, but also from the FDA. There are strict rules around what sellers of Schedule III substances can and can’t say in advertisements. They’re forbidden from advertising off-label uses — and since marijuana lacks an FDA approval, all therapeutic uses are off-label. It’s easy to imagine another operator in the Schedule III space filing a lawsuit demanding precisely that kind of enforcement.
In other words, rescheduling opens the door to regulatory chaos, even as it seems certain to add commercial firepower to an industry whose products, on the evidence, are extraordinarily harmful. How this combination will produce the benefits promised by proponents of rescheduling also remains unclear.
The federal government shouldn’t signal to the American people that a drug that lacks medical or scientific imprimatur somehow possesses such approval. Others disagree — and vocally. They have a lot of money riding on it. But we should be crystal clear about what their preferred policy would actually mean for American society — nothing good.
Kevin Sabet, a former three-time White House senior drug-policy adviser, is president of Smart Approaches to Marijuana.
Source: https://unherd.com/2025/08/the-illusion-of-safe-marijuana/?edition=us?
There is a growing body of research on the second-hand harms from alcohol and drug use that points to the negative health impacts of substance use extend beyond the individual engaged in the behavior. The literature on alcohol-related harms has explored the connections between secondhand alcohol and drug harms (ADH) and their impact on quality of life, well-being and mental health issues among those affected, often including family members, but there hasn’t been any specific research done on the family burden related to alcohol and other drug harms until now.
This study from PHI’s Alcohol Research Group and independent scientific research institute RTI International evaluates the familial burden of the secondhand ADHs, investigating associations between a seven-item summative burden scale and different types of harms attributed to someone else’s use of alcohol, cannabis or other drugs. The findings reveal the need for family support interventions and policy remedies to mitigate these burdens.
You can view the study here:

About RTI International
RTI International is an independent scientific research institute dedicated to improving the human condition. Our vision is to address the world’s most critical problems with technical and science-based solutions in pursuit of a better future. Clients rely on us to answer questions that demand an objective and multidisciplinary approach—one that integrates expertise across social, statistical, data, and laboratory sciences, engineering, and other technical disciplines to solve the world’s most challenging problems.
Originally published by International Journal of Alcohol and Drug Research
Notifications

Can New York clean up its public drug-use problem?
Mayor Eric Adams aims to try: On Thursday, he called on the state Legislature to allow clinicians and judges to compel people into treatment when their drug use is hurting them and the city.
“We must help those struggling finally get treatment, whether they recognize the need for it or not,” Adams said at an event hosted by the Manhattan Institute (where I work).
“Addiction doesn’t just harm individual users; it tears apart lives, families and entire communities, and we must change the system to keep all New Yorkers safer.”
Adams’ proposed state law, the Compassionate Interventions Act, may face an uphill battle in Albany, as “harm reduction” advocates assail it as coercive and dangerous.
But involuntary treatment should be a tool in New York’s arsenal for dealing with the public drug use that has plagued it for years.
Last year it reported nearly 4,000 homeless residents with a history of chronic substance use — probably an undercount, as such people are less likely to be identified by the city’s annual late-night census.
Regardless, it’s not hard to find people shooting up on New York’s streets — just visit the Hub in The Bronx or Washington Square Park in Manhattan.
Such behavior makes whole swaths of the city unlivable.
Public drug use hurts both users — there were more than 2,100 overdose deaths in the five boroughs last year — and the places where they use.
It deters commerce, and creates environments conducive to more serious crime.
Too often the city has responded to these situations with benign neglect, exemplified by its two “supervised consumption sites,” which give people a place to use with Narcan-wielding staff standing by.
These sites continue to operate, in spite of the fact that they don’t work and violate federal law.
Leaving people free to abuse drugs, it turns out, doesn’t save lives.
Involuntary treatment, by contrast, tries to correct the behavior that drives drug users to hurt both themselves and others.
That’s why 37 other states already permit it — and why New York under Adams’ plan would join them.
Critics will insist that involuntary drug treatment doesn’t work, and that people have to want to change.
But the balance of the evidence suggests that involuntary treatment performs as well as voluntary treatment.
That’s backed up both by older research on California’s involuntary-treatment scheme, and by strong indications that drug courts, which route drug offenders into treatment instead of prison, can reduce recidivism.
Opponents will also say that it’s immoral to compel people to get treatment they don’t want, and that it violates their “bodily autonomy.”
But there’s no right to shoot up in public spaces, or to ruin your body with fentanyl. And New Yorkers should have the right to expect their public spaces to be free from disorder, including public drug use.
The biggest challenge for Adams, though, may be the state’s limited treatment capacity.
New York state as a whole has only 134 long-term residential treatment facilities.
As of 2023, the most recent available data, they were serving 2,935 clients — fewer than the city’s tallied homeless drug-addict population.
Implementing the Compassionate Interventions Act will almost certainly require more funding for treatment beds, much as Adams’ previous efforts to institutionalize the seriously mentally ill did. That will have to be part of any ask in Albany.
But the mayor’s proposal will also allow diversion to outpatient treatment programs, including a new $27 million investment in contingency management therapy — an evidence-based intervention that has been shown to help treat drug addiction.
What happens if Albany says no to Adams’ proposal? Or if Adams is out of the mayoralty come the next legislative session?
The NYPD can still work to clear encampments. And the city can still try to divert drug users into its drug-courts system, which, while useful, faces administrative problems and lacks transparency.
But actually getting drug users the help they need, rather than just cycling them through the city’s jails, will be hard — much as the administration struggled to handle the seriously mentally ill before it had the power to compel them into treatment.
SOURCE: https://nypost.com/2025/08/14/opinion/involuntary-treatment-can-solve-the-public-drug-scourge/
Physical activity emerges as a powerful ally in exercise addiction recovery, offering hope and healing for those struggling with substance dependency. Recent groundbreaking research reveals how structured exercise programmes can reshape both body and mind, providing a natural pathway to wellness that supports long-term recovery goals.
The Science Behind Exercise Addiction Recovery
Two comprehensive studies from leading institutions demonstrate the remarkable impact of physical activity on individuals recovering from substance dependency. Research involving 90 participants in opioid substitution treatment and 43 individuals in drug rehabilitation centres reveals compelling evidence for physical activity recovery benefits.
Neurohormonal Changes Through Exercise
Exercise creates profound changes in the brain’s chemistry that directly counteract the damage caused by substance abuse. When individuals engage in regular moderate-intensity aerobic exercise, their bodies experience:
Increased β-endorphin production: These natural “feel-good” chemicals help restore the brain’s reward system, reducing cravings and improving mood without relying on substances.
Reduced cortisol levels: Exercise helps normalise stress hormone production, which is typically elevated during early recovery phases. This reduction helps manage anxiety, insomnia, and psychological distress.
Enhanced immune function: Regular exercise addiction recovery programmes boost white blood cell and neutrophil counts, strengthening the body’s natural defence systems weakened by substance abuse.
Physical Transformations Supporting Recovery
Body Composition Improvements
Research participants following structured exercise programmes showed remarkable physical changes after 24 weeks:
These improvements aren’t merely cosmetic—they represent fundamental changes that support sustained recovery by improving self-esteem and physical capability.
Fitness and Functional Capacity
Physical activity recovery programmes deliver measurable improvements across multiple fitness domains:
Cardiovascular health: Participants experienced substantial increases in vital capacity and overall cardiovascular function, supporting better oxygen delivery throughout the body.
Strength and endurance: Upper body and core muscle strength showed significant improvements, enabling individuals to engage more fully in daily activities and work responsibilities.
Flexibility and balance: Enhanced balance control and flexibility reduce injury risk whilst improving quality of life and confidence in physical activities.
Mental Health Benefits of Exercise Addiction Recovery
Anxiety and Depression Relief
The research demonstrates that structured exercise provides substantial mental health benefits:
The Mind-Body Connection
Exercise programmes that emphasise mind-body integration, such as Pilates, show particular promise. These activities combine physical movement with breath control and mental focus, helping individuals:
Types of Exercise for Addiction Recovery
Aerobic Exercise
Moderate-intensity aerobic exercise performed at approximately 70% of maximum heart rate proves most effective for exercise addiction recovery. Activities include:
The key lies in consistency—training three times per week for 20-minute sessions produces measurable neurohormonal improvements.
Mind-Body Practices
Research specifically highlights the benefits of Pilates training for individuals in recovery:
Creating Sustainable Exercise Addiction Recovery Programmes
Professional Supervision
Successful physical activity recovery requires proper oversight:
Long-Term Commitment
The research emphasises that benefits accumulate over time. Participants showed:
Integration with Comprehensive Care
Exercise works best as part of a holistic recovery approach that includes:
Practical Implementation Strategies
Starting an Exercise Programme
For individuals beginning their recovery journey, successful exercise addiction recovery programmes typically include:
Foundation Phase: Week 1-4:
Development Phase: Week 5-12
Maintenance Phase: Week 13-24
Monitoring Progress
Successful programmes track multiple indicators:
The Role of Exercise in Long-Term Recovery
Preventing Relapse
Physical activity recovery programmes address key relapse triggers:
Social Benefits
Group exercise activities offer additional advantages:
Building Support Networks
Family and Friends
Loved ones play crucial roles in supporting exercise addiction recovery:
Professional Support Teams
Effective programmes involve multidisciplinary teams:
Evidence-Based Outcomes
The research provides compelling evidence for physical activity recovery effectiveness:
These outcomes demonstrate that exercise isn’t merely an adjunct therapy—it’s a fundamental component of comprehensive recovery strategies.
Moving Forward with Exercise Addiction Recovery
The evidence overwhelmingly supports integrating structured exercise addiction recovery programmes into comprehensive treatment approaches. By addressing both physical and mental health simultaneously, exercise provides a natural, sustainable foundation for long-term recovery success.
For individuals and families affected by substance dependency, understanding the transformative power of physical activity offers hope and practical steps towards healing. The journey may be challenging, but with proper support, professional guidance, and commitment to consistent exercise, lasting recovery becomes not just possible but probable.
The path to recovery through exercise requires dedication, but the rewards—improved physical health, enhanced mental wellbeing, and sustained freedom from substance dependency—make every step worthwhile.
by Shalini Ramachandran and Betsy McKay – Wall Street Journal – July 31, 2025
Hundreds of thousands of veterans with PTSD have been prescribed simultaneous doses of powerful psychiatric drugs. The practice, known as “polypharmacy,” can tranquilize patients to the point of numbness, cause weight gain and increase suicidal thoughts when it involves pharmaceuticals that target the central nervous system, according to scientific studies and veterans’ accounts.
The VA’s own guidelines say no data support drug combinations to treat PTSD. The Food and Drug Administration warns that combining certain medications such as opioids and benzodiazepines can cause serious side effects, including death.
Nonetheless, prescribing cocktails of such drugs is one of the VA’s most common treatments for veterans with PTSD, and the number of veterans on multiple psychiatric drugs is a growing concern at the agency, according to interviews with more than 50 veterans, VA health practitioners, researchers and former officials, and a review of VA medical records and studies.
Polypharmacy has multiple definitions when it comes to central nervous system drugs. The VA defines it as taking five or more medications at the same time, while some medical researchers say it’s two or more and the American Geriatrics Society defines it as three or more.
There is an emerging medical consensus among VA doctors and researchers that taking multiple central nervous system drugs can wreak havoc on patients. Interactions between such drugs aren’t well understood, and their effects in combination can be unpredictable and extreme.
SOME CASE HISTORIES …
Mark Miller
U.S. Navy, Security Forces (1992-2007)
In 2007, Mark Miller was diagnosed with PTSD. The military put him on fluoxetine, otherwise known as Prozac. He became suicidal. Miller eventually weaned himself off medications and used “neuroplasticity” therapy which forms new connections in the brain. This April, returning suicidal thoughts prompted Miller to visit a VA hospital in San Antonio. A nurse practitioner prescribed a powerful antipsychotic in a five-minute appointment. Six days later, Miller returned, stepped off a shuttle bus and fatally shot himself in the head. “He did it clearly to speak for all the veterans who have no voice,” his father said.
‘They did not even listen to anything I said — just prescribed stuff. Unreal’— Text from Mark Miller to his father days before his suicide
The VA maintains that the best treatment for PTSD is talk therapy. But therapists are scarce and wait times are long, so overwhelmed doctors default to pills. Because there is no single drug designed specifically to treat PTSD, veterans often end up on drug cocktails as multiple specialists try to ease a variety of symptoms and prevent harm or suicide, according to VA clinical staff, studies and veterans.
“When it comes to the challenge of polypharmacy in these populations, it’s constantly chasing your tail,” said Dr. Ryan Vega, a chief healthcare innovation official at the VA until 2023, who still treats veterans. “It is where medicine is more art than science. We have medications that treat those symptoms but are we addressing the root cause?”
Nearly 60% of VA patients with PTSD were taking two or more central nervous system drugs at the same time in 2019, the latest year for which data are publicly available, according to a VA study. That works out to more than 520,000 patients, up 62% from a decade earlier, driven by a near doubling of the number of VA patients with PTSD due to more combat tours and better screening.
One silver lining highlighted by the study was that the percentage of PTSD veterans on five or more CNS medications declined to 7% from 12%, largely due to internal efforts to deprescribe opioids and benzodiazepines. (Central nervous system drugs affect the brain and spinal cord; psychiatric medications are a subset of CNS drugs). The VA declined requests from The Wall Street Journal to provide more recent polypharmacy numbers for veterans in its care.
The VA has long been aware of the risks of overprescribing, and has internal research since at least 2016 showing the potential harms, including increased risk of suicide. The internal polypharmacy data “was pretty concerning,” said Dr. Shereef Elnahal, who headed the VA health system until early this year. He recalled a veteran advocate who told him about three veterans on more than five psychiatric drugs each who died by suicide, one after the other. They had been “walking around like zombies” before they took their own lives, the advocate told him.
The VA’s use of psychiatric drugs has come under scrutiny from members of Congress and advocacy groups as the veteran suicide rate is roughly double that of U.S. adults who didn’t serve. Studies by VA researchers link the simultaneous use of multiple psychiatric drugs to suicide risk among veterans, including a 2016 paper that found Iraq and Afghanistan war veterans taking five or more central nervous system drugs faced higher risks of overdose and suicidal behaviors.
Lucas Hamrick
U.S. Army, Special Forces (1996-2019)
Lucas Hamrick was diagnosed with PTSD in the Army. There, and then at the VA, he was prescribed multiple central nervous system drugs. Some put him in a daze, others made him feel like he might want to kill himself. After losing 12 friends on similar drug combinations to suicide, Hamrick quit all the medications by 2023 and turned to meditation, mindfulness and breathing exercises. “It’s about structuring life around how not to let things spill over,” he said.
‘The quality of mental health care made me feel like I was there to check a box and complete the process instead of working toward any type of changes in perspective or disposition.’
Yet the agency has been slow to mandate changes. It has failed to implement nationwide electronic systems to alert doctors when they prescribe multiple psychiatric drugs, despite evidence from its own studies that these alerts improve care. The VA doesn’t uniformly require written informed consent for all psychiatric drugs with suicide risk, something that veterans groups and some members of Congress are urging. Some veterans who have resisted taking cocktails of drugs say they were warned by VA and military doctors that refusing them could jeopardize their eligibility for disability benefits, which can reach $4,500 a month.
“I’ve been mortified by practically every veteran I’ve seen having been prescribed multiple psychiatric medications, often without a timely referral to therapy or without any referral at all,” said Janie Gendron, a therapist who worked for the Defense Department and has seen hundreds of active-duty service members and veterans in the past 25 years.
A VA spokesman said the agency is looking into the issues raised by the Journal, and that the Trump administration is seeking to address serious problems it has identified in veterans’ healthcare that weren’t solved by the Biden administration.
VA Secretary Doug Collins said at a congressional hearing in May that the agency is pursuing the potential use of alternative therapies, such as psychedelics, to offer more options and reduce the risk of suicide among veterans.
The rise of the combat cocktail for PTSD has its roots in the overreliance on a single class of drugs: benzodiazepines. By the 1970s, the military and VA relied heavily on Valium and, later, Xanax as a primary treatment for traumatized service members and veterans returning from deployment. But in the 1990s, Defense Department researchers observed that high doses often yielded poor clinical outcomes, and, along with the VA, ultimately advised against their long-term use on veterans in 2004.
Still, against the guideline, the VA has doled out benzodiazepines to more than 1.7 million patients with PTSD diagnoses since 2005, its own data show. It took nearly a decade for the use of those drugs to start to decline.
At the same time, prescriptions to veterans with PTSD rose for other powerful psychiatric drugs.
VA doctors and patients say that existing tools to limit the number of psychiatric drugs a patient takes, and guidance to avoid the use of benzodiazepines and certain antipsychotics for veterans with PTSD, are frequently ignored.
A friend’s suicide
After his best friend’s suicide in 2013, Iraq war veteran Doug Gresenz was diagnosed with PTSD and borderline personality disorder and eventually put on six psychotropic drugs. After one medication’s dosage was increased, he attempted suicide and was hospitalized. When he protested the volume of medications there, he said VA doctors questioned his commitment to recovery and told him he needed the pills to lead a normal life. “I was guilt-tripped,” he said.
Doug Gresenz
U.S. Marine Corps, Assaultman (2006-2010)
‘I remember thinking: I’m literally poisoning myself.’
In 2016 alone, VA doctors prescribed him more than a dozen drugs, including antidepressants, antipsychotics, muscle relaxants and medications for nightmares, anxiety, pain and sleep, medical records show. Over little more than a decade, he received more than two dozen central nervous system medications. He recalled complaining to VA doctors that he was “so doped up” he would have accidents before getting to the bathroom.
“I remember thinking: I’m literally poisoning myself,” he said. In 2018, he quit benzodiazepines cold turkey and began to taper off the other drugs.
Within a couple of weeks, he collapsed, unable to use his legs. He developed a stutter and extreme light sensitivity. Violent spasms led to another fall, which caused complications that resulted in a severe foot injury and, eventually, an amputation last year.
The VA recommends any one of three antidepressants for PTSD—sertraline (Zoloft), paroxetine (Paxil) and venlafaxine (Effexor). But doctors are free to prescribe other additional drugs off-label—and many do.
“It’s super normal to see someone on five or six medications,” said Mary Neal Vieten, a retired Navy psychologist who has worked with thousands of members of the military and veterans. “That’s like an everyday thing.” Trauma has been medicalized, she said. “They’re acting as if the problem is in the person,” she said. Instead, it’s a normal response to an overwhelming experience, she said.
‘Stop-and-go’ pills
The culture of combat cocktails begins for some who are diagnosed with PTSD while still on active duty. In the military, too, drugs have long been given priority over psychotherapy, according to many veterans, former VA officials and therapists.
One Navy chaplain said his repeated calls to the Navy for more mental health resources went unanswered despite his documentation of more than 70 critical events, including suicide attempts, at a high-stress installation with nuclear submarines. When the chaplain himself grew suicidal, Navy doctors suggested that refusing the three-medication cocktail they prescribed could lead to discharge without benefits, instead of medical retirement with care.
Some veterans enter VA care dependent on psychiatric drugs that they were prescribed to improve combat readiness. They include Air Force veterans given “stop-and-go” pills—stimulants followed by sleeping pills.
Michael Valentino, who was chief pharmacist at the VA until 2021, said he grew alarmed by the rising numbers of service members entering VA care on stimulants without a diagnosis justifying it. “Then the VA has the burden of trying to undo it.”
Heather King
U.S. Air Force, Aircraft Maintenance Craftsman (2001-2010)
Heather King struggled with sleep after the Air Force prescribed Ambien following long flights. After her discharge, she was diagnosed with PTSD, and the VA added eight central nervous system drugs by 2020. King begged for help weaning off. Her VA doctor’s response: “Heather, under no circumstances are you ever going to be a person who is going to operate without meds.” She’s lately been sleeping soundly without pills for the first time, thanks to cognitive behavioral therapy for insomnia—something the VA only told her about recently.
‘It was like a death sentence. All these medications, they just made me numb. I wanted to feel my feelings, I wanted to actually heal.’
A Pentagon official said several medications at once are sometimes necessary for patients with multiple medical problems or who are treatment-resistant, adding that “records are reviewed to determine if the treating provider has provided clinical justification for the use of polypharmacy.” Service members and their families are offered “a robust and comprehensive array” of mental health programs, the official said.
Chemical messengers
Psychiatric drugs work by affecting levels of chemical messengers in the brain called neurotransmitters, which send signals between nerve cells and other cells in the body. For instance, many antidepressants increase levels of serotonin, a neurotransmitter associated with mood. Benzodiazepines enhance the activity of a neurotransmitter called GABA, while some antipsychotics block dopamine receptors. Layering on several of these central nervous system agents at once can magnify their effects.
Combining an antipsychotic drug that activates dopamine receptors with one that blocks dopamine can exacerbate psychosis, said Dr. Sanket Raut, a research fellow specializing in polypharmacy at Gallipoli Medical Research in Brisbane, Australia. By the same token, benzodiazepines and opioids taken together can increase the risk of overdose. “Polypharmacy is a big problem,” said Raut. “There are many side effects: cognitive impairment, dizziness and the risk of falls.”
Erika Downey
U.S. Army, Military Police (2007-2013)
Amphetamine-Dextroamphetamine
‘They give out these giant paper bags filled with medicine after your first psychiatrist appointment.’
“They give out these giant paper bags filled with medicine after your first psychiatrist appointment,” said Erika Downey, a 35-year-old retired Army sergeant with PTSD. Women are more likely to be prescribed multiple drugs concurrently against guidelines, VA researchers have found.
Downey’s bouts of suicidal ideation while taking antidepressants, benzodiazepines and stimulants were so bad she once called a friend to come take away her gun. After that, she decided talk therapy would be the best medicine. She weaned herself off the drugs on her own over two years. She had to wait three years for a VA psychotherapy appointment. “At the VA, you are more quick to get into a psychiatrist”—someone who can prescribe meds—“than a psychologist,” she said. Gray for WSJ
Only 15% of veterans diagnosed with depression, PTSD or anxiety are offered psychotherapy in lieu of medication, according to a 2019 report by the Government Accountability Office. “They’re really leveraging the prescribing to keep up with patient demand,” said Derek Blumke of the Grunt Style Foundation, a nonprofit veterans’ care group. Many VA providers’ impulse is to “get them in and get them out,” said Chris Figura, a patient advocate at a VA in St. Louis.
Navy veteran Dick Johnson, in the VA system for three decades and diagnosed with PTSD and bipolar disorder, was prescribed more than 25 different central nervous system drugs, including antipsychotics, antidepressants and epilepsy medications, sometimes on six concurrently, his medical records show. He blames them for the collapse of his two marriages. “They pretty much destroyed my life,” Johnson said. When he worsened on one antipsychotic and experienced intense withdrawal tapering off, VA doctors tried to patch him up with a cocktail of other medicines including benzodiazepines. In 2006, he started a prolonged dose of Seroquel, a powerful antipsychotic, to get off benzodiazepines, because doctors said it was supposed to be easier to stop. His weight soared and he developed diabetes. Quitting Seroquel “nearly killed” him, as he suffered intense vomiting, diarrhea and a near-inability to digest. He’s still tapering off Paxil and Tegretol today, using a jewelry scale and sandpaper.
Drugged for Decades
Dick Johnson, who joined the Navy in 1989, was diagnosed with bipolar disorder. After he was medically discharged in 1994, the VA put him on a heavy regimen of psychiatric drugs that made matters worse.
Dr. Saraswathy Battar, a VA geriatrician, launched a passion project in 2016 to decrease the use of potentially inappropriate medications. After noticing veterans suffering from debilitating symptoms that she attributed to overprescription, she developed an electronic tool that has helped providers discontinue more than three million prescriptions. About half of VA providers are using the optional tool, she said, but they’re mostly caring for older veterans or those in palliative care, while it’s been hard to get mental health providers to adopt the tool. Some said they were unaware of its existence. “Suicide and homicide get attention,” but “there’s no penalty for not prioritizing polypharmacy reduction,” she said.
A path forward
After years on psychiatric drug regimens prescribed by military and VA doctors, a growing number of veterans are taking healing into their own hands, often exploring unconventional treatments. Many veterans said they are frustrated and angry that the country spends heavily training them to be lethal, but there’s little support for their fragile mental health as they reintegrate back into society.
Scott Griffin, the former special operations soldier who contemplated suicide last year, reached out to a group called Veterans Exploring Treatment Solutions, or VETS, after the episode. Their suggestion: ibogaine, a powerful psychedelic derived from an African plant and illegal in the U.S., but only after tapering off his current medications. When Griffin asked his VA prescriber for help tapering, “he point-blank refused,” Griffin said.
He embarked on a gruelling self-taper. “I was white knuckling. I broke my teeth from clenching,” he recalled, battling intense vertigo and suicidality.
After 12 hours of altered consciousness on ibogaine in Mexico, Griffin took 5-MeO-DMT, a psychoactive compound most famously found in Colorado River toads’ poison, which he says was a profound spiritual experience. Since returning home in March, he has discarded his pills, prays daily and spends time with family, reconnecting after years of being “consumed by panic and anxiety.”
A Stanford study of 30 special operations forces veterans published last year found that ibogaine sharply reduced PTSD and related symptoms. A bipartisan bill in the House aims to fund VA research into psychedelics, which doctors caution remain largely unproven in clinical trials.
Says Griffin, “How does bark from a tree and venom off the back of a toad beat all this crap, all these pharmaceuticals they push down your throat?”
Source: Maggie Petito – www.drugwatch.org
OPENING REMARK BY NDPA:
Dianova presents itself as a “Swiss NGO recognized as a Public Utility organization, committed to social progress”. Examination of their publications places them as an organisation which is less committed to primary prevention than to reactive approaches, such as harm reduction. A telling quote in this context comes in their publication entitled “Between Music and Substances: a Look at Drug Use at Festivals” … they introduce this by saying “Drug use is a common occurrence at most music festivals: how can we promote self-care and harm reduction among participants?” – there is no mention of prevention as a policy option.
In their ‘history’ Dianova take a position found not infrequently in some other other critics of prevention i.e. any prevention program which does not achieve 100% success is deemed a failure … but no such assessment is made of reactive or accepting policies.
In this publication they dismiss the ‘Just Say No’ program as “…focusing mainly on white, middle-class children, it simply pointed the finger at others, particularly black communities, who were held responsible for the problem.” And yet immediately below this statement they include a photo of a White House ‘Just Say No’ rally, with Nancy Regan surrounded by black youngsters.
Dianova make judgemental remarks – without supporting evidence – in several places, and NDPA take would issue with several of these, but we have elected to retain this paper complete with their judgemental remarks, to illustrate their position on the ‘history’ as they see it.

From the early 20th century to the present day, an overview of the origins of drug use prevention, past mistakes and the current situation in this field
By the Dianova team – Over the past 40 years, prevention has become a key focus of public intervention in many areas, including responses to social issues such as alcohol and other drug use. Prevention strategies are now most often part of a comprehensive approach combining prevention, treatment and harm reduction, and taking into account the needs of people who use drugs and those of society as a whole.
These initiatives are developed on the basis of applied research in the humanities and social sciences, and their implementation and evaluation are based on scientifically validated strategies designed to answer one key question: do they work?

Understanding risk factors is crucial in modern drug prevention interventions, as it enables us to address the root causes of substance use and promote protective factors such as strong family bonds, engagement with school, and community support – Image by stokpic from pixabay, via Canva
Rather than raising awareness of the ‘dangers of drugs’, most initiatives today prefer to target risk factors and protective factors at the individual, family, community and environmental levels. These interventions are designed to be person-centred, while taking into account the many complex interactions between personal and environmental factors that may make certain populations more vulnerable to substance use or addiction. However, this has not always been the case. So what was prevention like before? Is prevention today so different from what it was in the past?
All forms of prevention stem from the 19th-century school of thought influenced by Pasteur’s work on the spread of disease: hygienism. This developed in a society plagued by diseases such as tuberculosis and cholera, which were widespread in most European countries, as well as in India, the United States and Canada.
With regard to substance use, it was alcohol that initially became the focus of efforts in Western countries. . In the countries concerned, the Industrial Revolution caused a profound change in drinking habits and exacerbated related problems. The advent of industrialization precipitated a period of exponential growth in the production, transportation and commercialization of alcohol. In urban areas, which experienced a significant increase in population following the rural exodus, millions of workers, reliant on their employers and lacking in social rights, found solace in alcohol, which had become readily available and inexpensive. Alcohol consumption increased significantly, as did the associated problems.
At the time, excessive drinkers were seen as a threat to their jobs, their families and society as a whole. In response, the temperance movement gained strength in America and Europe in an effort to combat alcoholism.
The temperance movement, a group of religious associations and leagues committed to combating the social ills of alcoholism, fought against the consumption of alcohol in the name of morality, good manners and the protection of the family unit. The influence of this movement grew until it reached its zenith in the early 20th century with the advent of alcohol prohibition laws, not only in the United States, but also in Canada, Finland and Russia – with the results we all know.

“The voluntary slave” – press illustration published in “La Fraternité” (France) for the Popular Anti-alcoholic league, author Adolphe Willette – circa 1875 – Adapted from screenshot from L’histoire par l’image
At the dawn of the 20th century, the concept of ‘illegal’ drugs had yet to be established. Europe and America had recently discovered a ‘remarkable substance’ – cocaine – lauded for its medicinal properties, touted as a panacea for all maladies. Initially imported in small quantities for medical research, its use grew rapidly, particularly within the medical community, and it was prescribed to treat a wide range of ailments, from toothache to morphine addiction. Sigmund Freud himself considered at the time cocaine to be a highly effective medicine for depression and stomach problems without causing addiction or side effects. With regard to cannabis and hashish, these were still available for purchase in all reputable pharmacies, while heroin, a registered trademark of the Bayer pharmaceutical company, was regarded as a sovereign remedy for… coughs.
It should be noted that the issue of substance addiction had not yet manifested itself in the context of affluent, colonizing nations. Elsewhere, the perspective was somewhat different: in a distant country – China – opium had already been wreaking havoc for several decades.
Introduced and marketed by Europeans, it had become a pervasive national scourge affecting millions of Chinese people. Opium addiction is a prime example of the impact of colonialism on local societies: not only did it trigger two wars against Western powers concerned solely with their economic interests (profits from the opium trade), but it also had profound social and political consequences that are still felt today.
The Western countries’ ‘honeymoon’ with drugs was not to last. The problems they posed became apparent rapidly and, under the influence of American temperance leagues, they swiftly transitioned from being regarded as a universal remedy to being perceived as a threat to society and moral values. This marked the beginning of American policies predicated on drug control (or the war on drugs, depending on one’s perspective), which would shape global policies in this domain for over a century.
The demonisation of drugs, the effects of which were felt from the beginning of the 20th century, is closely associated with a set of social, racial, political and economic dynamics that resulted in the stigmatization of both the substances themselves and the people who consumed them. As early as 1906, the United States initiated the legislative process, and the phenomenon grew until it culminated in a particularly restrictive and repressive international drug control policy – but that is another matter.

In the 1930s, the American government initiated a media offensive involving the use of racist stereotypes, sensationalist media, and political propaganda to portray cannabis as a dangerous substance that led to violence, insanity, and moral decay.
The process of demonizing drugs was gradual yet unstoppable. The discourse surrounding narcotics such as morphine, opium and heroin was initially shaped by their association with specific demographic groups, namely minorities, the economically disadvantaged, and migrants. This demonization continued over the following decades, fuelled by media sensationalism and public panic, particularly around the use of cocaine and cannabis – substances that were claimed to be the root cause of criminal behaviour and moral corruption.
The criminalization and stigmatization of substances and those who use them have had a profound impact. Not only have they perpetuated and reinforced racist prejudices against Afro-descendant, Latin American and other historically marginalized communities, but they have also completely distorted the approaches and prevention efforts implemented subsequently.
Before the 1960s, the ‘drug phenomenon’ was virtually non-existent in industrialised countries. Apart from a few opium enthusiasts, alcohol and tobacco reigned supreme in the field of substance addiction.
From the 1960s onwards, there was a rapid increase in the use of illegal drugs in the United States, particularly among the counterculture movement. The use of LSD and cannabis – and, to a lesser extent, amphetamines and heroin – spread and became a symbol of rebellion against authority, as part of a broader movement focused on social change.
Within the collective imagination, the 1960s are often regarded as the golden age of illegal drug use. This period was characterised by widespread use of cannabis, as well as the significant distribution of heroin among children in impoverished neighbourhoods. Notable figures such as Timothy Leary, a prominent Harvard professor, popularised the effects of LSD. However, an analysis of historical data reveals that the phenomenon was not as widespread as is commonly believed. Conversely, however, there was a marked increase in the perception of risk associated with drugs. For instance, in 1969, a mere 4% of American adults reported having used cannabis at least once. However, 48% of respondents indicated that drug use was a serious problem.

While many current prevention efforts have a solid theoretical basis and evidence of effectiveness, historic prevention strategies were often based on intuition and guesswork, with an emphasis on such scare tactics as the one depicted above (“Your brain on drugs” campaign, initially launched in 1987)
The notion of prevention as a concept was first developed in the early 1960s within the domain of mental health and behavioural disorders. In the context of drug policy, the first initiatives were echoing the pervasive fear of drugs that was prevalent in both America and Europe during that period. Logically, the primary initiatives were consistent with the propaganda campaigns initiated in previous decades with the objective of demonizing cannabis. The objective of these initial prevention initiatives was not to promote education, but rather to instil a sense of fear and intimidation.
‘People of my generation were taught that cannabis caused acne, blindness and sterility. It was a tactic based on fear, not on educating people.’
Children and young people in the 1960s and 1970s were no more stupid than anyone else and just as observant. They quickly realised that the messages promoted by schools and families did not correspond to reality.
In 1971, Richard Nixon declared drug abuse ‘public enemy number one’ and launched a widespread campaign against drug use, distribution and trafficking. This marked the beginning of a government policy that led to the incarceration of both traffickers and users. The policy would have far-reaching consequences for many countries, whilst in the United States it would have a disproportionately negative impact on the Black community.

The notion that one should ‘Just Say No’ to drugs is predicated on a rudimentary interpretation of the rational choice model, according to which people choose their behaviour in order to maximize rewards and minimize costs (negative consequences).

Nancy Reagan at a “Just Say No” rally at the White House in May 1986 – White House Photographic Collection, public domain
From 1983 onwards, this concept became central to the D.A.R.E. (Drug Abuse Resistance Education) programme. Initially implemented in Los Angeles, this school-based programme aimed to help young people understand that the harmful consequences of drug use far outweigh any perceived benefits. Young people can therefore avoid these consequences by refusing to take drugs.
The D.A.R.E programme’s model was based on three key elements: 1) drugs are bad; 2) when children understand how bad drugs are, they will avoid using them; and 3) the message is more effective when delivered by police officers, who are considered credible.
The programme was subsequently developed in the United Kingdom, and a similar model was adopted elsewhere in Europe during the same period — notably by associations of rehabilitated individuals — which replaced the credibility of police officers with that of former drug users ‘who could speak from experience’.

In response to findings on the ineffectiveness of the DARE programme, a new curriculum was developed (2009) with a stronger focus on interactive activities and decision-making skills, moving away from the traditional lecture-based approach by a police officer – AI-generated image, via Canva
Over the years, the programme has been the subject of extensive study. One study found that people who completed the programme had higher levels of drug use than those who did not. Another study found that teenagers enrolled in the D.A.R.E programme “were just as likely to use drugs as those who received no intervention”.
The aim here is not to portray the D.A.R.E. programme or similar interventions solely in an unfavourable or ridiculous light. Even though it has lost its central position, the programme is still implemented in most US states, and according to its website, it has been developed in 29 countries since its creation. It is true that the programme has since been adapted to incorporate various aspects, such as resistance to peer pressure and the development of social skills.
However, these initiatives face a major difficulty from the outset. As we know, experimentation and risk-taking are part of normal adolescent development, which is why providing young people with detailed information about different substances is likely to arouse their interest in these drugs, especially if the information is not presented in an appropriate manner. Secondly, this type of strategy only has an impact on young people who are susceptible to alarmist messages because of their cognitive patterns, and is not effective for everyone else, as we now know.

Officers in the DARE programme would sometimes arrive in sports cars seized from drug traffickers to exemplify their message on drugs and crime (Crime does not pay) – A Pontiac Firebird in D.A.R.E. livery in Evesham Township, New Jersey – image: – Flickr, licence: CC BY-SA 2.0
Furthermore, when talking about drugs, one must also consider the influence of popular culture, which, without openly glorifying substance use, often portrays alcohol, tobacco, and other drugs in a favourable light, particularly at an age when young people are most receptive.
We now know that providing information about drugs is not enough to make for a good prevention policy. While education and awareness can always play an important role, they are not sufficient, nor even necessary, to prevent addiction.
According to Dr Rebecca Haines-Saah, who spoke at a webinar organised by Dianova last May, the most effective drug prevention strategies do not focus on drugs, but on much broader social issues, such as reducing poverty, combating discrimination and implementing targeted community programmes.
Some prevention strategies even choose not to mention drugs at all, yet they have proven effective in reducing substance use by focusing on broader social, environmental and behavioural factors.
These approaches aim to create conditions that indirectly discourage drug use, particularly by strengthening social skills and improving people’s living conditions. For example, programmes focused on improving the school environment, teaching social skills or promoting healthy lifestyles can have a positive impact on reducing substance use without explicitly targeting drugs.
Similarly, family interventions that strengthen parent-child relationships and improve communication can also help prevent substance misuse by targeting underlying risk factors. These strategies highlight the importance of a holistic approach to prevention that goes far beyond direct drug education.
Preventing substance use – i.e. the use of all psychoactive substances regardless of their legal status – involves helping people, particularly young people, to avoid using substances. If they have already used substances, the objective is to prevent them from developing substance use disorders (problematic use or dependence).
However, the overall objective is much broader, as highlighted by the UNODC in the second edition of the International Standards on Drug Use Prevention. It also involves ensuring that children and adolescents grow up healthy and safe, so they can fulfil their potential and become active and productive members of society.

Drug prevention is now grounded in research and evidence-based practices. This multi-disciplinary field has developed over the last forty years, aiming to improve public health by identifying risk and protective factors, assessing the efficacy of preventive interventions, and identifying optimal means for dissemination and diffusion – AndreyPopov from Getty Images, via Canva
There is now a vast body of literature on substance use prevention. Its aim is to highlight effective and less effective strategies based on scientific evidence in order to guide decision-makers and practitioners in the field in their choices. Despite this, prevention activities are still sometimes poorly prepared and based primarily on beliefs or ideologies rather than scientific knowledge.
At Dianova, we believe that addiction prevention, particularly among young people, must take into account societal changes (new drugs, new patterns of use, changes in legislation, etc.) using scientifically validated strategies based on standards and methodological guidelines.
These strategies are based in particular on:
In conclusion, we must bear in mind the mistakes of the past so as not to repeat them and, above all, understand that no prevention system is sufficient on its own. Whatever approach is chosen, effective prevention systems must be evidence-based and integrated into broader, balanced systems that focus on health promotion, the treatment of substance use disorders, risk and harm reduction, and countering drug trafficking.
Effective, science-based programmes that can make a real difference to people’s lives can only be developed by integrating all these elements.
Source: https://www.dianova.org/publications/a-brief-history-of-drug-prevention/
OPENING REMARK BY NDPA.
This article involves several prestigious authors – not least Bertha K Madras. We therefore recommend readers to its contents, albeit they are lengthy and sometimes complex.
To access the full document:
We repeat this 2004 article by Stanton Peele as a useful position statement for us all. Peele’s classic 1975 text ‘Addiction and Love’ (Peele and Brosky – Published: Taplinger, New York) is also well worth reading in this context.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>

