by Payten M. Romero, Kennon J. Heard, Nicholas R. Oblizajek, Abdul Qadeer,Robert W. Kirchoff,
Cannabis hyperemesis syndrome (CHS) is a disorder of gut-brain interaction with symptoms of nausea, severe episodic vomiting, and abdominal pain. The primary pathways implicated in CHS are the endocannabinoid system and the transient receptor potential vanilloid-1 pathway. The lack of cannabis standardization and Fusarium mycotoxin contamination may also play a role in the development of CHS. Hot showers, capsaicin, and antipsychotics – but not traditional anti-emetics – have been shown effective for symptom management. Until recently, there has not been a specific diagnosis code for CHS, making it difficult for healthcare providers to document CHS in electronic health records. This hindered proper surveillance and epidemiology studies. Further research is needed to characterize the cannabis composition, mechanism of action, and genetic susceptibility associated with CHS.
A case study
A 24-year-old male presents to the emergency department with a 5-day history of vomiting. During the evaluation, he is violently retching and struggles to answer questions. He reports that the symptoms today started when he awoke this morning and he has been vomiting every 10 min for the last 2 h. He states that he tried to take a bath because that has helped him in the past but today it did not help. The patient reports that he does not drink or smoke cigarettes, but that he started smoking cannabis 2 years ago and he smokes cannabis several times a day for his anxiety and that he has done this for the past 2 years.
On his examination, he appears very uncomfortable. His heart rate, respiratory rate, temperature, blood pressure, and pulse oximetry are normal. His mouth and lips appear dry but his exam is otherwise unremarkable and notably he has no abdominal tenderness.
A review of his medical records shows that he has been treated in the emergency room twice in the past week for similar symptoms. An extensive workup including laboratory studies, an abdominal ultrasound, and an abdominal computed tomography scan is normal. Specifically, in laboratory studies, the electrolytes and renal function were normal. Both times he was treated with intravenous fluids and ondansetron with minimal improvement and was discharged home with a prescription for ondansetron and instructions to follow up with a gastroenterologist scheduled in 2 weeks. He was also referred to addiction medicine and his primary care provider.
After the initial treatment, the patient continued to have repeated episodes of retching and complained of severe nausea. Given his recurrent vomiting, an unremarkable prior workup, and long history of daily cannabis use, the team diagnosed CHS. The team ordered intravenous fluids for hydration and laboratory studies to evaluate him for dehydration which showed mild dehydration. The team also administered haloperidol to treat his nausea.
What is cannabis hyperemesis syndrome?
Cannabis hyperemesis syndrome describes a collection of symptoms that include severe episodic vomiting and abdominal pain in patients who use cannabis frequently (usually daily) for a prolonged time (usually a year or more) [1]. It was first described in Australia in 2004 [2] and was considered uncommon. However, with the widespread decriminalization of cannabis in the U.S., clinicians noted an increase in patients presenting to emergency departments with cyclic vomiting who reported frequent cannabis use [3]. The prevalence of CHS is not well described due to a lack of diagnosis codes [4]. However, a new diagnosis code for CHS (R11.16) is now effective in the 10th revision of the International Classification of Diseases (ICD-10) starting on October 1, 2025 [5].
What causes cannabis hyperemesis syndrome?
Cannabis hyperemesis syndrome is sometimes referred to as cannabinoid hyperemesis syndrome [1]. Despite the lack of mechanistic studies of CHS, literature reviews suggest the etiology of cannabinoid receptor 1 and 2 (CB1 and CB2) activation by tetrahydrocannabinol (THC) [∗∗6, ∗∗7, 8]. While the sensation of nausea is primarily a neurologic phenomenon, CHS is largely classified as a chronic disorder of gut-brain interaction, not primarily a neurologic disorder. Nausea is mediated by the area postrema and central emetic pathways. A key component of these pathways is the endocannabinoid system (ECS), which consists of a retrograde signaling pathway activated by CB1 in the CNS and gut [7]. The ECS is a neuromodulator and regulator of nausea and vomiting, especially during stress response [7]. Chronic use of cannabis down-regulates and de-sensitizes CB1 receptors [8]. This leads to a decrease in ECS signaling that is inversely correlated to the activation of the hypothalamic-pituitary stress axis (HPA) [9]. The increased activation of the HPA may account for the vomiting effect of anxiety, which is also observed in many patients with CHS. The cannabinoid etiology of CHS was extensively reviewed by Loganathan et al. (2024) [6].
Another plausible mechanism of CHS involves the transient receptor potential vanilloid-1 (TRPV1) channel-dependent pathway in the medulla, along gastric enteric and vagal nerves, and on cutaneous receptors in the dermis and epidermis [10]. Transient receptor potential vanilloid-1 is a polymodal, non-selective cation channel that can be activated by THC, low pH, and heat [10,11]. It is down-regulated and de-sensitized with prolonged exposure to cannabis, leading to nausea, altered gastric motility, and abdominal pain [10]. The TRPV1 channel also binds to capsaicin, a chemical found in chili peppers, which controls the release of substance P (a mediator involved in pain perception) and can alleviate the symptoms of CHS [1].
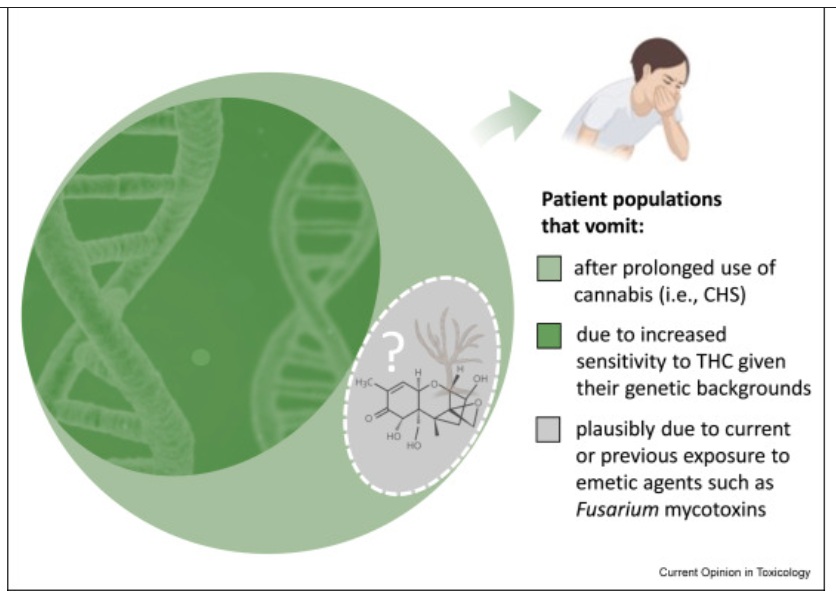
Genetic polymorphisms may also play a role in the onset of CHS symptoms (Figure 1) [12]. A preliminary study by Russo et al., in 2021 identified an association between CHS and genetic polymorphisms, including catechol-O-methyltransferase, which catabolizes dopamine; ATP-binding cassette transporter A1; TRPV1; the dopamine receptor D2 (DRD2); and the cytochrome P450 2C9 enzyme, which metabolizes THC in the liver [13]. However, the study had a limited sample size (n = 28) and was not validated in larger cohorts or incorporated into any diagnostic criteria. Other larger genome-wide association studies have examined genetic polymorphisms in cannabis use disorder [14,15], but vomiting is not examined as a phenotype in these studies. Further studies are needed to fully characterize the genetic profiles of patients with CHS.
Figure 1. Different causes of cannabis hyperemesis syndrome (CHS): Prolonged use, genetic backgrounds, and contaminant exposure.
Cannabis hyperemesis syndrome is linked to prolonged use of cannabis. Tetrahydrocannabinol (THC) activates cannabinoid receptor B1 and B2 (CB1 and CB2), with CB1 in the central nervous system being particularly relevant for emesis control, and THC also binds to transient receptor potential vanilloid-1 channels. Stimulation of CB receptors can lead to increased vagal nerve discharges contributing to vomiting. Some patients are more susceptible to the vomiting effect of high-dose THC due to their genetic backgrounds. Due to the lack of standardization in cannabis composition, production methods, and compliance testing, some patients may vomit due to exposure to cannabis contaminants (e.g., Fusarium mycotoxins) with a different mechanism of action.
What are the potential roles of cannabis standardization and Fusarium mycotoxins?
At the time of publication, cannabis is being rescheduled federally to a less restrictive Schedule III category in the U.S. [16]. Yet, cannabis remained listed in the U.S. as a controlled substance. Unlike other agricultural crops (e.g., tobacco), there is a lack of standardization in cannabis composition, production methods, and compliance testing in the state-legalized markets [17, ∗18, 19, 20]. Furthermore, black- and gray-market cannabis is estimated to account for over two-third of the cannabis market in the U.S. in 2022 [21] and the contamination level of pesticide residues, mycotoxins, and other chemicals in black- and gray-market cannabis is largely unknown. As such, it remains unclear whether the active components of cannabis (i.e., cannabinoids) are solely responsible for the etiology of CHS.