Change is natural. You no doubt act very differently in many areas of your life now compared with how you did when you were a teenager. Likewise, over time you will probably overcome or ameliorate certain behaviors: a short temper, crippling insecurity.
For some reason, we exempt addiction from our beliefs about change. In both popular and scientific models, addiction is seen as locking you into an inescapable pattern of behavior. Both folk wisdom, as represented by Alcoholics Anonymous, and modern neuroscience regard addiction as a virtually permanent brain disease. No matter how many years ago your uncle Joe had his last drink, he is still considered an alcoholic. The very word addict confers an identity that admits no other possibilities. It incorporates the assumption that you can’t, or won’t, change.
But this fatalistic thinking about addiction doesn’t jibe with the facts. More people overcome addictions than do not. And the vast majority do so without therapy. Quitting may take several tries, and people may not stop smoking, drinking or using drugs altogether. But eventually they succeed in shaking dependence.
Kicking these habits constitutes a dramatic change, but the change need not occur in a dramatic way. So when it comes to addiction treatment, the most effective approaches rely on the counterintuitive principle that less is often more. Successful treatment places the responsibility for change squarely on the individual and acknowledges that positive events in other realms may jump-start change.
Consider the experience of American soldiers returning from the war in Vietnam, where heroin use and addiction was widespread. In 90 percent of cases, when GIs left the pressure cooker of the battle zone, they also shed their addictions—in vivo proof that drug addiction can be just a matter of where in life you are.
Of course, it took more than a plane trip back from Asia for these men to overcome drug addiction. Most soldiers experienced dramatically altered lives when they returned. They left the anxiety, fear and boredom of the war arena and settled back into their home environments. They returned to their families, formed new relationships, developed work skills.
Smoking is at the top of the charts in terms of difficulty of quitting. But the majority of ex-smokers quit without any aid––neither nicotine patches nor gum, Smokenders groups nor hypnotism. (Don’t take my word for it; at your next social gathering, ask how many people have quit smoking on their own.) In fact, as many cigarette smokers quit on their own, an even higher percentage of heroin and cocaine addicts and alcoholics quit without treatment. It is simply more difficult to keep these habits going through adulthood. It’s hard to go to Disney World with your family while you are shooting heroin. Addicts who quit on their own typically report that they did so in order to achieve normalcy.
Every year, the National Survey on Drug Use and Health interviews Americans about their drug and alcohol habits. Ages 18 to 25 constitute the peak period of drug and alcohol use. In 2002, the latest year for which data are available, 22 percent of Americans between ages 18 and 25 were abusing or were dependent on a substance, versus only 3 percent of those aged 55 to 59. These data show that most people overcome their substance abuse, even though most of them do not enter treatment.
How do we know that the majority aren’t seeking treatment? In 1992, the National Institute on Alcohol Abuse and Alcoholism conducted one of the largest surveys of substance use ever, sending Census Bureau workers to interview more than 42,000 Americans about their lifetime drug and alcohol use. Of the 4,500-plus respondents who had ever been dependent on alcohol, only 27 percent had gone to treatment of any kind, including Alcoholics Anonymous. In this group, one-third were still abusing alcohol.
Of those who never had any treatment, only about one-quarter were currently diagnosable as alcohol abusers. This study, known as the National Longitudinal Alcohol Epidemiologic Survey, indicates first that treatment is not a cure-all, and second that it is not necessary. The vast majority of Americans who were alcohol dependent, about three-quarters, never underwent treatment. And fewer of them were abusing alcohol than were those who were treated.
This is not to say that treatment can’t be useful. But the most successful treatments are nonconfrontational approaches that allow self-propelled change. Psychologists at the University of New Mexico led by William Miller tabulated every controlled study of alcoholism treatment they could find. They concluded that the leading therapy was barely a therapy at all but a quick encounter between patient and health-care worker in an ordinary medical setting. The intervention is sometimes as brief as a doctor looking at the results of liver-function tests and telling a patient to cut down on his drinking. Many patients then decide to cut back—and do!
As brief interventions have evolved, they have become more structured. A physician may simply review the amount the patient drinks, or use a checklist to evaluate the extent of a drinking problem. The doctor then typically recommends and seeks agreement from the patient on a goal (usually reduced drinking rather than complete abstinence). More severe alcoholics would typically be referred out for specialized treatment. A range of options is discussed (such as attending AA, engaging in activities incompatible with drinking or using a self-help manual). A spouse or family member might be involved in the planning. The patient is then scheduled for a future visit, where progress can be checked. A case monitor might call every few weeks to see whether the person has any questions or problems.
The second most effective approach is motivational enhancement, also called motivational interviewing. This technique throws the decision to quit or reduce drinking—and to find the best methods for doing so—back on the individual. In this case, the therapist asks targeted questions that prompt the individual to reflect on his drinking in terms of his own values and goals. When patients resist, the therapist does not argue with the individual but explores the person’s ambivalence about change so as to allow him or her to draw his own conclusions: “You say that you like to be in control of your behavior, yet you feel when you drink you are often not in charge. Could you just clarify that for me?”
Miller’s team found that the list of most effective treatments for alcoholism included a few more surprises. Self-help manuals were highly successful. So was the community-reinforcement approach, which addresses the person’s capacity to deal with life, notably marital relationships, work issues (such as simply getting a job), leisure planning and social-group formation (a buddy might be provided, as in AA, as a resource to encourage sobriety). The focus is on developing life skills, such as resisting pressures to drink, coping with stress (at work and in relationships) and building communication skills.
These findings square with what we know about change in other areas of life: People change when they want it badly enough and when they feel strong enough to face the challenge, not when they’re humiliated or coerced. An approach that empowers and offers positive reinforcement is preferable to one that strips the individual of agency. These techniques are most likely to elicit real changes, however short of perfect and hard-won they may be.
Source: https://www.psychologytoday.com/gb/articles/200405/the-surprising-truth-about-addiction
Cannabis dependence affects millions globally, with over 23 million people worldwide struggling with problematic use patterns. As treatment demand continues rising, understanding which psychological interventions for cannabis dependence work best has become increasingly important. This comprehensive guide examines the latest evidence on therapeutic approaches that help individuals overcome cannabis-related difficulties.
Understanding Cannabis Dependence and Treatment Needs
Cannabis use becomes problematic when it significantly interferes with daily life, relationships, and responsibilities. The World Health Organisation recognises that whilst brief interventions may help casual users, those with established dependence require specialised psychological treatments for cannabis problems.
Recent statistics reveal the growing need for effective interventions:
Evidence-Based Psychological Interventions for Cannabis Users
A major systematic review from the University of Bristol analysed 22 clinical trials involving over 3,300 participants, providing crucial insights into which therapeutic approaches demonstrate real effectiveness.
Cognitive-Behavioural Therapy with Motivational Enhancement
The most extensively researched approach combines cognitive restructuring with motivation-building techniques. This integrated therapy helps individuals:
Research demonstrates this approach can increase abstinence rates nearly threefold compared to no intervention, establishing it as a cornerstone of evidence-based care.
Third-Wave Therapies: DBT and ACT Approaches
Newer psychological interventions for cannabis problems incorporate mindfulness and acceptance-based strategies. These therapies teach:
Studies show these approaches can quadruple abstinence rates when compared to basic psychoeducation alone.
Community Reinforcement Strategies
This approach restructures the individual’s environment to support recovery through:
Effectiveness of Psychological Treatments for Cannabis Dependence
The research reveals important findings about treatment outcomes:
Abstinence Achievement
Structured psychological interventions significantly improve abstinence rates. Individuals receiving cognitive-behavioural therapy are 18 times more likely to achieve abstinence compared to those awaiting treatment.
Reducing Use Frequency
For individuals not ready for complete abstinence, certain therapies effectively reduce consumption patterns. Acceptance-based approaches can decrease usage frequency by approximately 60%.
Treatment Duration and Structure
Effective programmes typically include:
Key Components of Successful Psychological Interventions for Cannabis
Research identifies several critical elements that enhance treatment effectiveness:
Skills Training
Teaching practical techniques for managing triggers, cravings, and high-risk situations proves essential for lasting change.
Motivational Enhancement
Building intrinsic motivation through personalised feedback and collaborative goal-setting improves engagement and outcomes.
Relapse Prevention
Comprehensive planning for potential setbacks helps maintain gains achieved during active treatment.
Environmental Modification
Addressing social and environmental factors that maintain problematic use patterns enhances long-term success.
Challenges in Delivering Effective Treatment
Despite proven effectiveness, several challenges affect treatment delivery:
Engagement and Retention
Maintaining participant engagement throughout treatment remains challenging, with completion rates varying significantly across different approaches.
Individual Differences
Treatment response varies based on:
Access to Services: Many individuals face barriers accessing evidence-based psychological treatments for cannabis problems, including geographical limitations and resource constraints.
Future Directions for Cannabis Treatment Research
As cannabis potency increases and use patterns evolve, treatment approaches must adapt accordingly. Priority areas include:
Implications for Treatment Seekers
For individuals considering treatment, research suggests:
The growing evidence base confirms that specialised psychological interventions for cannabis dependence can produce meaningful, lasting change when properly implemented and tailored to individual needs.
Conclusion: Current research provides strong support for several psychological approaches in treating cannabis dependence. Whilst cognitive-behavioural therapy with motivational enhancement shows the most consistent evidence, acceptance-based therapies and community reinforcement approaches also demonstrate effectiveness. As our understanding grows, these evidence-based treatments offer real pathways to recovery for those struggling with cannabis-related problems.
Source: https://nobrainer.org.au/index.php/resources/i-need-to-stop-this-help/1471-psychological-interventions-for-cannabis-dependence-latest-research-on-effective-therapies?
New allegations have emerged about China’s role in the global fentanyl supply chain, highlighting the complex nature of international drug trafficking and the urgent need for comprehensive prevention strategies.
What We Know About Project Zero
According to Yuan Hongbing, a former Chinese academic now living in Australia, sources within Beijing’s political circles have described a coordinated effort called “Project Zero.” This alleged initiative represents one aspect of the broader China fentanyl crisis that has contributed to America’s ongoing opioid epidemic.
Yuan’s claims suggest that some Chinese officials view the current drug crisis through the lens of historical grievances, particularly the 19th-century Opium Wars. Whether accurate or not, these allegations underscore the complexity of the Chinese fentanyl trade and its impact on communities worldwide.
The Evolution of Supply Routes
The China fentanyl crisis has evolved significantly since 2019, when Beijing officially banned fentanyl production under international pressure. Rather than ending the problem, this led to a shift in tactics within the Chinese fentanyl trade.
Companies began focusing on precursor chemicals instead of finished products. These substances travel from manufacturing facilities to Mexico, where they’re processed into fentanyl before reaching American markets. This indirect approach complicates efforts to address the China fentanyl crisis at its source.
Impact on Communities
The human cost of the ongoing crisis is staggering. More than 107,000 Americans died from drug overdoses in 2023, with synthetic opioids like fentanyl being the primary cause. These deaths represent families torn apart and communities struggling with the consequences of widespread addiction.
The China fentanyl crisis affects people from all backgrounds. Parents lose children, children lose parents, and entire neighbourhoods face increased crime and social instability. Understanding these impacts is crucial for developing effective Chinese fentanyl trade prevention strategies.
Government Responses and Investigations
Congressional investigations have revealed concerning patterns in how some aspects of the Chinese fentanyl trade operate. The House Select Committee found evidence that certain companies receive government benefits for exporting precursor chemicals, raising questions about official oversight.
These findings suggest that addressing the China fentanyl crisis requires diplomatic engagement alongside enforcement measures. The complexity of international trade makes it challenging to distinguish between legitimate chemical exports and those intended for illicit use.
Economic Measures and Trade Relations
The current trade tensions between the US and China reflect broader concerns about the Chinese fentanyl trade. Recent tariffs include specific measures targeting fentanyl-related commerce, with most Chinese goods facing increased duties.
These economic responses acknowledge that the China fentanyl crisis extends beyond traditional criminal justice approaches. However, trade measures alone cannot solve the underlying issues that drive demand for these substances in affected communities.
International Cooperation Challenges
Addressing the Chinese fentanyl trade requires unprecedented international cooperation. Different legal systems, varying enforcement capabilities, and complex diplomatic relationships all complicate efforts to tackle the China fentanyl crisis effectively.
Success depends on finding common ground between nations with different perspectives on regulation, enforcement, and prevention. This includes sharing intelligence, coordinating investigations, and developing consistent approaches to precursor chemical controls.
The Role of Prevention
Prevention remains the most effective long-term response to the China fentanyl crisis. Community-based programmes that educate young people about the dangers of substance use can reduce demand for these deadly drugs.
Effective prevention strategies address the root causes that make individuals vulnerable to addiction. This includes mental health support, educational opportunities, and strong community connections that provide alternatives to substance use.
When communities invest in prevention, they create protective factors that help people resist the appeal of drugs, regardless of their source. The Chinese fentanyl trade thrives where demand exists, making prevention efforts crucial for breaking this cycle.
Treatment and Recovery
For those already affected by the China fentanyl crisis, accessible treatment services provide hope for recovery. Evidence-based approaches that combine medical treatment with psychological support offer the best outcomes for people struggling with addiction.
Recovery programmes that involve families and communities tend to be more successful than those focusing solely on individual treatment. This holistic approach recognises that addiction affects entire social networks, not just individual users.
The Path to Prevention and Recovery
The allegations about Chinese involvement in fentanyl trafficking highlight the need for sustained international cooperation on drug prevention. Whether through diplomatic channels, trade measures, or community-based initiatives, addressing this crisis requires coordinated action.
Prevention must remain at the centre of any effective response to the China fentanyl crisis. By reducing demand through education and community support, we can address the root causes that make these supply chains profitable in the first place.
The Chinese fentanyl trade represents a complex challenge that requires nuanced solutions. Success will depend on combining international cooperation with strong local prevention efforts that protect vulnerable individuals and strengthen community resilience.
Only through sustained commitment to prevention, treatment, and community support can we hope to reduce the devastating impact of the China fentanyl crisis on families and communities worldwide.
Source: https://nobrainer.org.au/index.php/resources/wheelbarrows/1469-china-fentanyl-crisis-a-global-challenge-requiring-prevention?
Email From: Drug Free America Foundation – 11 July 2025
|
by Journal of Substance Use & Addiction Treatment, 2025,
Authors: Josh Aleksanyan, Zobaida Maria, Diego Renteria, Adetayo Fawole, Ashly E. Jordan, Vanessa Drury, … Charles J. Neighbors
Abstract:
Introduction: Transition-age (TA) adults, aged 18-25, have the highest prevalence of substance use disorder (SUD) among all age groups yet they are less likely to seek treatment and more likely to discontinue it than older adults, making them a high-priority treatment population. While structural barriers and varying expectations of recovery may affect treatment initiation, insights from providers working with TA adults can reveal what further impels and impedes treatment engagement.
Methods: We conducted two focus groups with 14 front-line treatment providers, representing urban and rural outpatient, residential, and inpatient SUD care settings across New York State. Providers were selected through stratified sampling using restricted-access treatment registry data. A semi-structured interview guide facilitated discussions, and transcripts were analyzed to identify key themes.
Results: Providers report that TA adults prefer briefer, innovative treatment approaches over traditional modalities like A.A./12-step recovery, driven by a desire to rebuild their lives through education and career. Post-pandemic social disruptions were cited as exacerbating engagement challenges and increasing the need for integrating mental health support. Providers highlighted the potential of technology to enhance treatment engagement, though expressed concerns regarding social isolation and the fraying of childhood safety nets and support systems (e.g., housing) undermining successful treatment outcomes and transitions to adulthood more broadly.
Conclusions: Providers report and perceive various challenges-unmet mental health needs, social alienation, and housing insecurity-that impede TA adults from successful SUD treatment. Understanding providers’ perceptions of the needs of young adults can inform patient and clinical decision-making, lead to the development of innovative treatment approaches tailored to TA adults and contribute to improved health outcomes over the life course.
To read the full text of this article, please visit the link below:
Source: https://drugfree.org/drug-and-alcohol-news/research-news-roundup-july-17-2025/
|
On April 22, the Department of Justice (DOJ) announced the termination of 365 awards that “no longer effectuate Department priorities.” Among these cuts were $88 million in Office of Justice Programs (OJP) funded programs administering substance use and mental health services. During Preisdent Trump’s first term, we witnessed a shift away from behavioral health models toward scare tactics and increased law enforcement activities — strategies known to be ineffective at preventing substance use. This term appears to be following that same trajectory.
America has a long history of reactively and emotionally addressing substance use in ways inconsistent with research and best practices. Large swings in political views and funding are not new and have detrimental effects on prevention efforts and communities. This latest rollback represents a reversion back to failed, punitive models, which threatens to unravel decades of progress in promoting community health and wellness.
Today’s substance use prevention activities are not the mass media scare campaigns seen during the 1960s to the 1990s or as simple as “Just Say No.” Substance use prevention takes a public health approach to promoting wellness and preventing substance use problems.
Unlike early iterations of “prevention,” the ultimate goal of prevention activities today is to promote wellness. Promoting wellness is not the same as advocating for the absence of a disease or illness but the presence of purpose in life, involvement in satisfying work and play, having joyful relationships, a healthy body and living environment, as well as general happiness. The Substance Abuse and Mental Health Services Administration (SAMHSA), drawing on Swarbrick’s wellness approach, describes wellness as having eight different dimensions – emotional, spiritual, intellectual, physical, environmental, financial, occupational, and social.
Effective prevention programs work across these dimensions to reduce factors that put people at risk of developing behavioral health disorders (i.e., risk factors) as well as promote or strengthen factors that protect people from these disorders (i.e., protective factors).
The way we have responded to substance use has always been reactionary and punitive. Responses to substance use in the U.S. has stretched back over a century and followed a repeating cycle of panic, punishment, and progress. A new drug “hits the streets,” a news article highlights the death of a young, innocent victim, or a new political ringleader will enter the scene spouting “tough on crime” rhetoric that causes a moral panic among the masses and calls for increased punishment. Those sentiments take hold for several years and lead to prison overcrowding and an increase in arrest rates. Eventually, scientific advancements push responses to substance use back into the behavioral health realm. Then, a political campaign or story regresses the U.S. back to failed models of addressing substance use with punishment and the cycle repeats.
The 1950s/1960s are generally seen as the beginning of the modern era of prevention — an era dominated by fear-based approaches. School talks aimed at “scaring kids straight” and media campaigns and movies painted exaggerated horror stories about drug use. But scare-based tactics never work, particularly when youth can see that the lessons don’t reflect their lived experience. By the 1970s, the “War on Drugs” had been launched, and President Nixon had called drugs America’s “public enemy number one” and ushered in a wave of punishment over support. One of the most popular mantras of prevention originated in the 1980s with Nancy Reagan’s famous phrase: ‘Just Say No.’ It was catchy, simple, and widespread, but ultimately ineffective.
In the 1990s, science began to shape prevention and we saw large drops in youth substance use rates ever since. Researchers began to examine risk and protective factors associated with substance use. These studies led to a more structured approach to prevention. New, evidence-based school curricula focused on building life skills, resilience, and relationships were implemented. Community coalitions like the Communities That Care model gained traction. This progress continued in the early 2000s, when prevention finally got a seat at the table in public health. Prevention efforts became evidence-based and multi-layered. Programs began to see substance use as due to a complex interaction between systems and started addressing the risk at the family-, peer-, school-, and individual-level, such as the Seattle Social Development Project.
But this progress is often undermined by political agendas.
The punitive spirit of the War on Drugs remains deeply embedded in U.S. policy. The first Trump administration marked a clear pivot away from behavioral health and back toward criminal justice responses. Law enforcement became the answer while programs focused on research and wellness were deprioritized. Youth substance use trends began to stabilize despite the steady decline they had been on since the 1980s, marking an early sign that prevention was losing its momentum. The Biden-Harris administration brought in a new wave of the War on Drugs by naming a specific adulterated substance, fentanyl combined with xylazine, as an “emerging threat to the United States,” a term traditionally held for matters of homeland security.
This new Trump administration brings new challenges and likely worse consequences as we witness an unprecedented time of widespread cuts to federal funding. Many communities rely heavily on these programs to help their fellow residents promote wellness in their area. Without these programs, improvements in trends in substance use will likely plateau, then potentially worsen. The challenge is that the consequences of cutting prevention are long-term, not immediate. As a result, many will turn to this time period in the next year to point out that there was no visible crisis or dramatic increase in substance use but that is based on a deep misunderstanding in evaluation research. The kids that would have relied on these programs will reach adulthood in the next few years which will be when we see the effects of not having these programs. People who relied on federally funded programs for treatment and support will experience worsening symptoms and rates of fatal overdoses will rise. Our schools will likely witness lower rates of attendance and a higher number of students dropping out or failing. Issues of overcrowding in jails and prisons will continue to worsen as increases in law enforcement activity will lead to greater arrests.
The defunding of mental health and substance use programming is a mistake. When prevention works, it’s invisible — no one sees the overdoses that didn’t happen, hears the fights that were avoided, or reads headlines about the crisis that never occurred. The invisibility of its effects does not mean it is not important.
We are at risk of repeating history by cutting prevention and returning to failed punitive models. Communities must lead where the federal government is failing. The momentum for prevention has always lain in the power of the community. The earliest substance use prevention movements started with everyday people who cared. Mothers Against Drunk Drivers (MADD) and other grassroots organizations started taking an active role in prevention in the 1980s, and ever since we have seen more communities taking the reins when it comes to promoting wellness in their area. Prevention is not an activity reserved solely for those in power; it is the duty and responsibility of every individual. Prevention is more than a policy or program; it is a promise to keep showing up for each other. If you are not sure where to start, start by telling your story and making space for others to lead. Prevention is strongest when it is shared.
Source: https://www.psychologytoday.com/us/blog/the-nature-of-substance-use/202505/defunding-prevention-a-setback-for-science-and-public
![]()
by Robyn Oster – Associate Director, Health Law and Policy – July 2025
Reminder: The U.S. Preventive Services Task Force (USPSTF), an expert panel, evaluates preventive services and recommends which should be provided at no cost.
The details:
The bigger context:
Source: https://drugfree.org/drug-and-alcohol-news/supreme-court-upholds-aca-preventive-care/
In Christian Daily – Forum 2025 – News & Stories – July 9, 2025
According to a report in ChristianDaily.com, a June 2025 study published in a peer-reviewed journal of the British Medical Association, found that daily cannabis users are 34% more likely to develop heart failure than non-users.
The study by researchers from France drew on data from over 150,000 U.S. adults tracked over several years, and also linked marijuana use with an increased risk of heart attack and stroke. The objective was to evaluate the possible association between major adverse cardiovascular events (MACE) and the use of cannabis or cannabinoids.
Dr. Matthew Springer, a heart disease biologist at the University of California, San Francisco (UCSF), told the New York Times that marijuana inhalation delivers “thousands of chemicals deep into the lungs,” potentially increasing cardiovascular risk. His lab recently found that both edible and inhaled forms of marijuana were associated with comparable levels of blood vessel dysfunction.
An accompanying editorial by researchers from California USA said about the study:
Legalisation of medical and recreational cannabis commerce is spreading around the world, associated with increased use1 and falling perception of the risk. Frequent cannabis use has increased in several countries, and many users believe that it is a safe and natural way to relieve pain or stress. In contrast, a growing body of evidence links cannabis use to significant harms throughout life, including cardiovascular health of adults. The robust meta-analysis of cannabis use and cardiovascular disease by Storck et al4 in this issue of Heart raises serious questions about the assumption that cannabis imposes little cardiovascular risk.
This study is backed up by a March 2025 publication by the American College of Cardiology which revealed that cannabis users under the age of 50 are six times more likely to suffer a heart attack and three times more likely to die from cardiovascular causes compared to non-users.
According to a review article in JACC: Journal of the American College of Cardiology – “Marijuana is becoming increasingly potent, and smoking marijuana carries many of the same cardiovascular health hazards as smoking tobacco.”
As reported by Christian Daily International, in 2019, the Christian Medical & Dental Associations (CMDA) — a U.S.-based nonprofit representing thousands of Christian healthcare professionals — issued a position statement cautioning against recreational and medicinal marijuana use. “[T]here is a need for limiting access to marijuana,” the CMDA said. It warned of addiction, cognitive impairment, psychosis, and long-term health effects, especially among youth. “The adolescent brain is still developing and more vulnerable to the adverse effects of marijuana,” the statement emphasised.
Source: https://www.christiandaily.com/news/new-study-links-marijuana-to-heart-failure-echoing-christian-medical-professionals-long-standing-warnings-against-recrea
Two large-scale surveys of California high school students found that teens who saw cannabis and e-cigarette content were more likely to start using those substances or to have used them in the past month
Teens who see social media posts showing cannabis or e-cigarettes, including from friends and influencers, are more likely to later start using those substances or to report using them in the past month, according to surveys done by researchers at the Keck School of Medicine of USC. Viewing such posts was linked to cannabis use, as well as dual use of cannabis and e-cigarettes (vapes). Dual use refers to youth who have used both cannabis and e-cigarettes at some point. The results were just published in JAMA Network Open.
The findings come amid a decline in youth e-cigarette use, reported in 2024 by the U.S. Food and Drug Administration (FDA) and U.S. Centers for Disease Control and Prevention. However, teen vaping, cannabis use and the dual use of e-cigarettes and cannabis remain a problem.
“While the rate of e-cigarette use is declining, our study shows that exposure to e-cigarette content on social media still contributes to the risk of using e-cigarettes with other substances, like cannabis,” said Julia Vassey, PhD, a health behavior researcher in the Department of Population and Public Health Sciences at the Keck School of Medicine.
The study, funded by the National Institutes of Health, also helps clarify how certain types of social media posts relate to teen substance use. Researchers surveyed more than 7,600 teens across two studies: a longitudinal study to understand whether viewing cannabis or e-cigarette posts on TikTok, Instagram and YouTube relates to a teen’s later choice to start using either substance or both, and a second survey looking at whether an association exists between the source of the content— friends, influencers, celebrities or brands—and substance use.
“Answering these questions can help federal regulators and social media platforms create guidelines geared toward preventing youth substance use,” Vassey said.
Data for the study came from California high school students, with an average age of 17, who completed questionnaires on classroom computers between 2021 and 2023. Researchers conducted two surveys, one focused on teens who used cannabis, e-cigarettes or both for the first time, the other focused on use during the past month.
In the first survey, which included 4,232 students, 22.9% reported frequently seeing e-cigarette posts on TikTok, Instagram or YouTube, meaning they saw at least one post per week. A smaller portion—12%—frequently saw cannabis posts.
One year later, researchers followed up with the students. Teens who had frequently seen cannabis posts—but had never tried cannabis or e-cigarettes—were more likely to have started using e-cigarettes, cannabis or both. Teens who had frequently seen e-cigarette posts on TikTok were more likely to have started using cannabis or started dual use of both cannabis and e-cigarettes. No such pattern was found for Instagram or YouTube. The data collected allowed researchers to look at platform-specific results for e-cigarettes posts, but not for cannabis posts.
“This is consistent with previous research showing that, of the three platforms, TikTok is probably the strongest risk factor for substance use,” Vassey said. That may be because TikTok’s algorithm pushes popular content broadly, including posts that feature e-cigarettes, even to users who don’t follow the accounts.
In the second survey, researchers asked 3,380 students whether they saw cannabis or e-cigarette posts from brands, friends, celebrities, or influencers with 10,000 to 100,000 followers. Teens who saw e-cigarette or cannabis posts from influencers were more likely than their peers to have used cannabis in the past month. Those who saw e-cigarette posts from friends were more likely to have been dual users of cannabis and e-cigarettes in the past month. Those who saw cannabis posts from friends were more likely to have used cannabis in the past month or to have been dual users of cannabis and e-cigarettes.
The link between e-cigarette posts and cannabis use is what researchers call a “cross-substance association” and may be explained by the similar appearance of nicotine and cannabis vaping devices, Vassey said.
Influencer posts deserve special attention because they often slip through loopholes in federal rules and platform guidelines. For example, the FDA can only regulate content when brand partnerships are disclosed, but influencers—consciously or not—may skip disclosures in some posts.
Studies show that these seemingly unsponsored posts are seen as more authentic, Vassey said, making them particularly influential.
Most social media platforms already ban paid promotion of cannabis and tobacco products, including e-cigarettes. Some researchers say those bans should be extended to cover additional influencer content. Others want platforms to partner with regulators to find a comprehensive solution.
“So far, it’s a grey area, and nobody has provided a clear answer on how we should act and when,” Vassey said.
In future studies, Vassey plans to further explore cannabis influencer marketing, including whether changes to social media guidelines impact what teens see and how they respond.
In addition to Vassey, the study’s other authors are Junhan Cho, Trisha Iyer and Jennifer B. Unger from the Department of Population and Public Health Sciences, Keck School of Medicine of USC, University of Southern California; Erin A. Vogel from the TSET Health Promotion Research Center, University of Oklahoma Health Sciences Center, Oklahoma City; and Julia Chen-Sankey from the Institute for Nicotine and Tobacco Studies and the School of Public Health, Rutgers University, New Brunswick, New Jersey.
This work was supported by National Institutes of Health [R01CA260459]and the National Institute on Drug Abuse [K01DA055073].
Source: https://keck.usc.edu/news/e-cigarette-and-cannabis-social-media-posts-pose-risks-for-teens-study-finds/
itvx news – Tuesday 24 June 2025

Cannabis activists and entrepreneurs, hold cannabis plant as they march to Government House in Bangkok, Thailand in 2024.Credit: AP
Thailand is moving to pass new legislation banning cannabis for recreational use in a major reversal, three years after the country became the first in Asia to decriminalise the drug, local media reports.
On Tuesday, Public Health Minister Somsak Thepsuthin said he had signed an announcement limiting cannabis to medical use only, Bangkok news site Khaosod confirmed.
Under the changes, people wishing to purchase cannabis must have a doctor’s prescription and a medical certificate indicating their illness.
Operators selling the drug will need to have a doctor present at the shop to renew or apply for a license to sell.
Somsak also said that in the future, cannabis will return to being considered a narcotic.
It is not clear when the regulation will take effect or when it will be re-listed.
Banged up abroad: How many Brits are being arrested over alleged drug smuggling?
Thailand to crack down on cannabis after smuggling cases involving UK tourists
Is cannabis legal in Thailand?
Medical marijuana has been legal in Thailand since 2018, but decriminalisation in 2022 took things a step further, making it no longer a crime to grow and trade marijuana and hemp products, or to use any parts of the plant to treat illnesses.
It was a rarity in the region where many countries give long jail terms and even death sentences for people convicted of marijuana possession, consumption or trafficking.
Smoking marijuana in public remained illegal even under the relaxed laws.
Subscribe free to our weekly newsletter for exclusive and original coverage from ITV News. Direct to your inbox every Friday morning.
What happened when cannabis was decriminalised?
The relaxed laws saw a lucrative cannabis industry catering to locals and foreigners alike boom across the Southeast Asian nation, with thousands of cannabis dispensaries sprouting up across Thailand, as well as other cannabis-themed businesses like weed cafes and hemp spas, and beauty treatment.
Cities like Chiang Mai and the capital Bangkok have even held weed festivals, and decriminalisation has been a major draw for tourists.
Pro-legislation advocates have argued that the cannabis boom across Thailand has helped many Thais, from farmers to small business owners and workers behind the counter.
Critics say the decriminalisation was rushed through, causing confusion about the regulations.
Last year, a new conservative government vowed to tighten the rules around the drug after a string of alleged smuggling cases involving tourists.
Hundreds of British citizens are currently detained across the world, accused of narcotics smuggling offences.
Prisoners Abroad – a charity assisting Britons who are arrested and detained overseas – told ITV News it is currently supporting 431 people around the globe who are facing drugs charges.
This includes 22 people in Thailand.
Source: https://www.itv.com/news/2025-06-24/thailand-to-ban-recreational-cannabis-three-years-after-decriminalisation
Inside a bright new building in the heart of Skid Row, homeless people hung out in a canopy-covered courtyard — some waiting to take a shower, do laundry, or get medication for addiction treatment. Others relaxed on shaded grass and charged their phones as an intake line for housing grew more crowded.
The Skid Row Care Campus officially opened this spring with ample offerings for people living on the streets of this historically downtrodden neighborhood. Pop-up fruit stands and tent encampments lined the sidewalks, as well as dealers peddling meth and fentanyl in open-air drug markets. Some people, sick or strung out, were passed out on sidewalks as pedestrians strolled by on a recent afternoon.
For those working toward sobriety, clinicians are on site to offer mental health and addiction treatment. Skid Row’s first methadone clinic is set to open here this year. For those not ready to quit drugs or alcohol, the campus provides clean syringes to more safely shoot up, glass pipes for smoking drugs, naloxone to prevent overdoses, and drug test strips to detect fentanyl contamination, among other supplies.
As many Americans have grown increasingly intolerant of street homelessness, cities and states have returned to tough-on-crime approaches that penalize people for living outside and for substance use disorders. But the Skid Row facility shows Los Angeles County leaders’ embrace of the principle of harm reduction, a range of more lenient strategies that can include helping people more safely use drugs, as they contend with a homeless population estimated around 75,000 — among the largest of any county in the nation. Evidence shows the approach can help individuals enter treatment, gain sobriety, and end their homelessness, while addiction experts and county health officials note it has the added benefit of improving public health.
“We get a really bad rap for this, but this is the safest way to use drugs,” said Darren Willett, director of the Center for Harm Reduction on the new Skid Row Care Campus. “It’s an overdose prevention strategy, and it prevents the spread of infectious disease.”
Despite a decline in overdose deaths, drug and alcohol use continues to be the leading cause of death among homeless people in the county. Living on the streets or in sordid encampments, homeless people saddle the health care system with high costs from uncompensated care, emergency room trips, inpatient hospitalizations, and, for many of them, their deaths. Harm reduction, its advocates say, allows homeless people the opportunity to obtain jobs, taxpayer-subsidized housing, health care, and other social services without being forced to give up drugs. Yet it’s hotly debated.
Politicians around the country, including Gov. Gavin Newsom in California, are reluctant to adopt harm reduction techniques, such as needle exchanges or supervised places to use drugs, in part because they can be seen by the public as condoning illicit behavior. Although Democrats are more supportive than Republicans, a national poll this year found lukewarm support across the political spectrum for such interventions.
Los Angeles is defying President Donald Trump’s agenda as he advocates for forced mental health and addiction treatment for homeless people — and locking up those who refuse. The city has also been the scene of large protests against Trump’s immigration crackdown, which the president has fought by deploying National Guard troops and Marines.
Trump’s most detailed remarks on homelessness and substance use disorder came during his campaign, when he attacked people who use drugs as criminals and said that homeless people “have no right to turn every park and sidewalk into a place for them to squat and do drugs.” Health and Human Services Secretary Robert F. Kennedy Jr. reinforced Trump’s focus on treatment.
“Secretary Kennedy stands with President Trump in prioritizing recovery-focused solutions to address addiction and homelessness,” said agency spokesperson Vianca Rodriguez Feliciano. “HHS remains focused on helping individuals recover, communities heal, and help make our cities clean, safe, and healthy once again.”
A comprehensive report led by Margot Kushel, a professor of medicine at the University of California-San Francisco, this year found that nearly half of California’s homeless population had a complex behavioral health need, defined as regular drug use, heavy drinking, hallucinations, or a recent psychiatric hospitalization.
The chaos of living outside, she said — marked by violence, sexual assault, sleeplessness, and lack of housing and health care — can make it nearly impossible to get sober.
The new care campus is funded by about $26 million a year in local, state, and federal homelessness and health care money, and initial construction was completed by a Skid Row landlord, Matt Lee, who made site improvements on his own, according to Anna Gorman, chief operating officer for community programs at the Los Angeles County Department of Health Services. Operators say the campus should be able to withstand potential federal spending cuts because it is funded through a variety of sources.
Glass front doors lead to an atrium inside the yellow-and-orange complex. It was designed with input from homeless people, who advised the county not just on the layout but also on the services offered on-site. There are 22 recovery beds and 48 additional beds for mostly older homeless people, arts and wellness programs, a food pantry, and pet care. Even bunnies and snakes are allowed.
John Wright, 65, who goes by the nickname Slim, mingled with homeless visitors one afternoon in May, asking them what they needed to be safe and comfortable.
“Everyone thinks we’re criminals, like we’re out robbing everyone, but we aren’t,” said Wright, who is employed as a harm reduction specialist on the campus and is trying, at his own pace, to stop using fentanyl. “I’m homeless and I’m a drug addict, but I’m on methadone now so I’m working on it,” he said.
Nearby on Skid Row, Anthony Willis rested in his wheelchair while taking a toke from a crack pipe. He’d just learned about the new care campus, he said, explaining that he was homeless for roughly 20 years before getting into a taxpayer-subsidized apartment on Skid Row. He spends most of his days and nights on the streets, using drugs and alcohol.
The drugs, he said, help him stay awake so he can provide companionship and sometimes physical protection for homeless friends who don’t have housing. “It’s tough sometimes living down here; it’s pretty much why I keep relapsing,” said Willis, who at age 62 has asthma and arthritic knees. “But it’s also my community.”
Willis said the care campus could be a place to help him kick drugs, but he wasn’t sure he was ready.
Research shows harm reduction helps prevent death and can build long-term recovery for people who use substances, said Brian Hurley, an addiction psychiatrist and the medical director for the Bureau of Substance Abuse Prevention and Control at the Los Angeles County Department of Public Health. The techniques allow health care providers and social service workers to meet people when they’re ready to stop using drugs or enter treatment.
Under harm reduction principles, officials acknowledge that people will use drugs. Funded by taxpayers, the government provides services to use safely, rather than forcing people to quit or requiring abstinence in exchange for government-subsidized housing and treatment programs.
Los Angeles County is spending hundreds of millions to combat homelessness, while also launching a multiyear “By LA for LA” campaign to build public support, fight stigma, and encourage people to use services and seek treatment. Officials have hired a nonprofit, Vital Strategies, to conduct the campaign including social media advertising and billboards to promote the expansion of both treatment and harm reduction services for people who use drugs.
The organization led a national harm reduction campaign and is working on overdose prevention and public health campaigns in seven states using roughly $70 million donated by Michael Bloomberg, the former mayor of New York.
“We don’t believe people should die just because they use drugs, so we’re going to provide support any way that we can,” said Shoshanna Scholar, director of harm reduction at the Los Angeles County Department of Health Services. “Eventually, some people may come in for treatment but what we really want is to prevent overdose and save lives.”
Los Angeles also finds itself at odds with California’s Democratic governor. Newsom has spearheaded stricter laws targeting homelessness and addiction and has backed treatment requirements for people with mental illness or who use drugs. Last year, California voters approved Proposition 36, which allows felony charges for some drug crimes, requires courts to warn people they could be charged with murder for selling or providing illegal drugs that kill someone, and makes it easier to order treatment for people who use drugs.
Even San Francisco approved a measure last year that requires welfare recipients to participate in treatment to continue receiving cash aid. Mayor Daniel Lurie recently ordered city officials to stop handing out free drug supplies, including pipes and foil, and instead to require participation in drug treatment to receive services. Lurie signed a recovery-first ordinance, which prioritizes “long-term remission” from substance use, and the city is also expanding policing while funding new sober-living sites and treatment centers for people recovering from addiction.
State Sen. Roger Niello, a Republican who represents conservative suburbs outside Sacramento, says the state needs to improve the lives of homeless people through stricter drug policies. He argues that providing drug supplies or offering housing without a mandate to enter treatment enables homeless people to remain on the streets.
Proposition 36, he said, needs to be implemented forcefully, and homeless people should be required to enter treatment in exchange for housing.
“I think of it as tough love,” Niello said. “What Los Angeles is doing, I would call it harm encouragement. They’re encouraging harm by continuing to feed a habit that is, quite frankly, killing people.”
Keith Humphreys, who worked in the George W. Bush and Barack Obama administrations and pioneered harm reduction practices across the nation, said that communities should find a balance between leniency and law enforcement.
“Parents need to be able to walk their kids to the park without being traumatized. You should be able to own a business without being robbed,” he said. “Harm reduction and treatment both have a place, and we also need prevention and a focus on public safety.”
Just outside the Skid Row Care Campus, Cindy Ashley organized her belongings in a cart after recently leaving a local hospital ER for a deep skin infection on her hand and arm caused by shooting heroin. She also regularly smokes crack, she said.
She was frantically searching for a home so she could heal from two surgeries for the infection. She learned about the new care campus and rushed over to get her name on the waiting list for housing.
“I’m not going to make it out here,” she said, in tears.
Source: https://www.news-medical.net/news/20250708/In-a-nation-growing-hostile-toward-drugs-and-homelessness-Los-Angeles-tries-leniency.aspx
|
|
by Jul 7,2025
Aims: To conduct exploratory analyses into the transported effect of the ASSIST (A Stop Smoking in Schools Trial) school-based smoking prevention intervention on weekly smoking in young people between 2004 and 2021.
Design: Secondary analysis of a cluster randomized control trial (cRCT).
Setting: England and Wales.
Participants: ASSIST trial participants comprised 8756 students aged 12-13 years in 59 schools assigned using stratified block randomization to the control (29 schools, 4193 students) or intervention (30 schools, 4563 students) condition. The target population was represented by 12-13-year-old participants in the Smoking, Drinking and Drug Use Among Young People in England Survey (SDDU) in 2004 (n = 3958), 2006 (n = 3377), 2014 (n = 3145), 2016 (n = 4874) and 2021 (n = 3587), which are randomly sampled school-based surveys with student response rates varying between 85% and 93%.
Intervention and comparator: The ASSIST intervention involved 2 days of off-site training of influential students to encourage their peers not to smoke over a 10-week period. The control group continued with their usual education.
Measurements: The outcome was the proportion of students who self-reported weekly smoking 2 years post-intervention.
Findings: The prevalence of weekly smoking at the 2-year follow-up in the ASSIST trial in 2004 was 4.1%, 49.5% of students were girls, and 7.8% ethnic minorities. In the SDDU in 2004, the prevalence of weekly smoking was 3.6%, 47.6% students were girls and 14.4% ethnic minorities and in 2021 0.2% were weekly smokers, 48.6% girls and 27.8% ethnic minorities. The odds ratio of weekly smoking in the ASSIST trial in 2004 was 0.85 [95% confidence interval (95% CI) = 0.71-1.02]. The estimated odds ratio in the SDDU target population in 2004 was 0.90 (95% CI = 0.72-1.13), in 2014 was 0.89 (95% CI = 0.70-1.14), and by 2021 was 0.88 (95% CI = 0.60-1.28). The confidence interval ratio was used to estimate precision in the transported estimates in the target population and was 1.57 in 2004, 1.63 in 2014 and 2.13 in 2021, reflecting increasing uncertainty in the effect of ASSIST over time. Subgroup analyses showed effects were comparable when restricted to only English schools in the ASSIST trial.
Conclusions: These exploratory analyses indicate the effect of the ASSIST school-based smoking prevention intervention reported in the original trial may not have been replicated in the target population over the 17-year period of its licensing and roll out.
Keywords: generalizability; prevention; randomized controlled trial; real world evidence; smoking; transportability.
Source: https://pubmed.ncbi.nlm.nih.gov/40623817/
Opinion by Kevin Sabet – SAM (Smart Approaches to Marijuana) – July 10, 2025,
President Donald Trump is facing a pivotal decision: whether to ease national restrictions on marijuana, a policy shift he hinted at during his 2024 campaign. But a major federal bust this week in Massachusetts — where the FBI arrested seven Chinese nationals connected with a multimillion-dollar pot-growing conspiracy — shows why loosening the rules would be a soft-power disaster.
First, some context.
The federal government, under the Controlled Substances Act, uses a five-part schedule to classify various drugs and other potentially addictive items. Drugs with no accepted medical use and high potential for abuse get listed on Schedule I.
That’s where marijuana is now placed — right where it belongs.
FDA-approved marijuana-based medications are rightly classified on lower schedules.
Raw weed, however, has no accepted medical use (whatever may be claimed in states that have legalized it), and addiction rates are around 30% and rising, with younger people hit hard.
That didn’t concern President Joe Biden’s Health and Human Services Department, which recommended moving cannabis to Schedule III, the list of drugs with an accepted medical use and a lower risk of abuse.
Now celebrities, star athletes and some MAGA influencers are pushing Trump to follow the Biden-era recommendation.
But this president — who correctly grasps the multifaceted strategic threat China poses to the United States — should reject their urgings.
Look at this week’s Justice Department charges.
Federal law enforcement on Tuesday rolled up a network of marijuana grow houses in Massachusetts and Maine, allegedly run by Chinese nationals and staffed with illegal immigrants pressed into what amounts to indentured servitude.
The operations generated millions of dollars in profits, which the growers sank into assets like jewelry, cars and real estate that expanded their criminal enterprise.
Chinese criminals played a major role in the US fentanyl crisis by manufacturing the drug’s precursor chemicals and selling them to Mexican cartels. Trump slammed China with a 20% tariff over that very fact.
Marijuana is looking like another big-time business unit for Beijing.
But it gets worse: China’s communist government appears to have significant links with these criminal weed enterprises.
Two Chinese nationals charged with running an illegal grow operation in Maine in 2023 had deep links to the Sijiu Association, a Brooklyn-based non-profit reportedly connected to China’s New York consulate and to the United Front Work Department — the branch of the CCP’s Central Committee that handles influence operations abroad.
Another report in 2024 tracked the connections of Zhu Di, one of China’s top US diplomats, to an Oklahoma cultural association that Sooner State authorities investigated for its links to the illicit weed business.
It’s beyond clear that Beijing smells the skunky funk of a tactical play against the United States rising from the red-hot marijuana trade.
That’s what makes rescheduling weed such a risk.
Moving marijuana to Schedule III would supercharge the pot market, letting canna-businesses take regular deductions — including on advertising — at tax time, and easing their access to banking and credit.
In other words, it would be a major step towards commercially normalizing Big Weed, and a massive boost for Chinese organized criminals with apparent CCP connections.
Worse — as New York has seen first-hand — far from eliminating the drug dealers, a juiced-up legal weed market leads to a bigger illegal market.
Post-legalization in the Empire State, New York City alone contains an estimated 3,600 illegal pot stores, dwarfing the mere dozens of legal ones. California and Michigan have seen a similar trend.
That’s yet another way rescheduling would hand an unforced victory to China, which is already elbow-deep in illegal weed operations stateside.
The worst part is that there’s no domestic benefit to this trade-off.
If weed goes on Schedule III, it will do nothing except help addiction profiteers get rich — and damage public health irreparably, even as a flood of new data confirms that marijuana is as bad as it gets for users’ mental and physical well-being.
Heart disease, schizophrenia, dementia, even tooth rot: Weed truly is the drug that does it all.
Yes, the American public seems to be waking up. Every state considering recreational marijuana at the ballot box in 2024 rejected it.
But Trump should remember that Beijing will exploit any and every policy misstep we make to the utmost.
Rescheduling marijuana would put Americans last, at home and abroad — and usher in the very opposite of the Golden Age the president has so memorably promised.
Kevin Sabet is president of Smart Approaches to Marijuana and a former White House drug policy adviser.
Source: https://nypost.com/2025/07/10/opinion/easing-weed-rules-will-harm-golden-age-and-boost-china/
Exactly one year ago today, we became the European Union Drugs Agency (EUDA) and embarked on our new mission to strengthen EU preparedness on drugs. Building on the work of the EMCDDA, and with a more proactive mandate, we set off to support the EU and its Member States in addressing emerging drug issues in an ever-changing world. Our work contributes to making Europe’s streets safer and to saving lives. Our motto — ‘Acting today, anticipating tomorrow’.
In our role, we help policymakers anticipate and respond effectively to drug-related threats. We issue health and security alerts and risk communications, share knowledge and recommend evidence-based policies and actions to address problems efficiently.
This first year has been one of many milestones. Among our achievements in these 12 months as the EUDA, we have:
Transforming from the EMCDDA into the EUDA marked the most significant organisational shift in the agency to date. To rise to this challenge, we accelerated our business transformation to build the capabilities needed to deliver innovative, future-oriented services while providing core monitoring services to support EU drug policy.
With a renewed baseline vision of being ‘your European Union Drugs Agency’, we enter our second year with a clear commitment to lead, innovate and partner in tackling drug-related challenges — for a healthier, safer and more resilient Europe.
Source: https://www.euda.europa.eu/news/2025/first-anniversary-euda-delivers-key-gains-strengthening-europes-preparedness-drugs_en

A study published Wednesday in the medical journal JAMA Network Open found that emergency room clinicians were much less likely to refer Black opioid overdose patients for outpatient treatment compared with white patients.
The researchers looked at the medical records of 1,683 opioid overdose patients from emergency rooms in nine states: California, Colorado, Georgia, Michigan, Missouri, New Jersey, New York, Oregon and Pennsylvania.
About 5.7% of Black patients received referrals for outpatient treatment, compared with 9.6% of white patients, according to the researchers, who received a federal grant from the National Institute on Drug Abuse to conduct the analysis.
While the nation saw a decrease in opioid overdose deaths in white people between 2021 and 2022, overdose death rates increased for American Indian, Alaska Native, Asian, Black and Hispanic people. Patients visiting ERs for opioid overdoses are more likely to die from an overdose after the visit, the authors wrote, underscoring the importance of gaining “an improved understanding of disparities in [emergency department] treatment and referral.”
In total, roughly 18% of the patients received a referral for outpatient treatment, 43% received a naloxone kit or prescription, and 8.4% received a prescription for buprenorphine, the first-line medication for treating opioid use disorder.
The researchers used records from 10 hospital sites participating in a national consortium collecting data on overdoses from fentanyl and its related drugs. The patient records were from September 2020 to November 2023.
Another study in JAMA Network Open, released last week, found similar disparities: Black and Hispanic patients were significantly less likely than white patients to receive buprenorphine. Black patients had a 17% chance, and Hispanic patients a 16% chance, to be prescribed the therapy, compared with a 20% chance for white patients.
The authors of that study, from the Icahn School of Medicine at Mount Sinai in New York City, looked at data from 176,000 records of opioid-related events between 2017 and 2022 across all 50 states.
Source: https://www.newsfromthestates.com/article/new-studies-find-wide-racial-disparities-opioid-overdose-treatment-referrals
From: Herschel Baker – International Liaison Director, Drug Free Australia – 06 July 2025
Drug Free Australia forwarded this paper by Dr Ross Colquhoun, Executive Committee Member and Research Fellow for DFA.
The paper runs to 105 pages; was written on April 12, 2025 and was posted on 2 May 2025
https://acrobat.adobe.com/id/urn:aaid:sc:AP:23cb5790-410e-4a7b-be9d-0d6d9a30bdaa?
This paper presents a critical evaluation of opioid agonist treatment (OAT), particularly methadone maintenance treatment (MMT), compared with opioid antagonist therapy using naltrexone. Drawing on a broad body of literature including randomized controlled trials, cohort studies, and government reports, the paper questions the longstanding assumptions regarding the effectiveness and safety of methadone. It highlights serious concerns regarding methadone-related mortality-especially during induction and cessation phases-long-term dependency, limited efficacy in preventing illicit drug use, and poor impact on the transmission of blood-borne viruses such as HIV and hepatitis C. The review also exposes methodological weaknesses and selective reporting in key studies supporting MMT. In contrast, evidence is presented to support the safety and effectiveness of long-acting naltrexone implants, which offer lower relapse rates, improved social functioning, and the potential for complete abstinence without ongoing opioid dependency. The paper argues that the continued privileging of methadone by public health institutions may be driven more by ideology and institutional inertia than evidence. It calls for a re-evaluation of harm reduction policies and urges greater accessibility to abstinence-focused, naltrexone-based treatment options, along with ancillary psychological and medical support. Recommendations include transparency in data reporting, broader dissemination of naltrexone research, and a policy shift toward full recovery rather than prolonged maintenance.
Keywords: Opioid Use Disorder (OUD), Methadone Maintenance Treatment (MMT), Naltrexone, Opioid Agonist Treatment (OAT), Harm Reduction, Opioid Dependency, Relapse Prevention, Public Health Policy, Overdose Mortality, Evidence-Based Treatment
Suggested Citation:
To access the full document:
UNITED NATIONS, Jun 27 (IPS) – Since 1989, the United Nations (UN) has recognized June 26 as the International Day Against Drug Abuse and Illicit Trafficking in an effort to raise awareness around the global drug problem and foster a more compassionate world, free of drug abuse. Through this year’s campaign, “Break the Cycle. #StopOrganizedCrime”, the UN underscores the importance of addressing the root causes of global drug abuse and illegal drug trading, and investing in reliable systems that prioritize prevention, education, and health.
Concurrently, the United Nations Office on Drugs and Crime (UNODC) released its annual World Drug Report, in which it analyzed the current trends in global drug abuse amid a “new era of global instability”. In the report, UNODC emphasizes the wide ranging implications of drug use on the economy, the environment, global security, and human society.
According to the report, roughly 316 million people used drugs (excluding tobacco and alcohol) around the world in 2023. UNODC also estimates that nearly half a million people around the world die annually as a result of drug use disorders, indicating a “global health crisis”. Roughly 28 million years of life are lost annually from disabilities and premature deaths due to addiction. Furthermore, there is an overwhelming lack of healthcare and education resources for individuals with drug use disorders, as only one in twelve people are estimated to have received treatment in 2023.
Cocaine has been described as the world’s fastest growing illicit drug in terms of global usage, production, and seizures. In 2023, approximately 3,708 tons of cocaine were produced, marking a 34 percent increase from the previous year. Roughly 2,275 tons were seized in 2023, a 68 percent increase from 2019’s figures. Additionally, global usage of cocaine has inflated to 25 million users in 2023.
As nations began to implement harsher crackdowns on drug production, the use and transportation of synthetic drugs, such as fentanyl and methamphetamine, has reached record-highs, accounting for nearly half of all global drug seizures. Drug trafficking groups have found ways to chemically conceal these drugs, making distribution much easier.
UNODC Executive Director Ghada Fathi Waly states that organized drug trafficking groups around the world continue to exploit global crises, disproportionately targeting the most vulnerable communities. With worldwide synthetic drug consumption having surged in recent years, the UNODC forecasts that civilians displaced by armed conflicts face heightened risks of drug abuse and addiction.
Although the cocaine market was once contained in Latin America, trade has extended through to Asia, Africa, and Western Europe, with Western Balkans having greater shares in the market. This is a testament to the influence of organized crime groups in areas facing instability, natural disasters, and economic challenges.
According to the report, since the end of the Assad regime in Syria and the subsequent political transition, nationwide use of fenethylline — also known as captagon, a cheap, synthetic stimulant — has soared. Although the transitional government of Syria has stated that there is zero tolerance for captagon trade and consumption, UNODC warns that Syria will remain a significant hub for drug production.
Angela Me, the Chief of Research and Analysis at UNODC, states that captagon use in the Arabian peninsula was spurred by regional violence, with members of terrorist organizations using it on battlefields to stay alert. Due to its highly addictive properties, as well as its severe impacts on physical and mental health, the drug has seen widespread consumption over the past several years.
“These groups have been managing Captagon for a long time, and production is not going to stop in a matter of days or weeks,” said Me. “We see a lot of large shipments going from Syria through, for example, Jordan. There are probably still stocks of the substance being shipped out, but we’re looking at where the production may be shifting to. We’re also seeing that the trafficking is expanding regionally, and we’ve discovered labs in Libya.”
Global drug trafficking is estimated to generate billions of dollars per year. National budgets to combat drug trafficking, in terms of law enforcement and prosecution, cost governments millions to billions annually as well. Healthcare systems, which are often underfunded for addiction-related treatments, are overwhelmed by the vast scale of needs. Furthermore, damages related to theft, vandalism, violence, and lost productivity in the workplace have significant impacts on gross domestic products.
Additionally, increased rates of deforestation and pollution are linked with global drug cultivation. Additional adverse environmental impacts include ecosystem damage from drug waste, which yields notable costs in environmental restoration efforts.
It is imperative for governments, policymakers, and other stakeholders to invest in programs that disrupt illicit drug trafficking groups and promote increased security, especially along borders, which are critical hubs for transporting concealed substances. Furthermore, cooperation at an international level is instrumental for the transfer of information and promoting a joint and multifaceted approach.
“We must invest in prevention and address the root causes of the drug trade at every point of the illicit supply chain. And we must strengthen responses, by leveraging technology, strengthening cross-border cooperation, providing alternative livelihoods, and taking judicial action that targets key actors driving these networks,” said Waly. “Through a comprehensive, coordinated approach, we can dismantle criminal organizations, bolster global security, and protect our communities.”
Source: https://www.globalissues.org/news/2025/06/27/40295
Assistant Professor of Public Health, University of Mississippi
Once associated with high-profile figures like John Belushi, River Phoenix and Chris Farley , this dangerous polysubstance use has become a leading cause of overdose deaths across the United States since the early- to mid-2010s.
I am an assistant professor of public health who has written extensively on methamphetamine and opioid use and the dangerous combination of the two in the United States.
As these dangerous combinations of drugs increasingly flood the market, I see an urgent need and opportunity for a new approach to prevention and treatment.
Dating back to the 1970s, the term speedballing originally referred to the combination of heroin and cocaine. Combining stimulants and opioids – the former’s “rush” with the latter’s calming effect – creates a dangerous physiological conflict.
According to the National Institute on Drug Abuse, stimulant-involved overdose fatalities increased markedly from more than 12,000 annually in 2015 to greater than 57,000 in 2022, a 375% increase. Notably, approximately 70% of stimulant-related overdose deaths in 2022 also involved fentanyl or other synthetic opioids, reflecting the rising prevalence of polysubstance involvement in overdose mortality.
Users sought to experience the euphoric “rush” from the stimulant and the calming effects of the opioid. However, with the proliferation of fentanyl – which is far more potent than heroin – this combination has become increasingly lethal. Fentanyl is often mixed with cocaine or methamphetamine, sometimes without the user’s knowledge, leading to unintentional overdoses.
The rise in speedballing is part of a broader trend of polysubstance use in the U.S. Since 2010, overdoses involving both stimulants and fentanyl have increased 50-fold, now accounting for approximately 35,000 deaths annually.
This has been called the fourth wave of the opioid epidemic. The toxic and contaminated drug supply has exacerbated this crisis.
A dangerous combination of physiological effects
Stimulants like cocaine increase heart rate and blood pressure, while opioids suppress respiratory function. This combination can lead to respiratory failure, cardiovascular collapse and death. People who use both substances are more than twice as likely to experience a fatal overdose compared with those using opioids alone.
The conflicting effects of stimulants and opioids can also exacerbate mental health issues. Users may experience heightened anxiety, depression and paranoia. The combination can also impair cognitive functions, leading to confusion and poor decision-making.
Speedballing can also lead to severe cardiovascular problems, including hypertension, heart attack and stroke. The strain on the heart and blood vessels from the stimulant, combined with the depressant effects of the opioid, increases the risk of these life-threatening conditions.
Increasing awareness about the dangers of speedballing is crucial. I believe that educational campaigns can inform the public about the risks of combining stimulants and opioids and the potential for unintentional fentanyl exposure.
There is a great need for better access to treatment for people with stimulant use disorder – a condition defined as the continued use of amphetamine-type substances, cocaine or other stimulants leading to clinically significant impairment or distress, from mild to severe. Treatments for this and other substance use disorders are underfunded and less accessible than those for opioid use disorder. Addressing this gap can help reduce the prevalence of speedballing.
Implementing harm reduction strategies by public health officials, community organizations and health care providers, such as providing fentanyl test strips and naloxone – a medication that reverses opioid overdoses – can save lives.
These measures allow individuals to test their drugs for the presence of fentanyl and have immediate access to overdose-reversing medication. Implementing these strategies widely is crucial to reducing overdose deaths and improving community health outcomes.
Source: https://theconversation.com/speedballing-the-deadly-mix-of-stimulants-and-opioids-requires-a-new-approach-to-prevention-and-treatment-257425
Andrew Yockey does not work for, consult, own shares in or receive funding from any company or organisation that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.
 |
by Sihyun Baek,
Grade 11, (16-17 years old) Chadwick International School 06.29.2025 |

[AI Generated, Addiction. Photo Credit to Pixabay]
South Korea is grappling with a mounting crisis as incidents of teenage drug use increase exponentially, raising serious concerns about youth safety and failed public education systems.
The latest incident, involving two middle schoolers caught using marijuana in a neighborhood playground in Seoul on April 25, has once again brought the issue to the forefront for concerned parents, teachers, and lawmakers alike.
The students were seen smoking liquid cannabis in broad daylight, prompting local residents to notify the police.
Authorities are currently looking into how the teens obtained the drugs.
Nationally, the number of juvenile drug offenders, aged 18 and younger, rose to 450 in 2021, marking a 43.8% increase from the previous year and nearly quadrupling since 2018, according to the Supreme Prosecutors’ Office.
In Seoul alone, teenage drug offenders surged nearly fivefold in just one year, from 48 in 2022 to 235 in 2023.
South Korea, known for its stringent drug laws and historically low rates of domestic usage, now finds itself fighting against a growing number of youth turning to drugs through online platforms and encrypted messaging services like Telegram.
The rise of drug transactions using anonymous cryptocurrency transactions such as Bitcoin has dramatically lowered the barriers to accessing such substances online.
In one case during the summer of 2022, for instance, a drug cartel run entirely online by an 18-year-old using encrypted apps to distribute methamphetamine and MDMA was exposed by police officers.
Similarly, in November of 2021, a drug-trading chat room was discovered on Telegram.
Prosecutors revealed that all 180 members of the chat room were members of a criminal drug organization, most of whom were teenagers.
But marijuana and party drugs aren’t the only substances of concern.
Illegally obtained prescription psychotropic medications are emerging as the country’s primary gateway drugs.
An increasing number of teenagers have been caught distributing fentanyl patches and pills like Dietamin, an appetite suppressant.
The pill, however, is also a dangerous psychotropic drug derived from amphetamines that produces hallucinations and has addictive properties.
These prescription drugs, often perceived as “safe” or “medically approved,” are creating a dangerous normalization of drug use among teens and increasing the risk of long-term addiction and overdose.
From 2019 to 2021, prescription psychotropics accounted for 55.4% of youth drug cases, followed by cocaine and heroin at 23.8%, and marijuana at 20.8%.
In one major investigation in June of 2023, 100 teenagers in South Gyeongsang Province were arrested for selling and abusing Dietamin tablets obtained online.
Experts point to peer pressure and stress as the key triggers, particularly within Telegram chat rooms.
Pop culture also plays a significant role; for example, fentanyl was commonly used by hip-hop rappers in 2019 and has since grown in popularity among teenagers.
To counter this growing issue, authorities have begun intense cyber investigations.
In 2023 alone, more than 1,000 online crackdowns led to the shutdown of 78 drug-dealing accounts on platforms like Telegram and Instagram.
Yet, the increasingly sophisticated methods of drug distribution pose serious challenges for law enforcement.
Dealers frequently change their online handles, communicate in code using emojis, and utilize “dead drop” methods, such as hiding drugs in public spaces for buyers to retrieve using GPS coordinates, making it difficult for someone to trace their tracks.
Understandably, the consequences of this rise in drug use among teenagers are devastating.
Drug abuse has been directly linked to an increase in youth suicide attempts.
Between 2019 to mid-2023, approximately 46.4% of teen suicide attempts resulting in hospitalization were associated with drug use, according to the National Medical Center.
In 2021 alone, 1,678 minors were treated for drug abuse, a 41.4% jump from the previous year.
To combat this issue, many suggest implementing strengthened education systems on drugs by collaborating with related institutions.
Likewise, while some lawmakers have recently proposed bills to mandate such education programs, experts say the movement lacks urgency and public support and is failing to garner much attention, with the country having yet to integrate drug prevention into its national school curriculum.
For instance, in May of 2024, Government Representative Lee Tae-kyu proposed a bill to mandate drug education in schools, requiring them to implement age-specific drug education programs in collaboration with public health agencies.
However, as of now, the bill remains stalled in committee.
Comparatively, in the United States, the implementation of Drug Abuse Resistance Education (DARE) programs nationwide began as early as the 1980s, laying the foundation for more modern prevention strategies.
Simultaneously, South Korea continues to face a lack of infrastructure for rehabilitation sites, as they still remain largely underdeveloped.
Experts estimate that around 40% of Korean drug offenders return to prison within three years of their release.
Such a high rate is often linked to the stigma they face in society, with many struggling to find employment, being rejected by hospitals, and being generally excluded from mainstream social life.
Likewise, the number of rehabilitation facilities for minors is limited.
KAADA, one of the few rehabilitation centers for teen users, receives about 1,000 patients per year, only 10% of whom are under 19.
Experts note that this is not reflective of actual use rates, but rather the result of underreporting and such social stigma that keep teens and their families silent.
Data gaps also hinder progress.
Because many teen users are released as first-time offenders, their cases often fail to reach prosecutors, resulting in underreported figures.
This makes it harder for lawmakers to assess the full scale of the crisis or design policies that address it adequately.
Parents have taken to online forums to express their fears, demanding school assemblies, national awareness campaigns, and stricter regulations on medical prescriptions.
In an interview with Ms. Cha, a concerned parent, commented, “It worries me even more because I don’t have a way of knowing what my child does online, especially as he gets older. You have to respect their autonomy, but at the same time, they could be accessing websites and chat rooms they shouldn’t be in.”
Another parent, Mr. Kim, stated, “We need more education programs about drug prevention at school. Our children know that drugs are bad, but they don’t fully understand the long-term consequences or how easily peer pressure can lead them down the wrong path.”
Source: http://www.heraldinsight.co.kr/news/articleView.html?idxno=5498
Salalah, 25 Jun (ONA) — The Ministry of Social Development, in Dhofar Governorate, organized today a community event titled “A Nation Free from Drugs” to raise awareness about the dangers of narcotics and psychotropic substances.
The initiative aimed to educate the public on the threat of drug abuse, its societal risks, and the importance of collective prevention while fostering health, social and cultural awareness.
The event featured a panel discussion titled “A Nation Free from Drugs,” where experts addressed the societal impacts of addiction and strategies for prevention and treatment.

“A Nation Free from Drugs” Awareness Campaign Held in Salalah.
Source: https://www.omannews.gov.om/topics/en/128/show/123051/ona

TORONTO, ONTARIO, CANADA, June 23, 2025 /EINPresswire.com/ — In his compelling and illuminating new book, “Single Handed,” retired lieutenant and police detective Joseph M. Kress reveals the stark realities of America’s ongoing drug crisis and the concerning shortcomings of the nation’s drug prevention programs. Inspired by true events, the story uncovers a journey shaped by tragedy and the hardened years in law enforcement.
The book begins with a very personal and tragic event: Joe Kress’s brother Greg was murdered while on his honeymoon following a robbery in New Orleans. This shocking act of violence sparks Joe’s determination to join the police force. What follows is a vivid, rapid-fire narrative of Joe’s years as an officer, exploring a diverse array of cases that unveil the most sinister aspects of society, from child disappearances to horrific sexual assaults. Despite suffering a gunshot wound to his leg and having to retire early due to injury, Joe is shown to be a man who is motivated by duty throughout it all.
However, “Single Handed” does not conclude with Joe’s time in uniform. In fact, the narrative takes a turn into thrilling and audacious realms. After leaving official service, Joe sets off on a unique journey of his own creation: pursuing drug dealers nationwide. Utilizing his SWAT training and special operations background, he embarks on a mission to tackle the soaring drug-related crime rates affecting American neighborhoods. This unfolds a vigilante crusade, crafted from genuine frustration and moulded by years of direct involvement in law enforcement and profound personal grief.
Amazon reviewer Sanjin highlights the book as crucial and relevant, praising the author’s direct and engaging storytelling that sheds light on an ongoing crisis affecting communities today. In a similar vein, reader Clarence Joseph shares this sentiment, highlighting that the story’s expertly crafted pace not only amplifies its suspense but also provides a captivating and delightful reading journey.
Source: https://fox59.com/business/press-releases/ein-presswire/824883015/joseph-m-kress-exposes-the-dark-reality-of-americas-drug-crisis-through-his-latest-candid-memoir/
|
|
|
by Ingrid Fadelli, Phys.org – edited by Gaby Clark, reviewed by Robert Egan – The GIST – June 26, 2025
Omicron Limited’ 36 Hope Street, Douglas, IM1 1AR, Isle of Man
While some studies have found that cannabis and especially cannabidiol (i.e., the non-intoxicating compound contained in it) can have medicinal effects, others have linked the abuse of its psychoactive variations (i.e., containing tetrahydrocannabinol or THC) with a greater risk of being diagnosed with psychiatric disorders.
As many individuals worldwide use cannabis on a regular basis, understanding the mechanisms that could link its consumption with psychiatric disorders could be highly valuable, as it might help to identify factors that increase the risk of developing specific disorders.
In a paper published in Nature Mental Health, researchers at Yale University School of Medicine, the Veterans Affairs Connecticut Healthcare System and Washington University School of Medicine shed new light on the genetic associations between cannabis use, cannabis use disorder (CanUD) and various psychiatric disorders.
CanUD is a mental health disorder characterized by a continued use of cannabis, difficulties experienced when trying to cut down its consumption or cease using it altogether, and an interference of the substance with daily activities, relationships or responsibilities.
“Increasing prevalence of cannabis use and CanUD may increase risk for psychiatric disorders,” wrote Marco Galimberti, Cassie Overstreet and their colleagues in their paper. “We evaluated the relationships between these cannabis traits and a range of psychiatric traits, running global and local genetic correlations, genomic structural equation modeling, colocalization analyses and Mendelian randomization analyses for causality.”

The researchers analyzed genetic, psychiatric and psychological data collected as part of earlier studies, using various statistical techniques. First, they tried to detect genetic patterns that linked cannabis use with specific psychiatric and personality traits, using a technique known as genomic structural equation modeling.
Subsequently, they ran colocalization analyses, a statistical analysis that allowed them to uncover instances where two traits shared the same underlying genetic variant. Finally, they used a technique called Mendelian randomization to uncover causal relationships between traits, or in other words, if a sporadic or problematic use of cannabis caused specific disorders via genetic factors and vice versa.
“Global genetic analyses identified significantly different correlations between CanUD and cannabis use,” wrote Galimberti, Overstreet and their colleagues. “A variant in strong linkage disequilibrium to one regulating CHRNA2 was significantly shared by CanUD and schizophrenia in colocalization analysis and included in a significant region in local genetic correlations between these traits. A three-factor model from genomic structural equation modeling showed that CanUD and cannabis use partially map together onto a factor with major depressive disorder and ADHD.”
Interestingly, the researchers found that although cannabis use and CanUD are in some ways related, they had different genetic relationships with psychiatric disorders. In fact, they found that variations in the regulation of the gene CHRNA2, which has also been linked to nicotine consumption and dopamine signaling, were common to both schizophrenia and CanUD, but not to casual or general cannabis use.
“In terms of causality, CanUD showed bidirectional causal relationships with most tested psychiatric disorders, differently from cannabis use,” wrote Galimberti, Overstreet and their colleagues. “Increasing use of cannabis can increase rates of psychiatric disorders over time, especially in individuals who progress from cannabis use to CanUD.”
Overall, the findings of this recent study suggest that there is a bi-directional genetic relationship between the abuse of cannabis, specifically CanUD, and various psychiatric disorders, including schizophrenia, ADHD, depression, and bipolar disorder. In other words, it appears that CanUD could increase the risk of developing mental health disorders, and being diagnosed with some psychiatric disorders could also prompt abuse of cannabis.
This recent work could potentially inform the development of public health interventions aimed at monitoring or limiting people’s consumption of cannabis early, to reduce the risk that they will later develop psychiatric disorders. In addition, the analyses could inspire other research groups to delve deeper into the genetic associations they uncovered, potentially by analyzing a wider pool of genetic, psychological and medical data.
Written for you by our author Ingrid Fadelli, edited by Gaby Clark , and fact-checked and reviewed by Robert Egan —this article is the result of careful human work. We rely on readers like you to keep independent science journalism alive. If this reporting matters to you, please consider a donation (especially monthly). You’ll get an ad-free account as a thank-you.
More information: Marco Galimberti et al, The genetic relationship between cannabis use disorder, cannabis use and psychiatric disorders, Nature Mental Health (2025). DOI: 10.1038/s44220-025-00440-4.
Source: https://medicalxpress.com/news/2025-06-explores-genetic-link-cannabis-psychiatric.html
by Haoliang Cui1; Jianyi Zhang1; Wenkai Luo1; Erri Du2; Zhongwei Jia1, , and Corresponding Author Zhongwei Jia, jiazw@bjmu.edu.cn
Author affiliations
The recognition of drug use as a global challenge requiring coordinated international response began with the first international conference on narcotic drugs held in Shanghai in 1909. Throughout the 20th century, three pivotal United Nations (UN) conventions on drug control (1961, 1971, and 1988) established the legal and institutional framework for a comprehensive multilateral system addressing prevention and enforcement. The creation of the United Nations Office on Drugs and Crime (UNODC) in 1997 further underscored the widespread nature of drug-related challenges confronting societies worldwide (1–2).
As nations develop more sophisticated approaches to addressing global drug challenges, international surveillance data continue to underscore both the magnitude of the problem and the critical importance of prevention strategies. The global population using drugs has reached 292 million in 2022, representing a 20% increase over the past decade (3). Particularly concerning is the finding that cannabis use prevalence among adolescents aged 15–16 years exceeds that of adults worldwide (3). It was estimated that 84 million adults aged 15–64 in Europe had used cannabis at least once, including approximately 15.3 million young adults aged 15–34 based on the European Drug Report 2023. (4). Similarly, in 2022, an estimated 70.3 million individuals aged 12 or older in the United States reported illicit drug use within the past year, with peak prevalence occurring among young adults aged 18 to 25. These statistics demonstrate the urgent need for targeted prevention investments, particularly among youth populations (5).
China has actively contributed to and responded to these global drug control initiatives. The Anti-Drug Law of the People’s Republic of China (6) was enacted in 2007, establishing a comprehensive triadic strategy that encompasses prevention, punishment, and rehabilitation. Following the law’s implementation, the number of newly identified drug users increased steadily, reaching its peak in 2015 (Figure 1). However, a series of national initiatives — including the “People’s War on Drugs,” the “Sword Action” (Liangjian Project), and the deployment of “Skynet” surveillance systems — led to a significant decrease in newly identified drug users. This decline was particularly pronounced during and after the COVID-19 pandemic, when the number of newly found drug users experienced a sharp drop (Figure 1).
The theme of this year’s International Day Against Drug Abuse and Illicit Trafficking — “The evidence is clear: invest in prevention, Break the cycle, Stop Organized Crime” (7) — underscores the public health nature of the drug problem and emphasizes the critical importance of preventive measures (Figure 2). The evolution of these annual themes reflects a fundamental shift in global attitudes toward drug policy. From 1996 to 2009, themes primarily emphasized the dangers and harmful consequences of drug use. The second stage (2010 to 2015) began treating the drug problem as a public health issue rather than solely a criminal justice matter. Since 2016, the focus has shifted toward prevention, early intervention, and youth-centered strategies, reflecting a more comprehensive and evidence-based approach to drug policy.
Nevertheless, emerging risks continue to challenge existing frameworks. Recent cases of adolescent substance abuse involving compounds not yet under formal regulatory control, such as nitrous oxide and etomidate, have been documented across China (8). Since January 2021, Guangzhou in Guangdong Province has implemented targeted enforcement measures against nitrous oxide distribution, resulting in 46 investigated cases by June 2022 (9). These novel psychoactive substances present distinct challenges due to their accessibility through online platforms, ambiguous legal classification, and limited public awareness — particularly among adolescents. In response to these evolving threats, the Ministry of Justice issued a national directive in early 2025 emphasizing “intensified drug prevention campaigns targeting adolescents” (10). Through strategic investments in early education programs, enhanced cross-sector collaboration, and implementation of evidence-based policy frameworks, China is proactively adapting its approach to address the dynamic landscape of emerging drug-related risks.

FIGURE 1. Trends in newly identified drug users in China, 2007–2022.
Note: Data from 2007 to 2013 were sourced from the Drug Abuse Population Estimation in the Key Cities of the Ministry of Public Security, while data from 2014 to 2022 were obtained from the respective annual editions of the Drug Situation in China report.
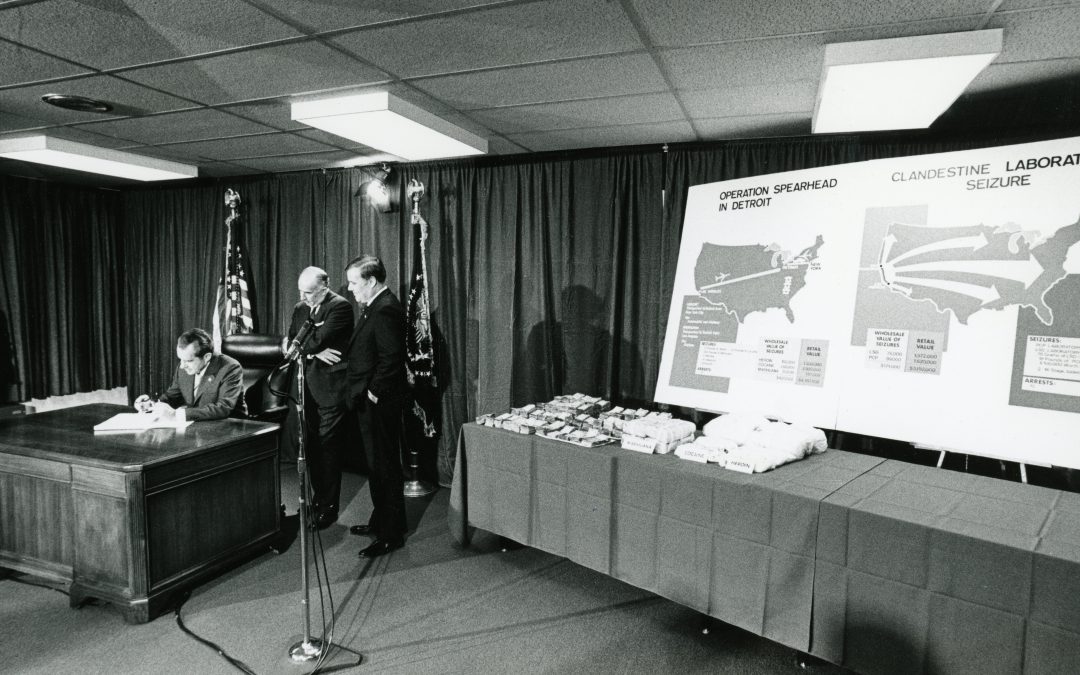
Contrary to the popular narrative, President Nixon’s comprehensive approach to drug policy provided an effective solution to a growing problem.
In the 1970s, the United States faced a growing heroin epidemic. By 1970, there were an estimated 600,000 heroin addicts and 7,200 overdose deaths—a crisis that demanded a national response.
President Richard Nixon took decisive action to address this crisis. While he did declare drug abuse “public enemy number one,” the phrase “war on drugs” was largely a media invention. The public perception that Nixon launched a punitive campaign against drugs has overshadowed the more nuanced reality of his policy and its measurable success.
Judge Robert Bonner, former DEA administrator and U.S. District Court judge, addressed this misconception during remarks at the Nixon Library on August 22, 2023. In his research into President Nixon’s drug policy, Bonner found that Nixon used the term “war on drugs” only once—in a little-known speech to Customs personnel in Texas. As Bonner put it, “The ‘war on drugs’ is a horrid metaphor. We’ve never treated it as a war, never funded it like one, and there’s no ultimate victory.”
Journalist Charles Fain Lehman, a Robert Novak Journalism Fellow, echoed this sentiment: “Despite what critics claim, there is no fifty-year straight line from Nixon to Reagan’s drug war.”
Instead of approaching the acute drug crisis like a war, President Nixon developed a strategic, two-pronged approach aimed at reducing heroin addiction in America. His strategy targeted both demand and supply. On the demand side, he expanded treatment and prevention programs. On the supply side, he cracked down on drug trafficking through law enforcement and international diplomacy. As Lehman puts it, “his policy agenda was responsive to a real and substantial drug epidemic, one which merited a proportional government response.”
One of President Nixon’s earliest legislative achievements was the Controlled Substances Act of 1970, the first comprehensive federal drug law. Contrary to later tough-on-crime narratives, this law actually eliminated mandatory minimum sentences for drug offenses—sentences that would only return with the Drug Abuse Act of 1986 under a different administration.
To enforce drug laws more effectively, President Nixon created the Drug Enforcement Administration (DEA), the first federal agency with a singular mission to combat drug trafficking. Under his leadership, the DEA partnered with international allies to curb the global heroin trade. In just two years, Nixon’s team helped disrupt heroin routes through France and negotiated efforts to ban opium production in Turkey. According to Bonner, these efforts helped reduce the number of heroin addicts in the U.S. from approximately 600,000 to fewer than 100,000—a number that remained low for over a decade.
Further busting the myth of a drug war, compassion was core to President Nixon’s drug policy. “Heroin addiction is a problem that demands compassion, not simply condemnation,” he said. To put that compassion into action, he created the Special Action Office for Drug Abuse Prevention and appointed Dr. Jerome Jaffe—a pioneer in addiction treatment—to lead it. One of the key objectives President Nixon assigned to Jaffe was addressing the treatment of servicemen returning from Vietnam with heroin addiction—an issue that, according to a 1971 congressional report, affected an estimated 30,000 to 40,000 veterans. Under President Nixon’s leadership, federally funded heroin treatment and education programs expanded dramatically. As Lehman noted, “Nixon spent more on drug treatment than enforcement year after year, and pioneered the use of methadone maintenance treatment.”
Richard Nixon’s approach—combining treatment, enforcement, and diplomacy—laid the groundwork for a more balanced and effective drug policy. As Bonner concluded, “In short, Nixon understood the problem. He also did something about it. It was a whole government effort—and it worked.”
View Judge Robert Bonner’s full remarks:
Bonner, Robert. Judge. 23 August 2023. Keynote Remarks by Judge Robert Bonner, YouTube, August 23, 2023.
Lehman, Charles Fain. “What Was the War on Drugs? Part I.” The Causal Fallacy, May 6, 2025.
Lehman, Charles Fain. “What Was the War on Drugs? Part II.”The Causal Fallacy, May 7, 2025.

As addiction clinicians and researchers, we have an obligation not only to improve our abilities at fighting the fires of active addiction, but also to enhance our ability to facilitate the processes of rebuilding in the aftermath, to reduce their future recurrence. Increasing the number of people achieving long-term recovery from SUDs is a national policy priority and a major goal of the research supported by NIDA—from basic neuroscience to understand how the brain rewires and recovers after addiction to an intensified focus on the supports and services that can help individuals thrive as they build healthier lives.3
Fortunately, the very same adaptability and neuroplasticity of the brain that makes it susceptible to developing addiction in the first place also enables it to heal, especially when internal and external conditions are supportive of recovery. The neurobiology underlying remission from SUDs has long been a focus of NIDA-funded research. Over two decades ago, as a NIDA grantee, I and my colleagues at Brookhaven National Laboratory and SUNY-Stony Brook used PET neuroimaging to show the recovery of lost dopamine transporters in the striatum of people with methamphetamine use disorder after prolonged abstinence.4 More recent longitudinal neuroimaging studies of people in SUD treatment show structural recovery in frontal cortical regions, insula, hippocampus, and cerebellum, and functional and neurochemical recovery in prefrontal cortical and subcortical regions.5
As the individual learns new behaviors, goals, and rewards, the learning process reshapes synaptic connectivity across a range of circuits, ultimately outcompeting drug-related memories and automatic behavioral patterns, which weaken over time.6 Among ongoing NIDA-funded projects is a study homing in on the circuits associated with medication adherence in patients with opioid use disorder (OUD) and those that predict return to opioid use during medication treatment. Another project is using biweekly neuroimaging of patients taking medications to treat OUD to characterize neural trajectories of remission.
NIDA has also made a major investment in research on services and supports that can make it easier for people in recovery to continue to choose non-drug rewards and thereby facilitate this neural rewiring. Such services may prove to be at least as important as treatment or overdose reversal in maintaining the recent gains made in reducing overdose deaths. A 2022 dynamic modeling study funded by the FDA projected that people returning to opioid use after a period of remission will account for an increasing proportion of OUD cases over the coming decade, compared to people newly developing OUD.7 Consequently, the authors found that, of 11 strategies to reduce OUD and fatal overdoses, services that help people stay in remission from OUD were likely to be among the most impactful.
Over the past few years, NIDA has funded several grants with the aim of building the infrastructure necessary to advance the science of recovery support. They included grants in 2020 and 2022 that supported the development of networks of recovery researchers working to establish key measures for the field, as well as clinical trial planning grants that establish the foundation necessary to conduct future large-scale clinical trials to understand the effectiveness of various recovery support services. NIDA is also supporting research on how to deliver services to groups like adolescents and young adults and people involved in the criminal-justice system, and to identify factors that are most predictive of recovery outcomes like recovery identity and meaningfulness.
One defining feature of recovery support services is the central role of peers who have lived or living experience of SUD. It can involve individual support by recovery coaches, living or working in settings with others in recovery such as recovery housing or recovery community centers, or mutual-aid groups like traditional 12-step programs and newer models like SMART Recovery. Among the many questions being addressed by NIDA grantees, therefore, are ways to support peers and their professional advancement to foster a more sustainable recovery workforce. NIDA is also working with startups to develop apps and other digital tools that can be used to facilitate connecting to peers, including mobile apps and digital peer-support platforms accessible in treatment settings for patients who are socioeconomically disadvantaged.
In whatever way recovery services are implemented, access and engagement over a longer duration of time than typical stints of addiction treatment can be crucial to help a person maintain remission and provide support when times get tough. Yet there is limited data on the optimal duration of recovery supports services, how the intensity or focus of services should change over the course of recovery, and, in the case of people taking medications for OUD, if and when medications can be safely discontinued. NIDA-funded recovery research is exploring the crucial question of optimal duration of medication treatment for people with OUD and developing discontinuation strategies for people who want to stop medication.
As we described in our New England Journal of Medicine commentary, the positive shift from punishing people experiencing addiction towards treating them in the clinic seen over the past four decades is now shifting into a new phase where the clinic is integrated with the community. The integration of support in the community is giving nonclinicians, including peers, friends, and family, an increasingly important role in the care of people with SUDs, facilitating the continuity of care beyond treatment. NIDA recently solicited applications for research projects on the role played by loved ones and other support persons in SUD recovery, with the goal of incorporating them into individuals’ recovery process as well as developing interventions to give support to those who are supporting a loved one in recovery.
As more addiction fires are extinguished through public health measures at the national, state, and community levels, we must direct more scientific attention to the end goal of long-term health and wellness for all people whose lives have been affected by addiction.
Source: https://nida.nih.gov/about-nida/noras-blog/2025/06/advancing-recovery-research
This book, and its review, engage with differing viewpoint s about addiction and addicts. Flanagan prefers to avoid the word ‘disease’ – characterising the condition as a behavioural ‘disorder’ – much in the way that Stanton Peele, in his classic 1975 text ‘Love and Addiction’ – (Peele and Brodsky – Pubd, Taplinger, New York) similarly views the condition. But in the professional field of today additional concepts have been introduced, what some might call ‘influencers’ – longest established is the notion of ‘harm reduction’ – this (in our opinion) has a valid purpose in limiting harm that users can experience, but it has also been ‘abused’ by campaigners who argue that ‘laws are harmful, so legalisation reduces harm’. More recently the notion of ‘stigma’ has become more prominent in the drug policy arena … and again, whilst there is a valid role for addressing gratuitous stigmatisation of users, the liberalising campaigners can be seen to abuse the notion, arguing that ‘all stigma is bad, therefore all stigma should be removed.’ In fact, society has long rationally deployed stigma where it can be seen as criticising an individuals drug abuse when this damages and jeopardises a healthful society, or threatens the health of people around the user … this is echoed in Flanagan’s text where, for example he says addicts are ‘… are by no means blameless just because they supposedly have a disease’. This dialogue will of course run and run, and NDPA will endeavour to maintain a balanced and rational journey through this jungle!
Owen Flanagan’s new book, What Is It Like To Be an Addict?, should be welcomed by anyone concerned with these issues. Despite its modest size, this is a work of large ambition and broad range informed not just by the author’s long career as a prominent philosopher but by his many years as a desperately addicted abuser of alcohol and sedatives.
“This is a deeply personal book,” he writes. “I was addicted to booze and benzos for twenty years on and off from the late 1970s until the early 2000s. The last years were especially ugly, requiring several hospitalizations, and involving constant self-loathing and suicidal despair.”
Unsurprisingly given his experience, Flanagan stresses that we should pay close attention to what the addicted have to tell us. And among the most important things addicts say is that they are by no means blameless just because they supposedly have a disease. On the contrary, many feel shame (for being an addict) and guilt (for behaviors that are slowly destroying them and harming their loved ones).
To Flanagan, these feelings are right and good. That stance may inspire horror from some people, who will see it as victim-blaming. But it’s consistent with Flanagan’s view that addicts can’t be reduced to flesh-and-blood automatons jerked about by their cravings. As he notes, even people who claim to believe this will then earnestly implore an addict to get help—a plea that could only be directed at someone presumed to have the ability to make choices. “Every treatment that works to unseat addiction,” he writes, “assumes that addicts are responsible and must participate in undoing their own addiction.”
Flanagan doesn’t even think addiction is a disease, exactly—more of a multifactorial disorder of enormous social, physical, psychological, and pharmacological complexity. Indeed, one of his book’s main points is that addiction cannot be seen as any one simple thing. But he doggedly insists that addicts retain some agency during their plight.
“Practices of compassion, forgiveness, and excusing are distinct from whether or not we hold the addict responsible,” he writes. “We hold addicts responsible in many respects and rightly so. Thus, the determination that addiction is a disease or mental disorder is much less consequential as far as holding addicts responsible goes than many suggest.”
Flanagan takes care to distinguish between unwilling addicts, willing addicts, and resigned addicts, helping us through these categories to think about what we mean by addiction and how best to mitigate it. Particularly notable are the minority who are willing addicts—he mentions as an example Keith Richards, who has said he was a longtime heroin user. At least some of these individuals are in control of the consequences of their habit and satisfied with their lives. Is their addiction any more meaningful than a coffee habit?
Unwilling addicts want to quit, and many will eventually succeed. And resigned addicts are those who wanted to quit, couldn’t, and just gave up, surrendering to hopelessness. They are in a sense beyond unwilling; by not trying to quit, they effectively acquiesce. Here, the author says, a kind of accommodation may help. One nonprofit in Europe helps resigned addicts to lead orderly lives through more disciplined consumption—in one methadone-like program, six pints of beer spread throughout the day—as well as suitable paid employment.
As for himself, the author credits Alcoholics Anonymous with saving his life by enabling his sobriety, but he also thinks it has a certain cultishness; like any good rationalist, he insists on “the distinction between the belief in a Higher Power having an effect and the Higher Power having an effect.”
Flanagan is also a capable researcher and reporter. Who knew that many addicts call the rest of us “earth people”? Or, more significantly, that there is so much overlap between addiction and other psychiatric disorders? “Twenty-five percent of individuals with severe mental illness, defined as a disorder that severely compromises normal functioning—schizophrenia with delusions or immobilizing depression—have a substance use disorder,” the author says. “In the other direction, 15 percent of individuals with a substance use disorder also have a severe mental illness.”
This book’s focus is substance abuse rather than, say, Facebook addiction, if such a thing exists. Flanagan is properly skeptical of the movement to medicalize all of life’s setbacks and sadnesses. He notes that men in most cultures are more likely than women to abuse alcohol and drugs, but that women are gaining. “There is no country where female alcoholism…rates are near 10 percent. But there are many countries in which the male alcoholism rate is above 10 percent and a few that top 13 percent: Russia (16.29 percent), Hungary (15.29 percent), Lithuania (13.35 percent), and South Korea (13.10 percent).”
He reminds us that while the war on drugs appears to be a costly failure, we can’t say for sure that many addictions wouldn’t be worse in its absence. And he notes some of the problems that have accompanied legalization initiatives. In Portugal, after a decade of good results, “substance use is on the rise, and fewer and fewer people in need are getting treatment. Recent data indicate that both overall drug use and drug overdose rates are up.” In Oregon, decriminalization Measure 110 “is being unwound” after evictions and fentanyl supplies surged. But he cautions: “The data do not mean, as some are quick to insist, that decriminalization, harm reduction, and treatment are not for the best.”
What Is It Like To Be an Addict? has its shortcomings, which largely stem from the author’s academic tribe. The book is not particularly well-organized or well-written; again and again, Flanagan tells us what he’s going to tell us, and then tells us the thing a couple more times to be on the safe side. And the book can be heavy on jargon. At one point, despite his professed sobriety, he writes: “When I report on the experiences of fellow addicts based on their autophenomenological reports, I am doing heterophenomenology.”
Particularly nettlesome is the author’s claim that, although addicts are responsible for their addiction, the rest of us are responsible too because of the woeful conditions we’ve allowed to persist. He wheels out the usual suspects including “social displacement,” poverty, inequality, racism, depression, “lack of good life options,” and other all-purpose woes that “are not caused by addicts.”
Blinkered by his ready-made list of villains, the author takes little account of other potential factors. Affluence in particular seems at least as likely a culprit as poverty. Today’s poor are often richer than middle-class Americans were in the middle of the last century, and today’s American middle class is extraordinarily affluent by historical and global standards. That means more of us can afford substance abuse of all kinds, not to mention addictions to shopping and other costly behaviors.
How about changes to family life or to levels of church attendance? Isn’t it possible that the religious and familial dimensions of A.A. are essential to its remarkable success? It’s noteworthy that the author’s own salvation came not from any arm of government but from a private, apolitical institution operating on a shoestring and making no attempt to end inequality or racism. Drunks come to A.A. and somehow get sober anyway.
But in truth, the author’s gestures toward collective responsibility feel more obligatory than emphatic. What he really wants is a humane, evidence-based approach to the problem of addiction consistent with individual agency, and that’s an approach fully in accord with a faith in human liberty. At the same time, we might as well recognize that voters will quickly lose their enthusiasm for legalizing drugs if they blame it for public chaos. Freedom always and everywhere relies on self-regulation.
These are tough times for individual agency. Many philosophers and psychologists scoff at the notion of free will, which others seem to regard as the sole province of the “privileged.” A therapeutic culture and the nanny state give us all incentives to see ourselves as victims, helpless in the face of implacable forces of oppression. It is refreshing to read a book that refuses to dehumanize addicts by depriving them of responsibility or delegitimizing the shame they feel for their actions.
Source: https://reason.com/2025/06/15/how-freedom-lovers-can-reckon-with-addicts-and-addiction/

Iran positions itself as a key partner for the SCO in tackling narcotics and boosting regional security.
Tehran, IRNA – Iran is prepared to become a regional hub for illicit drug prevention and treatment programs under the framework of the Shanghai Cooperation Organization (SCO), citing the country’s extensive experience and achievements in combating drug abuse, an official said.
Mohammad Narimani, head of the International Affairs Department of the Drug Control Headquarters, made the remarks on Sunday following his return from high-level SCO meetings in Xi’an, China.
“The SCO has strong structural capacities in the fight against drugs, but practical challenges still hinder its effectiveness,” Narimani said.
He stressed that the Islamic Republic has paid a heavy human and financial cost in the fight against drug trafficking and expects the SCO to use its political, security, and economic influence to assist Iran in that regard.
“This cooperation would not only benefit Iran but also contribute to the stability and security of the entire region,” he said.
Narimani added that Iran’s efforts to counter common threats such as terrorism, narcotics, and sanctions could strengthen the SCO’s standing as a powerful bloc in an increasingly multipolar world.
He also pointed to concrete areas where the SCO could support Iran, including identifying and dismantling drug trafficking and terrorist networks, pressuring the ruling Taliban to destroy heroin and methamphetamine production labs in Afghanistan, and facilitating Iran’s access to advanced border control equipment.
Source: https://en.irna.ir/news/85855787/Iran-seeks-to-become-regional-hub-for-drug-prevention-under

by Jessica Sherer B.A., Ashford University –
The “fenty fold” (also “fenty lean” or “fentanyl fold”) is a startling but common occurrence among regular users of fentanyl, and other illicit drugs like xylazine, where they are bent at the waist, slumped forward, in a rigid position. Their heads are bowed, their knees are bent, and they are often unable to respond or move.
While jarring to witness, the fenty fold has become a sad yet common phenomenon in cities like San Francisco and Baltimore, where fentanyl use has grown rampant alongside the growing nationwide trend. Chronic users of fentanyl can be stuck in this position for minutes to hours, with possible complications including decreased breath rate, poor circulation, and increased risk of falls and injuries.
Research has not yet pinpointed what exactly causes the fenty fold, as fentanyl use is not known to directly affect the spine. Instead, it’s becoming clear that it is a neuromuscular side effect of synthetic opioids like fentanyl. Studies from the Journal of Applied Physiology and the Harm Reduction Journal highlighted similar findings that fentanyl use can lead to severe and widespread muscle rigidity, particularly in the trunk muscles, which restricts respiration and affects posture and mobility.
Additionally, doctors and addiction professionals think the fold is also connected to the central nervous depression caused by opioids. After using fentanyl (usually in large amounts), people enter a state of slowed consciousness (nodding out), where their bodies and brains are functioning at a depressed level. This system depression leads to muscle weakness, which causes bending, and slowed thought processing, which inhibits the brain from instructing the body to stand upright, resulting in prolonged time spent in an unnatural position.
While more research is needed on the causes of fentanyl fold, it is clear that it is an uncomfortable and potentially dangerous side-effect of fentanyl use.
In the 2024 exposé on the fentanyl fold, the San Francisco Chronicle highlighted that many of the fentanyl users they interviewed were first introduced to the pain-numbing effects of opioids through prescription opioids. These people were prescribed opioids like oxycodone and hydrocodone for legitimate pain and turned to fentanyl when they could no longer obtain their prescriptions.
This is the story of many fentanyl users who become dependent on and develop a tolerance to opioids without realizing it until they are unable to get them. As they continue to seek a solution for their pain, fentanyl often fills the gap as a cheaper, easier-to-obtain alternative, leading to a cycle of addiction that supersedes most everything else in their life.
In 2024, videos started circulating on social media sites like X and TikTok of people experiencing the fold, often on urban streets, with tags of #fentyfold and #fentylean used. This exposure garnered both disdain and empathy as the real-life effects of fentanyl abuse were put on display.
Some videos of the fenty fold, often stripped of context, were met with ridicule and disdain for the people featured in the videos. However, public health officials and substance abuse professionals warn of the dehumanizing effects of social media and urge the general public to acknowledge it for what it is: a sobering reminder of the dangerous and debilitating effects of opioid addiction.
They further emphasize the need for harm reduction strategies and addiction treatment to help the growing problem of fentanyl abuse.
While more nationwide prevention efforts and reduction strategies are needed to combat the opioid epidemic, prevention can also start in the home. If you or a loved one is struggling with a fentanyl addiction, help is available. Inpatient treatment can provide you with a safe environment where you can detox and learn the tools necessary for a healthy recovery. Contact a treatment provider today to learn more and begin your healing journey.

The event was organised as part of ongoing community efforts to strengthen national belonging and reinforce Omani identity while addressing the dangers of drugs and psychotropic substances.
The seminar featured two main thematic discussions. The first segment addressed critical perspectives on the issue, examining the health consequences, legal implications, and religious rulings regarding drug abuse. The session began with an impactful theatrical performance by the Wahj Al Khayal team, illustrating the devastating effects of narcotics on individuals and society at large.
The second part of the seminar focused on identity and citizenship values. A working paper was presented about this theme that emphasised the fundamental role of national identity in building an aware and cohesive society capable of overcoming various challenges.
A highlight of the event was the official unveiling of the winning logo for Dhank’s Community Competition Team to Combat Drug Abuse. This initiative aims to enhance community awareness and support youth-driven projects in drug prevention efforts, reflecting the local commitment to addressing this critical social issue.
Source: https://timesofoman.com/article/158685-anti-drug-awareness-seminar-held-in-al-dhahirah

A new study reveals that a large number of American children are growing up in homes where at least one parent struggles with alcohol or drug use. This troubling environment may increase the chances that these children will face similar challenges later in life.
Using the latest available data from 2023, researchers estimate that 19 million children in the United States — that’s one in four kids under the age of 18 — live with a parent or caregiver who has a substance use disorder.
Even more concerning, around 6 million of these children are living in households where the adult also has a diagnosed mental illness along with their substance use disorder.
Alcohol is the most commonly misused substance among parents. The data suggests that about 12 million parents meet the criteria for some form of alcohol use disorder. Cannabis use disorder follows, affecting over 6 million parents. Additionally, approximately 3.4 million parents are struggling with the use of multiple substances at once.
The number living with a parent who had any substance use disorder in 2023 is higher than the 17 million estimated in a paper published just months ago that used data from 2020.
“The increase and fact that one in four children now live with parental substance use disorder brings more urgency to the need to help connect parents to effective treatments, expand early intervention resources for children, and reduce the risk that children will go on to develop substance use issues of their own,” said Sean Esteban McCabe, lead author of the new study and senior author of the recent one.
The new findings are published in the journal JAMA Pediatrics by a team from the University of Michigan Center for the Study of Drugs, Alcohol, Smoking, and Health, which McCabe directs. He is a professor in the U-M School of Nursing and Institute for Social Research, and a member of the U-M Institute for Healthcare Policy and Innovation.
Both studies used data from the National Survey on Drug Use and Health, a federal program that has tracked U.S. drug and alcohol use since the 1970s, yielding data that researchers and policymakers have used.
That survey faces an uncertain future due to staff and budget cuts at the federal agency where it’s based, the Substance Abuse and Mental Health Services Administration, or SAMHSA. The survey’s entire staff received layoff notices in April.
In addition to alcohol and cannabis, McCabe and his colleagues estimate that just over 2 million children live with a parent who has a substance use disorder related to prescription drugs, and just over half a million live with a parent whose use of illicit drugs such as cocaine, heroin and methamphetamine meets criteria for a substance use disorder.
The researchers include Vita McCabe, the director of University of Michigan Addiction Treatment Services in the Department of Psychiatry at Michigan Medicine, U-M’s academic medical center.
“We know that children raised in homes where adults have substance use issues are more likely to have adverse childhood experiences, to use alcohol and drugs earlier and more frequently, and to be diagnosed with mental health conditions of their own,” said Vita McCabe, a board-certified in addiction medicine and psychiatry. “That’s why it’s so important for parents to know that there is effective treatment available, including the medications naltrexone and/or acamprosate for alcohol use disorder, cognitive behavioral therapy for cannabis use disorder, and buprenorphine or methadone for opioid use disorder including both prescription and non-prescription opioids.”
Both the new paper and the one published in March in the Journal of Addiction Medicine based diagnoses of substance use disorders and major mental health conditions on the criteria contained in the Diagnostic and Statistical Manual of Mental Disorders 5, or DSM-5.
In the March study, the authors showed that the change in how substance use disorder was defined in DSM-5 compared with its previous version led to a major increase in the number of children estimated to be living with a parent with a substance use issue.
Ty Schepis, an addiction psychologist at Texas State University, was the lead author of the earlier paper and is senior author of the new paper.
“Our new findings add to the understanding of how many children are living with a parent who has a severe and comorbid substance use disorder and other mental illness such as major depression,” he said. “This is important to note because of the additional risk that this creates for children as they grow into adults.”
Source: https://scitechdaily.com/1-in-4-kids-lives-with-a-parent-battling-addiction-alarming-study-finds/

Substance use prevention targeting children and adolescents is a science that relies on evidence-based interventions to address the complex factors contributing to substance use disorders – Photo by Ernest Brillo on Unsplash
On Tuesday 12 May, the first session in a series of debates organized by G2H2 was opened. Entitled ‘People, power and policies in global health: perspectives from civil society’, the series was organized in the run-up to the 78th World Health Assembly, held from 19 to 27 May.
Co-hosted by Dianova and the Geneva Global Health Hub (G2H2) , the session ‘Growing up safe: public health approaches to drug use prevention and treatment for children and adolescents’ brought together high-level participants, including Anja Busse (WHO) and Wadih Maalouf, (UNODC).
G2H2 is a network of civil society organisations based in Geneva that promotes information exchange and joint political action on global health issues – Dianova International is a member of G2H2.
The main objective of the session, as outlined by Gisela Hansen (moderator, Dianova International), was to reconnect drug policies with public health, focusing on the prevention and treatment of substance use among children and adolescents. The aim was to promote models centred on health and human rights, especially in vulnerable or disadvantaged contexts around the world.
Head of the Unit on Drugs, Alcohol and Addictive Behaviours at the WHO. Anja has been involved in this field at the global level since 2005 and has been supporting science-based strategies for the treatment and care of drug dependence.
Anja took the floor and began by reminding the WHO’s commitment to promoting global health, particularly among the most vulnerable. The WHO Constitution (1946) emphasizes the importance of healthy child development: “Healthy development of the child is of basic importance, the ability to live harmoniously in a changing total environment is essential to such development.”
“A public health response to substance use prevention and treatment means reaching the highest number of people with the most effective, least costly, and least invasive strategy or intervention”
This involves creating environments in which children and adolescents can grow up healthy and safe, and where it is easier for them to avoid alcohol, tobacco and drugs. The burden of responsibility should primarily be placed on the system and on all of us rather than on the individual.

Safer is an initiative launched by the World Health Organization (WHO) in 2018, aiming to prevent and reduce alcohol-related harm in various countries – image: excerpt from presentation by Anja Busse, WHO
Globally, 22% of young people aged 15 to 19 consume alcohol, with significant regional differences demonstrating the fundamental role of our environment
UNODC data also reveal that, in 2021, around 5.3% of 15–16-year-olds had used cannabis in the previous year, and that, in most countries and regions, cannabis use is more prevalent among young people than in the general population.
Anja highlighted that the UNODC and the WHO have published several documents on the health and development of children and adolescents, as well as international standards on drug use prevention. These include strategies targeting the population as a whole, as well as those used in schools, the health system, the workplace, the community, and finally, families. She emphasised one of the basic principles of prevention: ‘The earlier we act, the better’, although it is never too late to implement interventions.
Science based strategies targeting the general population have the widest impact, but they must also consider implementing interventions for the most at-risk groups.

Children and adolescents face several obstacles when seeking mental health and drug services – image: excerpt from presentation by Anja Busse, WHO
According to Anja, the most effective strategies target multiple and multi-level vulnerabilities rather than limiting themselves to narrow interventions in single settings. Finally, Anja emphasised the need for well-conducted planning involving many stakeholders and for an effective social and health system providing accessible mental healthcare services at all levels, which is not the case everywhere.
While it is acceptable for a government to restrict or regulate the availability, distribution and production of drugs, it is important to avoid the unnecessary punishment of people who use drugs.
After reviewing various organizational prevention methods and their effectiveness, Anja also highlighted interventions that research has found to be ineffective or of questionable or unproven effectiveness. These include media awareness campaigns (not effective); use of social media and influencers (effectiveness unknown); information sessions on the consequences or harms of drugs (not effective); sports and other leisure activities (lack of evidence, controversies) strategies targeting children/youth particularly at risk (lack of evidence) and drug testing in schools (no evidence).
Oriol is a psychologist with over thirty years’ experience of helping people with addiction problems. He is the International Commissioner of the Proyecto Hombre association and coordinator of the Oviedo Declaration.
The impact of drugs, including tobacco and other legal substances, is enormous. This is not only an issue of security, economics or the law, but also a health issue affecting millions of people, including children and adolescents, in all aspects of their health: physical, emotional, intellectual and social.
We must invest in health now, while our children are healthy; otherwise, the future problem of substance use will be greater, not only for them, but for society as a whole – this is the paradox of prevention.

Some of the stakeholders involved in the Oviedo Declaration, following its presentation at the Commission for the Study of the Constitution (CND) in March 2024 – Photo: Proyecto Hombre, all rights reserved
This also presents a significant challenge to decision-makers and governments, as it necessitates planning and governance with a long-term vision. Launched last year, the Oviedo Initiative is a declaration comprising ten proposals in line with international standards on prevention. It is also a global mobilisation to incorporate prevention into drug policies once and for all. It is an inclusive, collective campaign that is already supported by over 3,000 institutions and several observers, including the UNODC.
The main strength of this initiative, which builds bridges between local and global levels, lies in the voluntary work of 174 focal points within countries. At Dianova International, we are honoured to contribute to this initiative as the focal point for Switzerland.
We hope that the resolution on prevention recently adopted by the CND in Vienna last March will mark a turning point towards the accelerated implementation of effective and forward-looking drug prevention policies.
As a public health expert and the Yemen focal point for the Oviedo Initiative, Shrooq works for the Yemeni NGO, the Psychiatric Care Developmental Foundation, providing mental health and psychological support services to vulnerable young people.
She points out that, after ten years of conflict, Yemen is facing one of the world’s worst humanitarian crises, exacerbated by ongoing violence, the consequences of climate change and the collapse of the economy, institutions and services. According to the 2024 Humanitarian Needs Assessment, approximately half of Yemen’s population, or more than 18 million people, require humanitarian assistance.
Research has shown that populations affected by armed conflict are at a higher risk of using drugs as a coping mechanism in response to such dramatic situations.
Furthermore, factors such as prolonged psychological trauma, disrupted education, unemployment and chronic poverty in Yemen further increase the risks. Despite this, mental health and substance use issues remain highly neglected. Therefore, ensuring adequate care for substance use issues in humanitarian contexts is a priority.
As the focal point for the Oviedo Declaration in Yemen, Shrook and her colleagues face significant challenges in advancing the initiative within government structures due to the many divisions between the government recognised by international institutions in the south and the de facto authorities in the north. This means that all activities must be coordinated with different entities, which is made more difficult by the sensitive nature of the issue.
Yemen lacks reliable data on substance use. As one of the Oviedo Declaration’s recommendations highlights, there is a need to focus on evidence-based strategies grounded in the collection and evaluation of data. This data would serve as a basis for implementing prevention programmes and national policies in this area.
Problems associated with substance use exist in Yemen and can no longer be ignored or denied.
Following the tragic loss of her son, Karim, in 2015, Cristina established the Karim Khan Afridi Welfare Foundation (KKAWF) to support young people and raise awareness of addiction. The foundation’s work is based on five pillars: drug awareness, sport, the environment, art and culture, and civic engagement.
Currently in Pakistan And across the region Drug use prevention strategies are significantly underrepresented In public policies agendas. The Oviedo declaration launched in 2024 represents a timely and powerful call to action urging nations to prioritize prevention in the drug policies For Pakistan this framework offers a critical opportunity to redirect focus towards long-term sustainable solutions.
Cristina emphasised the urgency of the situation: Pakistan lies at the heart of the Golden Crescent, one of the world’s most notorious drug producing region. Of all the countries in the region, Pakistan is the most affected by the drug menace. It harbors the largest heroin consuming population in the region, a crisis now compounded by the rise of crystal meth.
Drug use among young people poses a particular risk to democracy in Pakistan, a country with a population of around 250 million, 154 million of whom are under the age of 30. This massive young population is the country’s greatest asset and potential, but also its greatest vulnerability.
The growing threat of drug use among young people poses considerable social, health, and economic challenges for the nation. The KKAWF Foundation plays an active role in preventing drug use. It raises awareness among policymakers, civil society and other stakeholders of the importance of prevention.
Prevention must become the central pillar of national drug policies, but this requires essential resources, coordination and commitment — and urgently so!
The KKAWF develops numerous partnerships in its advocacy work for prevention. Here, the Foundation’s president, Cristina Von Sperling Afridi (right), with a representative of the Green Crescent Federation – Photo: KKAWF, all rights reserved
One of the Foundation’s main areas of focus is fostering collaboration between the government, civil society organisations, and the private sector, as only a unified, strategic approach can effectively address this public health crisis. It is also crucial to integrate drug education into school curricula at secondary and higher education levels.
The KKAWF advocates an evidence-based, stigma-free approach that promotes emotional intelligence, resilience, and critical thinking.
Cristina believes that prevention must become a way of life, not just a programme. She believes that only by cultivating a culture of prevention will it be possible to protect future generations.
Rajesh is the executive director of SPYM, an NGO that has worked in the field of addiction for over 40 years, receiving several national awards for its work with marginalised communities. SPYM has consultative status with ECOSOC, and Dr Kumar has served on numerous government and international bodies.
India’s proximity to the Golden Crescent and Golden Triangle has made the country a destination for large quantities of drugs. Substance use is therefore on the rise, particularly among children. In response to this serious violation of children’s rights, SPYM began working with children suffering from addiction in 2010.
In India, approximately 4 million children use opiates, 2.6 million inhale drugs, and 2 million use cannabis. Even with a population of over 1.4 billion, these figures represent a huge problem, particularly given that only 1% of affected children seek help.
While it is estimated that 99.9% of children do not use drugs, it is essential to invest in treatment and scientifically validated prevention strategies based on collaboration with families, communities and schools to ensure they stay on this path. These groups have a duty to ensure that substance use prevention and mental health are part of their regular activities, which is why SPYM has developed the Navchetna programme under the auspices of the Ministry of Social Justice and Empowerment.
The Navchetna school programme is designed with different modules tailored to students according to their age. It is run by trained teachers under the supervision of the Ministry of Education.
A significant part of SPYM’s work is carried out for the benefit of the well-being of the most disadvantaged children and adolescents – Photo: SPYM, all rights reserved
Once their training is complete, the ‘master trainers’ must in turn train up to 100 teachers within two years, with the ultimate goal of training one million teachers, although so far, only 100,000 have been trained. The programme also uses videos, which are currently available in English and Hindi and will soon be available in 12 regional languages.
SPYM also develops numerous programmes and activities to help vulnerable people, particularly children and teenagers. These include a community-based early intervention programme run by peers in nearly 300 districts in the country most affected by drug use, residential treatment centres for various populations including children and adolescents in conflict with the law, activities focused on life skills and rehabilitation, and advocacy activities.
SPYM and KKAWF are both associate members of Dianova International.
Cressida is the project coordinator and communications manager for the WFAD. She leads projects for this organisation in various countries, including the Democratic Republic of Congo, Kenya, India, and Georgia. She is also a member of the WFAD committees on gender and youth.
The continuum of care includes a wide range of interventions, from health promotion to recovery and follow-up, including various prevention strategies and different phases or modalities of treatment.