In a study in Arizona and California in 2025, Fusarium mycotoxins were found in one in six illegal cannabis samples [22]. The poisoning symptoms of Fusarium mycotoxins deoxynivalenol (vomitoxin), nivalenol, and T-2 toxin resemble the symptoms of CHS [23,24]. In an animal study [25], deoxynivalenol was shown to activate the transient receptor potential ankyrin 1 (another TRP channel different from TRPV1) and the calcium-sensing receptor, leading to increased vagal nerve discharges contributing to vomiting. Given that CHS appears with prolonged and frequent cannabis use and Fusarium contamination can vary from batch to batch, it is plausible that the sensation of cannabis use by itself may trigger vomiting via associative learning (i.e., classical conditioning). This mechanism has not been established as a primary etiology of CHS due to limited evidence in the literature. Furthermore, it is difficult to trace back any active components or contaminants of cannabis that could have accounted for the CHS patient’s visit to the emergency department. Further studies are needed to examine how cannabis composition is linked to CHS development.
Why do hot showers help?
One of the most notable aspects described by patients with CHS is the significant relief of symptoms with hot showers [26]. While not a universal feature, up to 90 % of patients report some relief [27]. It is important to note that the relieving effect of a hot shower is not unique to CHS, as a study in 2021 found that patients who did not use cannabis but had cyclic vomiting also demonstrated lessened nausea, vomiting, and abdominal pain from a hot shower [28].
There are several theories for why hot showers may be effective in relieving symptoms of CHS. The most widely supported theory in the literature is the TRPV1 channel activation theory. Hot water at temperatures above 41 °C activates cutaneous TRPV1 channels, modulating emetic pathways and may provide antiemetic effects through the release and subsequent depletion of substance P and other neuropeptides. This is further supported by the observed efficacy of topical capsaicin, a TRPV1 agonist, in relieving CHS symptoms [1]. The second theory has to do with the fact that CB1 in the hypothalamus aids in thermoregulation [26]. Through CB1-mediated thermoregulation disruption, high doses of cannabis decrease heat production and cause hypothermia [26,29]. Hot water decreases sympathetic nervous system activation, relieving the hypothermic effects that occur with large amounts of use and cannabis accumulation in the body [26,30]. The third theory is referred to as the cutaneous steal syndrome theory. In this theory, cutaneous vasodilation from heat changes the core temperature and redirects splanchnic circulation, resulting in relief in gastrointestinal/abdominal symptoms and pain [26].
Why do standard anti-emetics not work and why are anti-psychotics so effective?
Anti-emetics are relatively ineffective at treating CHS [31, ∗∗32, 33]. A plausible explanation is that the pharmacotherapeutic targets of anti-emetics are not implicated in CHS. The most common anti-emetics for treating nausea and vomiting, such as ondansetron, are serotonin 3 receptor antagonists, which are not implicated or dysregulated in CHS [34]. Other anti-emetics, despite having different mechanisms of action for the most part, like promethazine and metoclopramide, were also found to be less effective in treating CHS [33]. Promethazine’s main mechanism of action is antagonism on histamine H1 receptors, with some anti-cholinergic, anti-muscarinic and other properties [35]. Metoclopramide mechanisms of actions include both antagonism to the serotonin 3 receptors and the dopamine 2 receptors [36]. The antagonism to the dopamine 2 receptor in metoclopramide has a short life, and extrapyramidal symptoms had arisen with higher doses of metoclopramide for treating nausea and vomiting [37]. With clinicians being possibly conservative about higher dose of metoclopramide, the standard dose being given (10 mg) has been suggested to not reach a clinically relevant anti-emetic effect [37].
While evidence supporting treatments for CHS is limited to case series and small clinical trials, anti-psychotics have been shown more effective in treating nausea, abdominal pain, and vomiting linked to CHS [33,38]. Anti-psychotics are often antagonists to DRD2 in the chemoreceptor trigger zone in the brainstem, which regulates nausea and vomiting [32,39, 40, 41]. Haloperidol, an anti-psychotic, modulates the HPA stress axis, which is posited to also be dysregulated in CHS through the down-regulation of CB1 receptors [42], suggesting that haloperidol modulates two areas of mechanisms implicated in CHS. Droperidol, another anti-psychotic, is effective in reducing the length of hospital stay and decreasing the use of opioids and other medications in CHS patients [43]. Overall, limited data suggest that the anti-emetics are not as effective as anti-psychotics.
Future directions
As cannabis legalization efforts continue in the U.S. and worldwide, CHS has become an increasingly common condition that leads to emergency room visits. The new ICD-10 diagnosis code for CHS can greatly improve surveillance and epidemiology studies, resulting in a better understanding of the public health impact of CHS. While different signaling pathways have been proposed as part of the CHS etiology, more mechanistic studies are needed to understand the interaction of these pathways and the role of genetic backgrounds in CHS development. As the contribution of illicit cannabis to CHS incidence remains unclear, a nationwide cannabis checking program similar to existing programs for street drugs [44] and other substances [45] can clarify the causal roles of cannabinoids and cannabis contaminants in CHS. For regulated cannabis, standardizing production methods and compliance testing (particularly for emetic agents such as Fusarium mycotoxins) can be a useful mitigation measure for CHS.