The Continuum of Care in addiction treatment refers to a comprehensive approach that guides and tracks patients over time through various levels and intensities of care – Image: excerpt from presentation by Cressida de Witte
Although prevention programmes for young people generally target school-age children, adolescents and young adults due to the high risk of experimenting with substances, research has shown that prevention efforts should start even earlier.
The early years of a child’s life are a critical period for brain development. This is when the foundations of decision-making, impulse control and resilience are laid. As younger children learn to manage their emotions, resolve conflicts and set goals, they develop skills that will inform healthier choices in adolescence and adulthood.
However, prevention is not solely the responsibility of the child; it also depends on their environment, which is why action must be taken at all levels, from the macro to the micro, and from family dynamics to community support.
The WFAD is a multilateral community with ECOSOC consultative status, composed of over 470 NGOs in 73 countries. The organisation’s three pillars are capacity building through webinars, training courses and forums; advocacy at national, regional and international levels to strengthen prevention, treatment and recovery; and project development, particularly international projects. One such project is a youth project in the Democratic Republic of Congo: Sober Youth and Healthy Communities: Transforming Violent Youth in Kinshasa. Learn more about the project.
Within the framework of these advocacy efforts, the organisation launched the ‘Global Youth Declaration on Prevention, Treatment and Recovery’. Presented at the 68th session of the CND in March 2025, the declaration is based on six recommendations aimed at ‘ensuring access to prevention, treatment, rehabilitation and recovery services that are youth-friendly and respectful of their rights, in order to ensure a healthy, safe and drug-free future for all young people worldwide’. The declaration is available in seven languages.
Rebecca is a public health sociologist and associate professor at the University of Calgary. Her research interests include youth drug use, harm reduction approaches, and drug policy reform.
As a teenager, she was cast in a popular Canadian television programme in which her character experimented with substance use. This, in some way, launched her career and her commitment to supporting young people she said.
Rebecca believes that we need to radically rethink drug prevention for young people. Unfortunately, in North America as elsewhere, prevention has long been based on values rather than scientifically validated evidence of what works and what doesn’t. Past prevention campaigns, such as Nancy Reagan’s ‘Just Say No’ motto, were never evidence-based or evaluated.
“Prevention has been based on values rather than evidence for too long, which is why we need to radically rethink drug prevention for young people” – excerpt from presentation by Rebecca Haines-Saah
Even worse, an evaluation of the D.A.R.E. (Drug Abuse Resistance Education) programme – a series of lessons delivered by police officers in schools – showed that it was associated with a slight increase in substance use! It was hypothesised that the most marginalised young people reacted badly to the presence of police officers in the classroom. These campaigns primarily relied on stereotypes and stigmatisation of young people.
“In Canada, it has been highlighted that the most effective drug prevention programmes have very little to do with drugs”
If we want to improve prevention outcomes among young people, she stresses, we need to focus less on educating them about specific substances, and instead strive to promote community well-being, as well as individual and family resilience. That’s where we need to invest.
Scientific research indicates that effective strategies include psychosocial and developmental interventions that enhance conflict resolution and problem-solving abilities, social-emotional learning, and anything else that helps teenagers manage challenging situations with their peers and cope with trauma and community conflict. These strategies have demonstrated several positive long-term outcomes.
Rebecca also highlighted the implementation of a community-based prevention model in Calgary and other parts of the country. Planet Youth, the model implemented in Calgary and elsewhere, was developed based on the Icelandic prevention model: a participatory, evidence-based approach that has dramatically reduced substance use, particularly tobacco and alcohol.
Finally, Rebecca presented a slide on the ‘prevention pyramid’, particularly focusing on the first level: the more effort made to create equitable social and economic conditions, the better the results. She believes that this is a much more ambitious and difficult goal to achieve than simply setting up a programme or activity. However, it is on this point that our vision must be aligned.
The more effort that is made to create equitable social and economic conditions in prevention, the better the results.
In addition to prevention needs, Rebecca emphasised the urgent need to address young people’s harm reduction needs to prevent drug poisoning deaths. Drug poisoning is currently the leading cause of death among 10- to 18-year-olds in western Canada, ahead of cancer and car accidents, so this is a public health emergency.
Wadih is a public health professional who holds a PhD in mental health and drug epidemiology from the Johns Hopkins School of Public Health. With over 25 years’ experience, he is now the global coordinator of the addiction prevention programme at UNODC, and is one of the world’s leading prevention experts.
Wadih began by emphasising the importance and timeliness of this conversation because it is based on scientific evidence. A large number of standards have now been developed for prevention and treatment, thanks to collaboration between UNODC and WHO, and the science is available. He also noted that science is receiving greater recognition, not only from organisations working in the field, but also from civil society. This is evident in the 3,000 stakeholders who have rallied around the common agenda promoted by the Oviedo Declaration.
This recognition is also evident at government level, as demonstrated by the Commission on Narcotic Drugs’ resolutions, which call for early prevention to target different stages of development rather than drug use. These resolutions also call for multisectoral prevention, despite all the challenges posed by multilateralism.
There is now a desire to develop science-based, multisectoral prevention programmes for young people.
In his view, there is a real desire to prioritise science and prevention, particularly for young people, and to work across multiple sectors. With the right ingredients — science, political commitment, and action on the ground — it is possible to turn this knowledge into action.
As a people-centred approach, prevention must also focus on the environment and context in which people live, as well as their level of vulnerability. This systemic approach must aim to leave no one behind.
To achieve this, we must focus on different age groups, contexts of vulnerability and gender. This is an important consideration in the context of vulnerabilities, particularly for children, whose developmental trajectories may be affected in different ways.
The current generation of young people has the highest potential ever seen, which is why it is essential that they are meaningfully engaged in prevention efforts.
Young people are not only the beneficiaries of prevention; they must also be its agents because every child has the right to grow up healthy, and we have the means to make that happen.
| From sfunes@drugfreeamericafoundation.ccsend.com – 16 May 2025 |
|
Breaking down these silos requires intentional structural changes. Joint task forces that bring together representatives from various agencies can facilitate information sharing and collective problem-solving. These coalitions should include representatives from public health departments, hospitals, mental health services, law enforcement, schools, community organizations, and recovery support services.
Regular interagency meetings allow stakeholders to share data, identify trends, and develop coordinated strategies. Shared databases and information systems enable real-time communication about emerging threats and available resources, while protecting client privacy through appropriate safeguards.
Collaborative Prevention Strategies
Prevention represents the most cost-effective approach to reducing substance use. When agencies collaborate on prevention initiatives, they can leverage their collective expertise and resources to maximize impact.
Schools can partner with public health departments and law enforcement to implement evidence-based prevention curricula. Community-based organizations can work with healthcare providers to identify and support at-risk youth. Faith communities can collaborate with social services to offer supportive environments and positive activities for young people.
Prevention efforts should address not only the risks of substance use but also underlying factors such as trauma, mental health issues, poverty, and social isolation. This holistic approach requires input from diverse agencies with expertise in these various domains.
Creating Seamless Pathways to Treatment
When someone seeks help for substance use, they often encounter a confusing maze of services spread across different agencies. Collaborative approaches can create more seamless pathways to appropriate care.
One successful model involves establishing centralized assessment and referral systems where individuals can receive comprehensive evaluations and be connected to appropriate services based on their specific needs. These “no wrong door” approaches ensure that regardless of which agency someone initially contacts, they can be guided to the full spectrum of available resources.
A Residential Treatment Center for Youth offers a critical component within this continuum of care. These specialized facilities provide structured environments where young people can receive intensive therapeutic interventions away from environments that may contribute to substance use. When integrated into a broader system of coordinated care, residential treatment centers can work closely with schools, juvenile justice systems, and community-based services to ensure smooth transitions and ongoing support for youth and their families.
Shared Funding and Resource Allocation
Limited resources often create competition between agencies addressing substance use. Collaborative approaches can help overcome this challenge through shared funding mechanisms and strategic resource allocation.
Pooled funding models allow agencies to combine resources for greater impact. Joint grant applications can access funding streams that might be unavailable to individual organizations. Cost-sharing arrangements for shared staff positions or facilities can extend limited budgets.
Some communities have established dedicated funding streams for substance use initiatives through tax measures or fees. These resources can be allocated through collaborative decision-making processes that ensure they address community priorities and gaps in services.
Data Sharing and Outcome Measurement
Effective collaboration requires shared data systems and agreed-upon outcome measures. When agencies use different metrics to evaluate success, it becomes difficult to assess the collective impact of their efforts.
Communities that have made progress in addressing substance use typically establish common data elements that all participating agencies collect and report. These might include measures of substance use prevalence, treatment access and completion, overdose rates, related criminal justice involvement, and social indicators such as employment and housing stability.
Regular analysis of this shared data allows partners to identify trends, evaluate the effectiveness of interventions, and make evidence-based adjustments to strategies. This approach transforms the collaborative from a mere networking group into a data-driven learning community.
Overcoming Barriers to Collaboration
Despite its benefits, interagency collaboration faces significant challenges. Differing organizational cultures, competing priorities, confidentiality concerns, and turf issues can impede cooperative efforts.
Successful collaborative address these barriers through formal agreements that clarify roles, responsibilities, and information-sharing protocols. Regular relationship-building activities help develop trust between partners. Training on confidentiality laws and regulations ensures that information can be shared appropriately while protecting client privacy.
Leadership commitment from the highest levels of participating organizations is essential to overcoming institutional resistance. When agency heads model collaborative behavior and allocate resources to support cooperative efforts, staff at all levels are more likely to embrace the approach.
Community Engagement as a Unifying Force
Community members, particularly those with lived experience of substance use, bring valuable perspectives to collaborative efforts. Their involvement can help ensure that strategies are culturally appropriate, respectful, and responsive to community needs.
Recovery community organizations, family support groups, and neighborhood coalitions should be equal partners in planning and implementing interagency initiatives. Their participation helps build public trust and ensures that services address the actual barriers and needs experienced by those seeking help.
Final Word
The fight against drug use requires the coordinated efforts of multiple agencies working together toward common goals. By breaking down silos, sharing resources, creating seamless pathways to care, and engaging the community, these collaborative can address substance use more effectively than any single agency working alone.
The most successful models recognize that substance use is influenced by complex biological, psychological, and social factors that cross traditional agency boundaries. Only through true collaboration can communities provide the comprehensive response needed to prevent drug use, support recovery, and promote health and wellbeing for all residents.
While challenges to collaboration exist, communities across the country have demonstrated that with commitment, creativity, and persistence, agencies can work together effectively to reduce the impact of substance use and build healthier communities for all.
Source: https://dailytrust.com/how-agencies-can-come-together-in-the-fight-against-drug-use/

by Lisa Ryckman – NCSL’s associate director of communications. (National Conference of State Legislatures)
Somewhere in America right now, a teenager searches the internet for drugs. The pills they buy might look like the real thing—Xanax, maybe, or Adderall—but chances are, they’re not getting what they think they are.
The U.S. Drug Enforcement Administration estimates that six out of 10 pills bought online actually might contain lethal doses of the opioid fentanyl, says Rahul Gupta, director of the Office of National Drug Control Policy.
“So, the odds of dying from those pills is worse than playing Russian roulette with your life,” he told a session at the 2023 NCSL Legislative Summit.
“Substance use cuts across every geographic boundary, every sociocultural boundary. It doesn’t matter what race you are, how rich or poor you are, where you live.”
—Rahul Gupta, Office of National Drug Control Policy
More than 110,000 Americans died from drug overdoses in 2022, Gupta says.
“Substance use cuts across every geographic boundary, every sociocultural boundary. It doesn’t matter what race you are, how rich or poor you are, where you live,” he says. “It’s got your number.”
An iteration known as “tranq dope”—a potent cocktail of fentanyl, heroin and the animal tranquilizer xylazine—is the latest scourge to hit the streets, Gupta says. It is particularly problematic because the xylazine tends to increase the effect of the other drugs.
The costs of opioid addiction and trafficking fall mostly on the states: an economic loss of $1.5 trillion in 2020 alone, Gupta says. He outlines a two-pronged federal approach that includes treating addiction and disrupting drug trafficking profits. Making the drug naloxone, which can reverse an overdose, available over the counter has been a game-changer, he says, as have efforts to disrupt the fentanyl supply chain—chemicals from China, production in Mexico and sales in the U.S.
“We’re going after every choke point in this supply chain,” Gupta says, “and we’re putting sanctions on all of these folks to make sure that we’re choking off those important points the cartels and others depend on to create this deadly substance that kills Americans.”
In Oklahoma, fentanyl overdose deaths increased sixfold from 2019 to 2021, and fentanyl was involved in nearly three out of four opioid-related deaths, compared with 10%-20% in previous years, says state Sen. John Haste, vice chair of the Health and Human Services Committee.
The Legislature focused on prevention and treatment by expanding access to naloxone, including requiring hospitals and prisons to provide it to at-risk patients and inmates upon release, he says. Telehealth can now be used for medication-assisted treatment, and fentanyl test strips have been legalized, Haste says.
The state Department of Mental Health and Substance Abuse has launched a campaign to reduce the number of accidental overdoses through education awareness and resource access, he says. As part of the campaign, the department is placing more than 40 vending machines in targeted areas that freely dispense naloxone and fentanyl test strips. “This is the largest program of its kind in the country,” Haste says. “All around Oklahoma, you can see messages reminding the public to utilize test strips and naloxone on billboards, buses, local businesses and other strategic locations.”
In Hawaii, legislators are looking at safe alternatives to opioids for pain relief.
“It’s easy to say, just stop opioids, stop all drugs,” says Rep. John Mizuno, chair of the Hawaii House Committee on Human Services. “We know that chronic pain is complex; in addition to pain, you’ve got mental health. We need to think about the person’s quality of life. We’ve got to balance the patient’s right to manage his or her pain.”
Mizuno suggests that legislators meet with their state’s top pain management physician to learn about safe pain alternatives, including nerve blocks, implanted medication pumps, physical therapy, acupuncture, massage therapy, chiropractic treatment and medical cannabis.
His state has asked that Medicaid expand coverage for native Hawaiian healing that previously has been covered only for tribal members.
Mizuno says coverage is the main barrier to safer treatments, many of which might not be paid for under private health insurance or federal programs.
“But the best thing to do is work with your colleagues, work with your medical providers, and try to get these safe alternatives (covered),” Mizuno says. “It’s a lot better than being addicted to opioids.”
Source: https://www.ncsl.org/events/details/states-and-feds-are-partners-in-fight-against-opioid-epidemic
Scott Strode and his company have an active take on recovery and sobriety.
Wall Street Journal Andy Kessler March 23, 2025
It wasn’t hard to find Scott Strode when we first met. He was the big guy in a black T-shirt with the word “SOBER” splashed across it. Mr. Strode is founder of the Phoenix, a national “sober active” community. Addiction statistics in the U.S. are sobering. According to Mr. Strode’s book, “Rise. Recover. Thrive,” one-third of Americans have substance-abuse issues or mental disorders.
When drinking, Mr. Strode felt valued. “People wanted to spend time with me. And I found community,” he says. “It’s just what we were building it around wasn’t healthy.” Alcohol. Cocaine. Dependency. Until one night he finally hit bottom. “I couldn’t imagine someone having to tell my mom this is how I died.”
The road to sobriety wasn’t easy for Mr. Strode, but he found solace in physical challenges. “I saw a poster for ice climbing,” he said. “It gave me something to strive for, and that led me into the boxing gym and triathlons and racing Iron Mans.” But it wasn’t enough. “I realized when I took other people with me, I felt lifted in a different way.”
I wasn’t sure what he meant. “Getting into recovery is like getting out of a burning building,” he said. “But there are other people in there, so you have to reach back in to help get them out. By using my passion to help others, it filled a void. That was really what the Phoenix was born from.”
The Phoenix Multisport active recovery community, its original name, started in Boulder, Colo., roughly 20 years ago. It was funded by friends and a few grants—no fees. Others might have been content with helping one community. Not Mr. Strode. After a few years, he started helping active-duty service members and many others in Colorado Springs and set up a location in Denver.
What’s the magic? “Your life gets so much bigger, and you start to realize what’s possible. You connect somewhere where you feel valued, accepted and loved.” Climbing. Hiking. Running. Yoga. A fellow rider and Phoenix member, Ben Cort, told him, “I got sober because I didn’t want to die. I stayed sober because I wanted to live.”
A mother who heard about the Phoenix approached Mr. Strode and offered him $200,000 to expand to San Diego to help her son. Sadly, her son passed away before they could get there, but the idea of scaling to other communities kicked in for Mr. Strode. Maybe people’s desire to help others could be leveraged and help the Phoenix scale. “We opened up this opportunity on our website for folks to raise their hand to become volunteers,” Mr. Strode said. “We thought we’d get a few. We got 700.” Over the next 10 years, they were in 28 locations.
In 2016 the Phoenix received some funding from the philanthropic organization Stand Together. One of their pillars is to help solve addiction. They discussed scaling, and Mr. Strode told them that for each location, “it starts with a man and a bike.” In January 2020 they mutually agreed on $50 million in funding with a goal of “serving one million people impacted by substance use” in five years. A stretch, for sure. But it had to go from push to pull—“stimulating volunteers in places where we can’t reach.”
What started in Boulder with a deal with CrossFit is now in every state—almost 200 communities with more than 5,000 volunteers. “We have served over 800,000 since Phoenix started.” It scales because it works—83% of Phoenix participants stay sober after three months, compared with an average of 40% to 60% from other programs.
That’s the power of volunteers. And technology. The Phoenix has a mobile app called NewForm. Anyone can have a profile. The Phoenix isn’t in your community? Start one yourself. The app links to other nonprofits, such as SeekHealing, that help people overcoming trauma, a potential cause of addiction. The Phoenix also sets up sober supportive spaces at concerts and festivals—the app can reveal “thousands of other sober people in those spaces.”
“We distribute tablets in prisons across the country, so you can come to Phoenix virtually,” Mr. Strode says. “We joke that we’re the sober Peloton in prisons.” Smart. Plus, “you don’t have to turn to those old cellphone numbers in your phone when you return home. You can actually find new connections and community to help support you on your healing journey.”
What about other addiction programs? “At the Phoenix, we’re really focused on helping people with what’s possible in their recovery. So it’s very forward-looking. We start to dream of what’s possible in our sober life. In the 12-step community, people often identify as their disease. ‘I’m Scott, I’m an addict, I’m an alcoholic.’ But I always say, ‘I’m Scott, I’m in recovery, I’m an ice climber and so much more.’ We see everybody for their intrinsic strength, not a problem to be fixed.”
The Phoenix should hit its goal of one million people helped later this year. I’m convinced after talking to Mr. Strode that 10 million is a reachable goal.
Source: https://www.wsj.com/opinion/a-new-approach-to-addiction-phoenix-fitness-community-mental-health-a3591f99
The details: A model for evaluating treatments based on reduced use instead of abstinence exists with alcohol use disorder (AUD) and is in the works for smoking.
But:
Why it’s important:
From NIHCM Newsletter / April 2025

Learn about the latest news on substance use, including views on alcohol, and how fentanyl deaths are declining.
Resources & Initiatives
Source: https://nihcm.org/newsletter/the-relationship-between-alcohol-and-health
National Crime Agency exposes increasing ketamine use in England amid surge in ‘drug cocktails’
by Tony Diver, Associate Political Editor, The Telegraph (London) 21 February 2025
Drug use in England
Ketamine
2023: 10,600 kilograms consumed
2024: 24,800 kilograms consumed
Hotspots: Norwich, Liverpool and Wakefield
Street value: Unknown
Cocaine
2023: 87,600 kilograms consumed
2024: 96,000 kilograms consumed
Hotspots: Liverpool and Newcastle
Street value: £7.7 billion
Heroin
2023: 25,300 kilograms consumed
2024: 22,400 kilograms consumed
Hotspots: Liverpool and Birmingham
Street value: £1.1 billion
Ketamine usage more than doubled in England last year amid the rising popularity of designer “drug cocktails”, The Telegraph can reveal.
The largest and most accurate study of its kind, conducted on behalf of the National Crime Agency (NCA), has exposed a dramatic rise in the popularity of the drug.
Almost 25 tonnes of ketamine were consumed in England last year, up from 10.6 tonnes in 2023.
The drug is now more popular than heroin, with the worst hotspots in Norwich, Liverpool, and Wakefield.
The findings are revealed in Home Office data, seen by The Telegraph, which will form part of the NCA’s annual threat assessment next week.
The agency, dubbed Britain’s FBI, will warn of a rise in the use of several recreational drugs in Britain, including a 10 per cent increase in cocaine.
The sharp increase in the prevalence of ketamine on Britain’s streets is thought to be driven by drug cocktails, including “pink cocaine” – a combination of ketamine and other substances taken by Liam Payne, the One Direction star, before his death last year.
Payne, who fell to his death from a hotel balcony in Argentina in October last year, had taken a mixture of methamphetamine, ketamine and MDMA along with crack cocaine and benzodiazepine before he died, a toxicology report found.
Liam Payne reportedly had ‘pink cocaine’ along with other drugs in his system when he fell to his death in Buenos Aires Credit: Marc Piasecki/GC Images
Mixing ketamine and other drugs can produce hallucinogenic effects, but presents a greater risk to partygoers because the substances can be laced with even stronger narcotics including fentanyl.
The Home Office sampled wastewater from 18 treatment plants across England and Scotland over three years to build the most accurate picture of drug consumption in Britain ever compiled.
The samples, which covered wastewater from more than a quarter of the population, were analysed and scaled up by scientists from Imperial College London.
Previous estimates were based on the quantity of drugs seized by police and self-reported drug surveys, which are less accurate.
The final report found that almost 100 tonnes of cocaine were consumed in England alone last year, up from 88 tonnes in 2023.
Liverpool and Newcastle were the heaviest consumers of cocaine. Usage peaked in London during Christmas, the Euro 2024 football tournament and the Eurovision song contest.
Adjusted for purity, quantities of cocaine consumed in England last year had an estimated street value of £7.7 billion.
That figure is almost double the NCA’s previous estimate and the equivalent of £100 spent on cocaine each year by every person in the country.
Over the same period, heroin consumption is estimated to have decreased by 11 per cent, from 25,300 kilograms in 2023 to 22,400 kilograms in 2024. The highest rates were measured in wastewater from Liverpool and Birmingham.
Experts have previously warned of the dangers of trendy designer drug cocktails, including pink cocaine and “Calvin Klein” or “CK”, which refers to a mixture of cocaine and ketamine.
The combination of drugs can make it more difficult for users to know what substances they have taken.
CK, which is growing in popularity in the UK, has been blamed for overdoses among young people in nightclubs.
It comes as in this week’s Crime and Policing Bill, the Government will propose banning “cuckooing” – when criminals seize a vulnerable person’s home and use it as a drug den or for other illegal activity.
The Home Secretary will also propose new measures to jail those convicted of using children for crime Credit: Jacob King
Yvette Cooper, the Home Secretary, will also propose a new offence of child criminal exploitation, which is thought to affect around 14,500 children each year.
Under the new measures, people convicted of using children for crime, including county lines drug dealing, will face ten years in prison.
Ms Cooper said: “The exploitation of children and vulnerable people for criminal gain is sickening and it is vital we do everything in our power to eradicate it from our streets.
“As part of our Plan for Change, we are introducing these two offences to properly punish those who prey on them, ensure victims are properly protected and prevent these often-hidden crimes from occurring in the first place.
“These steps are vital in our efforts to stop the grooming and exploitation of children into criminal gangs, deliver on our pledge to halve knife crime in the next decade and work towards our overall mission to make our streets safer.”
Ministers and the NCA are also concerned about the rise of drug importers, who bring classified substances into the UK through weaker entry points and sell them to distributors around the country.
Source: https://www.telegraph.co.uk/news/2025/02/21/true-scale-uk-illegal-drug-use/
Visual

PLOS ONE | https://doi.org/10.1371/journal.pone.0317036 March 7, 2025 1 / 24
Citation: Onohuean H, Oosthuizen F (2025)
1 Biopharmaceutics Unit, Department of Pharmacology and Toxicology, Kampala International University
Western Campus, Ishaka-Bushenyi, Uganda, 2 Discipline of Pharmaceutical Sciences, School of Health
Sciences, Westville Campus, University of KwaZulu-Natal, Durban, South Africa
* onohuean@gmail.com
Abstract
Introduction
There is an ongoing global upsurge of opioid misuse, fatal overdose and other related
disorders, significantly affecting the African continent, due to resource-limited settings and
poor epidemiological surveillance systems. This scoping review maps scientific evidence
on epidemiological data on unlawful opioid use to identify knowledge gaps and policy
shortcomings.
Method
The databases (PubMed, Scopus, Web of Sciences) and references were searched
guided by Population, Concept, and Context (PCC) and PRISMA-ScR. The extracted
characteristics examined were author/year, African country, epidemiological distribution,
age group (year), gender, study design and setting, common opioid/s abused, sources of
drugs, reasons for misuse, summary outcomes and future engagement.
Results
A population of 55132 participated in the included studies of 68 articles, with the
largest sample size of 17260 (31.31%) in a study done in South Africa, 11281(20.46%)
in a study from Egypt and 4068 (7.38%) in a study from Ethiopia. The gender of the
participants was indicated in 65(95.59%) papers. The mean and median age reported
in 57(83.82%) papers were 15.9-38, and 22-31years. The majority of study-designs
were cross-sectional, 44(64.71%), and the most used opioids were heroin, 14articles
(20.59%), tramadol, 8articles (11.76%), and tramadol & heroin, 6 articles (8.82%)
articles. Study-settings included urban community 15(22.06%), hospital 15(22.06%),
university students 11(16.18%), and secondary school learners 6(8.82%). The highest
epidemiological distributions were recorded in the South African study, 19615(35.60%),
Egyptian study, 14627(26.54%), and Nigerian study 5895(10.70%). Nine (13.24%)
papers reported major opioid sources as black market, friends, and drug dealers. To
relieve stress, physical pain and premature ejaculation, improve mood and sleep-related
PLOS ONE | https://doi.org/10.1371/journal.pone.0317036 March 7, 2025 2 / 24
PLOS ONE The burden of unlawful use of opioid and associated epidemiological characteristics in Africa
problems and help to continue work, were the major reasons for taking these drugs as
reported in twenty articles (29.41%).
Conclusion
The findings of this scoping review show significant knowledge gaps on opioid usage in
the African continent. The epidemiological distribution of unlawful use of opioids among
young adults, drivers, and manual labourers in both genders is evident in the findings.
The reason for use necessity scrutinises the role of social interaction, friends and family
influence on illicit opiate use. Therefore, there is a need for regular epidemiological
surveillance and investigations into multilevel, value-based, comprehensive, and strategic
long-term intervention plans to curb the opioid problem in the region.
Introduction
Opiate use disorders and overdoses are an emerging global health concern. Both prescriptions
and non-clinical indications contribute to the escalating global opioid use disorder
problem (OUD). The opioid crisis has metamorphosed through the Use of: methadone in
1999, heroin in 2010, and the current wave of a combination of heroin, counterfeit pills,
and cocaine [1–8]. An estimated 62 million people globally used opioids in 2019, and
36.3 million were impacted by its associated problems [9]. In the US estimated use has
increased from 70029 in 2020 to 80816 in 2021 [10], and in Canada, 7560 opioid-related
fatalities occurred in 2021 [11]. In Italy opioid addiction affects more than five people per
1000 [12], while a regional study in Germany conducted amongst 57 million adults, found
opioid prescription prevalence of 38.7 or 12.8/1000 persons of low- and high-potency
opioids in 2020 [13]. However, little is known about the epidemiological characteristics in
Sub-Saharan Africa.
There are reports of opioid abuse, although not specifically on opioid fatal overdose or
its related disorders, in some African countries, including Egypt, Nigeria, Kenya, Tanzania,
and South Africa [14–24]. Some of these studies report the increasing use of tramadol
and heroin among university and secondary school students, factories and site workers,
long-distance drivers, sex workers, as well as unemployed youth [14–16,23,24]. However,
in many other African countries, there is scanty or no information regarding the ongoing
opioid crisis.
The findings on the reason for illicit opioid use includes; pleasure-seeking, craving, habits,
impulsivity, improving energy [25], relieving stress [26], peer pressure from friends [27],
engendering “morale” and “courage” to engage in sex work and “fight” potentially abusive
clients [28]. Some of the reported sources are the black market [29], friends and drug dealers
[30], roadways, bus terminals or intercity stands, low-income residential areas, abandoned or
unfinished buildings, and fishing camps along the Indian Ocean [31].
Global opioid trafficking channels exist from Afganistan, through the india ocean and
East Africa to the west [19,32,33]. This impacts heroin use among the population living in the
coastal region of Comoros, Tanzania, Kenya, northern Mozambique, Madagascar, Mauritius
and Seychelles [34–36]. Unlawful use of opioids could aggravate the already sporadic spread
of infectious diseases like malaria, cholera, and HIV [37–41]. In 2018, the UNODC [42,43]
predicted with insufficient evidence that another opioid crisis was developing in Africa. Inadequate
vital record-keeping and surveillance systems make it challenging to comprehend the
incidence burden and effects of opioid overdose in Africa [44].
To access the full document:
Source: journal.pone.0317036
The Hyannis Consensus Blueprint is a groundbreaking framework designed to guide international efforts in addressing the devastating impact of addiction. Key pillars shape this balanced drug policy, including prevention, intervention, treatment, recovery, supply reduction, and enhanced global collaboration. With addiction now at catastrophic levels in many regions, the blueprint represents a vital roadmap for sustainable change.
The principles outlined in the blueprint prioritise strategies that discourage drug use while addressing underlying systemic challenges. It promotes innovating criminal justice systems, encourages adopting evidence-based treatment options, and advocates uniting globally to combat addictive substances.
Failing to address addiction comes with an enormous human and economic cost. The transcript from the Hyannis Consensus launch highlights a pressing need to move beyond toxic cycles of permissive drug policies and normalisation. Legalisation of drugs, as seen in North America, has reportedly led to devastating effects, particularly among young people, and prioritised corporate profits over public health.
The Hyannis Consensus Blueprint stands as a counterpoint to this trend. It promotes a world where communities can thrive without the shadow of addiction, empowering individuals to recover fully and lead drug-free lives.
At its core, the Hyannis Consensus Blueprint revolves around prevention and recovery. Prevention aims to stop drug use before it starts, while recovery offers individuals a path to rebuild their lives. This proactive approach aims to not only reduce harm but also transform lives for the better.
The blueprint urges balancing efforts across criminal justice and public health systems. Effective drug courts alongside harm-reduction interventions serve as vital tools in discouraging drug use and fostering recovery. Nations serious about tackling addiction must consider these solutions to safeguard future generations.
Governments worldwide are now being urged to realign their national drug policies with the principles of the Hyannis Consensus Blueprint. Countries are encouraged to reaffirm their commitment to international drug conventions, reject legalisation experiments that prioritise private interests, and expand programmes rooted in criminal justice reform and effective public health measures.
The launch of this blueprint serves as a rallying cry for nations determined to prioritise human dignity and community wellbeing. By adopting the Hyannis Consensus Blueprint, countries can pave the way for healthier, more resilient societies.
Addiction is more than an individual struggle; it’s a societal challenge that affects families, economies, and futures. The Hyannis Consensus Blueprint is a bold step towards reversing the tide of permissive drug policies and ineffective strategies. For countries looking to protect their citizens, this balanced drug policy provides the tools and vision necessary for meaningful change.
Organisations like the Dalgarno Institute and WFAD are at the forefront of this global effort, highlighting the importance of this significant, timely initiative. Communities deserve policies that prioritise recovery, not exploitation, and the Hyannis Consensus Blueprint is uniquely positioned to achieve this goal.
Learn more here.
Source: https://wrdnews.org/the-hyannis-consensus-blueprint-a-landmark-in-balanced-drug-policy/
This story originally appeared on NPR’s “All Things Considered.”
Pennsylvania is seeing roughly 2,000 fewer drug deaths a year. Nationwide, the number of annual deaths from drug overdoses has dropped by more than 30,000 people a year.
On a blustery winter morning, Keli McLoyd set off on foot across Kensington. This area of Philadelphia is one of the most drug-scarred neighborhoods in the U.S. In the first block, she knelt next to a man curled on the sidewalk in the throes of fentanyl, xylazine or some other powerful street drug.
“Sir, are you alright? You OK?” asked McLoyd, who leads Philadelphia’s city-run overdose response unit. The man stirred and took a breath. “OK, I can see he’s moving, he’s good.”
In Kensington, good means still alive. By the standards of the deadly U.S. fentanyl crisis, that’s a victory.
It’s also part of a larger, hopeful trend. Pennsylvania alone is seeing roughly 2,000 fewer drug deaths a year.
Nationwide, the number of annual deaths from drug overdoses has dropped by more than 30,000 people a year.
That’s according to the latest provisional data from the Centers for Disease Control and Prevention, comparing drug deaths in a 12-month period at the peak in June 2023 to the latest available records from October 2024.
Officials with the CDC describe the improvement as “unprecedented,” but public health experts say the rapidly growing number of people in the U.S. surviving addiction to fentanyl and other drugs still face severe and complicated health problems.
“He’s not dead, but he’s not OK,” McLoyd said, as she bent over another man, huddled against a building unresponsive.
Many people in Kensington remain severely addicted to a growing array of toxic street drugs. Physicians, harm reduction workers and city officials say skin wounds, bacterial infections and cardiovascular disease linked to drug use are common.
“It’s absolutely heartbreaking to see people live in these conditions,” she said.
Indeed, some researchers and government officials believe the fentanyl overdose crisis has now entered a new phase, where deaths will continue declining while large numbers of people face what amounts to severe chronic illness, often compounded by homelessness, poverty, criminal records and stigma.
“Initially it’s been kind of this panic mode of preventing deaths,” said Nabarun Dasgupta, who studies addiction data and policy at the University of North Carolina-Chapel Hill. His team was one of the first to detect the national drop in fatal overdoses.
His latest study found drug deaths have now declined in all 50 states and the trend appears to be long-term and sustainable. “Now that we have found some effective ways to keep people alive, it’s really important to reach out to them and try to help them improve their whole lives,” Dasgupta said.
Source: https://whyy.org/articles/fentanyl-deaths-help-for-survivors/

Vienna (Austria), 14 March 2025 — The sixty-eighth session of the Commission on Narcotic Drugs (CND) concluded today after five days of intensive discussions on global drug policy, international cooperation and the implementation of international drug policy commitments. The strong engagement and high level of participation from governments and stakeholders in Vienna, 2,000 of whom gathered to exchange views and shape collective responses to evolving drug-related challenges, demonstrates the Commission’s relevance as the global platform for addressing the complexities of the world drug problem in an evidence-based, forward-looking manner.
In her closing remarks, United Nations Office on Drugs and Crime (UNODC) Executive Director Ghada Waly emphasized the importance of strengthening the CND. “In times of division and uncertainty, we need effective multilateral institutions more than ever,” she said. “And the level of engagement at this session has once again confirmed the enduring relevance of this Commission as the global forum for drug policy.”
She urged Member States to redouble their efforts, commitment and cooperation, recognizing that the evolution of the world drug problem demands a renewed and determined response. “UNODC will remain committed to working for a healthier and safer world, guided by the decisions of Member States,” she concluded.
In fulfilling its normative functions under the international drug control conventions, the Commission acted on recommendations from the World Health Organization (WHO), deciding to place six substances under international control. These include four synthetic opioids – N-pyrrolidino protonitazene, N-pyrrolidino metonitazene, etonitazepipne, and N-desethyl isotonitazene – which have been linked to fatal overdoses. The Commission also placed hexahydrocannabinol (HHC), a semi-synthetic cannabinoid with effects similar to THC that has been found in a variety of consumer products, under Schedule II of the 1971 Convention. Additionally, carisoprodol, a centrally acting skeletal muscle relaxant, widely misused in combination with opioids and benzodiazepines, was placed under Schedule IV of the 1971 Convention due to its potential for dependence and health risks. These scheduling decisions reflect the Commission’s ongoing efforts to respond to emerging drug threats and protect public health.
The Commission on Narcotic Drugs (CND) also adopted six resolutions, reinforcing global efforts to address drug-related challenges through evidence-based policies and strengthened international cooperation.
To protect children and adolescents, the Commission encouraged the implementation of scientific, evidence-based drug prevention programs, emphasizing the need for early interventions and cross-sectoral collaboration to build resilience against non-medical drug use.
Recognizing the growing impact of stimulant use disorders, another resolution promoted research into effective, evidence-based treatment options, calling on Member States to invest in innovative pharmacological and psychosocial interventions to improve care for those affected.
The importance of alternative development was reaffirmed with a resolution aimed at modernizing strategies that help communities transition away from illicit crop cultivation, ensuring long-term economic opportunities while addressing broader issues like poverty and environmental sustainability.
In response to the rising threat of synthetic drugs, the Commission adopted a resolution to protect law enforcement and first responders dismantling illicit synthetic drug labs and advocating for stronger safety protocols, enhanced training and international cooperation to reduce risks.
To strengthen the implementation of international drug control conventions and policy commitments, the Commission decided to establish an expert panel tasked with developing a set of recommendations to strengthen the global drug control system.
Additionally, recognizing the environmental damage caused by illicit drug-related activities, the Commission adopted another resolution calling on Member States to integrate environmental protection into drug policies and address the negative impacts on the environment resulting from the illicit drug-related activities.
These resolutions reflect the Commission’s commitment to providing concrete, coordinated responses and ensuring that drug control policies remain effective, adaptive and aligned with contemporary challenges.
Source: https://www.unodc.org/unodc/frontpage/2025/March/cnd-68-concludes_-six-new-substances-controlled-six-resolutions-adopted.html
![]() Delegation of the European Union to the International Organisations in Vienna
Delegation of the European Union to the International Organisations in Vienna
It is an honour to be here and to speak on behalf of the European Union and its Member States. Albania, Andorra, Bosnia and Herzegovina, Georgia, Iceland, Montenegro, North Macedonia, Republic of Moldova, San Marino and Ukraine align themselves with this statement.
Mr Chair,
We remain committed to strengthening the global cooperation to address drug-related challenges in accordance with an evidence-based, integrated, balanced and comprehensive approach. We acknowledge the important role of UNODC in monitoring the world drug situation, developing strategies on international drug control and recommending measures to address drug-related challenges.
As we meet today, conflicts and violence are unfolding in numerous parts of the world. The EU and its Member States call for the full respect for the UN Charter andinternational law, including international humanitarian law, whether in relation to Russia’s war of aggression against Ukraine, or the ongoing conflicts in the Middle East, Sudan, Ethiopia, DRC and elsewhere.
Drug trafficking controlled by organised crime groupsthreatens public health, our security, our economies and prosperous development worldwide, and even our democratic institutions and the rule of law. This is an important security challenge that Europe is currently facing. As demonstrated by the European Drug Report 2024, as a consequence of the high availability of drugs, large-volume trafficking and competition between criminal groups in Europe, some countries are experiencing an increase in violence and other forms of criminality linked to the operation of the drug market.
To address this concern, last November the EU hosted the European Conference on Drug-related Violenceas part of the implementation of the EU Roadmap to combat drug trafficking and organised crime. At the conference, the EU Drugs Agency called for action on drug-related violence, to encourage and support efforts to enhance safety and security across all sectors of society with measures to anticipate, alert, respond and learn from the growing complexities of drug-related violence. This initiative reflects our collective determination to address the increasing violence linked to drug trafficking.
In line with the pledge of the Global Coalition to address Synthetic Drug Threats that the EUcommitted to in September 2024, we are currently closely monitoring the risks of a potential increase in the supply and demand for synthetic opioids in Europe. This possible shift could represent unique challenges for public health systems and law enforcement.
Among such challenges is the growing number of illegal laboratories that produce synthetic drugs. Considering the threat they pose, Poland – on behalf of the EU – has tabled a resolution that draws attention to the protection of all those that are at the forefront of dismantling drug laboratories. Our aim is to set the ground for global standards in ensuring the safety of law enforcement officers, and we count on your support for this important resolution.
The EU and its Member States also call for greater consideration of development-oriented drug policies and alternative development measures, as well as the environmental damage linked to the direct and indirect impact of illicit drug crop cultivation, drug production and manufacture and drug policy responses. Conscious of the realities that shape our world, a resolution addressing the environmental impact of drugs has been tabled by France on behalf of the EU. This is atopic that needs more engagement from all of us, and we hope that you will back this resolution as well.
The EU and its Member States continue to emphasise that States are obliged to protect, promote and fulfilhuman rights, including when they develop and implement drug policies. All human beings are born free and equal in dignity and rights, and the EU and its Member States recall that the death penalty should be abolished globally. We condemn the use of capital punishment at all times and under all circumstances, including for drug-related offences. Additional measures should be taken for people in vulnerable and marginalised situations and to reduce stigma and discrimination. We underline that substance use disorders are a health issue requiring compassionateand evidence-based interventions. Stigmatisation and criminalisation of individuals with substance use disorders should be replaced with a health-centredapproach to reduce risks and harm.
Addressing drug-related harm also remains an important pillar of EU drug policy and the EU Drugs Strategy. The EU and its Member States are implementing a human rights-based approach with a range of measures in compliance with the three international drug conventions. The aim is to reduce drug supply and to take prevention, treatment, care and recovery measures, to reduce risk and harm to society and to the individual. We also ensure a meaningful involvement of scientific experts, civil society and affected communities. We urge the international community to further embrace pragmatic measures aimed at reducing the health and social harms, both for the individual and for society, associated with drug use. From needle and syringe exchange programmes to opioid agonist therapies, such evidence-based initiatives are essential for safeguarding public health and dignity. Prevention, treatment, care and recovery measures, risk and harm reduction must be expanded, adequately resourced, and firmly rooted in respect for human rights, as also set out in last year’s CND resolution 67/4 [on preventing and responding to drug overdose through prevention, treatment, care and recovery measures, as well as other public health interventions, to address the harms associated with illicit drug use as part of a balanced, comprehensive, scientific evidence-based approach].
In the context of current global drug-related challenges, it is important to stress that effective solutions can only be achieved through a balanced and whole-of-society approach as well as by engaging all relevant stakeholders, including health-care personnel, who provide critical support to those affected by substance use disorders; law enforcement officers, who risk their lives in targeting organised crime groups involved in drug production and trafficking; academia, which contributes with evidence-based research and innovative solutions; civil society organisations, which play an important role in prevention, and in risk and harm reduction initiatives. International cooperation is also indispensable to tackle the global drugs phenomenon and we count on the close involvement ofall relevant United Nations entities, including human rights bodies, to foster coordinated international action and inter-agency cooperation.
As set out in the high-level declaration by the CND on the 2024 mid-term review, we stress the urgent need for further ambitious, effective, improved and decisive actions as well as for more proactive, scientific evidence-based, comprehensive, balanced approaches to address drug-related challenges.
For that, we emphasise the critical importance of thorough data collection, monitoring, and scientific research. The European Union Drugs Agency is therefore key in developing Europe’s capacity to react to both current and future drug-related challenges, and we have made a concrete pledge in this regard at last year’s High-level segment of the CND.
Mr. Chair, to conclude,
Continuous drug-related challenges require our united front and cooperation to address them in the most effective and sustainable manner, and we count on global efforts to do so together. The EU and its Member States reaffirm their own commitment to fostering a comprehensive, inclusive, and balanced approach to addressing the world drug situation. We call on all Member States and stakeholders to join us in prioritising health, dignity, and human rights in all aspects of drug policy.
Thank you.
SOURCE: https://www.eeas.europa.eu/delegations/vienna-international-organisations/eu-statement-general-debate-68th-session-commission-narcotic-drugs-10-march-2025_en
After achieving six months of sobriety, Horning has become a vocal advocate for comprehensive substance use prevention and education programs aimed at helping students in Warren County lead substance-free lives.
His initiative, developed in collaboration with Dr. Patricia Hawley-Mead and district officials, seeks to implement substance use prevention and education services across the school district. The goal of the initiative is to provide students, teachers, and parents with the education, community resources, and intervention strategies needed to prevent substance use and promote healthier lifestyle choices.
“If you were to tell me eight months ago I would be standing in front of you talking about substance abuse prevention and putting Narcan in AED boxes, I would have said you were crazy,” Horning shared with the audience during a recent school board meeting.
Horning’s passion for substance use prevention stems from his own difficult experience with addiction. He has openly shared his struggles with substance use, depression, and unhealthy coping mechanisms that led him down a painful path.
“My addiction was full of loss, hardships, and failures,” Horning explained. “Nothing seemed to work, nothing was helping me, and most importantly, I wasn’t helping myself. I’ve been in and out of psychiatrists’ offices, tried different medications, and felt completely lost. The only way I found recovery was by chance, but it shouldn’t be that way. We need a system in place to give students a way out before it’s too late.”
Looking back on his darkest moments, Horning admitted he never imagined he would be advocating for change in front of a crowd.
“I was not a great person at that moment in time,” he said, becoming emotional. “I made a lot of mistakes. My family, who is sitting behind me today, can tell you that. People inside and outside of school districts saw me at my worst. The disease of addiction is a lifelong battle that I will face until the day I die. But that does not mean it has to end in tragedy. That is why I am standing here today – to fight for others like me.”
Horning recognizes that many students turn to substances for a variety of reasons–whether out of boredom, depression, anxiety, or as a way to cope with personal struggles. His initiative is designed not only to educate students on the dangers of substance use but also to provide them with the tools and support systems they need to make better, healthier choices.
“This initiative will not only help students stay alive in case of an overdose, but it will help them find a way out of addiction and into a new life,” he emphasized. “Even if this helps just one person, it will all be worth it.”
INITIATIVE’S INSPIRATION
The inspiration behind Horning’s initiative came after a district-wide program held on September 18, 2024. During the event, public speaker Stephen Hill presented the First Choice & A Second Chance program to high school students. The program aimed to break the stigma surrounding substance use disorder, raise awareness about the ongoing drug epidemic, and encourage students to make healthier decisions.
Following the event, Horning was motivated to take action. He reached out to district administrators, safety officers, the school nurse department head, and a Family Services of Warren County drug and alcohol counselor to begin crafting a proposal for a comprehensive Substance Use Prevention and Education Service in the district.
The proposal calls for the establishment of educational programs that would teach students about the risks associated with substance use, provide early intervention services, and offer mental health support. Additionally, Horning’s plan includes provisions for Narcan to be available in school AED boxes, ensuring that life-saving measures are ready in case of an overdose emergency.
Hawley-Mead, who has worked closely with Horning on the initiative, stressed the importance of early intervention and prevention.
“The increasing prevalence of substance use among young people is a growing concern,” Mead said. “It poses a significant risk to their academic success, emotional well-being, and future prospects. Early prevention and education efforts have been shown to reduce substance use, improve student decision-making, and help create a more supportive and empathetic learning environment.”
Mead believes that by fostering a collaborative effort among educators, parents, and community partners, the district can proactively address the issue of substance use and equip students with the knowledge and support they need to thrive.
“This initiative will provide students, teachers, and parents with education, resources, and intervention strategies to support healthy choices and foster a positive, drug-free environment,” Mead said.
Horning concluded his speech with an emotional reflection on his own personal journey and the importance of offering help to others who may be struggling.
“What drove me to do this was really a lot of depression and unhealthy coping skills,” he shared. “I was not in the right mindset when I first used. I was not okay. If somebody had sat me down and told me, ‘We can help you,’ it could have saved me years of pain. That’s why we need this now. We need to offer students the opportunity to get help before it’s too late.”
Horning is determined to ensure that no student has to face the same struggles he did. His initiative is not only aimed at providing support for those already struggling with substance use but also preventing others from ever going down that difficult path.
“The only way I found recovery was by chance,” he admitted. “That’s the best way I can put it. Recovery is important, but when you are in an active addiction, it feels impossible to get through to someone. That’s why, eight months ago, I would have called you crazy if you told me I’d be standing here today. But now, I’m here. I have made myself a better person, and I want to give back for what I have found.”
Horning and district officials are now seeking approval from the school board and the community to bring this initiative to life in Warren County schools. Their goal is to integrate substance use prevention education into the curriculum, provide resources for students and families, and ensure that Narcan is available in AED boxes to help prevent potential overdose deaths.
“We don’t have to live in tragedy like other schools have,” Horning said. “We need to teach students how to use Narcan, how to stay alive, and most importantly, how to find a way out of addiction. Recovery is possible, and I want to show others that they don’t have to suffer alone.”
HORNING’S PROPOSAL
Horning’s written proposal outlines five key goals for the pilot initiative: Enhance school safety by increasing access to Narcan for emergency overdose response. Educate the school community about substance use prevention, intervention, and response strategies. Establish a student club focused on substance use awareness, prevention, and peer education to increase awareness and reduce stigma surrounding substance use disorder. Actively engage stakeholders, including students, staff, families, and community partners, to establish an anonymous and supportive program where students can learn about and advocate for substance use prevention. Create a district-sponsored club dedicated to promoting substance use prevention and education.
Hawley-Mead emphasized that while Narcan is already available in nurse’s offices during school hours, having it in AED boxes would ensure it’s accessible during after-school activities and weekend events.
“This proposal aims to make Narcan more widely available and accessible to first responders during emergencies, regardless of the time of day,” she said. “We want to ensure that this life-saving measure is available whenever and wherever it’s needed.”
Horning also reached out to Family Services of Warren County, which has expressed strong support for the initiative.
“They are very, very responsive towards this program,” Horning said. “I’ve spoken with counselors, including Nicole Neukum, executive director, and they’re all willing to give us whatever we need to make this a success.”
School board member Mary Passinger asked Horning if he felt comfortable sharing the personal story behind his addiction.
“It was really a lot of depression and unhealthy coping skills,” Horning responded. “I was not in the right mindset when I first used. If someone had told me, ‘We can help you,’ it could have saved me from years of pain.”
Board member John Wortman commended Horning for his bravery in speaking out and bringing this important issue to the district’s attention.
“There is nothing more important than standing up for what you believe in,” Wortman said. “The proposals outlined here will help make a significant, positive impact on students in Warren County. And that’s something we can all support.”
Superintendent Gary Weber also voiced his strong support for the initiative.
“We are 100% behind this initiative,” he said. “It’s clear that Jessie and Dr. Mead have worked hard to bring together stakeholders and develop a plan that will have a lasting and positive impact. We want to make sure this program is sustainable, and we’re committed to supporting it every step of the way.”
The district is currently reviewing Horning’s proposal, and community members are encouraged to get involved in supporting this critical initiative. For updates and information on how to help, individuals can reach out to district officials or Family Services of Warren County.
With this initiative, Horning hopes to not only save lives but also inspire others to break free from addiction and reclaim their futures.
“Recovery is possible,” he said. “And I want to show others that they don’t have to suffer alone.”
Source: https://www.timesobserver.com/news/local-news/2025/03/student-leads-charge-for-substance-use-prevention/
Data from the Centers for Disease Control and Prevention show there were about 107,000 drug overdose deaths in the United States in 2023. Of those, about 75 percent, or 81,000, involved opioids.
With the aim of reducing those statistics, Lauren Jones ’22, who is in a post-baccalaureate at Harvard University, Brenna Outten ’22, a third-year doctoral student at Caltech and Leah Juechter ’24, who is working temporarily as a medical assistant, used computational chemistry as undergraduates at Furman to study the impacts of synthetic opioids.
Their work, with collaborators at Hendrix College and California State University, Los Angeles, was published in December in The Journal of Physical Chemistry B.
To say the project was formative for Jones and Outten is an understatement. They laid the foundation for the study during the height of COVID when traditional wet labs were all but shuttered.
“It’s amazing we were able to continue the work virtually during the pandemic,” said Jones, who researches sensory processing in children with autism and brain activity in children with rare neurodevelopmental and neurogenetic disorders at Boston Children’s Hospital.
Outten said the project “opened my eyes to how a scientist can contribute to fields like neuroscience, chemistry, biology and physics in ways I had never considered before.”
The paper focuses on work targeting the mu opioid receptor, or MOR. It resides mainly in the central nervous system and the GI tract. It’s like a molecular lock waiting for the right key (a drug like morphine or fentanyl) to unlock or activate a favorable response, such as reduced pain signals. But the same drugs can activate negative responses like drug tolerance, constipation, respiratory depression, addiction and overdose.
“There’s a lot we don’t understand about how opioids interact with the receptors embedded on nerves that mitigate the pain-signaling process,” Juechter said. “So the more we can uncover about how these drugs are interacting with the receptors in our bodies and the responses we feel, the better we’re able to help create pain therapeutics with reduced adverse effects and more beneficial safety profiles.”
What makes the researchers’ study unique is the application of both quantum mechanics conducted by Juechter, Outten and Jones, led by chemistry Professor George Shields, and molecular dynamics carried out by teams at Cal State and Hendrix College.
“It was interesting to see two drugs (morphine and fentanyl) that elicit almost identical effects are binding to the receptor in completely different ways,” Juechter said. “And to demonstrate that with highly accurate quantum mechanics was one of the first times we’ve seen that done.”
The manner in which opioids bind to MOR is diverse and complex. “So the need for a precise computing model becomes essential,” Juechter explained. “Even slight variations in calculations can drastically affect the data and subsequent conclusions.”
The ability to do research computationally can make drug development faster and cheaper, Juechter added. “Being able to paint the picture of what’s going on using empirically-supported mathematical theories, we can streamline the initial process of drug development.”
Impactful undergraduate research is a hallmark of The Furman Advantage, a four-year approach to education that creates a pathway for students to determine who they want to be and how they want to contribute to the world once they leave the university.
Juechter spent about eight months post-graduation fine-tuning the work with her co-authors before the paper was published.
“It was exceedingly evident Dr. Shields wanted to elevate me and give me the opportunity to pursue research,” Outten said.
Juechter hopes the project will set the tone for organic chemists involved in drug research and development.
“I want a role in the health care industry because I like the idea of affecting someone’s life in real time, in a positive way,” she said.
Source: https://www.furman.edu/news/neuroscience-grads-studied-how-to-make-opioids-safer
by Mark Gold M.D. – Professor of Psychiatry, Yale, Florida and Washington Universities
According to Sharon Levy, MD,Harvard Medical School’s pediatric addiction expert, nonmedical medication misuse may be much more common than previously reported. One of the older fads is in the news again: getting high from cough and cold medicines containing dextromethorphan (DXM). This drug is sometimes combined with prescribed promethazine with codeine. At very high doses, DXM mimics the effects of illegal drugs like phencyclidine (PCP) and ketamine.
More than 125 over-the-counter (OTC) medicines for cough and colds contain DXM. It’s in Coricidin, Dimetapp DM, Nyquil, Robitussin Cough and Cold, and store brands for cough-and-cold medicines. These products are available in pharmacies, grocery stores, and other retail outlets. A safe dose of products with DXM is about 15-30 milligrams (mg) over 24 hours. It usually takes 10 times that amount to make a teenager high.
A syrup head is someone using cough syrups with DXM to get high. Dexing is getting high on products with DXM. Orange Crush alludes to some cough medicines with DXM. (The name may stem from the orange-colored syrup—and packaging—Delsym.)
Poor man’s PCP and poor man’s X are also common terms, because these drugs are inexpensive, but can cause effects similar to PCP or ecstasy at high doses. Red devils refer to Coricidin tablets or other cough medicines. Robo usually refers to cough syrup with DXM. It derives from the brand name Robitussin but is common slang for any cough syrup. Robo-tripping alludes to abusing products with DXM and, specifically, to the hallucinogenic trips people can attain at high doses.
The Monitoring the Future (MTF) survey, conducted by the National Institute on Drug Abuse (NIDA) and the University of Michigan, provides insights into adolescent substance use. The survey began monitoring OTC cough-and-cold medication abuse every year in 2006. That year, the MTF reported that 4.2% of 8th-graders, 5.3% of 10th-graders, and 6.9% of 12th-graders misused OTC cough-and-cold medications in the previous year. In 2015, 2.6% of 8th-graders, 3.3% of 10th-graders, and 4.0% of 12th-graders reported past-year misuse. The most recent data, in 2024, indicate that the percentage dropped somewhat. However, a recent alert from the National Drug Early Warning System at the University of Florida (NDEWS) suggests a resurgence of interest in DXM and its combination with antihistamines.
When taken alone, DXM’s dissociative and hallucinogenic effects may include euphoria, altered perception of time, paranoia, disorientation, and hallucinations. Physical symptoms of intoxication are hyperexcitability, problems walking, involuntary eye movements, and irritability. High doses can lead to impaired motor function, numbness, nausea and vomiting, increased heart rate, and elevated blood pressure. Chronic misuse results in dependence and severe psychological or physical health issues.
Combining DXM with other substances, especially alcohol, sleeping pills, antihistamines, or tranquilizers, is highly risky, as is combining DXM with antidepressants affecting serotonin, due to the risk of a possibly life-threatening serotonin syndrome.
Combining the abuse of the prescribed antihistamine promethazine (Phenergan) with DXM may be increasing. The recent alert from the National Drug Early Warning System suggested that this new combination is an emerging threat.
The NDEWS recently checked for recent reports of saccharine (artificial sugar) being detected in abused drugs. Putting on their detective hats, the NDEWS team discovered that increased saccharine in drugs was caused by users adding cough syrup to promethazine. The signal for this combination was detected in more than double the number noted in early 2024.
Combining DXM and promethazine can amplify central nervous system depression, leading to increased drowsiness, dizziness, and impaired motor function. High doses may cause aggression, severe respiratory depression, hallucinations, delirium, paranoia, and cognitive impairments. Reddit social media reports noted an increased risks of falls and injuries due to severely impaired coordination and balance from the DXM-and-promethazine combination.
Promethazine with codeine is still available by prescription in the U.S., but access is restricted due to its classification as a Schedule V controlled substance at the federal level. Pharmacies and healthcare providers have become more cautious in prescribing promethazine with codeine due to its association with recreational use. Some manufacturers have discontinued production of promethazine with codeine, but generic versions remain on the market under tight regulation.
Purple drank is drug slang for the mixture containing codeine and promethazine mixed with a soft drink such as Sprite or Fanta—and sometimes with candy such as Jolly Ranchers. The drink gets its name from the purple color of some cough syrups. Purple drank has been popularized in certain music and hip-hop cultures, with some artists glorifying its use in their lyrics. However, many rappers who once promoted the drug later warned against its dangers after experiencing serious health consequences themselves or witnessing peers suffer from addiction and overdoses.
While the combination of DXM and promethazine is not commonly reported in drug abuse or emergency-room cases, misuse could lead to significant health risks. Stores have started to keep these cough and cold remedies behind the counter to reduce access and potential for teen abuse. Some makers of OTC medicines with DXM have put warning labels on their packaging about the potential for abuse. Many states have banned sales of meds with DXM to minors. These actions have helped reduce teen DXM abuse. However, recent teen interest in abuse of combined DXM and promethazine is concerning.
Source: https://www.psychologytoday.com/us/blog/addiction-outlook/202502/teenage-abuse-of-cough-medicines-and-promethazine

In November, Donald Trump made significant electoral gains in New York’s black and Latino neighborhoods, and in the city’s least affluent communities. Now he is poised to take an important step to improve public safety in these voters’ neighborhoods.
Rep. Nicole Malliotakis (R-SI) last week wrote to new Attorney General Pam Bondi, pleading for the administration to shut down the city’s two “safe injection sites.”
These facilities, located in East Harlem and Washington Heights, provide supervision to drug abusers as they consume harmful substances like fentanyl, meth, heroin and cocaine.
Yes, these are illegal drugs under federal law — and the aptly nicknamed federal “crack house statute” prevents individuals from retaining property for their consumption.
Indeed, Trump’s Justice Department successfully shuttered similar sites in the past – In 2019, his first administration sued to stop a Philadelphia injection center from opening, and in 2024 a US District Court judge in Pennsylvania finally agreed that the center was not exempt from federal drug laws.
Now Trump should listen to his NYC minority constituents and close the injection sites that are harming their neighborhoods.
New York’s two centers, both run by non-profit OnPoint, were the first in the nation, opening in 2021 under then-Mayor Bill de Blasio — who never met an injurious policy he wouldn’t support in the name of racial justice.
De Blasio gambled successfully that the Biden administration wouldn’t intervene.
OnPoint claims to have saved over 1,000 lives by preventing overdoses. But as my colleague Charles Fain Lehman has pointed out, the sites do not reduce addiction — so they are likely just delaying fatalities: More than 15% of those administered naloxone are dead within a year.
Indeed, data shows that NYC overdose rates have continued to rise since the centers opened.
That’s no surprise, since a rigorous look at the data from even the most touted injection sites in other countries provide no evidence of their effectiveness
But rigor has never been the calling card for politicians and advocates who happily sacrifice other people’s communities in the name of compassion.
State Sen. Gustavo Rivera (D-Bronx) has had the chutzpah to claim that “public drug use, syringe litter and drug-related crime goes down” around sites. In 2023, Rivera urged Gov. Hochul to expand supervised consumption sites statewide, and sponsored Senate legislation — still in committee — to do so.
In 2023, Mayor Eric Adams also proposed adding three more facilities to NYC — but he might be amenable to updating his views with some pressure from Washington.
And that pressure will come if Trump cares about the lives of local residents.
While major crimes fell 13% in northern Manhattan over the past two years, the predominantly black and Hispanic precinct around the East Harlem drug site has seen an almost 8% rise in major crime.
I’ve toured that location with the Greater Harlem Coalition. Members pointed out the large early-childhood education center directly across the street from the injection site, as parents hurried their tots into school in plain view of ongoing drug deals.
The perimeter of the block is dotted with addicts nodding off. Nearby restaurants have had to invest in private security to defend against the criminality the center attracts to the neighborhood.
What’s been keeping this site open despite four years in which the only evidenced change is neighborhood degradation?
Shameless advocacy by pompous, ideologically motivated and race-obsessed elites . . . whose kids don’t go to preschool in Harlem.
In August, Greater Harlem Coalition co-founder Shawn Hill was interviewed by one such far-left advocate: Ryan McNeil, director of harm reduction research at Yale’s School of Medicine.
McNeil was conducting funded “research” into safe injection sites — but a “hot mic” recording revealed his and his colleagues’ woke bias in favor of supporting safe injection sites (and drug decriminalization, more broadly).
But Trump has every reason to listen to these locals, three-quarters of whom are black or Latino.
And it would behove Adams, who faces a crowded primary race this summer, to reverse his past stance and voice support for a federal closure of the city’s two drug consumption sites.
In East Harlem, Trump won about 860 more votes last year than in 2020. Now these supporters, and their neighbors he has yet to persuade, are depending on his help.
Source: https://nypost.com/2025/02/16/opinion/inject-some-common-sense-shut-down-nycs-safe-drug-sites/
 Eyewitness News – Friday, February 14, 2025
Eyewitness News – Friday, February 14, 2025NEW YORK (WABC) — There are places people can go take illegal drugs under the watchful eye of supervisors to ensure they don’t die.
They are called Overdose Prevention Centers, or also known as safe injection sites, and there are two of them in New York City — the first of its kind in the nation.
Now, after more than three years of operating, there’s a new effort under a new president to shut down the centers that are run by a non-profit organization.
It’s called OnPoint NYC and they have two locations in Washington Heights and East Harlem.
Drug users can take their drug of choice from heroin to cocaine inside the centers and supervisors intervene, most times with oxygen, if the user starts to overdose. They also provide test strips for drugs to ensure they don’t have fatal doses of fentanyl inside.
Since opening in 2021, the executive director said they’ve intervened in more than 1,700 overdoses. They also provide services like medical help, substance abuse treatment and housing assistance.
Opponents say the centers encourage people to do illegal drugs.
“They’re encouraging people to use by giving them a community center to go to and to use heroin, it’s something that’s encouraging addicts not helping them,” said Congresswoman Nicole Malliotakis.
She sent a letter to the newly confirmed attorney general, asking her to shut down both locations along with any others that have opened across the country.
In response, the executive director of OnPoint NYC sent Eyewitness News a statement:
“OPCs save lives. At OnPoint NYC, our staff has intervened in over 1,700 overdoses, providing life-saving care to mothers, fathers, and loved ones,” said OnPoint NYC Executive Director Sam Rivera. “Every single one of them deserves compassion and a chance at healing. I’m incredibly proud of our team and continually inspired by the dedication they show every day. They don’t just look at the overdose epidemic and wonder what can be done-they don’t have that luxury. They act, because they have lives to save. This work is not just vital; it’s transformational. Lives are being saved, hope is being restored, and healing is possible.”
Source: https://abc7ny.com/post/president-trump-asked-shut-down-overdose-prevention-centers-have-operated-3-years-nyc/15907033/
Today, some members of America’s political class are desensitized to the drug crisis. They tolerate normalizing psychoactive substance use.
The relentless movement to legalize drug use has succeeded, largely by appealing to the goodwill and sympathies of the American public.
For supply reduction, the U.S. must send a clear message to the world that we are not an open market for drugs.
The federal government has long sought to prevent the horrors of drug addiction by interdicting the supply of dangerous psychoactive drugs—and reducing demand for them.
One step was the Anti-Drug Abuse Act of 1988. It established the Office of National Drug Control Policy (ONDCP) within the Executive Office of the President. Headed by a director colloquially known as “drug czar,” ONDCP had the task of developing a national drug-control strategy to reduce drug use. Its creation symbolized a strong bipartisan effort to prevent illicit drugs from destroying lives and weakening the nation.
Sadly, we have lost that shared mission. No president since George W. Bush has publicly demonstrated a deep and firm support for ONDCP and its mission.
The agency does not reside in the White House office building, let alone the West Wing. The federal government has largely been a bystander despite the unraveling of restrictive opioid prescribing, state implementation of medical/recreational marijuana programs in violation of federal laws, and the incipient movement by states to legalize psychedelics. Most presidents have largely ignored these trends.
The first Trump administration assembled a commission to combat drug addiction and the opioid crisis. The current one should support a comprehensive effort led by ONDCP to overhaul drug policies and strengthen America’s commitment to reducing and delegitimizing drug use. We need a revitalized ONDCP equipped with innovative goals and measurable outcomes to disrupt the pipeline to addiction and to cease preventable, premature deaths and mental health decline. A single centralized agency ensures coordination across federal agencies, state, and local levels to maximize efficiency and accountability.
Today, some members of America’s political class are desensitized to the drug crisis. They tolerate normalizing psychoactive substance use and the addiction, health crises, deaths, and collateral damage to families that follow.
Reformers advocate destigmatizing regular use of hazardous psychoactive drugs. “Harm reduction” practices, initially framed as temporary measures, now are uncritically promoted in some quarters without clear boundaries or outcome goals.
This “Meet drug users where they are” approach has regressed to a “Leave them where they are” one. The grim realities of “tranq”-induced catatonia on the streets of Philadelphia’s Kensington neighborhood, San Francisco’s Tenderloin district, Boston’s Mass and Cass intersection, and other drug-ridden homeless encampments lay bare the stark failure of America’s waning resolve to minimize drug use.
Among other nations, we are an outlier. America’s drug crisis has escalated dramatically since ONDCP was born. Overdose deaths surged from 3,907 (1.6 per 100,000) in 1987 to a record 107,543 (32.2 per 100,000) in 2023, with teen rates doubling recently. Among twelfth-graders, 13 percent use marijuana daily, despite heightened risks for addiction and psychosis. In 2023, daily use of marijuana and regular use of hallucinogens among 19- to 30-year-olds reached record levels, fueled by pervasive myths about “safety” or “medical” efficacy
Whether used for medical or recreational purposes, or both, 25 percent of cannabis users have a cannabis-use disorder; among twelve- to 24-year-olds, such a disorder is more prevalent than alcohol-use disorder. Over 90 percent of individuals with substance-use disorders (48.7 million people) neither recognize their need for help nor seek treatment.
Topping it off, seizures of fentanyl-laced pills exploded from 49,000 in 2017 to a staggering 115 million in 2023. Reversing this runaway train demands a transformative political and cultural shift led by the president, ONDCP, and Congress.
How?
Start by learning from past mistakes. The relentless movement to legalize drug use has succeeded, largely by appealing to the goodwill and sympathies of the American public. In 1996, activists persuaded California’s voters to adopt marijuana as a medicine by labelling it as “compassionate use” for end-stage cancer and HIV-AIDS wasting.
That success gave legalizers a foothold. Slowly, the movement persuaded other states to adopt medical-use marijuana for myriad purposes without a shred of evidence; this later morphed into recreational-use programs. Dual-purpose “dispensaries” now sell marijuana for any reason. Activists persuaded the medical profession that pain was the “fifth vital sign” and pressured caregivers to prescribe highly addictive opioids liberally for any type of pain. We know where that went.
Finally, recent campaigns to use political means to normalize hallucinogens for medical use bear a striking resemblance to the two campaigns noted above, including media hype and their tendency to lampoon cautious Cassandras. Compassion is a virtue, except when it leads to long-term harm.
Those who are driving the normalization of substance use as a chemical shortcut for pleasure or relief are willing to sacrifice long-term well-being for short-term escapism. Without prevention strategies to disrupt this pathway of use, addiction, and death, no amount of treatment or law enforcement will resolve the crisis.
We should oppose efforts to destigmatize drug use but support destigmatization of individuals with substance-use disorders to ease their entry into treatment and recovery. To end the frequently heard lament of parents—“If only I knew”—we need a national educational campaign that counters the myths promulgated by proponents.
We need more research to understand why substance-use disorders are resistant to treatment- and recovery. Harm-reduction strategies that don’t show objective reductions in disordered use should be challenged. And we must recognize that minorities are hurt, not helped, by liberalizing drug use because it can worsen the conditions in already suffering neighborhoods.
Finally, we should strengthen ONDCP by returning it to cabinet-level status and empowering it to adopt a results-driven business model. Steps would include, on the demand side, ensuring that federal funding is allocated to prevention and treatment programs that prioritize objective, evidence-based positive outcomes.
For supply reduction, the U.S. must send a clear message to the world that we are not an open market for drugs. This will involve stopping the smuggling of fentanyl, dismantling illegal markets, and seizing traffickers’ ill-gotten gains. Incentives and penalties can persuade nations that produce drugs and their precursor chemicals to curb their export of substances poisoning Americans.
President Trump has a unique opportunity to pivot and reform America’s recurring drug crises. A bold approach will signal America’s commitment to reversing our damaging trajectory.
This piece originally appeared in the National Review
Source: https://www.heritage.org/public-health/commentary/the-drug-crisis-hasnt-gone-away-the-trump-administration-should-confront
Journal: Substance Abuse Treatment, Prevention, and Policy, 2025, doi: 10.1186/ s13011-025-00635-z
Authors: Elian Rosenfeld, Sarah Potter, Jennifer Caputo, Sushmita Shoma Ghose, Nelia Nadal, Christopher M. Jones, … Michael T. French
Abstract:
Background: Alternative payment models (APMs) are methods through which insurers reimburse health care providers and are widely used to improve the quality and value of health care. While there is a growing movement to utilize APMs for substance use disorder (SUD) treatment services, they have rarely included SUD prevention strategies. Challenges to using APMs for SUD prevention include underdeveloped program outcome measures, inadequate SUD prevention funding, and lack of clarity regarding what prevention strategies might fit within the scope of APMs.
Methods: In November 2023, the Substance Abuse and Mental Health Services Administration (SAMHSA), through a contract with Westat, convened an expert panel to refine a preliminary conceptual framework developed for utilizing APMs for SUD prevention and to identify strategies to encourage their adoption.
Results: The conceptual framework agreed upon by the panel provides expert consensus on how APMs could finance a variety of prevention programs across diverse populations and settings. Additional efforts are needed to accelerate the support for and adoption of APMs for SUD prevention, and the principles of health equity and community engagement should underpin these efforts. Opportunities to increase the use of APMs for SUD prevention include educating key groups, expanding and promoting the SUD prevention workforce, establishing funding for pilot studies, identifying evidence-based core components of SUD prevention, analyzing the cost effectiveness of APMs for SUD prevention, and aligning funding across federal agencies.
Conclusion: Given that the use of APMs for SUD prevention is a new practice, additional research, education, and resources are needed. The conceptual framework and strategies generated by the expert panel offer a path for future research. SUD health care stakeholders should consider ways that SUD prevention can be effectively and equitably implemented within APMs.
To read the full text of the article, please visit the publisher’s website.
Journal: American Journal of Preventive Medicine, 2025, doi: 10.1016/j.amepre.2024 .10.019
Authors: Katrina A. Vickerman, Kelly M. Carpenter, Kristina Mullis, Abigail B. Shoben, Julianna Nemeth, Elizabeth Mayers, & Elizabeth G. Klein
Abstract:
Introduction: Broad-reaching, effective e-cigarette cessation interventions are needed.
Study design: This remote, randomized clinical trial tested a mHealth program and nicotine replacement therapy (NRT) for young adult vaping cessation.
Setting/participants: Social media was used from 2021 to 2022 to recruit 508 young adults (aged 18-24 years) in the U.S. who exclusively and regularly (20+ days of last 30) used e-cigarettes and were interested in quitting.
Intervention: All were offered 2 coaching calls and needed to complete the first call for full study enrollment. Participants were randomized to one of 4 groups in the 2×2 design: mailed NRT (8 weeks versus none) and/or mHealth (yes versus no; stand-alone text program including links to videos and online content).
Main outcome measures: Self-reported 7-day point prevalence vaping abstinence at 3 months.
Results: A total of 981 participants were eligible and randomized; 508 (52%) fully enrolled by completing the first call. Enrolled participants were 71% female, 31% non-White, and 78% vaped daily. Overall, 74% completed the 3-month survey. Overall, 83% in the mailed NRT groups and 24% in the no-mailed NRT groups self-reported NRT use. Intent-to-treat 7-day point prevalence abstinence rates (missing assumed vaping) were 41% for calls only, 43% for Calls+mHealth, 48% for Calls+NRT, and 48% for Calls+NRT+mHealth. There were no statistically significant differences for mailed NRT (versus no-mailed NRT; OR=1.3; 95% CI=0.91, 1.84; p=0.14) or mHealth (versus no mHealth; OR=1.04; 95% CI=0.73, 1.47; p=0.84).
Conclusions: This quitline-delivered intervention was successful at helping young adults quit vaping, with almost half abstinent after 3 months. Higher than anticipated quit rates reduced power to identify significant group differences. Mailed NRT and mHealth did not significantly improve quit rates, in the context of an active control of a 2-call coaching program. Future research is needed to examine the independent effects of coaching calls, NRT, and mHealth in a fully-powered randomized control trial.
To read the full text of the article, please visit the publisher’s website.
Journal: Alcohol, 2025, doi: 10.1016/j.alcohol.2024.12.003
Authors: Nousha H. Sabet, & Todd A. Wyatt
Abstract:
Science is now in a new era of exposome research that strives to build a more all-inclusive, panoramic view in the quest for answers; this is especially true in the field of toxicology. Alcohol exposure researchers have been examining the multivariate co-exposures that may either exacerbate or initiate alcohol-related tissue/organ injuries. This manuscript presents selected key variables that represent the Alcohol Exposome. The primary variables that make up the Alcohol Exposome can include comorbidities such as cigarettes, poor diet, occupational hazards, environmental hazards, infectious agents, and aging. In addition to representing multiple factors, the Alcohol Exposome examines the various types of intercellular communications that are carried from one organ system to another and may greatly impact the types of injuries and metabolites caused by alcohol exposure. The intent of defining the Alcohol Exposome is to bring the newly expanded definition of Exposomics, meaning the study of the exposome, to the field of alcohol research and to emphasize the need for examining research results in a non-isolated environment representing a more relevant manner in which all human physiology exists.
To read the full text of the article, please visit the publisher’s website.
Journal: JAMA Network Open, 2025, doi: 10.1001/jamanetworkopen.2024.55165
Authors: Jean Ye, Saloni Mehta, Hannah Peterson, Ahmad Ibrahim, Gul Saeed, Sarah Linsky, … Dustin Scheinost
Abstract:
Importance: Opioid use disorder (OUD) impacts millions of people worldwide. Prior studies investigating its underpinning neural mechanisms have not often considered how brain signals evolve over time, so it remains unclear whether brain dynamics are altered in OUD and have subsequent behavioral implications.
Objective: To characterize brain dynamic alterations and their association with cognitive control in individuals with OUD.
Design, setting, and participants: This case-control study collected functional magnetic resonance imaging (fMRI) data from individuals with OUD and healthy control (HC) participants. The study was performed at an academic research center and an outpatient clinic from August 2019 to May 2024.
Exposure: Individuals with OUD were all recently stabilized on medications for OUD (<24 weeks). Main outcomes and measures: Recurring brain states supporting different cognitive processes were first identified in an independent sample with 390 participants. A multivariate computational framework extended these brain states to the current dataset to assess their moment-to-moment engagement within each individual. Resting-state and naturalistic fMRI investigated whether brain dynamic alterations were consistently observed in OUD. Using a drug cue paradigm in participants with OUD, the association between cognitive control and brain dynamics during exposure to opioid-related information was studied. Variations in continuous brain state engagement (ie, state engagement variability [SEV]) were extracted during resting-state, naturalistic, and drug-cue paradigms. Stroop assessed cognitive control.
Results: Overall, 99 HC participants (54 [54.5%] female; mean [SD] age, 31.71 [12.16] years) and 76 individuals with OUD (31 [40.8%] female; mean [SD] age, 39.37 [10.47] years) were included. Compared with HC participants, individuals with OUD demonstrated consistent SEV alterations during resting-state (99 HC participants; 71 individuals with OUD; F4,161 = 6.83; P < .001) and naturalistic (96 HC participants; 76 individuals with OUD; F4,163 = 9.93; P < .001) fMRI. Decreased cognitive control was associated with lower SEV during the rest period of a drug cue paradigm among 70 participants with OUD. For example, lower incongruent accuracy scores were associated with decreased transition SEV (ρ58 = 0.34; P = .008). Conclusions and relevance: In this case-control study of brain dynamics in OUD, individuals with OUD experienced greater difficulty in effectively engaging various brain states to meet changing demands. Decreased cognitive control during the rest period of a drug cue paradigm suggests that these individuals had an impaired ability to disengage from opioid-related information. The current study introduces novel information that may serve as groundwork to strengthen cognitive control and reduce opioid-related preoccupation in OUD.
To read the full text of the article, please visit the publisher’s website.
Source: https://drugfree.org/drug-and-alcohol-news/research-news-roundup-february-13-2025/
bJanuary 14, 2025
Forwarded by Shane Varcoe • 05.02.25

Addiction science has undergone tremendous progress over the past five decades, transforming our understanding of drugs and their impact on the brain and society. Recent advancements offer hope in addressing the escalating challenges of drug use, addiction, and overdose. However, the need for evidence-based prevention and treatment strategies remains crucial in combating this ongoing public health crisis.
Prevention is one of the most effective ways to combat substance use disorders. Research consistently highlights how drug exposure can interfere with brain development from prenatal stages to young adulthood, setting the stage for lifelong challenges. Children and adolescents are particularly vulnerable, as early drug experimentation sharply increases the risk of addiction later in life.
Adverse childhood experiences—ranging from poverty to trauma—also contribute to substance use risks by disrupting brain development. Preventative measures can mitigate these risks and promote resilience. For example, school-based programmes and community initiatives have demonstrated significant success in reducing drug use among young people. Importantly, these interventions offer long-term benefits, improving mental health and reducing dependency rates across generations.
Scaling up these preventative approaches is vital. By investing in evidence-based prevention at schools, healthcare facilities, and community centres, society can safeguard future generations from the devastating impacts of drugs.
One of the greatest hurdles today is the lack of access to effective addiction treatment. Millions of people struggle with substance use disorders, yet only a small percentage receive adequate care. This gap highlights the pressing need to expand addiction treatment services and eliminate barriers such as stigma and limited healthcare coverage.
Treatment options, including medication and behavioural therapies, have proven to be effective for many struggling with addiction. For instance, medications that address opioid dependency, combined with comprehensive care, can significantly improve recovery outcomes. However, these treatments remain inaccessible to many, especially in underserved communities.
Expanding treatment availability within prisons, rural areas, and low-income communities could swiftly reduce addiction rates and improve recovery success. Research also shows that offering treatment to individuals in justice systems can lower overdose risks after release and reduce reoffending, creating broader societal benefits.
Scientific advancements are paving the way for more effective solutions to addiction. New innovations, such as brain stimulation therapies, target the neurological circuits disrupted by substance use, offering promising pathways for treatment. Additionally, cutting-edge pharmaceuticals like GLP-1 agonists, already used for managing diabetes, are showing potential in reducing cravings and dependency behaviours associated with addiction.
The use of artificial intelligence (AI) in addiction science is further revolutionising the field. AI tools can help detect overdose patterns, study drug impacts on mental health, and even guide personalised treatment interventions. Large-scale studies, such as those examining adolescent brain development, continue to shed light on how substance use affects young minds, offering invaluable insights for effective prevention.
While remarkable progress has been made, the fight against addiction is far from over. Preventing drug use, providing accessible treatment, and investing in research remain paramount. By adopting a proactive, science-backed approach to addiction prevention, we can reduce the devastating effects of substance use disorders and create healthier, drug-free communities.
Addiction science offers the tools needed to address these challenges, but lasting change requires collective effort. Only through unified actions can we overcome this crisis and protect future generations from the harms of addiction.
Start prioritising prevention and treatment today to help build a safer, healthier world.
Source: https://wrdnews.org/breakthroughs-in-addiction-science-over-50-years/
THIS ARTICLE IS INCLUDED FOR ITS INTERESTING DESCRIPTION OF THE CONSUMPTION ROOM PHILOSOPHY AND PRACTICE. NDPA HAS SEVERAL SERIOUS CONCERNS ABOUT SO-CALLED ‘CONSUMPTION ROOMS’ AND WOULD TAKE ISSUE WITH SOME OF THE CLAIMS MADE IN THIS ARTICLE, NOT LEAST THE HEADLINE CLAIM THAT THIS IS A ‘SAFE’ SITE … (SEE OTHER ARTICLES ON THE NDPA SITE), NEVERTHELESS, IT IS WORTH READING, IN ORDER TO BETTER UNDERSTAND THE ATTITUDE BEHIND THE PROVENANCE OF SUCH FACILITIES.
At 8 a.m. on a Monday morning, most of the soft recliners in the waiting area of the three-story East Harlem overdose prevention center (OPC) are already occupied by those who have come to consume their first dose of the day. Whether it’s for fentanyl, heroin, or another drug, people of all ages trickle into the consumption room at OnPoint NYC, where mirrored cubicles line opposite sides of the room and a staff station sits in the middle with trays of needles, elastics, and wipes organized in rows.
A man, who looks to be in his late 30s, unwraps today’s first fix of what most likely is the opioid fentanyl, which staff say is the most common drug used here. He simultaneously chats with the staff who welcome each visitor with familiarity. The calm ambiance is occasionally punctuated with noise as the metal doors swing, allowing another person to enter.
OnPoint NYC, which opened in 2021 as the country’s first overdose prevention site, aims to be a judgment- and persecution-free space for drug users to safely consume. The idea of preventing people from dying of an overdose is a controversial one. Last year, former U.S. attorney for the southern district of New York Damian Williams told The New York Times that OnPoint’s methods were illegal and hinted at a shutdown, while New York Gov. Kathy Hochul is also opposed, having repeatedly said the centers violate federal and state laws, putting their future operations in the balance.
But amid the national opioid epidemic, drastic measures are needed. More than 100,000 people die each year from drug overdoses in the U.S., according to the National Center for Health Statistics. In November, President-elect Donald Trump announced plans to impose further tariffs on Chinese imports in an attempt to curb what he believes are fentanyl deliveries into the U.S. It follows calls in 2022 from President Joe Biden to increase funding in the budget to address the overdose epidemic, while in 2023 New York Times editors declared that the U.S. had lost the war on drugs.
“Every 90 minutes…four New Yorkers die [of an overdose],” said Sam Rivera, the executive director of OnPoint NYC.
Advocates for OPCs say having a sanitary and safe place to consume drugs diminishes the element of haste or need for discretion that might exist in a public place. This reduces the risk of an overdose, but should one occur, medically trained staff dressed in jeans and leather are ready to respond.
Despite the progress, the center, and the few others like it in the U.S., remain controversial. When a similar center was opened in San Francisco in 2022, a group of local mothers protested while others posited that creating safe spaces to consume drugs only increases drug use.
However, research found that following the opening of an OPC in San Francisco, there was no visible increase in drug use, and a Brown University study found no affiliation between the centers and increased crime.
Instead, Michel Kazatchkine, a commissioner of the Global Commission on Drug Policy (GCDP), which advocates for drug policies to be more humane and prioritize public and individual health, believes it is the current approach of criminalizing drug users that is the problem.
“The criminal justice approach has sent hundreds of thousands of people to prison with no benefit for these people and no benefit for the society and huge expenses involved,” said Kazatchkine, who is also the former executive director of the Global Fund to Fight AIDS, Tuberculosis and Malaria, France.
Over 1.16 million people each year are incarcerated in the U.S. on drug offenses, while globally, governments spend $100 billion annually on punitive drug policies. In spite of such policies, global drug use has risen from about 180 million people in 2002 to 292 million in 2022, according to a report by the GCDP.
In states like New York, the response to tackle the drug problem has predominantly been to fund the distribution of naloxone and fentanyl test strips, which can detect the presence of fentanyl in other drugs, explained Toni Smith, the New York state director at Drug Policy Alliance. The group works with grassroots groups to advance public health solutions to drug use. While such resources are critical, Smith emphasized that the state must offer a full range of life-saving tools and services. More OPCs, Smith believes, could save more lives.
Historically, the U.S. has pushed back on any initiatives under the harm reduction umbrella, Kazatchkine said. Harm reduction, according to the World Health Organization (WHO), focuses on offering a suite of interventions designed to minimize the negative impacts related to drug use. That could include providing people with clean needles and syringes, with naloxone, with HIV testing, or with access to opioid substitution therapy programs. OPCs—often referred to as safe consumption sites in Europe, where they are widely used—are not on the WHO’s list of recommended harm reduction interventions but are a harm reduction approach.
“The concept of harm reduction is acknowledging that people use drugs and that these people have risks, but it is prioritizing health approaches over criminalization,” Kazatchkine said. “Acknowledging that people use drugs, you acknowledge something that is prohibited under the law and actually under criminal law, so a government or an international entity finds itself in a very uncomfortable situation.”
“Many people would come in and be shocked…They open the door and think everybody’s just using drugs. They don’t expect this kind of structure and loving environment,” he said. “We’ve invited the governor for three years. [She] hasn’t been here once. But you’re going to sit around and tell us the program doesn’t work.”
More than just a consumption space, the center offers a health clinic and, up a narrow staircase to a second floor, therapy rooms host complimentary holistic treatments such as reiki, massage, and sound baths. Rivera himself occasionally hosts one. All services, including health care, are free.
On this day, a woman sleeps deeply in a reclining chair as soft music tinkles in the background and candles burn in the corner; two others lie on massage tables awaiting their treatments. Shower facilities are available in another corner of the center, and an on-site psychologist offers mental health services in a bid to help tackle the underlying trauma behind the addiction. It’s “multidimensional” support to treat a problem that surpasses simply addiction but intersects with issues around housing, access to care, criminalization, food and nutrition, sleep, as well as structural racism, Smith said. And the services aren’t just for drug users but all local community members.
“Creating this community and this space around a loving environment is so impactful, and it changes the experience for folks who come in,” Rivera said.
In New York City, Rivera believes there have also been economic benefits. OnPoint’s data suggests a reduction in visits to the emergency room for overdoses that has relieved the burden on the health system and, Rivera said, potentially saved two New York City neighborhoods $45 million in less than three years.
More OPCs could benefit the U.S. and reduce the impact the drug crisis is having, said Kazatchkine, but amid what Rivera believes is a game of politics, whether that will happen remains to be seen. In the meantime, elsewhere in the U.S., people will shoot up in alleyways and parks, at increased risk of unnecessarily overdosing. But the reality, Rivera said, is that with OPCs, there’s the potential for no one to have to die this way again.
Source: https://www.nationofchange.org/2024/12/24/inside-the-countrys-first-official-safe-drug-consumption-site/
The Welfare and Peace Society, City University of Science and Information Technology (CUSIT) in collaboration with the Higher Education Regulatory Authority (HERA), Anti-Narcotic Force Pakistan and Anti-Drug Social Welfare Organization had hosted the seminar.
It was part of the efforts to promote peace through combating drug abuse in educational institutes. The activity was under the “Community Resilience Building for Countering Violent Extremism” project.
European Union funds the project. Collaboration is struck with the National Counter-Terrorism Authority and the UN Office on Drugs Crime Country. Key speakers of the seminar included Azazud Din, the HERA Advisor for Drug Use Prevention/Lead Policies, Umair, the Da Haq Awaz organization’s member, Fukhraz of Anti-Narcotic Force, Ikram of Khyber Pakhtunkhwa Centre of Countering Violence Extremism, and Ms Maria of the HERA.
Source: https://www.thenews.com.pk/print/1276828-strategies-shared-for-drug-prevention
Prevention is key, and we cannot forget that today’s marijuana is highly potent. In 2025 and beyond, federal agencies must prioritize public health and safety and work to undo legalization’s harmful consequences.
The Department of Health and Human Services (HHS) is positioned to implement a wide range of policy initiatives to prevent marijuana use and hold the industry accountable. For example, marijuana legalization has re-elevated the conversation about second-hand smoke. California recently passed a law permitting “cannabis cafes” in which users can openly smoke marijuana. Second-hand marijuana smoke has been found to be more harmful than second-hand tobacco smoke and contains many of the same cancer-causing substances. Our country has legally and culturally rejected indoor cigarette smoking. HHS must stand on science and reject indoor marijuana smoking by publishing strict guidelines prohibiting it, just as it did with indoor cigarette smoking.
Transparency within the “medical” marijuana industry is also desperately needed. As it did with opioids, HHS should create a registry of medical marijuana recommendation practices and make the information available to the public. The database could include information regarding regional breakdowns, a list of overprescribing doctors, and pot-industry kickbacks received by doctors.
Sunlight is the best disinfectant when it comes to quack doctors. In August, a Spotlight PA article uncovered Pennsylvania medical pot doctors who were doling out thousands of medical marijuana cards per year. These are similar to the “pill mills” that fueled the opioid epidemic.
Last year, the Food and Drug Administration (FDA) bucked federal legal precedent around marijuana rescheduling by inventing new, lower standards. Its flawed marijuana rescheduling review was designed to permit marijuana rescheduling. The ramifications of changing this precedent aren’t limited to marijuana; other dangerous drugs (e.g., psychedelics) could be reclassified to a lower schedule based on the new lax standards. HHS should issue internal agency guidance that advises FDA to adhere to the established five-factor test for determining currently accepted medical use. This will ensure that drug scheduling, which has direct implications for the availability of drugs, remains science based.
The Trump-Vance administration must soundly reject moving marijuana from Schedule I to Schedule III for one simple reason: marijuana fails to meet the legal definition of a Schedule III drug. It has not been approved by the FDA for the treatment of any disease or condition. Moving marijuana to Schedule III is a handout to corporations, as it would allow companies to deduct advertising and other expenses from their taxes, fueling the growth of an industry that profits from addiction.
Far from being a legitimate medicine, marijuana is harming the millions of Americans who misuse it. Given that 3 in 10 users develop a marijuana use disorder, better known as addiction to marijuana, the incoming administration needs to focus on helping connect Americans to treatment.
Federal law enforcement also plays a crucial role in curbing marijuana legalization and its effects. In 2013, the Obama administration issued the Cole Memo, a document that cemented the federal government’s non-enforcement policy on marijuana. The first Trump administration rescinded the memo, but more must be done to enforce federal laws already on the books. The Justice Department has the power to prevent distribution to minors, curtail drugged driving, and investigate state-legal dispensaries being used as a cover for illegal drug trafficking—all things the Obama administration promised to do. By beginning with this targeted enforcement strategy, law enforcement can shut down the operations of the industry’s worst actors.
To promote public safety, the Trump-Vance administration should also crack down on illegal marijuana grows, particularly those in remote areas on federal lands. These operations are often controlled by cartels and poison the surrounding natural environment with toxic chemicals.
We also need a new national anti-drug media campaign, updated for the 21st century. This campaign must broadcast messages widely through traditional and social media and talk about the dangers and truth behind the use of drugs. The Office of National Drug Control Policy (ONDCP), the drug policy office within the White House, has a key role to play, too, particularly in drug use prevention. ONDCP helps oversee the Drug-Free Communities Support Program, which is responsible for much of our federally funded drug prevention work. In an era in which drugs are sold and marketed via social media, it’s more important than ever that effective anti-drug prevention messages reach young people. ONDCP also oversees the High Intensity Drug Trafficking Areas program, which forms a crucial partnership between local, state, and federal law enforcement to curtail drug trafficking. Both these programs’ funding should be protected and prioritized.
A good strategy must focus on all drugs, but we can’t ignore the politically inconvenient ones. If President Trump wants to make America healthy again, the conversation must include marijuana, a drug with an addiction rate of up to 30 percent that is being pushed by a profit-driven industry that desperately needs federal accountability.
Dr. Kevin Sabet is the President of Smart Approaches to Marijuana (SAM) and the Foundation for Drug Policy Solutions (FDPS) and a former White House drug policy advisor to Presidents Obama, Bush and Clinton.
SOURCE: https://www.newsweek.com/making-america-healthy-again-must-start-better-drug-policy-opinion-2014657
Public News Service – Terri Dee, Anchor/Producer – Monday, January 6, 2025
One popular New Year’s resolution is to quit alcohol consumption.
Although easier said than done, one recovery center said there are modifications to try if previous attempts are not working. A good start is taking a hard look at what has worked and what has not.
Marissa Sauer, a licensed clinical addiction counselor at Avenues Recovery, a Fort Wayne recovery center, pointed out if there was a simple answer, everybody would use it. She added other influences are linked to alcohol and substance abuse.
“There’s genetics. Were my parents and my grandparents struggling with substances? Does someone have maybe adverse childhood experiences that have led to substances being a coping mechanism of some kind?” Sauer explained. “Maybe there are these mental health diagnoses.”
Sauer mentioned people, places, or things which could inhibit or enable someone to abuse drugs or alcohol, making it complicated to simply walk away. Medication, therapy or conversations with people who have beaten their addictions are all effective measures for recovery.
The US Surgeon General’s 2025 Advisory Report indicates alcohol consumption is the third leading preventable cause of cancer after tobacco and obesity and the public is taking notice.
There is a growing momentum of the “sober curious” movement, avoiding happy hours at bars, ordering a low or no-alcohol drinks known as mocktails, or completely abstaining from alcohol for 30 days for “dry January.” Sauer said longtime substance abusers fear change and she wants them to know there is hope.
“Whether you’re 21 or whether you’re 51, that ability to heal is there,” Sauer emphasized. “The best gift that you could give yourself for a healthy 2025 is to give your loved ones the absolute best version of yourself.”
An Indiana State Epidemiological report from 2021-2022 revealed almost 24% of residents aged 12 and older have participated in binge drinking, with the highest rate among young adults aged 18 to 25.
Source: https://www.publicnewsservice.org/2025-01-06/alcohol-and-drug-abuse-prevention/in-substance-recovery-center-supports-sober-existence/a94456-1
Alcohol is the leading driver of substance use-related fatalities in America: Each year, frequent or excessive drinking causes approximately 178,000 deaths.1 Excessive alcohol use is common in the United States among people who drink: In 2022, of the 137 million Americans who reported drinking in the last 30 days, 45% reported binge drinking (five or more drinks in a sitting for men; four for women).2 Such excessive drinking is associated with health problems such as injuries, alcohol poisoning, cardiovascular conditions, mental health problems, and certain cancers.3
In 2020, many people increased their drinking because of COVID-19-related stressors, including social isolation, which led to a 26% increase in alcohol-related deaths during the first year of the pandemic.4

Growth is driven by increases in both acute and chronic causes of death
Stacked bar graph shows yearly increases in alcohol-related deaths attributed to both chronic and acute causes from 2016-17 through 2020-21. Deaths related to chronic causes increased from approximately 89,000 to approximately 117,000 (a 32% increase), while acute deaths increased from approximately 49,000 to approximately 61,000 (a 24% increase).
Notes: Chronic causes of death include illness related to excessive alcohol use such as cancer, heart disease, and stroke, and diseases of the liver, gallbladder, and pancreas. Acute causes include alcohol-related poisonings, car crashes, and suicide.
Source: Marissa B. Esser et al., “Deaths From Excessive Alcohol Use—United States, 2016-2021,” Morbidity and Mortality Weekly Report 73, no. 8154-61, https://www.cdc.gov/mmwr/volumes/73/wr/mm7308a1.htm#T1_down
© 2024 The Pew Charitable Trusts
Nationwide, nearly 30 million people are estimated to have alcohol use disorder (AUD); it is the most common substance use disorder. AUD is a treatable, chronic health condition characterized by a person’s inability to reduce or quit drinking despite negative social, professional, or health effects.5 While no single cause is responsible for developing AUD, a mix of biological, psychological, and environmental factors can increase an individual’s risk, including a family history of the disorder.6
There are well-established guidelines for AUD screening and treatment, including questions that can be asked by a person’s health care team, medications approved by the U.S. Food and Drug Administration (FDA), behavioral therapies, and recovery supports, but these approaches often are not put into practice.7 When policies encourage the adoption of screening and evidence-based medicines for AUD, particularly in primary care, the burden of alcohol-related health problems can be reduced across the country.8
For adults of legal drinking age, U.S. dietary guidelines recommend that they choose not to drink or drink in moderation, defined as two drinks or fewer in a day for men, and one drink or fewer in a day for women.9 One drink is defined as 0.6 ounces of pure alcohol—the amount in a 12-ounce beer containing 5% alcohol, a 5-ounce glass of wine containing 12% alcohol, or 1.5 ounces of 80-proof liquor.10
Consumption patterns exceeding these recommended levels are considered:
Alcohol use disorder is defined by The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) as having symptoms of two or more diagnostic criteria within a 12-month period.13 The diagnostic criteria assess behaviors such as trying to stop drinking but being unable to, alcohol cravings, and the extent to which drinking interferes with an individual’s life.14 AUD can be mild (meeting two or three criteria), moderate (meeting four or five criteria), or severe (six or more criteria).15
Primary care providers are well positioned to recognize the signs of unsafe drinking in their patients. The U.S. Preventive Services Task Force recommends that these providers screen adults 18 years and older for alcohol misuse.16 One commonly used evidence-based approach, SBIRT—or screening, brief intervention, and referral to treatment—is a series of steps that help providers identify and address a patient’s problematic substance use.17
Using a screening questionnaire, a provider can determine whether a patient is at risk and, if so, can deliver periodic brief behavioral interventions in an office setting. Such interventions have been shown to reduce heavy alcohol use among adolescents, adults, and older adults.18 When a patient meets the criteria for AUD, providers can offer medication, connect them to specialty treatment, refer them to recovery supports such as Alcoholics Anonymous or other mutual-help groups, or all of the above, depending on a patient’s needs and preferences.19 When these interventions are used in primary care settings, they can reduce heavy alcohol use.20
While screening for AUD is common, few providers follow up when a patient reports problematic alcohol use. From 2015 to 2019, 70% of people with AUD were asked about their alcohol use in health care settings, but just 12% of them received information or advice about reducing their alcohol use.21 Only 5% were referred to treatment.22
Emergency departments (EDs) are another important setting for identifying AUD, and to maintain accreditation they are required to screen at least 80% of all patients for alcohol use.23 Alcohol is the most common cause of substance-related ED visits, meaning many people in these settings are engaged in excessive or risky alcohol consumption and could be linked to care.24
The use of SBIRT in the ED can also reduce alcohol use, especially for people without severe alcohol problems.25 Providers who use SBIRT can help patients reduce future ED visits and also some negative consequences associated with alcohol use, such as injuries.26
Commonly cited barriers to using SBIRT in these health care settings include competing priorities and insufficient treatment capacity in the community when patients need referrals. Conversely, SBIRT use increases with strong leadership and provider buy-in, collaboration across departments and treatment settings, and sufficient privacy to discuss substance use with patients.27
Jails and prisons should also screen for AUD, as well as other SUDs, to assess clinical needs and connect individuals with care. However, screening practices may not be evidence based. A review of the intake forms used to screen individuals in a sample of jails in 2018-19 found that some did not ask about SUD at all, and of those that did, they did not use validated tools accepted for use in health care and SUD treatment settings.28
Up to half of all people with AUD experience some withdrawal symptoms when attempting to stop drinking.29 For many, common symptoms such as anxiety, sweating, and insomnia are mild.30 For a small percentage, however, withdrawal can be fatal if not managed appropriately.31 These individuals can experience seizures or a condition called alcohol withdrawal delirium (also referred to as delirium tremens), which causes patients to be confused and experience heart problems and other symptoms; if untreated, it can be fatal.32 People with moderate withdrawal symptoms can also require medical management to address symptoms such as tremors in addition to anxiety, sweating, and insomnia.33
To determine whether a patient with AUD is at risk of severe withdrawal or would benefit from help managing symptoms, the American Society of Addiction Medicine recommends that providers evaluate patients with positive AUD screens for their level of withdrawal risk.34 Based on this evaluation, providers can offer or connect patients to the appropriate level of withdrawal management.35
At a minimum, high-quality withdrawal management includes clinical monitoring and medications to address symptoms.36 Providers may also offer behavioral therapies.37 Depending on the severity of a patient’s symptoms and the presence of co-occurring conditions such as severe cardiovascular or liver disease that require a higher level of care, withdrawal management can be provided on either an inpatient or an outpatient basis.38
According to the U.S. Department of Justice’s Bureau of Justice Assistance and the National Institute of Corrections, jails should also use evidence-based standards of care to address alcohol withdrawal. These standards include screening and assessing individuals who are at risk for withdrawal and, if the jail cannot provide appropriate care, transferring them to an ED or hospital.39
Withdrawal management on its own is not effective in treating AUD, and without additional services after discharge, most people will return to alcohol use.40 Because of this, providers should also connect people with follow-up care, such as residential or outpatient treatment, after withdrawal management to improve outcomes. Continued care helps patients sustain abstinence, reduces their risk of arrests and homelessness, and improves employment outcomes.41
Patients face multiple barriers to this follow-up care, however. For example, withdrawal management providers from the Veterans Health Administration cited long wait times for follow-up care, inadequate housing, and lack of integration between withdrawal management and outpatient services as reasons patients couldn’t access services.42 Patients have also cited barriers such as failure of the withdrawal management provider to arrange continued care, lengths of stay that were too short to allow for recovery to begin, insufficient residential treatment capacity for continued care, and inadequate housing.43
Promising practices for improving care continuity include: providing peer recovery coaches—people with lived expertise of substance use disorder who can help patients navigate treatment and recovery; psychosocial services that increase the motivation to continue treatment; initiating medication treatment before discharge; reminder phone calls; and “warm handoffs,” in which patients are physically accompanied from withdrawal management to the next level of care.44
In 2023, 29 million people in the U.S. met the criteria for AUD, but less than 1 in 10 received any form of treatment.45 Formal treatment may not be necessary for people with milder AUD and strong support systems.46 But people who do seek out care can face a range of barriers, including stigma, lack of knowledge about what treatment looks like and where to get it, cost, lack of access, long wait times, and care that doesn’t meet their cultural needs.47
For those who need it, AUD treatment can include a combination of behavioral, pharmacological, and social supports designed to help patients reach their recovery goals, which can range from abstaining from alcohol to reducing consumption.48
While for many the goal of treatment is to stop using alcohol entirely, supporting non-abstinence treatment goals is also important, because reduced alcohol consumption is associated with important health benefits such as lower blood pressure, improved liver functioning, and better mental health.49
Services for treating AUD—including medication and behavioral therapy—can be offered across the continuum of care, from primary care to intensive inpatient treatment, depending on a patient’s individual needs.50
Medications for AUD help patients reduce or cease alcohol consumption based on their individual treatment goals and can help improve health outcomes.51 Medications can be particularly helpful for people experiencing cravings or a return to drinking, or people for whom behavioral therapy alone has not been successful.52 But medications are not often used: Of the 30 million people with AUD in 2022, approximately 2% (or 634,000 people) were treated with medication.53
The FDA has approved three medications to treat AUD:
Additionally, some medications used “off-label” (meaning they were approved for treating other conditions) have also effectively addressed AUD. A systematic review found that topiramate, a medication approved for treating epilepsy and migraines, had the strongest evidence among off-label drugs for reducing both any drinking and heavy drinking days.68 Like naltrexone, it can reduce the incidence of alcohol-related liver disease.69
Despite the benefits that medications provide, they remain an underutilized tool for a variety of reasons—such as lack of knowledge among patients and providers, stigma against the use of medication, and failure of pharmacies to stock the drugs.70
Behavioral therapies can also help individuals manage AUD, and they support medication adherence:
All of these approaches can help address AUD, and no one treatment has proved more effective than another in treating this complicated condition.76 Combining behavioral therapies with other approaches such as medication and recovery supports, as described below, can improve their efficacy.77
Peer support specialists and mutual-help groups can also help people achieve their personal recovery goals:
People with AUD can use recovery supports on their own, in combination with behavioral treatment or medication, or as a method to maintain recovery when leaving residential treatment or withdrawal management.82
While the U.S. records more than 178,000 alcohol-related deaths each year, some populations have a higher risk of alcohol-related deaths, and others face greater barriers to treatment.83
Despite seeking treatment at higher rates than other racial/ethnic groups, American Indian and Alaska Native people have the highest rate of alcohol-related deaths.84
Alcohol‑related deaths per 100,000 people

A clustered column chart displays the rate of alcohol-related deaths per 100,000 people by racial and ethnic group for four years: 2012, 2016, 2019, and 2022. While the chart shows increasing rates for all included racial and ethnic groups (American Indian/Alaska Native, White, Hispanic, Black, and Asian or Pacific Islander), the mortality rates are highest each year for American Indian/Alaska Natives.
© 2024 The Pew Charitable Trusts View image
Risk factors that impact these communities and can contribute to these deaths include historical and ongoing trauma from colonization, the challenges of navigating both native and mainstream American cultural contexts, poverty resulting from forced relocation, and higher rates of mental health conditions than in the general population.85 Substances, including alcohol, are sometimes used to cope with these challenges.86
However, American Indian/Alaska Native communities also have rich protective factors such as their cultures, languages, traditions, and connections to elders, which can help reduce negative outcomes associated with alcohol use, especially when treatment services incorporate and build on these strengths.87
For example, interviews with American Indian/Alaska Native patients with AUD in the Pacific Northwest revealed that many participants preferred Native-led treatment environments that incorporated traditional healing practices and recommended the expansion of such services.88
To improve alcohol-related outcomes for American Indians and Alaska Natives, policymakers and health care providers must develop a greater understanding of the barriers and strengths of these diverse communities and support the development of culturally and linguistically appropriate services. The federal Department of Health and Human Services Office of Minority Health defines such an approach as “services that are respectful of and responsive to the health beliefs, practices, and needs of diverse patients.”89
Rural communities are another group disproportionately affected by AUD. People living in rural areas have higher alcohol-related mortality rates than urban residents but are often less likely to receive care.90 They face treatment challenges including limited options for care; concerns about privacy while navigating treatment in small, close knit communities; and transportation barriers.91
2012‑22 change in alcohol‑induced death rate per 100,000 by urban and rural areas

A graph with four bars shows the increase in alcohol-related deaths per 100,000 people in urban and rural areas from 2012 to 2022. In urban areas, the rate increased from 8.6 to 14.9 per 100,000 people, a 73% increase. In rural areas, the rate increased from 10.1 to 19.6 per 100,000 people, a 94% increase.
Telemedicine can help mitigate these barriers to care.92 Cognitive behavioral therapy and medications for AUD can be delivered effectively in virtual settings.93 People with AUD can also benefit from virtual mutual-help meetings, though some find greater value in face-to-face gatherings.94
Despite the value of virtual care delivery, people living in rural areas also often have limited access to broadband internet, which can make these interventions challenging to use.95 Because of this, better access to in-person care is also needed.
To improve screening and treatment for patients with AUD, policymakers, payers, and providers should consider strategies to:
AUD is a common and treatable health condition that often goes unrecognized or unaddressed. Policymakers can improve the health of their communities by supporting providers in increasing the use of evidence-based treatment approaches.98
If you are concerned about your alcohol consumption, you can use the Check Your Drinking tool created by the Centers for Disease Control and Prevention to assess your drinking levels and make a plan to reduce your use.
Source: https://www.pewtrusts.org/en/research-and-analysis/fact-sheets/2024/12/americas-most-common-drug-problem-unhealthy-alcohol-use
OPENING STATEMENT BY AUTHOR: Dec 31, 2024
Drug Free Australia has launched a new Substack where we start out with the foundational failure of Australia’s 1985 Harm Minimisation experiment which has literally seen thousands of families (5,400 between 2000 and 2007 alone) needlessly grieving for a lost loved one – all directly as a result of our adoption of Harm Reduction measures. If you think this is fanciful, you need to look at the cold, hard evidence.
If you live in another country, this is precisely a drug policy approach you need to fight to avoid and you may need to use this data to do it.
Gary Christian, President, Drug Free Australia. Phone: 0422 163 141


Meant to reduce drug-related deaths and harm, Australia’s mortality quadrupled during the first 14 years from around 250 deaths in 1984 to 1,116 in 1999.

Looking at United Nations’ Drug Report figures for all countries worldwide, by 1998 Australia had the highest drug use amongst OECD countries, almost double that of the third, fourth and fifth highest countries. Only New Zealand, in second place, came close, having also adopted Harm Reduction programs in 1987
In 1998, the Federal Government, responding to community alarm at the unacceptable mortality, introduced a new approach called Tough on Drugs. Quadrupling the drugs budget to focus on prevention messaging, heavily expanded rehab and better policing of borders saw use of any illicit drug decrease by 39% and overdose deaths plummet by 67% by 2001, which is where mortality remained for 7 years. Throughout this period the Government chose not to close any Harm Reduction programs, which in light of this analysis, were simply running interference as an impediment to even better outcomes.
Nevertheless, this drug policy approach over a nine year period acted as a control by which the other two periods of Harm Reduction ascendency can be judged.
With a new Federal Government scrapping Tough on Drugs in 2007, prevention and rehab took a back seat, although heroin supply at the borders remained suppressed. And what happened was a virtual repeat of the first Harm Reduction era, demonstrating the same harm-multiplying dynamic. Yet with this official government graph below (with our added commentary overlaid) there is more to see than with the previous data.
In the decade following 2007 opiate deaths increased 260%, while other illicits drugs contributing to overdose deaths each increased 210%-590%. The reinstatement of a Harm Reduction priority was clearly a tide that lifted all boats.
We therefore find it conclusive that Harm Reduction has very demonstrably, substantially and consistently multiplied drug-related deaths and harm in this country.
Harm Reduction proponents will invariably claim that there is some hidden confounder that invalidates any conclusion, but the lockstep rise and fall of all drug types in concert with the differing drug policy eras rules out any major change in supply for any illicit (barring the 2000 heroin drought), just as it does with any possibility of a change in definition of a drug-related death. There are no viable confounders.
What is clear is that drug prevention and rehabilitation, as the first demand reduction pillar of Australia’s ‘Harm Minimisation’ approach, along with supply reduction at our borders, are both undermined by any ‘safe use of illicit drugs’ programming which is an explicit and implicit message of any harm reduction intervention.
Australia has given the world the gift of a viable ‘control’ drug policy period which ably shows the devastation caused by Harm Reduction.
It is time for the world to stand up and take notice. Hundreds of thousands of lives will be saved each year when all countries, including Australia, follow the lead of Australia’s Tough on Drugs policy.
___________________________________
** Harm Reduction, by definition, has no vested interest in drug prevention.

Source: https://open.substack.com/pub/drugfreeaustralia/p/how-harm-reduction-devastated-australia?r=1hnlai&utm_campaign=post&utm_medium=web
A study of nearly 10,000 adolescents funded by the National Institutes of Health (NIH) has identified distinct differences in the brain structures of those who used substances before age 15 compared to those who did not. Many of these structural brain differences appeared to exist in childhood before any substance use, suggesting they may play a role in the risk of substance use initiation later in life, in tandem with genetic, environmental, and other neurological factors.
This adds to some emerging evidence that an individual’s brain structure, alongside their unique genetics, environmental exposures, and interactions among these factors, may impact their level of risk and resilience for substance use and addiction. Understanding the complex interplay between the factors that contribute and that protect against drug use is crucial for informing effective prevention interventions and providing support for those who may be most vulnerable.”
Nora Volkow M.D., Director of NIDA
Among the 3,460 adolescents who initiated substances before age 15, most (90.2%) reported trying alcohol, with considerable overlap with nicotine and/or cannabis use; 61.5% and 52.4% of kids initiating nicotine and cannabis, respectively, also reported initiating alcohol. Substance initiation was associated with a variety of brain-wide (global) as well as more regional structural differences primarily involving the cortex, some of which were substance-specific. While these data could someday help inform clinical prevention strategies, the researchers emphasize that brain structure alone cannot predict substance use during adolescence, and that these data should not be used as a diagnostic tool.
The study, published in JAMA Network Open, used data from the Adolescent Brain Cognitive Development Study, (ABCD Study), the largest longitudinal study of brain development and health in children and adolescents in the United States, which is supported by the NIH’s National Institute on Drug Abuse (NIDA) and nine other institutes, centers, and offices.
Using data from the ABCD Study, researchers from Washington University in St. Louis assessed MRI scans taken of 9,804 children across the U.S. when they were ages 9 to 11 – at “baseline” – and followed the participants over three years to determine whether certain aspects of brain structure captured in the baseline MRIs were associated with early substance initiation. They monitored for alcohol, nicotine, and/or cannabis use, the most common substances used in early adolescence, as well as use of other illicit substances. The researchers compared MRIs of 3,460 participants who reported substance initiation before age 15 from 2016 to 2021 to those who did not (6,344).
They assessed both global and regional differences in brain structure, looking at measures like volume, thickness, depth of brain folds, and surface area, primarily in the brain cortex. The cortex is the outermost layer of the brain, tightly packed with neurons and responsible for many higher-level processes, including learning, sensation, memory, language, emotion, and decision-making. Specific characteristics and differences in these structures – measured by thickness, surface area, and volume – have been linked to variability in cognitive abilities and neurological conditions.
The researchers identified five brain structural differences at the global level between those who reported substance initiation before the age of 15 and those who did not. These included greater total brain volume and greater subcortical volume in those who indicated substance initiation. An additional 39 brain structure differences were found at the regional level, with approximately 56% of the regional variation involving cortical thickness. Some brain structural differences also appeared unique to the type of substance used.
While some of the brain regions where differences were identified have been linked to sensation-seeking and impulsivity, the researchers note that more work is needed to delineate how these structural differences may translate to differences in brain function or behaviors. They also emphasize that the interplay between genetics, environment, brain structure, the prenatal environment, and behavior influence affect behaviors.
Another recent analysis of data from the ABCD study conducted by the University of Michigan demonstrates this interplay, showing that patterns of functional brain connectivity in early adolescence could predict substance use initiation in youth, and that these trajectories were likely influenced by exposure to pollution.
Future studies will be crucial to determine how initial brain structure differences may change as children age and with continued substance use or development of substance use disorder.
“Through the ABCD study, we have a robust and large database of longitudinal data to go beyond previous neuroimaging research to understand the bidirectional relationship between brain structure and substance use,” said Alex Miller, Ph.D., the study’s corresponding author and an assistant professor of psychiatry at Indiana University. “The hope is that these types of studies, in conjunction with other data on environmental exposures and genetic risk, could help change how we think about the development of substance use disorders and inform more accurate models of addiction moving forward.”
Miller, A. P., et al. (2024). Neuroanatomical Variability and Substance Use Initiation in Late Childhood and Early Adolescence. JAMA Network Open. doi.org/10.1001/jamanetworkopen.2024.52027.
Source: https://www.news-medical.net/news/20241230/Structural-brain-differences-in-adolescents-may-play-a-role-in-early-initiation-of-substance-use.aspx
Published: December 31, 2024
DOI: 10.7759/cureus.76659
This is a large article. To access the full document:
There is undoubtedly an alarmingly rising trend of substance use among older adults. This has necessitated a paradigm shift in healthcare and propelled strategies aimed at effective prevention and screening. Age-related physiological changes, such as diminished metabolism and increased substance sensitivity, make older adults particularly vulnerable to adverse effects of substances. This not only has adverse psychological consequences but also physical consequences like complicating chronic illnesses and harmful interactions with medications, which lead to increased hospitalization.
Standard screening tools can identify substance use disorders (SUDs) in older adults. Tools like the Cut-down, Annoyed, Guilty, and Eye-opener (CAGE) questionnaire and Michigan Alcohol Screening Test-Geriatric (MAST-G) are tailored to detect alcoholism, while the Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST) and Alcohol Use Disorders Identification Test (AUDIT) assess abuse of illicit and prescription drugs. Since older adults are more socially integrated, screening should be done using non-stigmatizing and non-judgmental language.
Prevention strategies include educational programs, safe prescribing practices, and prescription drug monitoring. Detection of substance abuse should be followed by brief interventions and specialized referrals. In conclusion, heightened awareness, improved screening, and preventive measures can mitigate substance abuse risks in this demographic. Prioritizing future research on non-addictive pain medications and the long-term effects of substances like marijuana seems justified.
Such experiences contribute to a feeling that research is a one-way transaction benefiting scientists but giving little back to the community. Lack of meaningful community engagement also compromises the quality of the science by not incorporating the valuable ideas and insights of people who use drugs.
NIDA is committed to improving community engagement in all parts of the research process. For that reason, we have asked the National Advisory Council on Drug Abuse (NACDA)—the body of experts that advises on NIDA’s scientific research priorities—to convene a working group to recommend ways to enhance the meaningful engagement of people who have experience with drug use in the research our Institute funds. The workgroup will inform the creation of resources that outline NIDA’s expectations regarding community engagement and help both applicants and community partners navigate this critical work.
NIDA has long encouraged community-engaged research, and it is required element in various NIDA research funding opportunities, including those supported through our Racial Equity Initiative. The evolving opioid overdose crisis has underscored the importance of ensuring that people’s lived experience of substance use is centered in the science we support. For example, one of the pillars of the NIH Helping to End Addiction Long-term (HEAL) Initiative is that research must be relevant and responsive to the individuals, families, and communities it aims to help. One way HEAL studies are doing this is by drawing on the input of community advisory boards to ensure that the research is best tailored to the needs of the people most impacted by it.
The NIDA-funded Harm Reduction Research Network is a nationwide set of projects to enhance the impact of harm-reduction efforts, and its community advisory boards have already helped shape some of the studies. One project involves the development of a survey instrument to capture experiences of people who use drugs, and advisory board members helped tailor the wording of the instrument so that it reflected language more likely to be used by people who use drugs. Another study aimed at reducing overdose and increasing engagement in harm reduction and treatment services had originally been limited to people who use methamphetamine. Based on the input of advisors with more up-to-date knowledge of drug-use in their community, the study was broadened to include people who use cocaine, as that was identified as an emerging stimulant in their area.
The Integrative Management of Chronic Pain and OUD for Whole Recovery (IMPOWR) project is addressing the needs of people with substance use disorders and pain via a network of multidisciplinary team science collaborations. Its community advisory boards weigh in on funding decisions for pilot studies, and some of these studies have included a community partner as a co-investigator. Based on community input about the important role of PTSD and discrimination in healthcare settings in pain and opioid misuse and addiction, IMPOWR researchers added PTSD and stigma/discrimination items to their common data elements (the standardized questions that facilitate data-sharing across studies).
The Native Collective Research Effort to Enhance Wellness (NCREW) Initiative is partnering with Tribal organizations to support community-driven research projects that address opioid misuse and pain in Native communities. By providing needed training, technical assistance, and tools, the NCREW project is building capacity within Native communities to conduct locally prioritized research that incorporates indigenous knowledge and lived experience, with the aim of building effective, sustainable, and strengths-based interventions.
As outlined in NIDA’s Strategic Plan, NIDA is committed to partnering with people with lived and living experience in the development of new treatments for substance use disorder. Consistent with that goal, NIDA is funding four Patient Engagement Resource Centers (PERCs) to test various models of patient engagement that can inform research on SUD treatment services. Each PERC will recruit members of a particular patient population to understand what prevents them from finding or receiving evidence-based treatment services. This information will be used to pilot test patient-informed solutions to these challenges that can ultimately serve as models for the development of interventions in other settings.
There are many other ways that partnering with people with living experience of substance use could benefit both science and the community. Surveillance is one example. The drug market is rapidly changing, and people who actively use drugs and live this reality are best poised to provide information on the drug supply and its effects. And through their engagement in surveillance efforts, participants could gain information on new adulterants and contaminants that could help inform their own decisions.
In these, as with other research efforts, people who use drugs need to be treated with respect, and their confidentiality must be protected. They must also be compensated fairly for their time, their input, and their commuting and childcare costs.
Including people with experience of substance use and addiction in the scientific workforce—and making sure they feel safe and recognized as valuable members of the research team—must also become a priority for our science. As some of my colleagues at NIDA’s Intramural Research Program argued two years ago in the Journal of Addiction Medicine, people with lived and living experience of substance use disorders have unique perspectives that are invaluable in making sure that the right research questions are asked.
These are just some of the possible topics that may be discussed in the new NACDA workgroup. For that group, we are seeking individuals who identify as having experience with substance use or a substance use disorder or as a family or caregiver of someone who does. Participants will meet virtually three or four times during 2025 and potentially early 2026 and will be compensated for their time during the meetings. If you are interested in participating, further information is available on the Council Workgroups page. We are accepting application statements through January 10, 2025.
Associated links:
<https://links-1.govdelivery.com/CL0/https:%2F%2Fwww.facebook.com%2FNIDANIH/1/010001935f514dad-3bc896f6-09a3-4a99-9a57-650fc67cd8ad-000000/gZawcxuqmqpVxlDYl5KRA6aAb0F6qaVMf-PxgI6LnuI=380> <https://links-1.govdelivery.com/CL0/https:%2F%2Fx.com%2FNIDAnews/1/010001935f514dad-3bc896f6-09a3-4a99-9a57-650fc67cd8ad-000000/mpqUEYpIuhc9JFHxEKtJYgd0sO2MkRK2lTyjYLfCx1E=380> <https://links-1.govdelivery.com/CL0/https:%2F%2Fwww.linkedin.com%2Fcompany%2Fthe-national-institute-on-drug-abuse-nida/1/010001935f514dad-3bc896f6-09a3-4a99-9a57-650fc67cd8ad-000000/MDAOeV4b9UqgdTQKqsv8NP1IxaNy1-VJZf0pPGIdSLM=380> <https://links-1.govdelivery.com/CL0/https:%2F%2Fwww.youtube.com%2Fuser%2FNIDANIH/1/010001935f514dad-3bc896f6-09a3-4a99-9a57-650fc67cd8ad-000000/XDdTYlTHjOr7nahEQDBsHClsGu3q7NdUBzatmgv6P7E=380>
Source: Forwarding Agency:
Herschel Baker, International Liaison Director & Queensland Director
Drug Free Australia
Illegal drugs are the source of immense human suffering. Those most vulnerable, especially young people, bear the brunt of this crisis. People who use drugs and those struggling with addiction face a multitude of challenges: the harmful effects of the drugs themselves, the stigma and discrimination they endure, and often, harsh and ineffective responses to their situation.
The global drug problem is a complex challenge affecting millions of people worldwide. According to the World Drug Report, there are nearly 300 million drug users globally.
The issue spans from individuals with substance use disorders to communities affected by drug trafficking and organized crime. The drug problem is deeply connected to organized crime, corruption, economic crime, and terrorism. To effectively address this challenge, it is crucial to adopt a science-based, evidence-driven approach that prioritizes prevention and treatment.
The drug trade problem was recognized early in the 20th century, leading to the first international conference on narcotic drugs in Shanghai in 1909. In the decades that followed, a multilateral system was established to control the production, trafficking, and abuse of drugs.
Evidence-based drug prevention programmes can safeguard individuals and communities. By reducing drug use, these programmes can also weaken the illicit economies that exploit human misery.
Drugs are chemical substances that affect the normal functioning of the body or brain. They can be legal, like caffeine, nicotine, and alcohol, or illegal. Legal drugs, such as medicines, help with recovery from illness but can also be abused. Illegal drugs are considered so harmful that international laws, under United Nations conventions, regulate their use, making it unlawful to possess, use, or sell them.
Illegal drugs often have various street names that can vary by region and change over time. Their effects include immediate physical harm and long-term impacts on psychological and emotional development, especially for young people. Drugs can impair natural coping mechanisms and potential, and mixing them can result in unpredictable and severe consequences.
Additionally, drug use can impair judgment, leading users to take risks such as unsafe sex, which increases the risk of contracting hepatitis, HIV, and other sexually transmitted diseases.
Most common illegal drugs include:
In recent years, New Psychoactive Substances (NPS) have become a global phenomenon. NPS are substances of abuse not controlled under international drug conventions, but may pose public health risks. The term “new” refers to substances recently introduced to the market, not necessarily newly invented.
Known as “designer drugs,” “legal highs,” or “bath salts,” NPS often mimic the effects of illicit or prescription drugs. They are created by modifying the chemical structures of controlled substances to bypass legal restrictions.
The rapid appearance of diverse NPS on the global market poses public health risks and challenges for drug policy. Limited knowledge about their effects complicates prevention and treatment efforts, while their chemical diversity makes identification and analysis difficult. Effective monitoring, information sharing, and early warning systems are critical for addressing these challenges.
Since its founding, the United Nations has been tackling the global drug problem in a systematic manner.
The United Nations Commission on Narcotic Drugs (CND) was established in 1946 by the Economic and Social Council (ECOSOC) through resolution 9(I). Its purpose is to assist ECOSOC in overseeing the implementation of international drug control treaties.
Three drug control conventions were adopted under the auspices of the United Nations (in 1961, 1971 and 1988). Adherence is now almost universal.
The International Narcotics Control Board (INCB) is an independent, quasi-judicial expert body established under the 1961 Single Convention on Narcotic Drugs. It was formed by merging two earlier organizations: the Permanent Central Narcotics Board, created by the 1925 International Opium Convention, and the Drug Supervisory Body, established under the 1931 Convention for Limiting the Manufacture and Regulating the Distribution of Narcotic Drugs. The INCB monitors and assists governments in complying with international drug control treaties.
The World Health Organization (WHO) is a key player in the United Nations’ efforts to combat the global drug problem. Sustainable Development Goal 3, specifically Target 3.5, calls on governments to enhance prevention and treatment programs for substance abuse. WHO’s approach to addressing the global drug problem focuses on five key areas: prevention, treatment, harm reduction, access to controlled medicines, and monitoring and evaluation.
The United Nations Office on Drugs and Crime (UNODC) supports governments in implementing a balanced, health- and evidence-based approach to the world drug problem that addresses both supply and demand and is guided by human rights and the agreed international drug control framework. This approach involves: treatment, support, and rehabilitation; ensuring access to controlled substances for medical purposes; working with farmers who previously cultivated illicit drug crops to develop alternative sustainable livelihoods for them; and establishing adequate legal and institutional frameworks for drug control through using international conventions. UNODC works in all regions through balanced, evidence-based responses to address drug abuse and drug use disorders, as well as the production and trafficking of illicit drugs.
In 2009, governments adopted the Political Declaration and Plan of Action on International Cooperation Towards an Integrated and Balanced Strategy to Counter the World Drug Problem, which includes goals and targets for drug control.
Progress towards addressing the world drug problem and related issues is assessed at the United Nations General Assembly Special Session (UNGASS). All nations are encouraged to keep in mind the key principles of the 2030 Agenda for Sustainable Development and to leave no one behind. The Special Session in 2016 resulted in an outcome document, Our joint commitment to effectively addressing and countering the world drug problem.
In 2019, the Commission on Narcotic Drugs adopted the Ministerial Declaration on Strengthening actions at the national, regional and international levels to accelerate the implementation of joint commitments made to jointly address and counter the world drug problem. In the Declaration, governments reaffirmed their determination “to address and counter the world drug problem and to actively promote a society free of drug abuse in order to help ensure that all people can live in health, dignity and peace, with security and prosperity, and reaffirm our determination to address public health, safety and social problems resulting from drug abuse.” They also decided to review the progress made in implementing the policy commitments in 2029.
National legislative frameworks govern the responses of criminal justice systems to the world drug problem. In the vast majority of countries, illicit cultivation of drug crops, diversion of precursors and drug trafficking are criminal offences, but the criminal nature of drug use or possession for use varies across countries and regions.
Drug use or possession is considered a criminal offence in about 40 per cent of the 94 countries where data are available, representing a significant proportion of the global population. Available data indicate that more punitive measures are imposed for drug use or possession in Asia compared with other regions, while the Americas and Asia are the most punitive regions for drug trafficking.
Long-term efforts to dismantle drug economies must focus on providing socioeconomic opportunities and alternatives that address the root causes of illicit crop cultivation, such as poverty, underdevelopment, and insecurity. These efforts should go beyond simply replacing illicit crops or incomes. Additionally, they must address the factors that lead to the recruitment of young people into the drug trade, as they are particularly vulnerable to synthetic drug use.
According to newly available estimates, in 2022 only about 1 in 11 people with drug use disorders received drug treatment globally. It is recommended that all individuals affected by the world drug problem, including women, who face disproportionate stigma and discrimination, are ensured their universal right to health. To achieve this, drug treatment, care, and services must be comprehensive, effective, voluntary, and accessible to everyone without discrimination. These services should be designed to uphold and preserve the dignity of all individuals, including those who use drugs, as well as their communities.
The United Nations acknowledges the importance of fostering strong partnerships with civil society organizations to address the complex challenges of drug abuse and crime, which weaken the fabric of society. Active participation from civil society— non-governmental organizations, community groups, labour unions, indigenous groups, charitable organizations, faith-based groups, professional associations, and foundations — is crucial in supporting the UN’s efforts to fulfill its global mandates effectively.
UNODC supports NGOs participation in relevant drug-related policy discussions and meetings, particularly the CND regular and intersessional meetings and encourages the increased dialogue between NGOs, member states and UN entities, through the Vienna NGO Committee on Drugs (VNGOC).
Recognizing that youth are a vulnerable population, it is essential for the international community to address the issue of substance abuse effectively. Through the Youth Initiative, the UN provides opportunities for youth to actively participate in efforts to prevent substance use. This programme enables young people to join a community of peers committed to promoting health and well-being.
The Youth Forum is an annual event organized by the UNODC Youth Initiative as part of the broader framework of the Commission on Narcotic Drugs. It brings together young people from around the world, nominated by governments, who are actively engaged in drug use prevention, health promotion, and youth empowerment.
The forum provides a platform for participants to exchange ideas, share visions, and explore diverse perspectives on enhancing the health and well-being of their peers. Additionally, it offers an opportunity for youth to present their collective message to global policymakers, contributing their voices to international discussions and decisions.
Source: https://www.un.org/en/global-issues/drugs
Cultural, systemic and historical factors have converged to create the perfect storm when it comes to Black overdose deaths.
By Liz Tung – June 14, 2024 Reporter at The Pulse
In this Jan. 23, 2018 photo, Leah Hill, a behavioral health fellow with the Baltimore City Health Department, displays a sample of Narcan nasal spray in Baltimore. The overdose-reversal drug is a critical tool to easing America’s coast-to-coast opioid epidemic. (AP Photo/Patrick Semansky)
From Philly and the Pa. suburbs to South Jersey and Delaware, what would you like WHYY News to cover? Let us know!
A recent study from the Pennsylvania Department of Health has found that Black people who died from opioid overdoses were half as likely as white people to receive the life-saving drug naloxone, otherwise known as Narcan. The study also found that Black overdose deaths in Pennsylvania increased by more than 50% between 2019 and 2021, compared with no change in white overdose deaths.
In an email, a representative with the Department of Health said that similar rises in overdose deaths are being seen across the country, especially among Black, American Indian and Alaska Native populations. But researchers are still investigating what’s behind the spike.
“There does not appear to be a single reason why rates are increasing for Black populations and holding steady among white populations,” the statement reads. “The volatile and rapidly changing drug supply certainly has been a challenge as fentanyl is now found in every type of drug. Inequities in terms of treatment for substance use disorder may also play a factor as white people are more likely to have better access to the most evidence-based treatments and are more likely to stay in treatment.”
Abenaa Jones, an epidemiologist and assistant professor of human development and family studies at Penn State who was not involved in the study, has conducted similar research in Baltimore. She agreed that fentanyl-contaminated drugs — which are more common in lower-income neighborhoods — and less access to health care are likely factors in the growing number of overdose deaths among Black populations.
Jones said the criminal justice system, and its unequal treatment of Black people, also plays a role.
“We know that the intersection of criminal justice and substance use, and criminalization of drug use and how that disproportionately impacts minorities, can limit the accessibility of harm reduction services to racial-ethnic minorities for fear of harassment by police for drug paraphernalia,” Jones said, adding that even syringes obtained through needle-exchange programs can be considered illegal paraphernalia.
Fear of arrest, in turn, leads more people to using drugs in isolation.
“That may protect you from criminal legal involvement, but then in the event of an overdose, you may not have someone to help you,” Jones said. “So it could be that by the time the EMS come, it’s been too long for them to even consider administering naloxone.”
An unexpected observation that Jones made in the course of her research could also be a factor in rising death rates — the fact that many of the Black people dying of opioid overdoses are older.
“For any other racial groups, overdose deaths peak around midlife — 35, 45,” she said. “For Black individuals, it’s more like 55, 64, and we were wondering what was going on with that.”
After investigating that question, Jones and her colleagues formulated a working theory.
“The running hypothesis for us is that this is a cohort effect,” she said. “Individuals who’ve been using drugs over time, particularly Black individuals back from the ‘80s and ‘90s with the cocaine epidemic, never stopped using.”
Those individuals may have remained relatively stable until fentanyl began to contaminate their drug supply without them knowing.
“So whatever harm reduction tools that you were using for so many years that’s been helping you, when fentanyl’s involved, it’s a different game,” Jones said. “You have to use less, but you have to also know that you have fentanyl in your drugs, right?
It’s a problem that Marcia Tucker, the program director of Pathways to Recovery — a partial hospitalization program focused on co-occurring substance use and mental health challenges — sees frequently among their mostly Black clients.
“If you come into treatment saying that I’m a cocaine user, or I’m a crack cocaine user, or I use marijuana, you’re not even thinking that an opioid overdose or fentanyl overdose could possibly happen to you,” Tucker said. “And it does happen.”
In fact, Tucker said, she’s seen more of these kinds of overdoses over the past two years than in the three decades she’s spent working in addiction treatment. Despite that, there’s still a lack of education — and even stigma — surrounding both medication-assisted treatments (MATs) for opioid addiction, and the use of naloxone.
“I think sometimes culturally with the African American community, as far as MATs are concerned, there are some taboos about getting that extra help when they decide to come into treatment and get clean,” she said. “A lot of people feel like they want to do it from the muscle. They see it as another form of using.”
She said others may not know how to use naloxone, what kinds of effects it has or how to get it.
“I think a lot of folks don’t even know that they can walk into a pharmacy and get naloxone — you don’t have to have a prescription for that,” Tucker said. “And I think that information is just not always presented to communities, especially poor communities that don’t have a lot of resources.”
Other sources of hesitation are more immediate. Aaron Rice, a therapist at Pathways to Recovery, said that many of their clients fear naloxone because of its physical effects.
“I think they associate it with precipitated withdrawal at times,” Rice said, referring to the rapid-onset withdrawal that can cause symptoms including anxiety, pain, seating, nausea, vomiting and diarrhea.
“The only thing they’re thinking about is feeling better. And that feeling is going to supersede logic at that moment. It always does.”
The Department of Health acknowledged that the study only paints a partial picture, as it doesn’t include individuals whose overdoses were reversed by naloxone, and added that during the years of the study (2019–2021), naloxone was available by prescription only — a fact that likely played into the race-based disparity.
“There are recognized inequities in access to health care among persons of color, the concept of which likely extends to access to naloxone,” the Department of Health statement reads. “Historically, many public health materials and messaging more narrowly focused on persons using opioids. With people now taking two or more drugs together (whether intentionally or unintentionally), public health materials and messaging need to be more inclusive of all persons using drugs, regardless of the type.”
The study, researcher Abenaa Jones, Marcia Tucker and Aaron Rice all agreed on at least one intervention that could increase Black people’s access to naloxone — relying on trusted community leaders and institutions, like churches, to help educate residents and distribute the overdose-reversing drug.
“I just can’t stress enough how it’s a lifesaver — it’s the difference between life and death,” Tucker said. “I think people who aren’t medical professionals and find themselves in a situation where it might need to be used would probably be a little fearful — fearful about how to use it or how the person is going to react or whether it’s really going to work — just know that you’re better off with it and trying it. You don’t want to have to second guess yourself later and say, ‘I wish we had it. I wish we had gotten it,’ or, ‘I wish we had used it.’”
Source: https://whyy.org/articles/black-pennsylvanians-overdoses-naloxone-less-likely-to-receive/
Washington, D.C. – Today, White House Office of National Drug Control Policy (ONDCP) Director Dr. Rahul Gupta released the following statement on the latest provisional data from the Centers for Disease Control and Prevention (CDC), showing drug overdose deaths decreased by 12.7% year-over-year (in the 12-months ending May 2024). This is the largest recorded reduction in overdose deaths, and the sixth consecutive month of reported decreases in predicted 12-month total numbers of drug overdose deaths.
“When President Biden and Vice President Harris took office, the number of drug overdose deaths was increasing 31% year-over-year. They immediately took action: making beating the overdose epidemic a key pillar of their Unity Agenda for the Nation and taking a comprehensive, evidence-based approach to strengthening public health and public safety. As an Administration, we have removed more barriers to treatment for substance use disorder than ever before and invested historic levels of funding to help crack down on illicit drug trafficking at the border. Life-saving opioid overdose reversal medications like naloxone are now available over-the-counter and at lower prices. We are at a critical inflection point. For the sixth month in a row, we are continuing to see a steady decline in drug overdose deaths nationwide. This new data shows there is hope, there is progress, and there is an urgent call to action for us all to continue working together across all of society to reduce drug overdose deaths and save even more lives.”
Source: https://www.whitehouse.gov/ondcp/briefing-room/2024/10/16/white-house-drug-policy-director-statement-on-latest-drug-overdose-death-data/
The Cherokee Nation Community Action Network (CAN) coalition was originally developed in 2006 and became a Drug-Free Community coalition in 2018. The CAN uses culture as a strategy to prevent and reduce substance use in Cherokee communities. They partner with Sequoyah School, a tribal school in Tahlequah that young people can attend from anywhere within the reservation. The reservation includes some very rural and isolated communities with limited resources.
To increase community connectedness, the coalition teaches a National Association for Addiction Professionals-certified curriculum based on the book Walking in Balance by Abraham Bearpaw. Bearpaw was raised in one of the Cherokee Nation communities and, after coping with alcohol use for several years, decided it was time for a change. He reconnected with his culture by prioritizing mindfulness, health, and trust and has been in recovery for 12 years. He partners with different communities to teach his curriculum to young people in hopes of reducing the likelihood of them engaging in substance use. The curriculum includes 12 weekly lessons that teach students how to reconnect with culture, manage stress, and care for themselves. The leading principle is “Walking in Balance,” which emphasizes balancing traditional Cherokee culture with modern contemporary culture in their everyday lives.
The CAN coalition initially faced challenges with young people’s willingness to return to the ceremonial grounds. Due to some forbidden traditional practices, they felt they were too far removed. However, the coalition encouraged them to attend to learn and reconnect with their roots. Of the 100 young people living in the current town they serve, 75 showed up to participate in the curriculum. The day-to-day traditional and cultural activities include the making of clay beads, ribbon skirts, corn-bead necklaces, basket weaving, and stickball. The community activities are a source of Cherokee knowledge-building, sharing, and resiliency that helps build a culture of connectedness. The instructor teaches ceremonial values of youth and elder interaction, respect for ancestors, and the importance of taking care of the land. One community member said, “Our tribe has long known that building a sense of belonging, helping youth grow a connection to community, and cultural identity helps them grow into healthy adults.” The Cherokee Nation CAN will continue to foster safe and healthy environmental conditions, providing social support, encouraging school connectedness, and creating safe and caring communities on the reservation to improve the lives of those living there.
Source: https://www.cdc.gov/overdose-prevention/php/drug-free-communities/cherokee-nation.html
Manuel Balce Ceneta/Associated Press by CARMEN PAUN – 10/27/2024 04:00 PM EDT
Traffickers are to blame, the candidates say. Virtually no one’s talking about treatment.
The Harris and Trump campaigns said the presidential candidates are talking about drug treatment, albeit more quietly than they are border security. |
There’s a rare point of agreement among Republican and Democratic candidates this election year: America has a drug problem and it’s fentanyl traffickers’ fault.
Republicans, including former President Donald Trump, are hammering Democrats over border policies they say have allowed fentanyl to surge into the country. Democrats, including Vice President Kamala Harris, respond that they, too, have cracked down on traffickers and want stricter border enforcement.
The consensus reflects the resonance of border control among voters — most of the country’s fentanyl comes from Mexico — and a hardening of the nation’s attitude toward addiction. Troubled by drug use, homelessness and crime, voters even in the country’s most progressive states favor cracking down. Politicians from Trump and Harris on down the ballot say they will.
“It’s one of those things that people don’t want in their community,” said Rep. Jahana Hayes, a Democrat running for a fourth term representing a district including suburbs of Hartford, Connecticut, and rural areas to their west, of illicit drugs. “They want a tough-on-crime stance on it. They want it to go away. They’re afraid for their families, they’re afraid for their children.”
That view worries public health experts and treatment advocates, who see a backsliding toward the law enforcement focus that once looked futile in the face of Americans’ insatiable appetite for drugs. They fear it bodes ill for additional efforts from Washington to expand addiction care.
“There are a lot of things that both parties can point to, as far as progress that’s been made in addressing overdoses: We’ve seen bipartisan efforts to expand access to treatment, to expand access to health services for people who use drugs, and I wish they would talk about that more,” said Maritza Perez Medina, federal affairs director at Drug Policy Action, an advocacy group that opposes the law enforcement-first approach.
Six years ago, when a bipartisan majority in Congress passed the SUPPORT Act to inject billions of dollars into treatment and recovery services, and then-President Trump signed it, the vibes in Washington around drug use were more empathetic.
President Donald Trump declared the opioid crisis a nationwide public health emergency in October 2017. | Brendan Smialowski/AFP via Getty Images But after it passed, fatal drug overdoses driven by illicit fentanyl skyrocketed, hitting a record 111,451 in the 12 months ending in August 2023 before starting to recede. Homelessness, sometimes tied to drug addiction, also spiked.
When the SUPPORT Act came up for renewal last year, Congress wasn’t as motivated. The Democratic Senate hasn’t voted on a bill, while a House-passed measure from the chamber’s GOP majority offers few new initiatives and no new money.
Attitudes are similar in the states. Oregon, where voters legalized drugs for personal use in 2020, reimposed criminal penalties this year after its largest city, Portland, was overrun with homeless drug users. Polls indicate California voters, frustrated, too, by homelessness and crime, are likely to boost penalties for drug users by ballot initiative next month.
Candidates aim to prove they share voters’ frustration.
Republicans have spent more than $11 million on TV ads in the past month attacking Democratic opponents on fentanyl trafficking, according to a tally by tracking firm AdImpact. And Democrats have spent nearly $18 million defending themselves, mostly by highlighting their efforts or plans to provide more resources and personnel to combat trafficking.
“It’s an easy shortcut in a 30-second commercial to tie a broader issue to one that has an easy explanation,” said Erika Franklin Fowler, a professor of government at Wesleyan University who directs a project analyzing political advertising.
Trump’s not talking about the SUPPORT Act, one of his most consequential legislative successes. Vice President Kamala Harris is not touting the treatment policies of the president she serves, Joe Biden, who expanded access to medications that help people addicted to fentanyl, as well as to drugs that can reverse overdoses. Some public health specialists credit increased access to the drugs with reducing overdose death rates in the past 12 months after years of grim ascent.
Trump used his first anti-Harris ad this summer to blame her for the more than 250,000 deaths from fentanyl during the Biden-Harris administration.
Vice President Kamala Harris met state attorneys general in July 2023 to discuss possible actions against fentanyl. | Saul Loeb/AFP via Getty Images Harris responded by touting her prosecution of drug traffickers when she was California’s attorney general and a promise to strengthen the border.
“Here’s her plan,” a deep-voiced narrator intoned in Harris’ ad: “Hire thousands more border agents, enforce the law and step up technology — and stop fentanyl smuggling.”
‘A political cudgel’
Similar attacks and responses have played out in Senate and House races across the country.
In the tight Arizona race to replace Sen. Kirsten Synema (I-Ariz.), Republican Kari Lake has accused her opponent, Democratic Rep. Ruben Gallego, of empowering drug cartels to import fentanyl by supporting Biden-Harris administration border policies.
“We’re losing an entire generation of people, and you should know better, Ruben,” Lake told Gallego in a debate earlier this month, referencing the deaths of teens who took counterfeit pills laced with fentanyl.
Gallego, who was elected to Congress in 2014 as a progressive but has shied from that label in his Senate run, responded by touting bills he’s supported or introduced to fund more technology at the border and track fentanyl money flows across Mexico and China, where chemicals to make the drug are manufactured.
A mother visit her son’s grave, who died of a fentanyl overdose at 15. | Jae C. Hong/AP In Colorado’s hotly contested 8th congressional district, which encompasses Denver suburbs and rural areas to the north, Republican state Rep. Gabe Evans has blamed the incumbent, Democrat Yadira Caraveo, for the fentanyl crisis.
“This is our reality now: a 100 percent increase in fentanyl deaths because liberals open the border, legalize fentanyl and let criminals out of jail,” says a police officer in an ad for Evans. “And Yadira Caraveo voted for it all,” Evans adds.
Caraveo defended herself in a debate with Evans earlier this month, noting the bill he’s referring to was state legislation that “tried to balance the need to punish drug dealers and cartels but not incarcerate every single person that is addicted.”
In Connecticut, the National Republican Congressional Committee attacked Hayes for voting against a bill to permanently subject fentanyl to the strictest government regulation, reserved for those drugs with high likelihood of abuse and no medical uses.
Hayes said she opposed the bill because it included mandatory minimum prison sentences for people caught with drugs and no provisions supporting prevention, treatment or harm reduction.
“I hate that this is being used as a political cudgel because we’re missing out on an opportunity to say: ‘How do we address the root causes?’” Hayes said in an interview.
Hayes said she has responded to the attacks on the campaign trail and talked to constituents about the need for treatment, despite some advice to the contrary.
“Even amongst Democrats, there were people who were like: ‘You don’t want the headache, you don’t want people to think that you’re soft on crime or soft on drugs.’ And I was like: ‘This has to be about more than optics if we truly are trying to save people’s lives,’” Hayes said. ‘If we don’t keep the momentum going’
Oregon, where voters legalized drugs for personal use in 2020, reimposed criminal penalties this year after its largest city, Portland, was overrun with homeless drug users. | Patrick T. Fallon/AFP via Getty Images The lesson the Drug Policy Action’s Medina takes from the campaigns is that talking about drug treatment doesn’t sell in American politics.
“People are struggling. Social services aren’t where they need to be, health services aren’t where they need to be,” she said. “It’s easier to run a fear-based campaign rather than talking about really tough issues,” like breaking the cycle of addiction.
Ironically, the tough talk on the border comes as policymakers, for the first time in years, have evidence that the tide of fatal drug overdoses is receding.
The CDC estimates that overdose deaths, most caused by fentanyl, declined by nearly 13 percent between May 2023 and May 2024, to just under 100,000.
Harris’ running mate, Tim Walz, mentioned the dip during his debate with Trump’s vice-presidential pick, JD Vance, earlier this month.
The number is now about where it was when Biden took office, though still 50 percent higher than when Trump did in January 2017.
Expanding access to treatment, the Food and Drug Administration’s decision to make the opioid-overdose-reversal medication naloxone available over the counter last year, increased fentanyl seizures at the border, and the arrest and sanctioning of Mexican drug cartel leaders have contributed to the recent drop, Biden said last month.
Advocates for drug treatment say that’s all good cause for candidates to tout their access-to-treatment efforts and promise to expand them.
“The worst outcome for overdose prevention coming out of this election would be if we don’t keep the momentum going,” said Libby Jones, who leads the Overdose Prevention Initiative, an advocacy group.
But there’s not the groundswell of interest on Capitol Hill that there was in 2018, when Congress passed the SUPPORT Act.
Congress has continued to fund opioid treatment authorized in that law, but it mostly hasn’t taken the law’s 2023 expiration as an opportunity to increase funding or try big new ideas.
The Food and Drug Administration decision to make the opioid-overdose-reversal medication naloxone available over the counter last year has contributed to a drop in fatal overdoses over the past year, President Joe Biden said last month. | Diane Bondareff/AP The 2024 federal funding law Congress passed in March included some minor changes in the form of bipartisan legislation to require state Medicaid plans to cover medication-assisted treatment for substance use disorder. It also created a permanent state Medicaid option allowing treatment of substance use disorder at institutions that treat mental illness, in an effort to expand access to care.
But bipartisan legislation approved by the Senate committee responsible for health care to make it easier for others to gain access to methadone, a drug effective in helping fentanyl users, hasn’t gone to the floor and faces opposition from key Republicans in the House.
The Harris and Trump campaigns said the presidential candidates are talking about drug treatment, albeit more quietly than they are border security.
Vice President Harris’ campaign pointed to her web site, where she touts her prosecution of drug traffickers and the Biden-Harris administration’s investment in “lifesaving programs.”
Republican National Committee spokesperson Anna Kelly said “President Trump is uniquely able to connect with families combating addiction,” pointing to times when he’s talked about his brother’s struggles with alcohol use disorder and to his administration’s efforts to contain the opioid crisis.
But she added that the tough talk on the border is relevant: “Combating fentanyl is a public health issue and stopping it begins with securing the border.”
Source: https://www.politico.com/news/2024/10/27/fentanyl-drugs-elections-00185576
MEDICINAL cannabis has been the hottest of hot-button issues in medicine for some years now. It’s one the few medications where media hype and patient demand seem to have moulded – some would say muddied – the regulatory framework in a way that has troubled many clinicians.
In Australia, there are now three different pathways to legally accessing medicinal cannabis. The Category A Special Access Scheme (SAS) allows the importation of unregistered products on compassionate grounds, but requires import licences and customs clearance, while Category B SAS gives access to locally stored medicinal cannabis, but requires TGA and state review and approval. Specialists can also obtain an Authorised Prescriber status to prescribe cannabis – these will usually be either oncologists for cancer-related pain, or paediatric neurologists for the control of severe epilepsy in children.
But what is the evidence for medicinal cannabis, and is it sufficient for clinicians to feel comfortable prescribing it? These issues are explored in two articles published in the MJA, one a Perspective from the Royal Australasian College of Physicians (RACP) and the other a Narrative Review on the challenges of prescribing cannabis for paediatric epilepsy, authored by researchers from the Sydney Children’s Hospital.
The RACP comes down on the side of caution. It notes that Australia, along with the rest of the world, is “navigating unchartered waters with pharmaceutical grade cannabinoids”, and that more research is needed before we can say whether or not cannabis has a place in contemporary medical practice.
In paediatric epilepsy, some of that research seems to be coming into focus. Last May, a randomised, double-blind trial of cannabidiol, a cannabis derivative that does not contain the psychoactive ingredient tetrahydrocannabinol, provided hard data for the first time that the treatment may work in children with Dravet syndrome – a severe form of childhood epilepsy with often drug-resistant seizures. This was followed by another trial, published last month in the Lancet, that showed similar efficacy of cannabidiol in Lennox–Gastaut syndrome, another form of paediatric epilepsy characterised by multiple seizure types.
Laureate Professor Ingrid Scheffer, who is Chair of Paediatric Neurology Research at The University of Melbourne and co-author of the trial of cannabadiol in Dravet syndrome, says that although her study does provide solid evidence for the drug’s efficacy, it should in no way be considered a miracle cure.
“It’s been sold as a magic bullet by the media. And you have families who are on a terrible rollercoaster, they’re vulnerable and medicinal cannabis is being cast as this drug that may save their child. And the answer is that it often does not. It may help, and in our study cannabidiol had a 43% responder rate, defined as at least a 50% reduction in the seizure frequency. But that’s exactly the same as some of the other drugs we use.”
But she says that doesn’t mean it shouldn’t be prescribed.
“Dravet syndrome is usually drug-resistant and you don’t know which drugs will work, so it could be worth trying if others have failed. But the families should be aware of its chances of success and the fact that it can have side effects.”
She says the key is more research.
“What people are accessing is very variable. They’re importing it from all over the place, they may even be getting friends to grow it in their backyard, so we do not know what they’re giving their child. What we need to do is go forward with more trials in different populations and with different formulations. If we’re going to invest in this, we need to know it works and we’re not wasting our health dollar on it.”
Professor Scheffer says that another drug currently being trialled, fenfluramine, may end up the more successful treatment. Trial results have yet to be published, but interim findings suggest that fenfluramine may have a dramatically higher responder rate of up to 70%.
Dr John Lawson, a Sydney-based paediatric neurologist and co-author of the Narrative Review on cannabis and childhood epilepsy, agrees that cannabidiol, though worth trying in some children, is no wonder drug.
“I’m not hanging my hopes on cannabidiol,” he says in an exclusive podcast for MJA Insight.
“I came in as quite a sceptic, but my attitude has changed. I now believe that it is an antiepileptic, but I’m not sure what place it has. It’s the early stages of development, and there are other compounds that haven’t been looked at.”
Dr Lawson says that he wouldn’t suggest it to a family until many other antiepileptics had already failed, and the chances of the next drug working were already low.
“I’ve come around to bringing it up in conversation because everyone knows about it, and families know I’ve prescribed it. But the biggest reason to not prescribe is cost. For a small child, it will cost over $1000 every couple of weeks to give a Therapeutics Goods Administration-approved product. Almost the only people I have prescribed it for are those who have an absolute ‘bucketload’ of money. Or I form a contract with them, and I say look, this will cost you $3000, but all the trials say you will know very quickly if it’s working or not.”
He says that in the patients who are helped by cannabidiol, the effect is still relatively modest.
“Patients are very rarely seizure-free. It may have a role in the future, once the hype has died down, but it will be a very low [on a list of preferred antiepileptics].”
Source: https://www.doctorportal.com.au/mjainsight/2018/6/medicinal-cannabis-miracle-cure-or-media-hype/

Tulsa World Indigenous Affairs Reporter
The Cherokee Nation’s approach to substance abuse recovery is harm reduction, which has drawn criticism from some who work in addiction recovery.
“Harm reduction is a pretty controversial topic. A lot of people feel it can be enabling drug users. It can feel counterproductive and counter intuitive,” said Jennifer Steward, director of the University of Tulsa’s Behavioral Health Clinic.
In a Tulsa World interview, Steward said the controversial aspect comes from the fact that harm reduction does not encourage abstinence from drug use, which makes it different from traditional substance abuse rehabilitation programs. Harm reduction instead focuses on keeping active drug users alive, with considerations for their health and safety.
The Cherokee Nation harm reduction program utilizes a mobile unit that brings supplies to drug-users on the streets: clean needles, cotton swabs and Narcan, which can reduce cravings and combat a potentially fatal overdose.
Steward said many harm reduction programs also provide a safe, clean environment to partake in drug use, free of disease such as HIV or hepatitis C, with staff ready to assist in case of overdose.
Cherokee Nation prevention specialist Coleman Cox said that his tribe recognized the potential for addiction among the Cherokee people after being exposed to the opioid epidemic is “far reaching and the latest in a long line of injustices brought upon indigenous peoples.”
According to the Centers for Disease Control, in 2021 the highest rate of drug overdose deaths was in American Indian and Alaskan Native individuals. Data from the Substance Abuse and Mental Health Services Administration indicates 5.1% of Natives have misused opioids, which can include prescribed pain-relief medications, hydrocodone, oxycodone, fentanyl and heroin.
“We bent the opioid industry to a settlement for the harm it inflicted, and we are making the opioid industry help pay for every single penny of this facility,” said Cherokee Nation Chief Chuck Hoskin Jr. in reference to their treatment facility they broke ground for Thursday morning.
The Cherokee Nation received a Substance Abuse and Mental Health Services Administration grant last year for harm-reduction services. They now operate a storefront at 214 N. Bliss Ave. in Tahlequah. It is open not only to tribal members but also to the public, and all participants can remain anonymous.
The new facility that the tribe broke ground on this week is a $25 million dollar addiction treatment center just outside of Tahlequah.
The Cherokee Nation’s Public Health and Wellness Fund Act of 2021 dedicated $100 million in settlement funds from opioid and e-cigarette lawsuits for a variety of public health programs.
Cox said harm reduction meets people where they are at in their addiction. This means that if the user does not want to seek rehabilitative services, they do not have to. Rehabilitation services may be recommended, but they are not a requirement.
“Harm reduction is more than Narcan and clean needles. It’s treating others how they want to be treated — with dignity, respect and value, without conditions,” said Cox.
Evan White, a member of the Absentee Shawnee tribe, is the director of Native American research at Laureate Institute for Brain Research in Tulsa. He has worked with various tribal behavioral health programs through his research.
“Harm reduction is a model that has a strong evidence base for good outcomes,” he said, “especially in substance use disorders.”
White believes harm reduction could be attractive to Native communities as it values a person’s autonomy.
“I see a consistent value of a person as an individual within Native communities. Healing is an important part of the process in these cultural spaces, even though there is a lot of stigma around substance abuse in our broader society,” he said.
For Native individuals with substance abuse issues, White said participating in cultural activities may enhance self-control and mindfulness.
The Cherokee Nation’s program provides opportunities for Native people in recovery to partake in cultural activities.
“We planted a Three Sisters Garden: corn, beans and gourds,” said Cox. “Corn provides the bean a pathway for growth. Beans give back by imparting nitrogen to the soil. Gourd provides protection and covers the ground. Three different things working in harmony. Body, mind and spirit.”
Members of the program get to adopt a plant, name it and tend to it. Cox said the vegetables are not for eating, however.
“They are meant to harvest seeds for the future bounty, beyond what we can see now. Just like when our members come to us for whatever kind of help, we plant a seed that one day they will harvest a healthier life,” he said.
Cox said the harm reduction staff launched a new chapter of “wellbriety movement” that they call “recovery rez.” It’s a cultural approach to the traditional 12-step recovery plan.
“At Recovery Rez they begin with prayer and fellowship meal, then smudge and hold a talking circle guided by the passing of an eagle feather from speaker to speaker. They close out the evening with a drum circle and singing. All are welcome, and citizens don’t need to be in recovery to benefit from the cultural protective factors,” said Cox.
Steward said it can be difficult to view harm reduction as a substance abuse program because harm reduction focuses on the long-term.
“The goal is to help someone be ready to engage in rehabilitation later on, but in order to do that, they have to be alive,” she said.
According to Cherokee Nation spokeswoman Julie Hubbard, the tribe’s harm reduction program has had 3,099 encounters for service, and it has 1,049 members currently. The number of people who still inject drugs within the program is 743. The amount of lives saved at the program from Narcan distribution is 44.

Perhaps we’re finally turning a corner when it comes to lowering overdose deaths. While the number of people dying as a result of an overdose remains frighteningly high, a new report signals modest progress in efforts to reduce fatalities.
Updated figures from the Centers for Disease Control and Prevention (CDC) found fatal drug overdoses fell 2.4% from 2022 to 2023. The toll from the overdose crisis reached 108,317 lives last year, according to data the CDC posted Aug. 4. While that’s lower than the 111,029 overdose deaths in 2022, it still represents a massive number of preventable deaths, and there’s yet more we can do to ensure that fatalities continue to decline.
That is one of the goals of International Overdose Awareness Day, observed on August 31.
In recognition of the day, the National Council has created an informative new video to help people understand how to administer naloxone. Naloxone (often known by the brand name Narcan) is a medication that reverses opioid overdoses. It is quite literally a lifesaver.
The lower number of overdose fatalities in 2023 may be related to the Food and Drug Administration’s March 2023 decision to make naloxone available over the counter, a decision we applauded. But having naloxone available doesn’t mean everyone who may need it has access to the drug. And it doesn’t mean that everyone knows how to administer naloxone.
Let’s hope the modest drop in overdose fatalities last year was an early indication that we’re finally flattening the curve of overdose deaths.
That’s exactly why we made this video.
Everyone should carry naloxone, especially those who work with the public — whether as a teacher, ambulance driver, librarian, coach or in some other capacity.
The Substance Abuse and Mental Health Services Administration (SAMHSA) continues to promote naloxone distribution through state opioid response (SOR) grants. Naloxone distribution and saturation planning is a federal-state partnership (of sorts) to optimize naloxone distribution.
States are required to create distribution and saturation plans as part of their SOR grant; every state is required to make one. The purpose is for states to meaningfully plan and coordinate their naloxone distribution based on data and input from impacted community partners so they optimize reach, including focusing distribution efforts to those most likely to experience and/or witness an overdose.
Substance use isn’t going away anytime soon. July’s release of the 2023 National Survey on Drug Use and Health provides important new data about substance use challenges and the nature of substance use among people of all ages. For instance:
Among people aged 12 or older in 2023, 70.5 million people (24.9%) had used illicit drugs in the past year, up from 70.3 million people in 2022 and 61.2 million in 2021.
In 2023, 48.5 million people 12 or older (17.1%) had a substance use disorder in the past year, down slightly from 48.7 million in 2022.
In 2023, 8.9 million people 12 and older (3.1%) used opioids in a non-prescribed way in the past year, compared to 8.9 million in 2022 and 9.4 million in 2021.
This data shows us that no one is immune from a substance use challenge.
We can’t turn our backs on people with a substance use disorder or ignore the tragic consequences of substances, whether they’re considered illicit or socially acceptable, like alcohol. To support people with a substance use disorder or their loved ones, the Start With Hope project also recently published many new resources, including:
The Start With Hope project was started in November 2023 by The Ad Council, in partnership with the CDC, the National Council and Shatterproof to deliver a message of hope to those living with substance use disorders as well as those at risk of developing one.
Let’s hope the modest drop in overdose fatalities last year was an early indication that we’re finally flattening the curve of overdose deaths. When it comes to lives lost, we can’t be satisfied with modest improvements. Let’s ensure continued progress by spreading the word about lifesaving resources.
Check out our new video, and let us know what you’re doing in your communities to reduce overdose deaths and provide resources to those with a substance use disorder.
We can and will learn from one another on how to best support people and communities.

In 2022, he found himself without a vehicle and without a home, which forced his two teenage children to move in with friends. He had burned bridges with friends and family and it took a drug-induced stint in the hospital for him to realize his cocaine addiction was going to be a “death sentence.”
Rubick, who lives in the Denver suburb of Arvada, Colorado, knew he needed help. But first he had to figure out what to do with one of the only sources of unconditional love and support he had left: his beloved German shepherd rescue, Tonks.
Most residential rehab centers in the United States don’t allow patients to bring their pets along, said Rubick, 51. So when his brother could no longer help care for the dog, Rubick thought he would have to make the excruciating decision to give up Tonks.
“It basically came down to being able to take care of my dog or being able to take care of myself,” he said.
Rubick — who has been sober for more than two years and is now an addiction recovery coach — was connected to the group PAWsitive Recovery, which fosters animals while their owners receive treatment for drug and alcohol abuse, and for people dealing with domestic violence or mental health crises.
“People that are trying to get into recovery sometimes have lost their families, their children, any kind of support system that they have had,” said Serena Saunders, the organization’s program manager. “You’re not going to compound trauma that you’ve already had by giving up the one thing that hasn’t given up on you, and that’s people’s animals.”
Saunders founded PAWsitive Recovery in Denver three years ago. Since then, it’s helped more than 180 people and their pets, and Saunders said the group has looked to expand nationally after it became a part of the Society for the Prevention of Cruelty to Animals International. The organization, whose largest foster network is in Colorado but accepts applications nationwide, is one of just a few programs in the U.S. that cares for the pets of people seeking treatment for substance abuse.
Saunders’ own experience with drug and alcohol addiction has helped her tailor the program. She said she had a “pretty broken childhood,” with her mother being schizophrenic and addicted to methamphetamine and her father also struggling with addiction. She sought comfort in alcohol when she was about 12 and was using hard drugs by the time she was 14.
“Addiction just gave me trauma after trauma,” said Saunders, now 41.
Saunders was seeing a therapist for her depression and PTSD when a fortuitous session planted the seed of PAWsitive Recovery. With a background in veterinary and shelter medicine, which focuses on caring for homeless animals, she told her therapist she wanted to incorporate her love of dogs in her recovery.
“And that’s what we did,” said Saunders, who fostered Tonks for several months while Rubick was in treatment and facilitated visits between the two best friends.
“To see a broken person when we’re meeting them in a parking lot, when they have nothing left to live for but their animal. And to see how broken and how desperate they are in that moment, and then to circle back around six months later and see them completely turn their lives around is just so special. It’s amazing,” said Saunders, who has been sober for 3 1/2 years.
That sentiment is echoed by the organization’s volunteer foster families, some of whom are drawn to the program because of their own experiences with addiction.
Denver resident Ben Cochell, 41, who has been sober from alcohol for more than seven years, has two dogs of his own and has fostered several more.
“One of my favorite parts about fostering in this program is the ability to teach my kids some life lessons in how to help others and how to care for animals and be kind, be loving. And to just give of yourself,” he said. “That’s what you have. Your time and your energy. And you can give that away freely.”
If not for PAWsitive Recovery, Rubick said he probably would have ended up living on the streets with his dog and trying to figure out recovery on his own. But as it turned out, by being able to keep his rescue dog, Tonks ended up rescuing Rubick, he said.
“It’s that connection, caring for another creature and having something else care for you the way that animals do,” Rubick said. “It’s just unconditional, and sometimes that’s one of the things that people in recovery really need to be able to feel.”
Associated Press writer Colleen Slevin contributed to this report.
LIMA — The Lima Police Department recently posted on its Facebook page about an increase in overdoses in Lima over the past few weeks.
With September being National Recovery Month, where organizations try to increase public awareness about mental health and addiction recovery, local organizations and law enforcement agencies shared their experiences with addiction and overdoses and the help that is available.
The problem
Lima Fire Chief Andy Heffner said his department responded to 85 overdoses so far this year. He said the overdose numbers have risen and fallen throughout the year, with about one-week breaks in between. He believed the numbers were based on the drugs available in the area.
Project Auglaize County Addiction Response Team Project Coordinator/Peer Support Specialist Brittany Boneta spoke on the reason for the overdose spikes.
“When it comes to overdoses, one is too many,” Boneta said. “I think the number of overdoses comes in waves. There could be a really bad batch of heroin or fentanyl that gets distributed throughout the county that could lead to a spike in overdoses.”
Heffner cited the Drug Enforcement Administration’s website, which said seven out of every 10 pills seized by the DEA contain a lethal dose of fentanyl. The website also said 2 milligrams of fentanyl can be enough to kill someone.
“It only takes one time when Narcan is not available that you could lose your life. If you get clean, you will never have to worry about an overdose, and neither will the people that love you,” Heffner said.
Bath Township Fire Chief Joe Kitchen said his department used Narcan 21 times on patients from August 2023 to August 2024. The department also distributes Narcan to families just in case an overdose occurs.
“Although we have only left behind a few kits so far, I think it gives the family of a known addict some peace of mind that they could assist them in the event of an OD prior to EMS arrival,” Kitchen said.
Another problem is a tranquilizer called Xylazine is being mixed with fentanyl, which does not respond to the usual methods of reversal.
“There are always new drugs/drug combinations being introduced on the streets that make it difficult for those in the treatment world to keep up with and know how to effectively treat,” said Jamie Declercq, the vice president of clinical operations for Lighthouse Behavioral Health Solutions. “Right now, we are seeing an increase in substances (such as Xylazine) across the county which does not respond to Narcan, so that is likely one reason for the increase in overdose deaths.”
Their stories
Boneta was addicted to opiates and crack cocaine over a seven-year period, and her addiction journey started when she was prescribed Percocet by a cardiologist for a heart condition when she was 18.
“There wasn’t a drug I wouldn’t use,” Boneta said. “I was an honor roll student in high school with more trauma than almost anyone I know, and when I went off to college I wasn’t educated on the true dangers of drugs, the thirst to fit in, and all of my trauma stuffed down.”
When her doctor stopped prescribing Percocet, she bought them from drug dealers, not knowing they were laced with heroin.
“When the drug supply of the fake Percocet ran out, I was just buying actual heroin. The heroin was starting to have fentanyl added to it, and before long that was all I was consuming,” Boneta said.
Boneta was eventually sent to prison for drugs, and during that time her 6-year-old son was involved in a house fire and suffered serious injuries.
“I was transported from the prison, in my orange jumpsuit and shackles on my wrists and ankles, to say my goodbyes to my son. I think seeing him lying there in a coma covered in bandages was something so soul-shaking that I knew this was my rock bottom,” Boneta said.
“My son had countless surgeries and was getting better and stronger as the months went by, so I decided I was going to completely reset my life and work my butt off just as hard,” Boneta continued. “I completed as many recovery groups and classes as possible and started learning coping skills and tools to use when I was released from prison. I knew that I wanted to help other people like me and show them that people can understand what they are going through and not have judgment towards them.”
Diane Urban, of Delphos, the founder/president of the Association of People Against Lethal Drugs, started APALD because her youngest son died from a fentanyl overdose. Her older son is also a former addict, and her niece is in active addiction.
“He was clean for the last nine months of his life, he came to live with me, and he relapsed due to an ingrown wisdom tooth that was coming in, his face was swelling up, and because he had Medicaid, we couldn’t find him any help anywhere except for a place in Van Wert, and it was a two-week out appointment. Unfortunately, unbeknownst to me, he relapsed, and I found him dead in his bedroom from a fentanyl overdose,” Urban said.
Challenges to get help
Transportation, not enough of a variety of local recovery options available and financial barriers were all cited as issues addicts face when they decide to get help.
“For peers that are needing inpatient treatment or sober living, we have to send them to other counties for help,” Boneta said. “There is definitely a need for more substance abuse treatment in our county.”
Declercq said Allen County also has a need for inpatient or residential treatment, and people who need that care have to go to one of the major cities nearby.
Urban dealt with having to go outside the area when her son got help.
“Seven years ago when I had to get help for my son, we had to go to Columbus. There was no help to get in right away because (Coleman Health Services) was so backed up,” Urban said. “There can never be enough resources because what happens is all these resource centers and rehabilitation centers, they keep you for a period of time then they release you, and a lot of people when they get released like that, they don’t have adequate support for more of a long-term stay, more of them tend to relapse.”
Urban said her son got treatment for free with Medicaid, but in her experience, organizations prioritize people who have insurance.
Auglaize County Sheriff Mike Vorhees also mentioned a challenge with people not having a way to get to treatment.
“We don’t provide transportation yet, but that’s something that we’re working on,” Vorhees said in regard to the services Project ACART provides. “It depends on who it is. If it’s an elderly person, we can work with the Council on Aging; if it’s a veteran we go through Veterans Services.”
Financially, Declercq said Lighthouse Behavioral Health Solutions’ case managers help people apply for Medicaid, or the local mental health board has options for those who don’t qualify for Medicaid.
“One of the most frustrating barriers for seeking treatment is those with commercial insurance or Medicare, as those companies only pay for very limited services,” Declercq said. “Commercial plans typically pay for a short detox stay and limited individual/group counseling sessions, but do not pay for the intensive level of treatment that a program like Lighthouse offers.”
“Thirty days of treatment and/or 10 individual counseling sessions are not enough to truly treat a person who has been in active addiction for years,” Declercq continued. “Oftentimes even one year of intense treatment only touches the surface of the issues that someone in addiction needs to address.”
Available help
Project ACART has only been around about a year, and Boneta is working part-time and is the only employee. She has reached out to 19 people so far, and only two have denied treatment. She put together a resource guide in 2023 including mental health and substance abuse centers; residential detox treatment centers; 24/7 support services; substance use support groups; where to find Narcan; food pantries, hot meals and clothing; housing assistance and shelters; and low income and subsidized housing.
Boneta received help from peer support specialists through Coleman Health Services during her addiction. Now, as a peer support specialist, she uses a combination of her own experiences and formal training. She equated her role to being like a cheerleader. She is available to clients day and night to connect them to agencies to get help or just talk about their struggles.
“I meet people where they’re at and treat every situation differently. Some of the things I do are assessing needs and struggles, setting goals, advocating for my peers, giving resources, facilitating engagement with my peers and their families or service providers, and encouraging and uplifting them,” Boneta said.
Project ACART’s services are also free because of an Ohio grant.
“Many people in active addiction do not have housing, food, clothing, money or insurance, but they should still have the opportunity to get the help they need,” Boneta said.
Declercq said Lighthouse Behavioral Health Solutions also recently opened a peer support center in Lima for clients to have a place to go for sober activities.
“Downtime/boredom is often a trigger for people who are early in recovery, so this gives them a place to fill that time in a positive way,” Declercq said. “Our peer supporters offer a unique support system to our clients because they are people with past lived experience in addiction who are able to show them that life beyond addiction is achievable and fulfilling.”
Coleman’s seemed to be the go-to choice for law enforcement referrals, and Urban also directs people to the organization.
“My oldest son was a success story, he went to Coleman’s, got treatment, got on the MAT (medication-assisted treatment) program, Suboxone, and he’s thriving today. Owns his own house, owns his own business, married, doing absolutely wonderful. He’s like eight years clean,” Urban said.
Ohio Department of Commerce Division of Securities Recovery Within Reach program also provides a list of recovery resources and offers ways to pay for treatment.
Source: https://www.limaohio.com/top-stories/2024/09/06/local-organizations-share-addiction-experiences-challenges-resources/
Methods: We recruited 58 MA-dependent young adult females from a compulsory isolation drug rehabilitation center in Sichuan Province and randomly divided them into an MBRP group (n = 29) and a control group (n = 29) according to their degree of psychological craving. The MBRP group received 2 hours of MBRP training twice a week for 4 weeks, alongside routine treatment at the drug rehabilitation center. Meanwhile, the control group solely received routine treatment at the drug rehabilitation center without any additional interventions. The assessment was conducted before and immediately after the intervention, with the Compulsive Drug Use Scale (OCDUS) used to assess craving and the Five-Factor Mindfulness Scale (FFMQ) used to assess trait mindfulness. Also, a “mental feedback monitoring balance” instrument was used to assess concentration and relaxation during some training sessions. This randomized trial was conducted to evaluate the effectiveness of decreasing psychological craving and increasing trait mindfulness.
Results: At baseline, there were no significant differences in total or dimension scores for FFMQ or OCDUS between the two groups (all P > 0.05). After the intervention, the repeated measures ANOVA showed a significant time main effect on changes in observing, non-judging, and non-reacting scores (all P < 0.05), and a significant interaction effect between time and group on both FFMQ total score and OCDUS score (P < 0.01 or P < 0.05). Mental feedback monitoring indicated significant improvement in concentration and relaxation after breath meditation exercises (P < 0.05 or P < 0.001). Additionally, the MBRP group showed improved relaxation during the body scan exercise (P < 0.01).
Conclusion: MBRP training can improve the trait mindfulness of MA addicts and reduce psychological cravings effectively.
The full article can be accessed via the source link below:
Source: https://www.frontiersin.org/journals/psychiatry/articles/10.3389/fpsyt.2024.1339517/full
In recent years, police forces in England and Wales have worked more closely with health, education and other local partners to address social issues, such as drug use, youth violence and people in mental health crisis.[1] This aims to ensure that vulnerable people are supported by the most appropriate professional, and that certain complex social issues are not automatically met with a criminal justice response.
These initiatives are sometimes referred to as public health approaches to policing.[2] They can include interventions aimed at preventing offending altogether (for example, early years school-based programmes), as well as ones covering offenders or people coming into contact with the police.[3]
In 2018, organisations representing public health bodies, health services, voluntary organisations and police forces signed an agreement to work more closely together to prevent crime and protect the most vulnerable people in England.[4] Public Health Scotland and Police Scotland announced a formal collaboration in 2021.[5] In 2019, Public Health England and the College of Policing published a discussion paper on public health approaches to policing,[6] and the Association of Police and Crime Commissioners issued guidance in 2023 to support implementation of such approaches.3
Research has found that cooperation between police and health services can help to improve social outcomes. For example:
There are examples of police forces working with health partners and other agencies to improve responses to vulnerable people in England and Wales:
Since 2020, Scotland has seen increasing use of diversion from prosecution schemes.[21] In October 2024, the UK’s first official consumption facility for illegal drugs, including heroin and cocaine, was opened in Glasgow.[22]
In 2023, HM Inspectorate of Constabulary and Fire & Rescue Services noted how police forces were often the “service of last resort” doing the work of other public services, especially with regards to mental ill health.[23] For some vulnerable people, police custody may provide their only space for healthcare interventions.10 Both police forces and voluntary organisations suggest that, at a time when police capacity is under pressure, public health approaches can reduce the amount of time police officers spend dealing with people with complex health needs, who may be referred to other health, care or support services.[24],[25] However, this can also lead to demand and capacity pressures being displaced onto these services.
For example, drug diversion schemes may increase the demand on local drug treatment services, which themselves are facing significant pressures. In her independent review of drugs for the government in 2021, Dame Carol Black raised significant concerns about the capacity and resourcing of drug treatment services in England, and the impact of funding reductions.[26] The Criminal Justice Alliance has called for increased funding for local drug services, to accommodate people being diverted away from the criminal justice system.[27]
The government’s 10-year drug strategy (2021) committed to invest £533 million into local authority commissioned substance misuse treatment services in England from 2022/23 to 2024/25, as part of its aim to “rebuild local authority commissioned substance misuse treatment services in England”.[28] In 2023, the Home Affairs Committee called for all police forces in England and Wales to adopt drug diversion schemes.[29] It also expressed concern about the long-term sustainability and security of funding for the drug treatment and recovery sector.26
Similar pressures in mental health services have led to concerns about the safety of the national rollout of Right Care, Right Person. In November 2023, the Health and Social Care Committee identified urgent questions around the available funding for health services, and the lack of evaluation, in the rollout of the scheme[30] The Royal College of Psychiatrists and the Royal College of Nurses agreed that people with mental illness should be seen as quickly as possible by a mental health professional.[31],[32] However, they and other health, local government, and mental health charities, have expressed several concerns about the programme. These include: the speed and consistency of implementation, lack of funding, the potential for gaps in provision, and increased welfare risks.[33],[34],[35],[36]
Outside the UK, some public health approaches have involved a significant shift away from enforcing drug possession for personal use through the criminal justice system.[37] For example:
Citing international examples, some drug policy experts have called on the government to go further in its adoption of a public health approach to drug use.37 The Home Affairs Committee stated in 2023 that the government’s drug strategy should have adopted a broader public health approach, and called for responsibility for misuse of drugs to be jointly owned by the Home Office and Department of Health and Social Care.26 In 2019, the Health and Social Care Committee recommended the government shift responsibility for drugs policy from the Home Office to the Department of Health and Social Care, and for the government to “look closely” at the Portugal model for decriminalisation of drug possession for personal use.[42]
However, Portugal’s approach has also faced criticism. For example, a research review in 2021 highlighted continued social and political resistance to some of the measures 20 years after being introduced.[43] A 2023 editorial in the Lancet highlighted how a recent rise in the use of illicit drugs in Portugal had led to renewed criticism of the policy.[44] More recently, some states in North America have reversed decriminalisation policies, reportedly due to adverse consequences of drug decriminalisation.33,[45], [46]
This points to a mixed evidence base internationally for a fully public health approach to drug use. However, it may be difficult to compare international examples, given the different models of decriminalisation that have been adopted, and in a variety of social, economic, political and legal systems.[47]
Source: DOI: https://doi.org/10.58248/HS62
At the behest of the district’s mayor, DuPont developed a D.C.-based clinic, the Narcotics Treatment Administration. It treated more than 15,000 heroin addicts over the next three years, and the D.C. crime rate plummeted by 50%, in a direct correlation.
Robert L. “Bob” DuPont, born in 1936, graduated from Emory University and Harvard Medical School and completed his psychiatric training at the National Institutes of Health. He became the first director of the newly-created National Institute on Drug Abuse (NIDA), where he created a first-of-its-kind comprehensive training program for doctors, nurses, and counselors working in addiction treatment programs. Drug overdose deaths began declining, from from 6,413 to 2,492 by 1980.
In 1978, DuPont left government service to create the Institute for Behavior and Health (IBH), a think tank focusing on drug policy. Dupont has published more than 400 journal articles and 15 books, most recently Chemical Slavery: Understanding Addictions and Stopping the Drug Epidemic (2018).
The IBH conducted the first national study of doctors dependent on drugs and alcohol, their treatment, and five-year outcomes. “Physicians are given a comprehensive assessment by a team of professionals and get treatment for comorbidities, but the focus is on their addictions. They typically attend a month or more of residential treatment and, as outpatients, are monitored for five years with random drug and alcohol testing. If they miss a scheduled test or test positive for any drug, including alcohol, they are taken out of their practice again, assessed, and sent back to treatment.”
DuPont points out that many doctors who entered the program were initially resentful because they didn’t think there was anything wrong with them—typical of individuals with substance use disorder from all walks of life. Yet, most physicians greatly value their medical license, and the overwhelming majority cooperated because participation and success meant they could continue to practice medicine.
His study of nearly 1,000 drug-addicted physicians closely monitored for five years showed what is possible for the rest of the population. Seventy-eight percent never tested positive for drugs or alcohol, an excellent record. In addition, of those who did have a positive or missed drug test, nearly two-thirds never had a second positive test.
A follow-up study of physicians who successfully completed treatment and monitoring contracts five or more years ago showed that more than 95% were still in recovery. Physicians rated the treatment they had received as important to their recovery but said the most valued part of their care was involvement in the 12 steps.
DuPont says many people don’t realize that it’s rarely just one drug abused by most problematic substance users. And that is particularly true of individuals who die from drug overdoses, in whom two or more drugs are often identified post-mortem.
He also notes that many drugs used today are not in their natural forms but instead are ultra-potent synthetics, like fentanyl. In 2022, about 111,000 people died, and in 2023, about 108,300 people died of drug overdose. .
Early diagnosis and treatment is key
The earlier patients are diagnosed and treated, the better their chances of achieving and sustaining recovery, says DuPont. Many people can stop using substances for some period. However, the real problem is not drug withdrawal, as many people believe, but, instead, the repeated relapses. Yet he has known many individuals with seemingly hopeless drug or alcohol issues who emerged sober and productive. He largely credits organizations like Alcoholics Anonymous and Narcotics Anonymous.
Prevention is best
Whenever possible, prevention of drug use is best, particularly among young people. Not only is adolescence a time when most addictions begin, it’s also a time when the brain is uniquely vulnerable..
DuPont now focuses on youth substance-use prevention: no alcohol, nicotine, marijuana/THC, or other drugs by those under age 21. He notes that the percentage of 12th graders who report never using in their lifetime has increased from around 26% in 2018 to 32% in 2023. The trend is also evident in younger students. DuPont emphasizes, “This trend is key to reversing decades of pain, suffering, and addictions.“
At age 88, Robert DuPont, M.D., advocates for treatment research, long-term treatment with outcome reporting, mental health treatment parity (as important as physical health), and prevention. Recovery, he insists, is possible.
Today, the U.S. Department of Health and Human Services’ (HHS) Substance Abuse and Mental Health Services Administration (SAMHSA) released the results of the 2023 National Survey on Drug Use and Health (NSDUH), which shows how people living in United States reported their experience with mental health conditions, substance use and pursuit of treatment. The 2023 NSDUH report includes selected estimates by race, ethnicity and age group. The report is accompanied by two infographics offering visually packaged highlight data as well as visual data by race and ethnicity.
“Each year, data from the annual NSDUH provides an opportunity to identify and address unmet healthcare needs across America. We’re pleased to see that more people received mental health treatment in 2023 than the previous year,” said Miriam E. Delphin-Rittmon, Ph.D., HHS Assistant Secretary for Mental Health and Substance Use and the leader of SAMHSA. “Also, to build upon increasing accessibility to data, this year’s release features two infographic reports: one focusing on race and ethnicity and one highlighting selected overall data.”
The 2023 NSDUH Report includes the following selected key findings.
Mental Health:
Substance Use:
Services and Recovery:
About the National Survey on Drug Use and Health
Conducted by the federal government since 1971, the NSDUH is a primary source of statistical information on self-reported substance use and mental health of the U.S. civilian, noninstitutionalized population 12 or older. For the 2023 NSDUH national tables and some reports, statistical testing was conducted between estimates from different years (e.g., past month alcohol use in 2023 vs. the estimate in 2022). Where testing involved 3 years of comparable data for 2021 to 2023, pairwise testing was conducted between estimates in these years (i.e., 2021 vs. 2022, 2021 vs. 2023, and 2022 vs. 2023). Statistical tests for overall trends from the baseline year to the current year will not be conducted until four comparable NSDUH data points are available. The NSDUH measures include:
Addressing the nation’s mental health crisis and drug overdose epidemic is a top priority of the Biden-Harris Administration and are core pillars of the Administration’s Unity Agenda. The President’s Unity Agenda is operationalized through the HHS Overdose Prevention Strategy, the HHS Roadmap for Behavioral Health Integration, and the National Strategy for Suicide Prevention.
If you or someone you know is struggling or in crisis, help is available. Call or text 988 or chat at 988lifeline.org. To learn how to get support for mental health, drug or alcohol issues, visit FindSupport.gov. If ready to locate a treatment facility or provider, go directly to FindTreatment.gov or call 800-662-HELP (4357).
This page is part of the European Drug Report 2024, the EMCDDA’s annual overview of the drug situation in Europe.
The use of illicit drugs is a recognised contributor to the global burden of disease. Interventions designed to reduce this burden include prevention activities, intended to reduce or slow the rate at which drug use may be initiated, and the offer of treatment to those who have developed drug problems. A complementary set of approaches goes under the general heading of harm reduction. Here the emphasis is on working non-judgementally with people who use drugs in order to reduce the risks associated with behaviours that are mostly associated with adverse health outcomes, and more generally to promote health and well-being. Probably the best known of these is the provision of sterile injecting equipment to people who inject drugs, with the aim of reducing the risk of contracting an infectious disease. Over time these sorts of approaches appear to have contributed to the relatively low rate, by international standards, of new HIV infections now associated with injecting drug use in Europe. Over the last decade, as patterns of drug use have changed and the characteristics of those who use drugs have also evolved, to some extent, harm reduction interventions have also needed to adapt to address a broader set of health outcomes and risk behaviours. Prominent among these are reducing the risk of drug overdose and addressing the often-considerable and complex health and social problems faced by people who use drugs in more marginalised and socially excluded populations.
Chronic and acute health problems are associated with the use of illicit drugs, and these can be compounded by factors such as the properties of the substances, the route of administration, individual vulnerability and the social context in which drugs are consumed. Chronic problems include dependence and drug-related infectious disease, while there is a range of acute harms, of which drug overdose is perhaps the best documented. Although relatively rare at the population level, the use of opioids still accounts for much of the morbidity and mortality associated with drug use. Injecting drug use also increases risks. Correspondingly, working with opioid users and those who inject drugs has been historically an important target for harm reduction interventions and also the area where service delivery models are most developed and evaluated.
Reflecting this, some harm reduction services have become increasingly integrated into the mainstream of healthcare provision for people who use drugs in Europe over the last three decades. Initially, the focus was on expanding access to opioid agonist treatment and needle and syringe programmes as a part of the response to high-risk drug use, primarily targeting injecting use of heroin and the HIV/AIDS epidemic. Recent joint EMCDDA-ECDC guidance on the prevention and control of infectious diseases among people who inject drugs recommends providing opioid agonist treatment to prevent hepatitis C and HIV, as well as to reduce injecting risk behaviours and injecting frequency, in both the community and prison settings. The guidelines also recommend the provision of sterile injecting equipment alongside opioid agonist treatment to maximise the coverage and effectiveness of the interventions among people who inject opioids.
To access the full report, please click on the link below:
Source: https://www.euda.europa.eu/publications/european-drug-report/2024/harm-reduction_en
This report is based on information provided to the EMCDDA by the EU Member States, the candidate country Türkiye, and Norway, in an annual reporting process.
The purpose of the current report is to provide an overview and summary of the European drug situation up to the end of 2023. All grouping, aggregates and labels therefore reflect the situation based on the available data in 2023 in respect to the composition of the European Union and the countries participating in EMCDDA reporting exercises. However, not all data will cover the full period. Due to the time needed to compile and submit data, many of the annual national data sets included here are from the reference year January to December 2022. Analysis of trends is based only on those countries providing sufficient data to describe changes over the period specified. The reader should also be aware that monitoring patterns and trends in a hidden and stigmatised behaviour such as drug use is both practically and methodologically challenging. For this reason, multiple sources of data are used for the purposes of analysis in this report. Although considerable improvements can be noted, both nationally and in respect to what is possible to achieve in a European-level analysis, the methodological difficulties in this area must be acknowledged. Caution is therefore required in interpretation, in particular when countries are compared on any single measure. Caveats relating to the data are to be found in the online Statistical Bulletin 2024, which contains detailed information on methodology, qualifications on analysis and comments on the limitations in the information set available. Information is also available there on the methods and data used for European-level estimates, where interpolation may be used.
This page draws on the latest data available to provide an overview of the current situation and emerging drug issues affecting Europe, with a focus on the year up to the end of 2023. The analysis presented here highlights some developments that may have important implications for drug policy and practitioners in Europe.
Understanding Europe’s drug situation in 2024 – key developments
Analysis of the supply-related indicators for commonly used illicit drugs in the European Union suggests that availability remains high across all substance types. On this page, you can find an overview of drug supply in Europe based on the latest data, supported by the latest time trends in drug seizures and drug law offences, together with 2022 data on drug production and precursor seizures.
Drug supply, production and precursors – the current situation in Europe
Cannabis remains by far the most commonly consumed illicit drug in Europe. On this page, you can find the latest analysis of the drug situation for cannabis in Europe, including prevalence of use, treatment demand, seizures, price and purity, harms and more.
Cannabis – the current situation in Europe
Cocaine is, after cannabis, the second most commonly used illicit drug in Europe, although prevalence levels and patterns of use differ considerably between countries. On this page, you can find the latest analysis of the drug situation for cocaine in Europe, including prevalence of use, treatment demand, seizures, price and purity, harms and more.
Cocaine – the current situation in Europe
Amphetamine, methamphetamine and, more recently, synthetic cathinones are all synthetic central nervous system stimulants available on the drug market in Europe. On this page, you can find the latest analysis of the drug situation for synthetic stimulants in Europe, including prevalence of use, treatment demand, seizures, price and purity, harms and more
Synthetic stimulants – the current situation in Europe
MDMA is a synthetic drug chemically related to the amphetamines, but with somewhat different effects. In Europe, MDMA use has generally been associated with episodic patterns of consumption in the context of nightlife and entertainment settings. On this page, you can find the latest analysis of the drug situation for MDMA in Europe, including prevalence of use, seizures, price and purity and more.
MDMA – the current situation in Europe
Heroin remains Europe’s most commonly used illicit opioid and is responsible for a large share of the health burden attributed to illicit drug consumption. Europe’s opioid problem, however, continues to evolve in ways that are likely to have important implications for how we address issues in this area. On this page, you can find the latest analysis of the drug situation for heroin and other opioids in Europe, including prevalence of use, treatment demand, seizures, price and purity, harms and more.
Heroin and other opioids – the current situation in Europe
The market for new psychoactive substances is characterised by the large number of substances that have emerged, with new ones being detected each year. On this page, you can find an overview of the drug situation for new psychoactive substances in Europe, supported by information from the EU Early Warning System on seizures and substances detected for the first time in Europe. New substances covered include synthetic and semi-synthetic cannabinoids, synthetic cathinones, new synthetic opioids and nitazenes.
New psychoactive substances – the current situation in Europe
Alongside the more well-known substances available on illicit drug markets, a number of other substances with hallucinogenic, anaesthetic, dissociative or depressant properties are used in Europe: these include LSD, hallucinogenic mushrooms, ketamine, GHB and nitrous oxide. On this page, you can find the latest analysis of the situation regarding these substances in Europe, including seizures, prevalence and patterns of use, treatment entry, harms and more.
Other drugs – the current situation in Europe
Despite a continued decline in injecting drug use over the past decade in the European Union, this behaviour is still responsible for a disproportionate level of both acute and chronic health harms associated with the consumption of illicit drugs. On this page, you can find the latest analysis of injecting drug use in Europe, including key data on prevalence at national level and among clients entering specialist treatment, as well as insights from studies on syringe residue analysis and more.
Injecting drug use – the current situation in Europe
People who inject drugs are at risk of contracting infections through the sharing of drug use paraphernalia. On this page, you can find the latest analysis of drug-related infectious diseases in Europe, including key data on infections with HIV and hepatitis B and C viruses.
Drug-related infectious diseases – the current situation in Europe
Estimating the mortality attributable to drug use is critical for understanding the public health impact of drug use and how this may be changing over time. On this page, you can find the latest analysis of drug-induced deaths in Europe, including key data on overdose deaths, substances implicated and more.
Drug-induced deaths – the current situation in Europe
Opioid users represent the largest group undergoing specialised drug treatment, mainly in the form of opioid agonist treatment. On this page, you can find the latest analysis of the provision of opioid agonist treatment in Europe, including key data on coverage, the number of people in treatment, pathways to treatment and more.
Opioid agonist treatment – the current situation in Europe
Harm reduction encompasses interventions, programmes and policies that seek to reduce the health, social and economic harms of drug use to individuals, communities and societies. On this page, you can find the latest analysis of harm reduction interventions in Europe, including key data on opioid agonist treatment, naloxone programmes, drug consumption rooms and more.
Harm reduction – the current situation in Europe
The European Drug Report 2024 was designed as a digital-first product, structured by modules, and optimised for online reading. Within each chapter, you may download a PDF version of the page. We are also making available here a PDF version of the full report (all modules and annex tables combined). Please note that some errors may have occurred during the transformation process and that it is possible that this version does not contain all corrections made since the report was first published (please check the last updated date).
Download full PDF version of the European Drug Report 2024 (16 MB, last updated 14.06.2024)
Source: https://www.euda.europa.eu/publications/european-drug-report/2024_en
Public health initiatives and the development of cardioprotective medications have led to an increase in life expectancy in the past six decades, giving rise to an ageing population.
This ageing population is suffering from a different set of medical issues than the population a century ago, with cancer, coronary heart disease, dementia, and stroke being the four leading causes for mortality and morbidity in England.
In 2019, these four conditions accounted for 59% of all deaths and 5·1 million disability-adjusted life-years in England.
Research investment is essential to combat major public health challenges, facilitating the development of new treatments and interventions that can improve rates of prevention, treatment, or management of diseases, enhancing quality of life and reducing their economic burden. However, it is important that the distribution of research funding across diseases is proportionate to their respective impact on society. In 2008, a UK study (Dementia 2010) evaluated the economic costs of, and research investment into dementia, and compared these costs and investments with those for cancer, coronary heart disease, and stroke.
Such estimates are important to inform health policy and identify diseases in need of greater investment,
with successive UK Governments having placed a greater priority for research funding in dementia.
CPRD Aurum is a large database of routinely recorded primary care electronic health records of patients from 738 general practices in England (10% of practices), covering 13% of the population.
The database contains information on symptoms, diagnoses, prescriptions, referrals, tests, immunisation, and medical staff. Primary care and secondary care diagnosis codes were used to identify the four conditions of interest. CPRD Aurum codes used to diagnose patients in primary care are reported in the appendix (pp 2–55). CPRD records were then linked to secondary care records contained in HES using Aurum (version 2.3) from August, 2019. In secondary care records, cancer was defined by ICD-10 category codes I00–I99, coronary heart disease by codes I20–I25, dementia by codes F00–F03 and G30, and stroke by codes I60–I69. The use of CPRD Aurum for this study was approved by the independent scientific advisory committee for CPRD research (protocol reference CPRD00120051). CPRD obtains annual research ethics approval from the UK’s Health Research Authority Research Ethics Committee (05/MRE04/87) to receive and supply patient data for public health research. No further ethical permissions were required for the analyses of these anonymised patient-level data. The analysis was based on 4 161 588 patients registered on Jan 1, 2018, in a CPRD general practice with HES-linked records, omitting all children younger than 1 year (appendix pp 56–57).
Informal and formal care information was obtained from the English Longitudinal Study on Ageing (ELSA).
ELSA collects data from people older than 50 years, with spouses from age 40 years also included, to understand all aspects of ageing in England. More than 18 000 people have taken part in the study since it started in 2002, with the same people re-interviewed every 2 years. For this study, we used information on wave 9 (2018–19; appendix pp 58–59). Access to ELSA, through the UK Data Service, was obtained as part of the UK Access Management Federation. ELSA has been approved by the National Research Ethics Service (London Multicentre Research Ethics Committee [MREC/01/2/91]).
Of the more than 10 million people in England aged 65 years or older in 2018, 5% were living in a nursing or residential care home.
Using patient-level data from CPRD Aurum, we apportioned the proportion of people living in a nursing or residential care home in England due to cancer, coronary heart disease, dementia, and stroke (table 1; appendix pp 65–66). Nursing and residential home care home cost was valued at £837 per week,
taking into account the relative proportions of people living in nursing and residential homes,
and the local authority, not-for profit, and profit sector provision case mix.
Informal care costs were equivalent to the opportunity cost of unpaid care (ie, the time [work, leisure, or both] that carers forgo), valued in monetary terms, to provide unpaid care for relatives or friends with cancer, coronary heart disease, dementia, or stroke, and based on the conservative assumption that only patients limited in daily activities received care. We valued informal care using the proxy good method, in which an hour of informal care provided was valued using the labour market price of a close market substitute
(i,e. the mean hourly wage for a home care assistant [£7·85]).
Hence, for informal care, we multiplied the age-specific and gender-specific products of age-specific and gender-specific prevalence of cancer, coronary heart disease, dementia, and stroke in England;
the probability of living in the community (appendix p 66); the probability of being severely limited in daily activities as a result of each of the four conditions under study (appendix p 67); the probability of receiving informal care conditional on being limited in daily activities (appendix p 67); and the hours of informal care received, conditional on being limited in daily activities and receiving informal care (appendix p 67).
Formal care costs included the costs associated with paid care for patients living in the community, which was valued at £27·00 per h.
For formal care, we multiplied the age-specific and gender-specific products of age-specific and gender-specific prevalence of cancer, coronary heart disease, dementia, and stroke in England;
the probability of living in the community (appendix p 66); the probability of receiving formal care (appendix p 68); and the hours of formal care received, conditional on receiving formal care (appendix p 68).
Annual days off sick were obtained from the European Working Conditions Surveys.
To the total number of days of work due to sickness, we applied the proportion of absence that was attributable to cancer, coronary heart disease, dementia, and stroke, which was obtained from the UK Department of Works and Pensions (personal communication).
To calculate permanent absence from work due to sickness or disability, information on the numbers of working-age individuals receiving incapacity or disability benefits and not being able to work was obtained, including recipients of the disability living allowance, employment support allowance (ESA), and incapacity benefit by condition.
Given that recipients of ESA can work up to 45·82% of their time, we only included the proportion of time that was not worked.
Days of absence from work due to sickness or disability were multiplied by mean daily earnings.
Furthermore, for permanent absence, we used the friction period approach because absent workers are likely to be replaced, whereby only the first 90 days of work absence were counted.
We assumed an initial working age of 15 years and a maximum age of retirement of 79 years. Age-specific and gender-specific deaths due to cancer, coronary heart disease, dementia, and stroke were obtained.
The number of potential working years lost was then estimated as the difference between the age at death and maximum age of retirement. Each lost year of working life was valued using average annual earnings.
However, not all of the population is economically active until age 79 years; hence, age-specific and gender-specific unemployment and activity rates
were applied to the potential foregone earnings. Following UK-recommended guidelines, future earnings lost due to mortality were discounted to present values using a 3·5% annual rate.
Finally, we projected the costs estimated for 2018 to 2050 based on future projections of the population alone,
excluding other factors such as epidemiological trends of the four conditions under investigation, risk factor prevalence rates, and life expectancy.
For this, we applied age-specific and gender-specific rates of resource use, prevalence, mortality, and disability observed in 2018 to the predicted distribution of the population in 2050. We valued resource use in 2050 using 2018 costs. For more details, see the appendix (pp 69–71).

The population of England, excluding those younger than 1 year, is expected to increase from 55 million in 2018 to 65 million in 2050 (18% increase), with the population aged 65 years or older projected to increase by 49% (from 10 million to 15 million).
Assuming no changes in age-specific and gender-specific prevalence rates, this population increase will increase the number of people with cancer by 39% (2·0 million), coronary heart disease by 45% (2·3 million), dementia by 81% (1·2 million), and stroke by 41% (0·8 million; appendix p 69).
These increases in the overall disease prevalence will result in cost increases between 2018 and 2050 of 40% (95% CI 39–41) to £26·5 billion (25·7–27·3) for cancer, 54% (53–55) to £19·6 billion (18·9–20·2) for coronary heart disease, 100% (97–102) to £23·5 billion (19·3–25·3) for dementia, and 85% (84–86) to £16·0 billion (15·3–16·6) for stroke (table 3). Costs with the highest increases are those related to social care, which are projected to rise between 2018 and 2050 by 88% (95% CI 86–90) to £2·9 billion (2·7–3·3) for cancer, 91% (90–92) to £4·4 billion (4·1–4·6) for coronary heart disease, 110% (109–111) to £13·5 billion (12·1–14·8) for dementia, and 109% (107–108) to £7·1 billion (6·6–7·5) for stroke (figure 2).

Whereas a previous study has assessed the overall costs of chronic conditions, our study made use of individual patient-level data to generate more precise cost estimates for cancer, coronary heart disease, dementia, and stroke, using the same methodology and sources across conditions. Previously the total costs of dementia in the UK were calculated as £23·4 billion, followed by cancer (£12·0 billion), coronary heart disease (£7·8 billion), and stroke (£5·0 billion).
These estimates are not comparable with the findings in this study, possibly due to methodologies and sources of data varying considerably across conditions.
Our results show that the areas of the economy bearing these costs differed substantially by disease area. For example, health-care costs of dementia accounted for 13% (£1·5 billion) of the total, with most costs being borne by the social care system (£6·4 billion, 55% of total costs). By contrast, in cancer, the majority of costs were borne by the labour market, with £8·3 billion in lost productivity (44% of total costs). These findings are notable in that they further emphasise the need for interventions designed to prevent or screen for early-stage disease. For cancer and, to a lesser extent, coronary heart disease, with so much of the cost borne by the labour market, interventions that prevent the disease will not only increase the health of the population and reduce health-care costs, but also improve labour productivity. However, these findings also raise important questions about perceived fairness and equality.
In the UK, about 90% of hospital cases, which according to our findings is where most of the care of patients with cancer or coronary heart disease takes place, is funded by the government (data are from the Eurostat database). By contrast, for dementia and, to a lesser extent, stroke, most of the care takes place in either the social care system, of which 60% is funded by the government, or by relatives and friends through informal care (data are from the Eurostat database). Therefore, patients with dementia and stroke are substantially at higher risk of having to fund their care themselves than those with cancer or coronary heart disease.
Our study also shows the effect of the projected population ageing over the coming decades. On the basis of demographic change alone, we project that the costs of cancer will increase by 40%, those of coronary heart disease by 54%, those of dementia by 100%, and those of stroke by 85%. With the population aged 65 years or older projected to increase by 49%, the costs with the fastest projected rise will be, averaged across all four conditions, for social care, with a 104% projected increase in costs, and informal care, with a projected increase of 78%. Therefore, research funding into interventions aimed to prevent, treat, and care for disease are required as a way to help to reduce or mitigate this projected increase in costs and improve health, especially in those conditions—ie, stroke and dementia—seeing the fastest increase in costs, and that historically have received the lowest levels of research funding.
The limitations of this study should be noted. Our results are based on diagnostic coding from both primary and secondary care records, rather than on careful ascertainment of patients through multiple and overlapping methods such as in population-based cohort studies. Therefore, our results might not reflect the absolute prevalence and costs of disease. Given that there is no single and simple diagnostic test for dementia, this under-ascertainment of disease in routinely collected health data or surveys might be most prevalent in dementia.
The failure to identify these undiagnosed cases might explain the relatively low levels of health-care resource use identified in CPRD Aurum due to dementia.
However, in ELSA, respondents were not explicitly asked for supervisory activities received, with our results likely to be an underestimate. We were unable to quantify the costs of formal and informal care in people younger than 40 years. This will, inevitably, have reduced our total estimates of costs, especially for cancer and stroke, where people younger than 40 years account for 6% (110 000) and 8% (60 000) of cases, respectively, compared with 2% (41 000) for coronary heart disease and less than 1% (5000) for dementia.
Finally, our projection of costs from 2018 to 2050 was based on future projections of the population alone, and might be considered simplistic. Our projections did not include other factors, such as epidemiological trends of the four conditions under investigation or the predicted rise in comorbidities predicted for England.
For example, analyses based on ELSA have projected the costs of dementia in the future based on current trends in cardiovascular disease incidence rates.
In addition, new treatments that prevent, slow progression, or successfully treat the four conditions under study, will undoubtedly affect the projected costs estimated in this study.
Source: https://www.thelancet.com/journals/lanhl/article/PIIS2666-7568(24)00108-9/fulltext
|
|
National Institute on Drug Abuse Director Nora Volkow explains the need to leverage the successes of HIV care to prevent overdose deaths. HIV and substance use are inextricably linked. An analysis of the New York City HIV surveillance registry found that in 2017, rates of overdose deaths for people with HIV were more than double overall overdose death rates for the city, but that 98% of those who died of overdose had been linked to HIV care after their HIV diagnosis and that more than three-quarters had been retained in care. This highlights an overlooked opportunity to save lives. Drug overdose claims more lives of people with HIV than HIV-related illness. Volkow says 81% of people who received an HIV diagnosis in 2019 in the U.S. were linked to HIV care within a month, 66% received care and 50% were retained in care. It is sometimes hard to reach people who use drugs with substance use treatment or harm reduction, but when people with HIV seek and receive treatment for HIV, it presents a promising opportunity to deliver addiction services. Delivering naloxone and overdose education in HIV care settings is a relatively easy way to prevent overdose deaths.
Source: We should leverage the successes of HIV care to prevent overdose mortality (National Institute on Drug Abuse)
Lawmakers who backed hemp legalization in the 2018 Farm Bill expected the plant to be used for textiles and nonintoxicating supplements. They did not realize that, with some chemistry, hemp can get you high. People anywhere in the U.S. can use hemp-derived THC without breaking federal law. Hemp and marijuana are varieties of the same plant species. Marijuana is defined by its high content of delta-9 THC. Hemp contains very little delta-9 THC but can contain a large amount of CBD, a cannabinoid that does not get you high. The Controlled Substances Act explicitly outlawed both hemp and marijuana. The Farm Bill defines hemp in a way that allows the plant and products made with it as long as they contain less than 0.3% delta-9 THC, making it seemingly legal to convert CBD into delta-8 THC as long as the process started with a plant that contained less than 0.3% delta-9 THC. The Farm Bill also appears to authorize the creation of hemp-based delta-9 THC products as long as the total delta-9 content is 0.3% or less of the product’s dry weight. The hemp-derived cannabinoid industry is now worth billions of dollars, and hemp-derived intoxicants are available at vape shops and gas stations, but they are not regulated.
Source: Congress Accidentally Legalized Weed Six Years Ago (The Atlantic)
National Institute on Drug Abuse Director Nora Volkow highlights the need to expand access to methadone. Only a fraction of people who could benefit from medications for opioid use disorder receive them, due to a combination of structural and attitudinal barriers. In 2023, the federal government eliminated the waiver requirement for buprenorphine. This year, it changed methadone regulations to make permanent the increased take-home doses of methadone established during the COVID emergency, along with other provisions aimed to broaden access. Changes implemented during COVID have not been associated with adverse outcomes, and patients reported significant benefits. Recent trials of models of methadone dispensing in settings other than methadone clinics have not supported concerns that making methadone more widely available will lead to harms. Data suggest that counseling is not essential for reducing overdoses or retaining patients in care, though it can be beneficial for some. It will also be critical to pursue other ways that methadone can safely be made more available to a wider range of patients.
Source: Guest Editorial: To Address the Fentanyl Crisis, Greater Access to Methadone Is Needed (American Society of Addiction Medicine)
Several top Centers for Disease Control and Prevention (CDC) officials testified before the House Energy and Commerce Committee to defend their agency’s programs. The hearing comes after House Republicans passed a budget that would cut CDC funding by 22%. Republicans claimed the agency has failed to fulfill its responsibilities and lost the public’s trust. Republicans accused the CDC of straying from its core mission of keeping the public healthy and said the agency is spending too much time on programs some GOP lawmakers deemed unnecessary or duplicative. The CDC program directors pushed back, citing work they deemed critical to public health. They emphasized three areas of focus – improving readiness and response to disease outbreaks, improving mental health and supporting young families. Allison Arwady, director of the National Center for Injury Prevention and Control, which would be eliminated under the proposed funding bill, spoke about why the center’s work on overdose prevention is necessary.
Source: CDC Defense (Politico); CDC fields GOP criticism at E&C hearing (Politico)
The federal Kids Online Health and Safety Task Force released a report with recommendations and best practices for safer social media and online platform use for youth. The report provides a summary of the risks and benefits of social media on the health, safety and privacy of young people; best practices for parents and caregivers; recommended practices for industry; a research agenda; and suggested future work, including for the federal government. In collaboration with the Task Force, the Center of Excellence on Social Media and Youth Mental Health is launching a variety of new web content, including best practices resources; age-based handouts for parents that pediatricians and others can distribute at well-check visits; new clinical case examples for pediatricians and other clinicians demonstrating how to integrate conversations about media use into health consultations with teens; and expanded content for teens. The report outlines 10 recommended practices for online service providers.
Source: Kids Online Health and Safety Task Force Announces Recommendations and Best Practices for Safe Internet Use (Substance Abuse and Mental Health Services Administration)
The Food and Drug Administration (FDA) authorized sales of certain tobacco-flavored Vuse Alto e-cigarette products from R.J. Reynolds. Vuse is the top-selling e-cigarette brand in the country, comprising more than 40% of the market. The marketing authorization applies to six tobacco-flavored pods, which are sealed, prefilled and nonrefillable. Last year, the FDA banned the sale of Vuse Alto menthol and fruit-flavored e-cigarettes, citing increasing popularity among kids.
Source: FDA allows sale of best-selling tobacco e-cigarette Vuse (The Hill)
Montana health officials are considering a new strategy to make naloxone more accessible. Drawing on a pool of behavioral health funds set aside by lawmakers in 2023, health officials have proposed installing two dozen naloxone and fentanyl test strip vending machines around the state at behavioral health drop-in centers and service locations for homeless people. The $400,000 plan to build, stock and maintain 24 vending machines for a year has not yet been approved by the governor. Different versions of the harm reduction vending machine model are being tried in at least 33 states, becoming increasingly popular especially in places with hard-to-reach populations. Some local public health groups in Montana have already begun using vending machines to distribute free naloxone, drug testing strips and other supplies, using public grants or private philanthropy, but these would be the first vending machines in Montana being directly funded by the state.
Source: Montana’s Plan To Curb Opioid Overdoses Includes Vending Machines (KFF Health News)
Iowa Governor Reynolds announced that the state’s opioid treatment and recovery providers can begin applying for $13 million in grants to expand or improve facilities or develop sober living housing options. The funding opportunities were announced in May as part of a larger $17.5 million investment to help address the opioid crisis. The $10 million Iowa Opioid Treatment and Recovery Infrastructure Grant will assist opioid treatment and recovery providers with physical infrastructure and capacity building. The Iowa Recovery Housing Fund includes $3 million for grants for nonprofit organizations to develop sober recovery housing. The grants leverage federal American Rescue Plan Act funds. An additional $1.5 million will be used for programs focused on prevention, including a $1 million education initiative for health care providers to support opioid-alternative pain management and $500,000 for a comprehensive multimedia opioid overdose prevention campaign. The remaining $3 million will support the completion of a residential addiction treatment center for adolescents.
Source: Gov. Reynolds announces grant funding, education programs to support opioid prevention, treatment and recovery (Iowa Governor Kim Reynolds)
The Legislative Analysis and Public Policy Association released two pieces of model state legislation. The first would require a state department of health and human services to apply for a Medicaid Reentry Section 1115 demonstration waiver to allow a state Medicaid program to cover pre-release services for Medicaid-eligible incarcerated individuals for up to 90 days prior to release and to require the department to conduct comprehensive monitoring and evaluation of the demonstration if the waiver is approved. The second is focused on reducing collateral consequences of conviction. It would establish a process for the identification, collection and publication of collateral consequences that impact individuals convicted of crimes; establish a process by which an individual can obtain a certificate of relief from certain collateral consequences before records are eligible to be sealed or expunged; establish mechanisms for the automatic sealing and expungement, as well as a process for petitioning; prohibit certain entities from inquiring into an individual’s criminal history; etc.
Source: Model Medicaid Reentry Section 1115 Demonstration Waiver Act; Model Relief from Collateral Consequences of Conviction Act (Legislative Analysis and Public Policy Association)
Some public health experts hope that mobile treatment programs will help increase access to methadone. Addiction experts say methadone is particularly important as the strength of street fentanyl has lessened the effectiveness of other medications and approaches for some. The mobile vans were approved by the federal government in 2021, lifting a moratorium on their use that had been in place since 2007. Their goal is to reach some of the millions of Americans with opioid use disorder that methadone clinics cannot. While the vans make treatment more accessible, the cost and ongoing restrictions limit the number of people that they can help, as well. Constructing and outfitting a methadone van costs about $375,000. They have to replicate the high-security environments of clinics, with a security guard, 360-degree cameras and a safe for the medication. There are now 42 vans registered nationally, though not all are operational yet.
Source: https://drugfree.org/drug-and-alcohol-news/policy-news-roundup-july-25-2024/
Posted July 29, 2024 Reviewed by Michelle Quirk
With this tragic news just in, there are several important things to say about the drug overdose situation in this country.
The first is this: It is important that we don’t talk about the more than 107,000 overdose deaths in the United States last year like it’s just a statistic.
These are people’s lives that ended, people like you and me. People with friends and loved ones who cared about them, and who wanted them to succeed.
This is where we are with the continuing drug epidemic, according to the recently released Centers for Disease Control and Prevention (CDC) data from 2023:
1. Greater availability of Narcan: I’m a huge advocate for this overdose reversal drug, which is naloxone in nasal spray form. I have argued often that it should be as ubiquitous as the red-boxed automated external defibrillators (AEDs) you now see in malls, hotel lobbies, schools, airports, and workplaces.
The U.S. Food and Drug Administration (FDA) took a big and meaningful step in that direction when it approved Narcan for over-the-counter use in March 2023. I have no doubt the increased availability of Narcan has helped bring the overdose numbers down, since Narcan targets opioids like fentanyl and heroin.
2. The stepping up of harm-reduction efforts: Harm reduction means reducing the health and safety dangers around drug use. The goal is to save lives and protect the health of people who use drugs through such measures as fentanyl test strips, overdose prevention sites, and sterilized injection equipment and services.
Harm reduction was a key plank of the White House’s 2022 National Drug Control Strategy aimed directly at the overdose epidemic. Countless harm-reduction efforts have gained traction at the local and state level as well. Again, this continued push may have helped bring down the overdose numbers last year.
3. Increased efforts around law enforcement drug seizures: Of the 107,543 people who overdosed in 2023, 74,702 (70 percent) of them did so after using the synthetic opioid fentanyl, which is many times more potent than heroin. For the first time in years, that number of deaths was lower than the year before.
Why? No doubt in part because 115 million pills containing fentanyl were seized by law enforcement in 2023. That compared to 71 million fentanyl-laced pills seized in 2022. These seizure efforts seem to be working, and they need to be stepped up even more.
Ultimately, the best way to save lives, end the opioid epidemic, and halt the spread of substance use disorder is to stop people from becoming addicted in the first place.
The big news: Statistics show that drug use may be trending down among young people. Even delaying the onset of addiction can change the trajectory of the problem, says Nora Volkow, MD, director of the National Institute on Drug Abuse.
When asked recently about the lower number of overdose deaths last year, Volkow said: “Research has shown that delaying the start of substance use among young people, even by one year, can decrease substance use for the rest of their lives. We may be seeing this play out in real time [in 2023]. The trend is reassuring.”
As the antismoking campaign that began in the 1960s showed us, massive and well-coordinated public health efforts can work.
Surgeon General warning labels, hard-hitting public service announcements, school-based programs—all of those had a cumulative effect on smoking habits in this country, especially among young people. Those efforts all targeted one thing: prevention.
We need to do much more of that in 2024 around opioids, methamphetamines, cocaine, and other lethal drugs. Lives depend on it.
Source: https://www.psychologytoday.com/us/blog/use-your-brain/202407/a-closer-look-at-107543-lives-lost-to-drug-overdoses
This blog was also published in the American Society of Addiction Medicine (ASAM) Weekly on July 24, 2024.
Growing evidence suggests that methadone is as safe and effective as buprenorphine for patients who use fentanyl. In a 2020 naturalistic follow-up study, 53% of patients admitted to methadone treatment who tested positive for fentanyl at intake were still in treatment a year later, compared to 47% for patients who tested negative. Almost all (99%) of those retained in treatment achieved remission. An earlier study similarly found that 89% of patients who tested positive for fentanyl at methadone treatment intake and who remained in treatment at 6 months achieved abstinence.
Methadone may even be preferable for patients considered to be at high risk for leaving OUD treatment and overdosing on fentanyl. Comparative effectiveness evidence is emerging which shows that people with OUD in British Columbia given buprenorphine/naloxone when initiating treatment were 60% more likely to discontinue treatment than those who received methadone (1). More research is needed on optimal methadone dosing in patients with high opioid tolerance due to use of fentanyl, as well as on induction protocols for these patients. It is possible that escalation to a therapeutic dose may need to be more rapid.
It remains the case that only a fraction of people who could benefit from medication treatment for OUD (MOUD) receive it, due to a combination of structural and attitudinal barriers. A study using data from the National Survey on Drug Use and Health (NSDUH) from 2019—that is, pre-pandemic—found that only slightly more than a quarter (27.8%) of people who needed OUD treatment in the past year had received medication to treat their disorder. But a year into the pandemic, in 2021, the proportion had dropped to just 1 in 5.
Efforts have been made to expand access to MOUD. For instance, in 2021, the U.S. Department of Health and Human Services (HHS) advanced the most comprehensive Overdose Prevention Strategy to date. Under this strategy, in 2023, HHS eliminated the X-waiver requirement for buprenorphine. But in the fentanyl era, expanded access to methadone too is essential, although there are even greater attitudinal and structural barriers to overcome with this medication. People in methadone treatment, who must regularly visit an opioid treatment program (OTP), face stigma from their community and from providers. People in rural areas may have difficulty accessing or sticking with methadone treatment if they live far from an OTP.
SAMHSA’s changes to 42 CFR Part 8 (“Medications for the Treatment of Opioid Use Disorder”) on January 30, 2024 were another positive step taken under the HHS Overdose Prevention Strategy. The new rule makes permanent the increased take-home doses of methadone established in March 2020 during the COVID pandemic, along with other provisions aimed to broaden access like the ability to initiate methadone treatment via telehealth. Studies show that telehealth is associated with increased likelihood of receiving MOUD and that take-home doses increase treatment retention.
Those changes that were implemented during the COVID pandemic have not been associated with adverse outcomes. An analysis of CDC overdose death data from January 2019 to August 2021 found that the percentage of overdose deaths involving methadone relative to all drug overdose deaths declined from 4.5% to 3.2% in that period. Expanded methadone access also was not associated with significant changes in urine drug test results, emergency department visits, or increases in overdose deaths involving methadone. An analysis of reports to poison control centres found a small increase in intentional methadone exposures in the year following the loosening of federal methadone regulations, but no significant increases in exposure severity, hospitalizations, or deaths.
Patients themselves reported significant benefits from increased take-home methadone and other COVID-19 protocols. Patients at one California OTP in a small qualitative study reported increased autonomy and treatment engagement. Patients at three rural OTPs in Oregon reported increased self-efficacy, strengthened recovery, and reduced interpersonal conflict.
The U.S. still restricts methadone prescribing and dispensing more than most other countries, but worries over methadone’s safety and concerns about diversion have made some physicians and policymakers hesitant about policy changes that would further lower the guardrails around this medication. Methadone treatment, whether for OUD or pain, is not without risks. Some studies have found elevated rates of overdose during the induction and stabilization phase of maintenance treatment, potentially due to starting at too high a dose, escalating too rapidly, or drug interactions.
Although greatly increased prescribing of methadone to treat pain two decades ago was associated with diversion and a rise in methadone overdoses, overdoses declined after 2006, along with methadone’s use as an analgesic, even as its use for OUD increased. Most methadone overdoses are associated with diversion and, less often, prescription for chronic pain; currently, 70 percent of methadone overdoses involve other opioids (like fentanyl) or benzodiazepines.
Recent trials of models of methadone dispensing in pharmacies and models of care based in other settings than OTPs have not supported concerns that making methadone more widely available will lead to harms like overdose. In two feasibility studies, stably maintained patients from OTPs in Baltimore, Maryland and Raleigh, North Carolina who received their methadone from a local pharmacy found this model to be highly satisfactory, with no positive urine screens, adverse events, or safety issues. An older pilot study in New Mexico found that prescribing methadone in a doctor’s office and dispensing in a community pharmacy, as well as methadone treatment delivered by social workers, produced better outcomes than standard care in an OTP for a sample of stably maintained female methadone patients.
Critics of expanded access to methadone outside OTPs sometimes argue that the medication should not be offered without accompanying behavioural treatment. Data suggest that counselling is not essential. In wait-list studies, methadone treatment was effective at reducing opioid use on its own, and patients stayed in treatment. However, counselling may have benefits or even be indispensable for some patients to help them improve their psychosocial functioning and reduce other drug use. How to personalize the intensity and the level of support needed is a question that requires further investigation.
Over the past two decades, the opioid crisis has accelerated the integration of addiction care in the U.S. with mainstream medicine. Yet methadone, the oldest and still one of the most effective medications in our OUD treatment toolkit, remains siloed. In the current era of powerful synthetic opioids like fentanyl dominating the statistics on drug addiction and overdose, it is time to make this effective medication more accessible to all who could benefit. The recent rules making permanent the COVID-19 provisions are an essential step in the right direction, but it will be critical to pursue other ways that methadone can safely be made more available to a wider range of patients with OUD. Although more research would be of value, the initial evidence suggests that providing methadone outside of OTPs is feasible, acceptable, and leads to good outcomes.
Source: https://nida.nih.gov/about-nida/noras-blog/2024/07/to-address-the-fentanyl-crisis-greater-access-to-methadone-is-needed
Cannabis or more commonly known as marijuana, is one of the most frequently used drugs in the United States. In 2022, marijuana became more popular than alcohol as the preferred daily drug of use among Americans. In the same year, it was found that 30 out of every 100 high school age students reported using the drug within the past 12 months, and 3 of every 50 reported using it daily.
Marijuana is often perceived as harmless, which has influenced its increased use by a factor of 15 within the past three decades, but this substance can have severe physical and mental health effects.
This blog will share the heart-wrenching stories of Brant Clark and Shane Robinson, as told by their families, along with a recent article by Alton Northup editor-in-chief of KentWired. Their lives were tragically cut short by marijuana induced psychosis.
Brant Clark

Ann Clark shares the heartbreaking story of her 17-year-old son, Brant, who experienced cannabis-induced psychosis leading to his tragic suicide. She recounts his rapid descent into hopelessness and the devastating impact on their family to raise awareness about the dangers of marijuana use on mental health.
Ann Clark shares the heartbreaking story of her 17-year-old son, Brant, who experienced cannabis-induced psychosis leading to his tragic suicide. She recounts his rapid descent into hopelessness and the devastating impact on their family to raise awareness about the dangers of marijuana use on mental health.
Brant Clark (pictured) was a happy and bright 17-year-old who reported using marijuana socially. However, during his last high school winter break, after smoking marijuana at a party with friends, he experienced a psychotic break believed to have been triggered by smoking a large amount of potent marijuana.
After the party Brent expressed to his mother his feelings of “emptiness and hopelessness”, and deep regret, lamenting his decision to smoke marijuana. Within two days of the onset of symptoms, Brant was admitted to the ER and psychiatric care unit. Tragically, three weeks later, he ended his own life, leaving behind a note revealing his intense mental anguish and regret.
Brant’s doctor diagnosed him with Cannabis-Induced Psychosis, a condition where marijuana use leads to severe mental disturbances. Brant’s case highlights how this condition can manifest suddenly and with tragic consequences. Ann, Brant’s mother, recalls the happiness her son brought to her life, and the pain that lingers after his loss.
 |
Shane Robinson
In 2009, Lori Robinson’s son faced a similar fate. Shane, a vibrant 23-year-old, turned to marijuana for pain relief after a knee injury. Despite his parents’ concerns, Shane believed that the drug was a safe alternative to pain medication. However, Shane’s behavior changed drastically. He began to experience hallucinations and delusions. After being hospitalized several times and a prolonged struggle with mental health, Shane took his own life at the age of 25. Lori, Shane’s mother, shared that the psychologists who treated her son questioned marijuana’s role in Shane’s mental illness, but neither Shane nor Brant had any prior history of mental illness, and their symptoms rapidly emerged after using marijuana. Cannabis-Induced Psychosis would finally be added as a recognized mental health diagnosis in the year of 2013. |
Medical and Scientific Insights
Although research still has a long way to go and should continue to examine how mental health disorders are affected by marijuana use independently, it should also focus on understanding the physiological mechanisms, as well as the effects of increased potency and contaminants in marijuana. The progress that has been made is enough to encourage the continuation of this field of research. Recent studies have shown strong associations between cannabis use disorder (CUD) and psychotic episodes. One study showed that 5 out of every 6 teenagers who sought help for a psychotic episode had used marijuana and that they were 11 times more likely to experience psychotic episodes compared to non-users of the drug. Another study showed a 30% increase in schizophrenia cases among men aged 21-30 were associated with CUD.
Dr. David Streem from the Cleveland Clinic shared with the editor of KentWired that he has observed a dramatic increase in psychosis cases over the past decade, which aligns with the increase in marijuana potency from less than 10% in the 90s to 30% or more today.
Advocating for Prevention
Ann Clark and Lori Robinson have become advocates, raising awareness about the dangers of cannabis-induced psychosis. Despite facing skepticism and opposition, they courageously continue to share their son’s stories to educate others about the potential risks of marijuana use.
As marijuana becomes widely legalized, Ann believes that “it only gives our young people a lower perception of harm, and a false sense of security and safety”. However, increased levels of THC and the building body of evidence linking marijuana to mental health conditions, call for greater public health education and regulations.
The tragic stories of Brant and Shane underscore the urgent need for awareness about cannabis-induced psychosis as the use of marijuana becomes more prevalent among younger populations.
The epidemic began about 25 years ago when drug and healthcare companies began to enthusiastically promote these very-addictive chemicals, claiming they were effective in relieving suffering and did not cause dependency.
A study published this past May by researchers at the Johns Hopkins Bloomberg School of Public Health found that one out of every three Americans have lost someone – a relative or a friend – to an opioid or other drug overdose. The US National Institute on Drug Abuse found that more than 320,000 American children have lost parents from overdoses in the past decade, and the annual financial costs to the US of the opioid crisis is $1 trillion.
Incredibly, Israelis today are the largest consumers per capita in the world of opioids, and an untold number of them are addicted or have already died. No one knows the fatality figures here, as the causes of death are described as organ failures, seizures, heart attack or stroke – not listed by what really caused them.
Is this another example of a “misconception” – wishful thinking on the scale of the belief by the government, the IDF, and the security forces that Hamas would “behave” if regularly paid off with suitcases full of cash? Is Israel headed to where the US already is? Perhaps. What is clear is that our various health authorities now have to somehow clean up the opioid mess.
The scandal has been indirectly embarrassing for Israel because among the most notorious companies involved in the opioid disaster is the Sackler family, who own the Purdue Pharma company that manufactured and promoted the powerful and addictive opioid OxyContin and who are now drowning in huge lawsuits. Tel Aviv University’s Medical Faculty that was for decades known as the Sackler Faculty has deleted it from its name.
Last year, the Knesset Health Committee met to discuss the rise in opioid consumption here, with testimony from Ben-Gurion University of the Negev School of Public Health dean and leading epidemiologist Prof. Nadav Davidovitch, who is also the principal researcher and chairman of the Taub Center Health Policy Program. He stressed that inappropriate use of strong pain medications leads to addiction and other severe negative consequences and noted that while most of the rise in consumption is among patients of lower socioeconomic status, the well-off are also hooked. Davidovitch called for the launching of serious programs to treat addicted Israelis based on the experiences of other countries with the crisis.
Opioids attach themselves to opioid-receptor proteins on nerve cells in the brain, gut, spinal cord, and other parts of the body. This obstructs pain messages sent from the body through the spinal cord to the brain. While they can effectively relieve pain, they can be very addictive, especially when they are consumed for more than a few months to ease acute pain, out of habit, or from the patients’ feeling of pleasure (they make some users feel “high”). Patients who suddenly stop taking them can sometimes suffer from insomnia or jittery nerves, so it’s important to taper off before ultimately stopping to take them.
The Health Ministry was forced in 2022 to alter the labels on packaging of opioid drugs to warn about the danger of addiction after the High Court of Justice heard a petition by the Physicians for Human Rights-Israel and the patients’ rights organization Le’altar that claimed the ministry came under pressure from the pharmaceutical companies to oppose this. After ministry documents that showed doctors knew little about the addictions caused by opioids were made public by the petitioners, psychiatrist Dr. Paola Rosca – head of the ministry’s addictions department – told the court that the synthetic painkillers cause addiction. She has not denied the claim that the ministry was squeezed by the drug companies to oppose label changes.
In an interview with The Jerusalem Post, Prof. Pinhas Dannon – chief psychiatrist of the Herzog Medical Center in Jerusalem and a leading expert on opioid addiction – noted that anyone with a medical degree can prescribe synthetic painkillers to patients. “There is no special prescription, no time limit, no supervision,” he said.
“A person who undergoes surgery who might suffer from serious pain is often automatically given prescriptions for opioids – not just one but several,” Dannon revealed. “Nobody checks afterwards whether the patient took them, handed them over to others (for money or not), whether they took several kinds at once, or whether they stopped taking them. They are also prescribed by family physicians, orthopedists treating chronic back pain, urologists, and other doctors, not only by surgeons.”
Dannon, who runs a hospital clinic that tries to cure opioid addiction, said there are only about three psychiatric hospitals around the country that have small in-house departments to treat severely addicted patients. “Not all those addicted need inpatient treatment, but when we build our new psychiatry center, we would be able to provide such a service.”
Since opioids are relatively cheap and included in the basket of health services, the four public health funds that pay for and supply them have not paid much attention. Once a drug is in the basket, it isn’t removed or questioned. Only now, when threatened by lawsuits over dependency, have the health funds begun to take notice and try to promote reductions in use.
Dannon declared that the health funds, hospitals, and pharmacies must seriously supervise opioid use by tracking and be required by the ministry to report who is taking them, how much, what ages, and for how long. Opioids are meant for acute pain, not for a long period. “The Health Ministry puts out fires but is faulty in prevention and supervision,” he said.
A Canadian research team has just conducted a study at seven hospital emergency departments in Quebec and Ontario to determine the ideal quantity of prescription opioids to control pain in discharged patients and reduce unused opioids available for misuse.
They recommended that doctors could adapt prescribing quantity to the specific condition causing pain, based on estimates to alleviate pain in 80% of patients for two weeks, with the smallest quantity for kidney or abdominal pain (eight tablets) and the highest for back pain (21 tablets) or fractures (24 tablets), and add an expiry date for them. Since half of participants consumed even smaller quantities, pharmacists could provide half this quantity to further reduce unused opioids available for misuse.
Rosca, who was born in Italy where she studied medicine and came on aliyah in 1983, has worked in the ministry since 2000; in 2006, she became head of the addictions department.
“In Italy, every psychiatrist must learn about alcohol and other drug addictions including opioids,” she said. “Here, there is no mandatory course in any medical school on the subject. We tried to persuade the Israel Medical Association and its Scientific Council, which decides on curricula and specializations, but we didn’t succeed. Maybe now, in the face of the crisis, it will change its mind. We run optional courses as continuing medical education for physicians who are interested.”
Her department wanted pharmacists to provide electronic monitoring of opioid purchases, but “the Justice Ministry opposed it on the grounds that it would violate privacy. I wasn’t asked for my opinion.”
She concedes that the ministry lacks statistics on the number of addicted people, and Arabs have been excluded from estimates until now. “We’re doing a study with Jerusalem’s Myers-JDC-Brookdale Institute to find out how many. Some say one percent, some say five percent. We hope that by December, we will get more accurate figures. Before the COVID-19 pandemic, the ministry set up a committee on what to do about opioids, but its recommendations were never published, and there was no campaign,” Rosca recalled.
In 1988, the government established the statutory Anti-Drug Authority that was located in Jerusalem’s Givat Shaul neighborhood. It was active in fighting abuse and shared research with foreign experts, but seven years ago, its name was changed to the National Authority for Community Safety and became part of the Ministry for National Security, losing much of its budgets – and, according to observers, its effectiveness as well.
The Health Ministry used to be responsible for setting up and operating clinics for drug rehabilitation, but it handed this over in 1997 to a non-profit organization called the Israel Public Health Association, which employs numerous former ministry professionals. Its director-general, lawyer Yasmin Nachum, told the Post in an interview that the IPHA is very active in fighting drug addiction.
“Israel can’t deny anymore that we are in a worrisome opioid epidemic like that in the US: We are there,” he said. “We see patients every day. Some used to take heroin and other street drugs, but with the easy access and low price, they have switched to opioids. If they are hospitalized for an operation and don’t use all the prescriptions they are given, they sell them to others. We want to have representation in every hospital to warn doctors and patients.”
Of a staff of 1,100, the IPHA has 170 professionals – narcotics experts, social workers, occupational therapists, and others working with 3,000 addicted patients every day. Its other activities include mental health, ensuring safety of food and water, and rehabilitation.
“We work in full cooperation with the ministry,” Nachum said. “Our approach is that when opioids are taken for pain for as long as six months, it’s the time to stop taking them. The doctors provide addicted patients with a drug called buprenorphine, sold under the brand name Subutex, which is used to treat opioid-use disorder, acute pain, and chronic pain.”
Buprenorphine is a mixed opioid agonist and antagonist. That means it has some of the effects of opioids but also blocks some of their effects. Before the patient can take it under direct observation, he must have moderate opioid-withdrawal symptoms. The drug relieves withdrawal symptoms from other opioids and induces some euphoria, but it also blocks the efficacy of many other opioids including heroin, to create an effect.
Buprenorphine levels in the blood stay consistent throughout the month. Nachum said the replacement drug is relatively safe, with some side effects, but fortunately, there is no danger of an overdose.
NARCAN (NALOXDONE) is another prescription drug used by some professionals to fight addiction. Not in Israel’s basket of health services, it blocks the effects of opioids by temporarily reversing them, helping the patient to breathe again and wake up from an overdose. While it has saved countless lives, new and more powerful opioids keep appearing, and first responders are finding it increasingly difficult to revive people with it.
Now, US researchers have found an approach that could extend naloxone’s lifesaving power, even in the face of continually more dangerous opioids by using potential drugs that make naloxone more potent and longer lasting. Naloxone is a lifesaver, but it’s not a miracle drug; it has limitations, the team said.
After the Nova massacre on October 7, when significant numbers of participants who were murdered were high on drugs, the IPHA received a huge number of calls. In December, Nachum decided to open a hotline run by professionals about addiction that has been called monthly by some 300 people. “We also hold lectures for pain doctors, family physicians, and others who are interested, because there has been so little awareness.”
All agree that the opioid crisis has been seriously neglected here and that if it is not dealt with seriously and in joint efforts headed by healthcare authorities, it will snowball and add to Israel’s current physical and psychological damage.
Source: https://www.jpost.com/health-and-wellness/article-811126
A 2020 study in Rhode Island estimated that overdose deaths could be reduced by 30% in the state if jails and prisons made all three medications available to those who needed them. Studies also show that people who receive these medications while in jail or prison are less likely to return to substance use and more likely to continue with treatment in the community afterward.
Less than half of jails nationwide, and fewer than 10% of state prisons, offer all three medications. While 96% of jails did provide the overdose reversal drug naloxone to staff, only 1 in 3 provided naloxone and training on how to use it to decarcerated citizens during the critical period when they were returning to their communities.
Neglecting to provide access to these lifesaving treatments and harm-reduction measures creates deadly gaps for people when they leave jail or prison. The repercussions reverberate throughout communities and generations. They deepen racial inequities and overrepresentation of communities of color within the criminal justice system. They cause devastation for children and families.
Providing medications for opioid use disorder in jails and prisons benefits public health and public safety. It’s cost–effective. It can help break the cycle of recidivism. It can reduce the burden on the wider health care system, including emergency departments.
Programs across the country are underway to offer naloxone and medications for opioid use disorder in jails and prisons, paired with instruction, training, and social support. Federal agencies have launched programs to help people manage withdrawal in jails and provide financial health care support for people who are about to reenter the community. A recently published revised methadone rule now allows any jail or prison registered as a hospital or clinic to dispense medications for opioid use disorder in certain circumstances.
Law enforcement leaders are starting to see how addiction treatment increases safety for everyone. Chris Donelan, the sheriff of Franklin County, Mass., has partnered with researchers to study what happens when jails offer all three FDA-approved opioid use disorder medications. His jail became one of the few in the nation to be licensed as an opioid treatment program.
“When someone is booked into our facility, often we are the first treatment provider the person has seen in years,” Donelan told his University of Massachusetts research partners. “These treatments save lives and help people enter into recovery. Treatment makes the work of our facility much easier. We have less fights, less contraband, and a much safer facility.”
Since 2019, the National Institutes of Health has funded partnerships across the country to figure out how to link people with addiction to care during and after their time in the corrections system. These researchers are poised to share new evidence as it emerges that will help other communities make data-driven changes so they can implement what is most efficient in justice settings.
There is still a long way to go. A dangerous supply of street drugs, fragmented treatment systems, lack of funding, lack of training, pervasive stigma, and complex logistics all work against people with substance use disorders as they work to rebuild their lives after incarceration. Support in recovery and continuity of care are essential during this vulnerable time.
Fundamentally, an individual’s best or only option to receive addiction treatment should not have to be during incarceration. In an ideal world, treatment and prevention systems in the U.S. would proactively address social drivers of health and mental health needs to stop the cycle between addiction and incarceration. Moving away from criminalization of substance use disorders toward a public-health approach would remove a key structural practice that perpetuates inequalities. It would improve lives for people and their families.
| Nora D. Volkow, M.D., is a psychiatrist, scientist, and director of the National Institute on Drug Abuse, which is part of the National Institutes of Health.
|
|
Tisha Wiley, Ph.D., is a social psychologist, associate director for justice systems at NIDA, and leads the NIH Justice Community Opioid Innovation Network initiative, which studies approaches to increase high-quality care for people in justice settings with opioid misuse or opioid use disorder.
|
The International Day Against Drug Abuse and Illicit Trafficking, observed every year on 26 June, serves as a global reminder of the urgent need to combat the menace of drug abuse and illicit trafficking. This day aims to raise awareness about the severe impact of drug addiction on individuals, families and communities worldwide. It also emphasises the importance of prevention, treatment and rehabilitation efforts to address this complex issue.
Governments, organisations and individuals come together on this day to advocate for policies and actions that promote a drug-free world, supporting those affected by addiction and working towards sustainable development and peace. The day calls for solidarity and collective action to safeguard public health and build healthier, safer societies for all.
On the occasion of the International Day Against Drug Abuse and Illicit Trafficking, Firstpost interviewed Dr Prabhat Chand, professor at the Department of Psychiatry, Centre for Addiction Medicine & NIMHANS Digital Academy VKN ECHO, Bangalore to gain insights into drug abuse trends in India and its broader societal implications.
How grave is drug abuse in India and how have their usage patterns changed over time?
Drug abuse in India is a significant public health challenge affecting diverse populations across the nation. The most abused substances after alcohol are cannabis and opioids. According to national surveys, the prevalence of cannabis users is 3.1 crore and about 72 Lakh are problem users. The opioid use increased significantly from 0.7 per cent to 2.1 per cent (i.e., 2.3 crore) during the same period. Other substances such as sedatives (1.08 per cent), inhalants (0.7 per cent), cocaine (0.10 per cent), amphetamines (0.18 per cent), and hallucinogens (0.12 per cent) also contribute significantly to the drug abuse landscape. The International Day Against Drug Abuse and Illicit Trafficking on June 26th, 2024, with the theme ‘The evidence is clear: invest in prevention,’ underscores the urgency of this issue.
How do socio-economic factors influence vulnerability to substance abuse in India? What are the demographics mostly affected and at high risk?
Socio-economic factors such as peer influence, societal pressures, difficult childhood and lack of access to supportive environments significantly influence vulnerability to substance abuse in India. The demographics mostly affected and at high risk include young male adults aged 18-25, people from low socio-economic backgrounds and those with lower educational attainment. Over the years, the age of onset for first substance use has been decreasing consistently.
What are the primary challenges in accessing addiction treatment facilities across different tiers of cities in India?
Access to treatment facilities varies significantly across different regions and city tiers. The treatment gap for addictive disorders is as high as 75 per cent, as per various national surveys. It means 75 out of 100 people with addictive disorders do not have access to care. The challenge is twofold – 1. Accessibility of care 2. Quality of care. For example, for opioid use disorder, Opioid against treatment (OAT) is evidence-based care across the world. But in India, the supply of OAT is available in very few places. That means people have to travel far to access the care. It is well known that addiction is a chronic brain condition and needs good aftercare. These are compounded by strong social stigma and low awareness. This emphasises the need for significant investments to enhance treatment options and optimise resource allocation based on national survey evidence.
How does stigma impact treatment-seeking behaviours in rural areas compared to urban centres?
Social stigma and low awareness about available treatment options significantly impact treatment-seeking behaviours. This leads people with addictive disorders to seek treatment at the later stage of the addiction cycle. Also, the studies show that more than 50 per cent of patients likely have comorbid psychiatric disorders, which also makes care more challenging. Bridging this gap requires tailored health service information campaigns to inform users and the general population about the available treatment services.
What strategies are recommended to bridge the treatment gaps between urban and rural areas, especially in smaller pockets and villages?
To bridge the treatment gaps – 1. Increase access to care 2. Making knowledge the effective interventions to the health care providers 3. Early identification by physicians, nurses or healthcare providers 4. Identification of high-risk youth and provider of holistic support 5. Integrate common substance use along with routine care like hypertension or diabetes.
Integrated care models and effective coordination between drug supply control and entities focused on demand reduction and harm reduction are crucial. Additionally, targeted outreach and education programmes can help prevent substance abuse and identify people in need of treatment at an earlier stage.
Why is it crucial to address gender disparities in treatment-seeking behaviours?
Addressing gender disparities in treatment-seeking behaviours is crucial because men predominantly access services compared to women. Tailored health service information campaigns are necessary to engage women and marginalised communities effectively, ensuring equitable access to treatment and support services. By promoting inclusivity in treatment access, India can foster a supportive societal framework that empowers people affected by substance abuse.
How can integrated care models improve outcomes for people with co-occurring substance abuse and mental health disorders?
Integrated care models can improve outcomes by providing comprehensive services that address both substance abuse and co-occurring mental health disorders. This necessitates significant investments to enhance treatment options and ensure effective coordination between drug supply control, demand reduction, and harm reduction entities. Such models are essential for addressing the multifaceted nature of substance abuse and its associated mental health issues.
What role do government policies, healthcare providers, NGOs and communities play in tackling the drug abuse crisis in India and how can collaboration be enhanced to achieve better outcomes?
Government policies, healthcare providers, NGOs and communities play a crucial role in tackling the drug abuse crisis in India. Collaboration among these entities can be enhanced by fostering coordination between drug supply control and demand reduction efforts, expanding treatment accessibility, promoting inclusivity in treatment access, and implementing targeted outreach and education programmes. By prioritising evidence-based strategies and fostering a supportive societal framework, India can empower people affected by substance abuse to reclaim their lives and contribute meaningfully to society. Sustained efforts in prevention, treatment infrastructure expansion and effective policy formulation are essential to achieving better outcomes and paving the way towards a healthier, drug-free future for Indian citizens.
Healthcare providers like doctors can use the ‘Addiction Rx mobile app’ as a guidance tool for screening, assessment and intervention in addictive disorders. This app is developed as a part of the standard treatment guidelines by the Ministry of Health and Family Welfare DDAP Addiction Rx app: iOS and Android.
The doctors, counsellors and nurses can discuss the cases and enrol in certificate courses at the NIMHANS Digital Academy ECHO weekly tele-platform to learn best practices.
Source: https://www.firstpost.com/india/international-day-against-drug-abuse-a-significant-public-health-challenge-affecting-india-13786238.html
SPECIAL REPORT: ADVANCES IN PSYCHIATRY
Benzodiazepines, a controversial treatment widely prescribed for patients with anxiety and insomnia, carry a considerable risk of abuse. The poster “Mood Over Matter: Literature Review on Benzodiazepine Tapering, Current Practices and Updates on Adjunct Mood Stabilizers,” which was presented at the 2024 APA Annual Meeting, summarized a literature review of current benzodiazepine tapering practices, outpatient detoxification challenges, and potential barriers to discontinuation. The poster presenters also prioritized reviewing literature that highlighted mood stabilizer adjunct use.
Research demonstrates why clinicians should use caution when prescribing benzodiazepines. Results of a recent study revealed that between 2014 and 2016 an estimated 25.3 million (10.4%) adults in the United States reported using benzodiazepines, and approximately 17.2% of these individuals admitted to misuse.
Similarly, the National Institute on Drug Abuse documented that benzodiazepines were implicated in more than 14% of opioid overdose deaths in 2021. Furthermore, a report from the Centers for Disease Control and Prevention pinpointed benzodiazepines as a factor in nearly 7000 overdose deaths across 23 states from January 2019 to June 2020, constituting 17% of all drug overdose deaths. This time frame saw a staggering 520% surge in deaths related to illicit benzodiazepines, and fatalities from prescribed benzodiazepines rose by 22%.
The poster presenters stated that psychiatric and addiction- focused clinicians play an integral role in preventing benzodiazepine misuse and addiction.
To help patients taper benzodiazepines to discontinuation, clinicians must be up-to-date on practices; if clinicians mismanage tapering, sudden withdrawal can prove fatal. Challenges to tapering patients with chronic benzodiazepine use can be found in the Table.
Table. Challenges to Tapering Chronic Benzodiazepine Use
As for tapering strategies, the presenters suggested adjunct mood stabilizers such as carbamazepine and oxcarbazepine. Carbamazepine, when used as an adjunct or prophylactically, can help reduce intense withdrawal symptoms and thus keep patients on track for discontinuation. However, carbamazepine has received criticism regarding its efficacy, and it is well documented to have a series of concerning adverse effects such as skin reactions, agranulocytosis, leukopenia, and significant drug-drug interactions by nature of its metabolism. This makes some clinicians wonder: Are the risks worth the benefit?
Oxcarbazepine has also been proposed as an alternative. Results of some small-scale clinical trials noted moderate efficacy for oxcarbazepine in helping patients with detoxification, and it has fewer adverse effect concerns. The presenters suggested that other mood stabilizers, particularly those with antiepileptic effects, require further research for their potential help with benzodiazepine addiction.
“Through a more current literature review, we hope to increase the tools available to psychiatrists for more success in discontinuation and maintaining sobriety for patients,” the presenters wrote.
In a previous Psychiatric Times article, Steve Adelman, MD, of the University of Massachusetts Medical School in Boston, suggested 8 universal precautions adapted from Gourlay et al for use by psychiatrists who must decide whether to initiate or continue pharmacotherapy with benzodiazepines. They include making a diagnosis with an appropriate differential and creating and ratifying a treatment agreement. However, other clinicians, such as Daniel Morehead, MD, a Psychiatric Times columnist and featured cover author in this issue, suggest that although benzodiazepines carry risks, those risks are exaggerated by government officials, critics, and the public at large.
Source: https://www.psychiatrictimes.com/view/how-to-safely-and-effectively-taper-benzodiazepines
By Carole Tanzer Miller HealthDay Reporter
MONDAY, June 10, 2024 (HealthDay News) — Though overdose deaths continue to surge, there is no approved medication to treat methamphetamine use disorder.
Now, an experimental two-drug therapy has yielded promising results, UCLA researchers report.
“These findings have important implications for pharmacological treatment for methamphetamine use disorder,” said researcher Dr. Michael Li, an assistant professor-in-residence of family medicine at the David Geffen School of Medicine at UCLA, adding that methamphetamine-involved overdoses have surged.
His team published its findings June 10 in the journal Addiction.
In urine tests for methamphetamine, drug-free results rose 27% among participants who received a combination of injectable naltrexone plus extended-release oral buproprion. Negative tests rose only 11%, meanwhile, in a control group.
Methamphetamine abuse is a growing problem around the world, with an estimated 34 million users in 2020 compared to 33 million 10 years earlier. In the United States alone, overdose deaths rose fivefold between 2012 and 2018.
The National Institute on Drug Abuse Clinical Trials Network has supported various trials, including this one, to evaluate different treatments for methamphetamine use disorder.
This trial, known as ADAPT-2, ran from May 2017 to July 2019 at eight sites. More than 400 participants were included, including 109 who received the experimental drug therapy in the first phase. That demonstrated that the combo worked at six weeks.
The new findings are from the trial’s second phase, which looked at a longer period. Partipants were drug-tested at weeks seven and 12 and again, after treatment, at 13 and 16 weeks.
While their results were encouraging, researchers said further study is needed to find out if the treatment lasts longer than 12 weeks and leads to further reductions in drug use.
“Prior stimulant use disorder treatment trials suggest that change in use is gradual [consistent with our findings], unlikely to result in sustained abstinence in a typical 12-week trial, and dependent on treatment duration,” the researchers said in a UCLA news release. “This warrants future clinical trials to quantify changes in [methamphetamine] use beyond 12 weeks and to identify the optimal duration of treatment with this medication.”
Source: https://www.medicinenet.com/two_drug_treatment_could_curb_meth_addiction/news.htm
Cultural, systemic and historical factors have converged to create the perfect storm when it comes to Black overdose deaths.
By Liz Tung – June 14, 2024
Reporter at The Pulse
WHYY (PBS) 14th June 2024
A recent study from the Pennsylvania Department of Health has found that Black people who died from opioid overdoses were half as likely as white people to receive the life-saving drug naloxone, otherwise known as Narcan. The study also found that Black overdose deaths in Pennsylvania increased by more than 50% between 2019 and 2021, compared with no change in white overdose deaths.
In an email, a representative with the Department of Health said that similar rises in overdose deaths are being seen across the country, especially among Black, American Indian and Alaska Native populations. But researchers are still investigating what’s behind the spike.
“There does not appear to be a single reason why rates are increasing for Black populations and holding steady among white populations,” the statement reads. “The volatile and rapidly changing drug supply certainly has been a challenge as fentanyl is now found in every type of drug. Inequities in terms of treatment for substance use disorder may also play a factor as white people are more likely to have better access to the most evidence-based treatments and are more likely to stay in treatment.”
Abenaa Jones, an epidemiologist and assistant professor of human development and family studies at Penn State who was not involved in the study, has conducted similar research in Baltimore. She agreed that fentanyl-contaminated drugs — which are more common in lower-income neighborhoods — and less access to health care are likely factors in the growing number of overdose deaths among Black populations.
Jones said the criminal justice system, and its unequal treatment of Black people, also plays a role.
“We know that the intersection of criminal justice and substance use, and criminalization of drug use and how that disproportionately impacts minorities, can limit the accessibility of harm reduction services to racial-ethnic minorities for fear of harassment by police for drug paraphernalia,” Jones said, adding that even syringes obtained through needle-exchange programs can be considered illegal paraphernalia.
Fear of arrest, in turn, leads more people to using drugs in isolation.
“That may protect you from criminal legal involvement, but then in the event of an overdose, you may not have someone to help you,” Jones said. “So it could be that by the time the EMS come, it’s been too long for them to even consider administering naloxone.”
An unexpected observation that Jones made in the course of her research could also be a factor in rising death rates — the fact that many of the Black people dying of opioid overdoses are older.
“For any other racial groups, overdose deaths peak around midlife — 35, 45,” she said. “For Black individuals, it’s more like 55, 64, and we were wondering what was going on with that.”
After investigating that question, Jones and her colleagues formulated a working theory.
“The running hypothesis for us is that this is a cohort effect,” she said. “Individuals who’ve been using drugs over time, particularly Black individuals back from the ‘80s and ‘90s with the cocaine epidemic, never stopped using.”
Those individuals may have remained relatively stable until fentanyl began to contaminate their drug supply without them knowing.
“So whatever harm reduction tools that you were using for so many years that’s been helping you, when fentanyl’s involved, it’s a different game,” Jones said. “You have to use less, but you have to also know that you have fentanyl in your drugs, right?
It’s a problem that Marcia Tucker, the program director of Pathways to Recovery — a partial hospitalization program focused on co-occurring substance use and mental health challenges — sees frequently among their mostly Black clients.
“If you come into treatment saying that I’m a cocaine user, or I’m a crack cocaine user, or I use marijuana, you’re not even thinking that an opioid overdose or fentanyl overdose could possibly happen to you,” Tucker said. “And it does happen.”
In fact, Tucker said, she’s seen more of these kinds of overdoses over the past two years than in the three decades she’s spent working in addiction treatment. Despite that, there’s still a lack of education — and even stigma — surrounding both medication-assisted treatments (MATs) for opioid addiction, and the use of naloxone.
“I think sometimes culturally with the African American community, as far as MATs are concerned, there are some taboos about getting that extra help when they decide to come into treatment and get clean,” she said. “A lot of people feel like they want to do it from the muscle. They see it as another form of using.”
She said others may not know how to use naloxone, what kinds of effects it has or how to get it.
“I think a lot of folks don’t even know that they can walk into a pharmacy and get naloxone — you don’t have to have a prescription for that,” Tucker said. “And I think that information is just not always presented to communities, especially poor communities that don’t have a lot of resources.”
Other sources of hesitation are more immediate. Aaron Rice, a therapist at Pathways to Recovery, said that many of their clients fear naloxone because of its physical effects.
“I think they associate it with precipitated withdrawal at times,” Rice said, referring to the rapid-onset withdrawal that can cause symptoms including anxiety, pain, seating, nausea, vomiting and diarrhea.
“The only thing they’re thinking about is feeling better. And that feeling is going to supersede logic at that moment. It always does.”
The Department of Health acknowledged that the study only paints a partial picture, as it doesn’t include individuals whose overdoses were reversed by naloxone, and added that during the years of the study (2019–2021), naloxone was available by prescription only — a fact that likely played into the race-based disparity.
“There are recognized inequities in access to health care among persons of color, the concept of which likely extends to access to naloxone,” the Department of Health statement reads. “Historically, many public health materials and messaging more narrowly focused on persons using opioids. With people now taking two or more drugs together (whether intentionally or unintentionally), public health materials and messaging need to be more inclusive of all persons using drugs, regardless of the type.”
The study, researcher Abenaa Jones, Marcia Tucker and Aaron Rice all agreed on at least one intervention that could increase Black people’s access to naloxone — relying on trusted community leaders and institutions, like churches, to help educate residents and distribute the overdose-reversing drug.
“I just can’t stress enough how it’s a lifesaver — it’s the difference between life and death,” Tucker said. “I think people who aren’t medical professionals and find themselves in a situation where it might need to be used would probably be a little fearful — fearful about how to use it or how the person is going to react or whether it’s really going to work — just know that you’re better off with it and trying it. You don’t want to have to second guess yourself later and say, ‘I wish we had it. I wish we had gotten it,’ or, ‘I wish we had used it.’”
Source: https://whyy.org/articles/black-pennsylvanians-overdoses-naloxone-less-likely-to-receive/
A friend called me today and informed me the federal Minister for Mental Health and addictions stated the “minister believes fear and stigma are driving criticism of the government’s decision to support prescribing pharmaceuticals to drug users to combat the country’s overdose crisis…”
After reading the article I realized there will be no hope of taking control of this drug crisis while the Liberals are in power, or any other government that supports harm reduction.
The feds have allowed B.C. to experiment with Canadian lives in that province, pushing experimental policies on the population which have failed, increasing fatal overdoses, not reducing them. How many more thousands of people must die before you admit your policies are a failure?
In 2003, due to overdoses from heroin, Vancouver introduced the first safe injection site on the continent, but after 20 years the evidence is clear that harm reduction practices only magnify the issues. Instead of admitting failure, they have blamed many other factors for why fatal overdoses, the numbers of addicts, mental health issues, crime and homelessness continue to increase. Instead of dramatically increasing mental health and addiction treatment, they pump billions of taxpayer and donor dollars into programs that encourage and enable addicts, and even their safe consumption sites now fail to offer any assistance for treatment. They have decriminalized small amounts of drugs, and hand out prescribed safe supply illegal drugs now made in B.C., such as cocaine, morphine, MDMA (ecstasy) and heroin, and the interview process for these exempted controlled drugs includes minors.
Minors do not need parental consent and parents will not be informed. This is how insane the federal government has become, allowing B.C. to progress into the abyss with these wild experiments that have taken thousands of lives, with no end in sight as fatal overdoses increase every year.
B.C. has over 32 safe consumption sites (SCS), and with all the radical programs they have been allowed to employ, they still have more fatal overdoses per capita than Alberta, Saskatchewan or Manitoba.
Barry Ewing – Lethbridge Herald
Source: https://lethbridgeherald.com/commentary/letters-to-the-editor/2024/02/28/theres-no-hope-of-fixing-drug-crisis-through-harm-reduction/
Why Do People Relapse? Understanding and Overcoming Relapse in Substance Abuse Recovery: Embarking on the journey of addiction recovery is a tough, but worthwhile goal. However, it is not uncommon for you to face setbacks in the form of relapse during your recovery journey.
In this blog post, we will explore the reasons why people relapse in drug addiction, explore the various stages of relapse, and discuss effective strategies for preventing relapse. Understanding these aspects is crucial for you, your family members, and addiction treatment programs to help you best achieve recovery.
The biggest stumbling block people face on the path of recovery is when they slip up. Knowing why relapse happens is critical for those working on getting clean and those helping them out. Let’s dive into the four big causes of going back to drugs during recovery – how mental health problems, ineffective ways of dealing with stress or emotions, intense withdrawal symptoms, and not setting solid limits work together to trip people up.
Mental health challenges often coexist with substance abuse. Attending a dual diagnosis treatment program, which addresses both mental health issues and substance use disorder, can significantly increase the effectiveness of your recovery efforts.
Your dual diagnosis treatment team understands how substance use disorders are a chronic disease and will work to give you the tools you need to successfully tackle recovery and lay the groundwork for a sober life.
Many individuals turn to drugs or alcohol as a coping strategy to deal with negative emotions, stress, conflict in relationships, and peer pressure. As the Marlatt and Gordon model establishes, the seeds of relapse are planted in a high-risk scenario and nurtured by unhealthy coping skills.
If you are facing elevated stress levels, coupled with poor coping skills, you are at a much greater risk for addiction relapse. Negative emotions like anger, depression, anxiety, and boredom can also increase your risk for returning to drug and alcohol use for comfort.
Simply put, without effective coping skills, relapse rates drastically increase.
The physical discomfort experienced during withdrawal can be overwhelming, leading your to turn to substance use to alleviate these symptoms. All will to stay sober can easily vanish in the face of intense cravings and physical pain, even if you are fully aware of the consequences.
The vulnerability during the withdrawal phase, coupled with the desire to avoid physical and mental distress, underscores the importance of comprehensive support and coping strategies to navigate this critical stage of the recovery journey successfully.
A strong contributor to relapse is your social environment- the people you surround yourself with. Having friends or family members who engage in drug abuse and significantly challenge your recovery and your resolve to stay sober. Even just being around them can trigger intense cravings, heightening your risk of relapse.
Establishing and maintaining well-defined boundaries is crucial for preventing relapse. Without clear boundaries, individuals may find themselves in situations that trigger drug use.
A relapse can happen in many ways. What is commonly seen as a “traditional” relapse happens when you consciously decide to consume alcohol or use drugs. This might involve choosing to smoke marijuana to reduce stress after a substantial period of sobriety or having a glass of wine with friends, believing you can handle it without spiraling into excessive use.
On the flip side, a “freelapse” is the informal term for an accidental relapse, which occurs when you unintentionally use drugs or alcohol.
At times, the path toward a relapse unfolds without you even realizing it, manifesting in actions taken weeks or months before using drugs or alcohol. Specific thoughts, emotions, and events can act as triggers, sparking cravings and urges for drug use. If not effectively addressed, these triggers can significantly elevate the risk of relapse, which is why it is extremely important to proactively manage these risk factors in the recovery process.
The onset of the emotional relapse stage before actually picking up a drug or sipping a drink. In this phase, you may find yourself struggling to manage your negative emotions in a healthy manner. Rather than addressing your feelings openly, there might be a tendency to bottle them up, withdraw from social interactions, deny the existence of problems, and overlook self-care.
Although the thought of drug and alcohol use may not be at the forefront of your mind during this stage, the avoidance of confronting emotional pain and challenging situations sets the stage for potential relapse in the future. Recognizing and addressing these early signs becomes crucial in preventing future relapse and fostering a healthier recovery journey.
In the mental relapse phase, you may struggle with conflicting emotions surrounding sobriety. Within this stage, there is an internal struggle: one side strives to remain sober, while the other wrestles with cravings, harboring secret thoughts about a potential relapse.
Mental relapse goes beyond mere internal conflict; it includes romanticizing past drug use, downplaying the negative feelings and consequences, and actively seeking opportunities for using drugs or alcohol. This intricate mental struggle highlights the delicate balance you have to maintain between your substance addiction and your will to recover.
The physical relapse stage is where the actual addiction relapse occurs. What starts out as an initial slip, perhaps with just a few sips of a drink or or hit of a drug, can quickly escalate into a full-blown relapse, characterized by a complete loss of control over your actions and total drug dependence.
The importance of recognizing early warning signs and implementing effective strategies to prevent progression towards physical relapse in the ongoing journey of drug recovery.
Whether you have relapsed before or not, knowing what to do if you slip back into the throws of drug abuse is critical for getting back on track and preventing future relapse. No relapse is insurmountable and there’s always an opportunity for recovery.
If you have experienced a relapse, quickly follow these proactive steps to minimize the negative effects of drug use and prevent further substance use.
1. Ask for help. Seeking assistance from family members, friends, and other addicts in the recovery process can significantly help you navigate the challenges of relapse. Create a sober support system and immerse yourself in it. The worst thing you can do in early recovery is suffer in silence.
2. Find support groups near you. Both traditional twelve-step support groups like Alcoholics Anonymous (AA) and Narcotics Anonymous (NA), as well as science-based alternatives like SMART Recovery, offer nonjudgmental spaces for you to discuss substance abuse relapses openly. With meetings available on a daily basis, you can quickly find a support group that’s right for you, allowing you to talk about your relapse experiences within 24 hours of it happening.
3. Avoid triggers at all costs. Being around people, places, situations, etc… that are triggering to you, in the aftermath, of a relapse can be detrimental to your recovery, and actually intensify your cravings. By putting distance between yourself and your triggers helps to create an environment ripe for addiction recovery.
4. Establish healthy boundaries. In all stages of substance abuse recovery, but especially shortly after a relapse, it’s vital to set boundaries to protect yourself from threats against your sobriety. A key component to maintaining firm personal boundaries is steering clear of people who are not completely onboard with your choice to be sober. These people will only try to pressure you back into a lifestyle of using drugs or alcohol, so surrounding yourself with your sober support system is the only way to remain sober after a relapse.
5. Prioritize your self-care. Both your mental and physical well-being should be taken care of, especially in the wake of a relapse, and is one of the key components of recovery, and it gives you a way to relieve tension and reduce stress.
6. Self-reflect about why the relapse happened. Rather than seeing a relapse as a setback, you can see it as a learning tool. Dedicate time to reflect on the circumstances leading to the relapse. Explore the events that unfolded before the relapse occurred. Did you try out any other coping mechanisms prior to resorting to substance use? Think about potential alternatives to using or drinking that you could have used.
Asking yourself these questions offers insights into what you can do differently, encouraging a constructive approach to managing challenges that arise along your path to substance use disorder recovery.
7. Come up with a relapse prevention plan. This is a guide designed to be a steadfast companion to help you maintain sobriety. It should be as detailed as possible, and easy to follow when needed.
Acting promptly after a relapse significantly increases your chances of a quick recovery with minimal negative consequences. It is important to remember that recovery is not linear or bound by time constraints. It is never too late to regain control after a relapse.
If early recovery seems too overwhelming, seek drug addiction treatment to help manage the task. Some treatment centers offer an inpatient program with medical detox and behavioral therapies to help you regain your footing and relapse prevention classes to help you assimilate back into your daily life with the help of addiction specialists.
Preventing relapse in addiction recovery involves a complex approach that addresses both the physical and psychological aspects of your substance use.
To start off, recognizing the specific situations or emotions that may lead to relapse and developing effective coping strategies, whether through therapy, mindfulness, or healthy activities, is paramount in navigating through moments of weakness. Building and maintaining a strong support system, made up of supportive friends, family, and possibly support groups, provides a crucial safety net.
Additionally, the creation of a personalized relapse prevention plan, including detailed strategies for recognizing and managing triggers, is vital to staying sober. Regular self-reflection and adjustments to the plan over time ensure its continued effectiveness, empowering you to maintain lifelong sobriety.
Creating a personalized plan to prevent addiction relapse is a crucial component of substance abuse recovery. This plan should include strategies for recognizing triggers and coping with cravings. It should also outline your specific triggers for drug use, as well as at least 3 positive coping skills that work for you.
Additionally, your relapse prevention plan should list specific people who are in your sober support system, with their phone numbers, who you can call for help when you are feeling the urge to use. You should also compile a list of local addiction support groups that can be there for you in your time of need.
Regularly consulting and revising this plan is instrumental, making sure it stay relevant to your evolving life experiences and fortifying your commitment to a sober life.
Building a strong support system and fostering a supportive environment are key factors in maintaining long-term sobriety. Creating a nurturing atmosphere involves not only external factors but also the changes you make within yourself.
Most addicts relapse because they do not change both the people they hang around with, as well as the way they approach situations in life after completing an addiction treatment program and in the early stages of recovery. By attending a local support group meeting, you can meet and befriend people who are going through the same things you are and you can be pillars of strength for each other.
Further, you may find it helpful to make a list of fun activities that do not involve drinking alcohol or using drugs. This list may be helpful when you are experiencing cravings and need to divert your attention.
Cultivating a positive mindset not only enhances your motivation and resilience during challenging times but also reinforces your belief in yourself and your capacity for personal growth and living a fulfilling, sober life. Your positive outlook serves as a powerful ally in overcoming obstacles, nurturing a sustainable foundation for lasting recovery.
Prioritizing self-care, including healthy habits and activities, contributes to overall well-being and reduces the risk of relapse. Self-care encompasses a range of activities that bring you pleasure without causing harm, including but not limited to yoga, meditation, exercise, reading, journaling, and eating healthy foods.
Recovery from drug addiction is a complex journey that requires dedication, resilience, and ongoing support. By understanding the reasons behind relapse, implementing effective treatment programs, and adopting preventative strategies, you can increase your chances of achieving and maintaining long-term sobriety.
Remember, relapse does not signify failure but rather serves as an opportunity for growth and reinforcement of your commitment to recovery.
Source: https://www.hippocraticpost.com/addiction/understanding-and-overcoming-substance-abuse-relapse/
Foreword
The National Institute on Drug Abuse (NIDA) is pleased to publish in its Research Monograph series the proceedings of the 48th Annual Scientific Meeting of the Committee on Problems of Drug Dependence, Inc. (CPDD). This meeting was held at Tahoe City, Nevada, in June 1986.
The scientific community working in the drug abuse area was saddened by the untimely death of one of its very productive and active leaders: Joseph Cochin, M.D., Ph.D. Joe was a talented scientist who was greatly admired by his students and colleagues. For the past five years, Joe had served as the Executive Secretary of the CPDD. This monograph includes papers from a symposium on “Mechanisms of Opioid Tolerance and Dependence,” dedicated to his memory. These papers were presented by many of his friends and colleagues, who took the opportunity to express their high esteem for Joe.
The CPDD is an independent organization of internationally recognized experts in a variety of disciplines related to drug addiction. NIDA and the CPDD share many interests and concerns in developing knowledge that will reduce the destructive effects of abused drugs on the individual and society. The CPDD is unique in bringing together annually at a single scientific meeting an outstanding group of basic and clinical investigators working in the field of drug dependence. This year, as usual, the monograph presents an excellent collection of papers. It also contains progress reports of the abuse liability testing program funded by NIDA and carried out in conjunction with the CPDD.
This program continues to represent an example of a highly successful government/private sector cooperative effort. I am sure that members of the scientific community and other interested readers will find this volume to be a valuable “state-of-the art” summary of the latest research into the biological, behavioral, and chemical bases of drug abuse.
Charles R. Schuster, Ph.D.
Director
National Institute on Drug Abuse
For the full contents, please go to:
Source: https://babel.hathitrust.org/cgi/pt?id=ien.35557000188076&seq=11 This version September 2023
Powered by WordPress






That’s as true of spy balloons as it is of public-health policies with nothing but negative domestic implications.